
Self-Perception and Self-Acceptance Are Related to Unhealthy Weight Control Behaviors in Catalan Adolescents: A Cross-Sectional Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection and Tests
2.2.1. Perceptual and Cognitive-Affective Dimensions
2.2.2. Behavioral Dimension
2.3. Statistical Analysis
3. Results
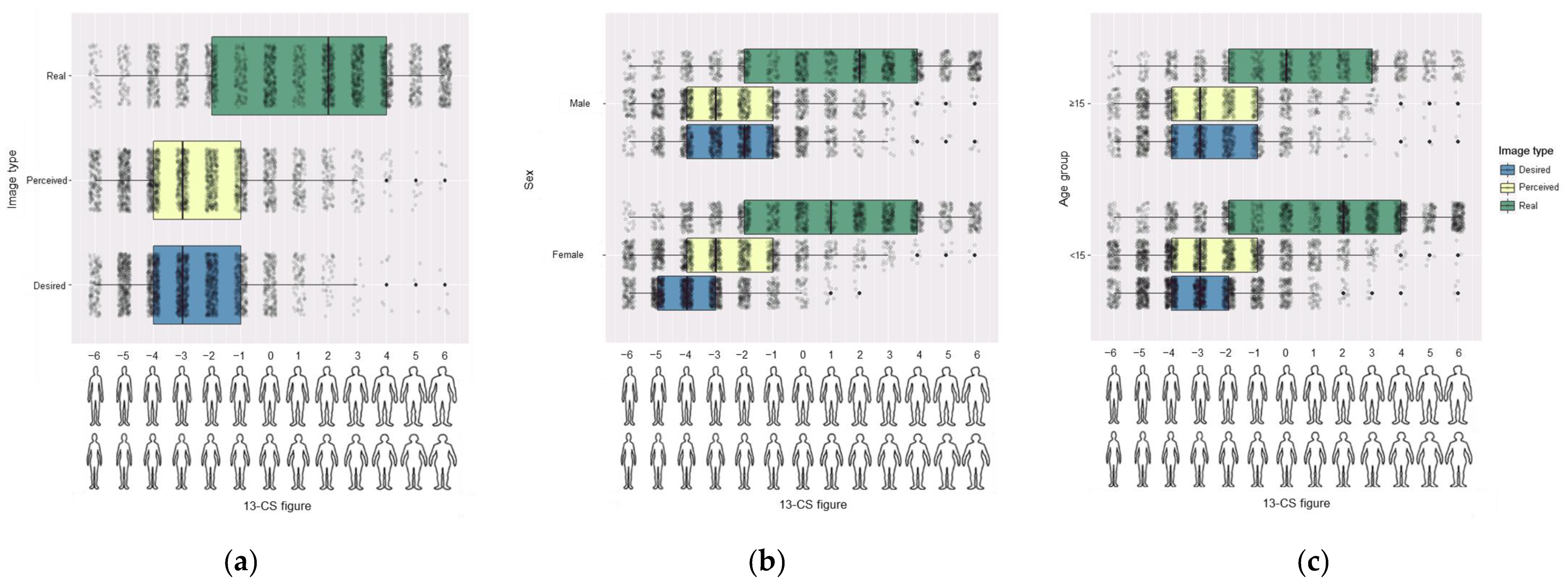
3.1. Perceptual Dimension
3.2. Cognitive-Affective Dimension
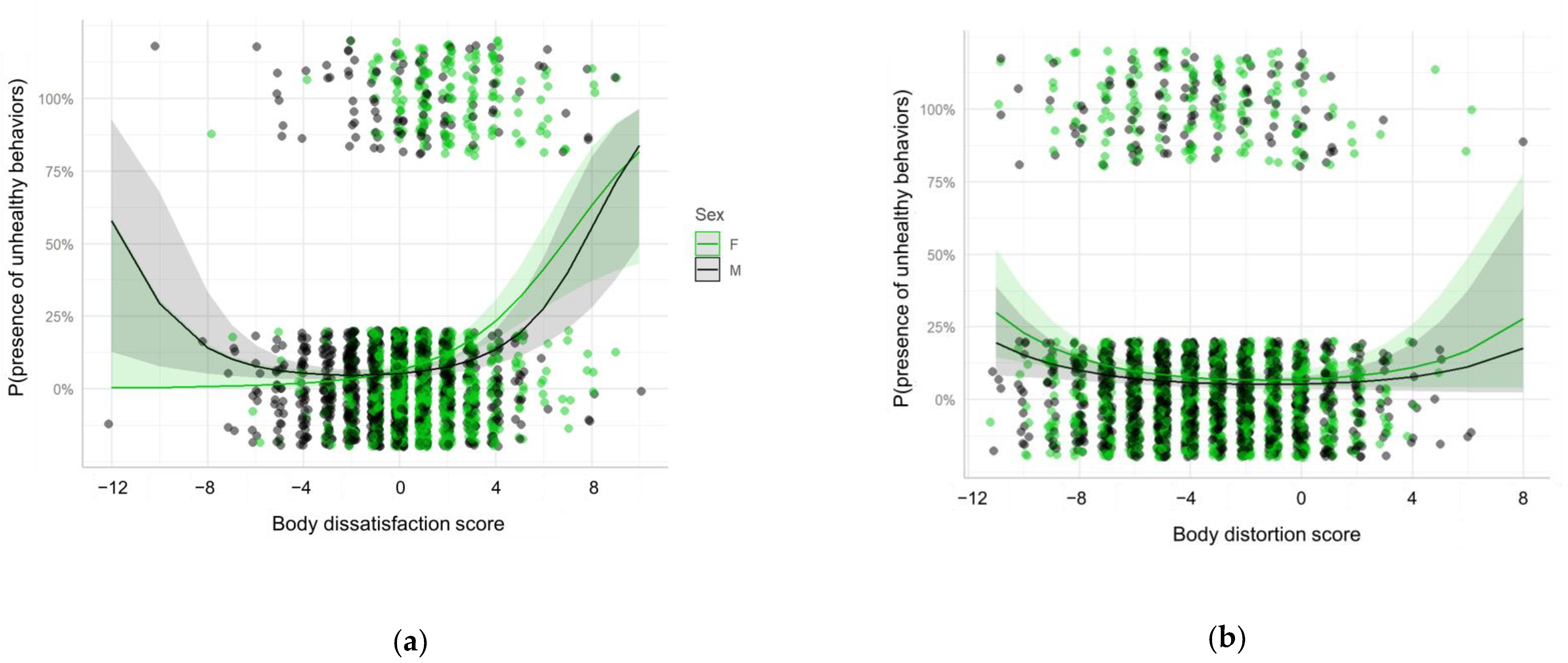
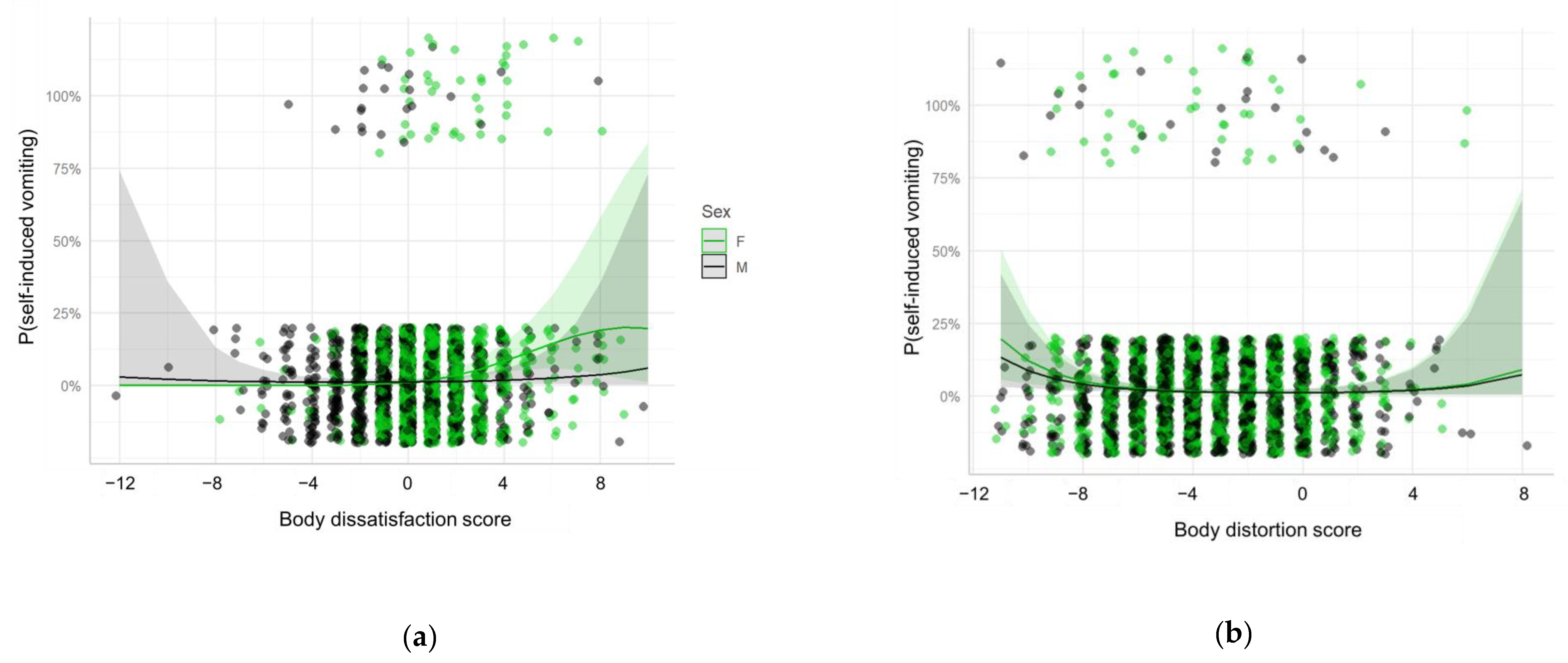
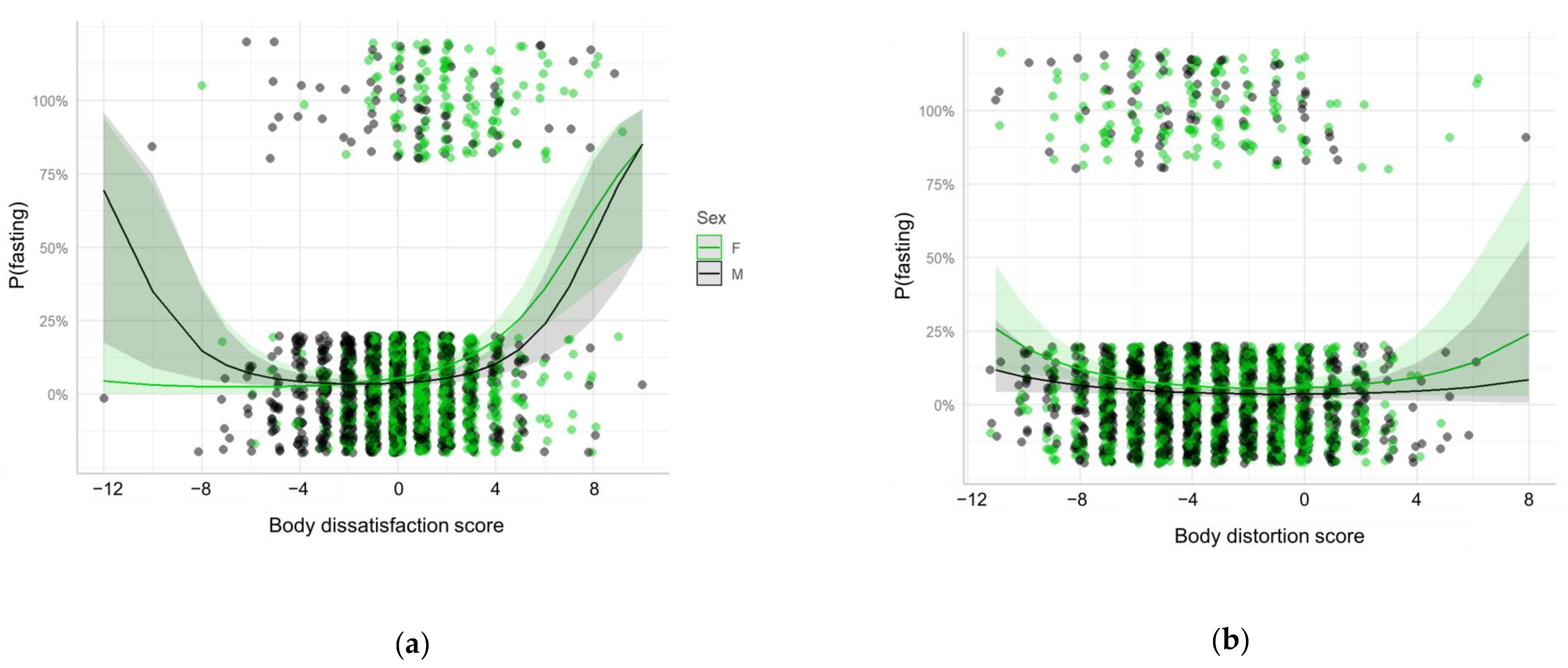
3.3. Behavioral Dimension
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Lleida: Aida Castelló Corretge, Alberto Seoane Barbosa, Ana Maria Castan Campanera, Antonieta Vidal Tolosa, Araceli Clemente Baules, Aranzazu Nieto Moreno, Blanca Aguarod Salillas, Carlos Gatius Tonda, Carmen Borbón Nadal, Clara Huguet Baldomà, Daniel Gros Esteban, Eduardo Delgado Roche, Elena Duque Navasa, Eva Camats Escoda, Eva Escola Acuña, Eva Maria Suárez Magaña, Gemma Martín Servet, Gemma Terrer Manrique, Iraida Gimeno Pi, Josep Ramon Marsal Mora, Keyko Sole Melero, Laura Seoane Barbosa, Lidia Carulla Canales, M. Montserrat Zaballos Hernandez, M. Antonia Clemente Mirón, Ma. Carmen Martin Anson, Magdalena Riera Veciana, Manuela Milla Ocaña, Maria Carmen Greoles Valls, Maria Isabel Garrido Santiago, Maria Pilar Aguarod Salillas, Maria Rosa Escriba Salvado, Meritxell Regany Rodriguez, Mireia Pascual Rebollo, Monica Roig Farrás, Natalia Bravo Andrés, Natalia Vall Faura, Patricia Aixalá Olivan, Rosa Blanca Guiu Badia, Silvia Ferraz Sopena, Silvia Prado Muñoz, Silvia Solís Vidal, Susana Pérez Osuna, Teresa Real Llovera, Yolanda Pascual Arrazola.
- Rural: Adelina Albana Mola, Albert Romero Gracia, Álvaro Vilela Pájaro, Ana Maria Parra Pérez, Anna Pagés Consul, Anna Pla Moro, Anna Ribé Miró, Anna Torné Cortés, Anna Torres Saladrigues, Annabel Areny Tallarí, Annabel Vidal Cupons, Carme Estela Abad, Carme Florensa Piró, Carme Juni Carnicer, Cristina Garcia Serrano, Cristina Cebrián Aiguadé, David Jordana Ariza, Dolors Segura Querol, Ester Mateus Solé, Estrella Lalueza Lafuente, Evelin Maria Manga Domínguez, Gemma Amat Camats, Gemma Planelles Font, Imma Nadal Creus, Inma Morales Bara, Joana García Hinojosa, Joana Gassó Jordán, Josep Mª Jimenez Ramos, Judit Mari Villagrassa, Laura Pallàs Martín, Lídia Sanz Borrell, Mª José Freixinet Ayala, Magda Barberà Farré, Magdalena Camí Capell, Maite Puig Solé, Mari Fe Quelle Alonso, Maria Belen Garriga Figueres, Maria Belen Mas Gardo, Maria Jesús Fernández Galán, Maria Teresa Ortiga Pifarré, Marta Farré Bergadà, Marta Pifarré Ortiz, Marta Puig Fitó, Mercè Bellmunt Bonet, Mercè Font Arbó, Mercè Lozano Vergara, Mercè Segura Serra, Meritxell Batlle Bosch, Meritxell Corrales Gomà, Mireia Biosca Pàmies, Mireia Villalta Martí, Míriam Duch Visart, Mª Carme Salgado Valle, Mª Carmen Martínez López, Mª José Lara Tostado, Mª Teresa Palou Solé, Mª José Estadella Servalls, Mònica Carbonell Badia, Mònica Guillen Mesalles, Mònica Martínez Mayoral, Montserrat Junyent Solé, Montserrat Vidal Ballesté, Neus Arola Serra, Neus Piqué Palacín, Núria Huguet Bea, Núria Serra Solans, Olivia Guasch Niubó, Patricia Ferreira Prat, Pilar Serra Solans, Raquel Plasència Atienza, Raúl Rodríguez Flores, Rita Sancho Borot, Rosa Company Marimon, Rosa Puigdemont Fortet, Sandra Farré Prunera, Sara Martí Martí, Sònia Sans Vollmer, Tere Carulla Fusté, Tere Pelegrí Pach, Teresa Guasch Clapés, Teresa Pujol Puyané, Victòria Ruiz Iglesias.
- Pirineus: Anna Llusà Parramon, Elena Alcover Bloch, Elisabeth Vila Mirabet, Ester Prat Gallart, Hilda Toscani Paris, Maria del Mar Mata Sáez, Montse Figueroa Piñol, Neus Calvelo Coronado, Núria Gardeñes Llorens, Núria Tomas Bea, Patricia Álvarez García.
References
- Unicef Nations Cildren’s Fund. The State of the World’s Children 2011: Adolescence—An Age of Opportunity; Division of Communication, UNICEF: New York, NY, USA, 2011. [Google Scholar]
- Parent, A.S.; Teilmann, G.; Juul, A.; Skakkebaek, N.E.; Toppari, J.; Bourguignon, J.P. The timing of normal puberty and the age limits of sexual precocity: Variations around the world, secular trends, and changes after migration. Endocr. Rev. 2003, 24, 668–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogol, A.D.; Roemmich, J.N.; Clark, P.A. Growth at puberty. J. Adolesc. Health 2002, 31, 192–200. [Google Scholar] [CrossRef]
- Rosenberg, M. Society and the Adolescent Self-Image; American Psychological Association: Washington, DC, USA, 1989. [Google Scholar]
- Pinheiro Mota, C.; Mena Matos, P. Parents, teachers and peers: Contributions to self-esteem and coping in adolescents. An. Psicol. 2014, 30, 656–666. [Google Scholar] [CrossRef]
- Cocca, A.; Blanco, J.R.; Peinado, J.E.; Viciana, J. Actual, social and ideal body image in Mexican adolescents and their relation with body dissatisfaction: Gender differences. Retos 2016, 30, 189–192. [Google Scholar] [CrossRef]
- Bjornsson, A.S.; Didie, E.R.; Grant, J.E.; Menard, W.; Stalker, E.; Phillips, K.A. Age at onset and clinical correlates in body dysmorphic disorder. Compr. Psychiatry 2013, 54, 893–903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5), 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Phillips, K.A.; Menard, W.; Fay, C.; Pagano, M.E. Psychosocial functioning and quality of life in body dysmorphic disorder. Compr. Psychiatry 2005, 46, 254–260. [Google Scholar] [CrossRef] [Green Version]
- Albertini, R.S.; Phillips, K.A. Thirty-Three cases of body dysmorphic disorder in children and adolescents. J. Am. Acad. Child. Adolesc. Psychiatry 1999, 38, 453–459. [Google Scholar] [CrossRef]
- Schneider, S.C.; Turner, C.M.; Mond, J.; Hudson, J.L. Prevalence and correlates of body dysmorphic disorder in a community sample of adolescents. Aust. N. Z. J. Psychiatry 2017, 51, 595–603. [Google Scholar] [CrossRef]
- Clay, D.; Vignoles, V.L.; Dittmar, H. Body image and self-esteem among adolescent girls: Testing the influence of sociocultural factors. J. Res. Adolesc. 2005, 15, 451–477. [Google Scholar] [CrossRef]
- Williamson, D.; Davis, C.; Duchman, E.; Watkin, P. Assessment of Eating Disorders: Obesity, Anorexia & Bulimia Nervosa; Pergamon Press: New York, NY, USA, 1990. [Google Scholar]
- Vitousek, K.B.; Hollon, S.D. The investigation of schematic content and processing in eating disorders. Special Issue: Selfhood processes and emotional disorders. Cogn. Ther. Res. 1990, 14, 191–214. [Google Scholar] [CrossRef]
- Ramos, P.; Moreno-Maldonado, C.; Moreno, C.; Rivera, F. The role of body image in internalizing mental health problems in spanish adolescents: An analysis according to sex, age, and socioeconomic status. Front. Psychol. 2019, 10, 1952. [Google Scholar] [CrossRef] [PubMed]
- Siemen, J.R.; Warrington, C.A.; Mangano, E.L. Comparison of the millon adolescent personality inventory and the suicide ideation questionnaire—Junior with an adolescent inpatient sample. Psychol. Rep. 1994, 75, 947–950. [Google Scholar] [CrossRef]
- Vaquero-Cristóbal, R.; Alacid, F.; Muyor, J.M.; López-Miñarro, P.Á. Imagen corporal: Revisión bibliográfica. Nutr. Hosp. 2013, 28, 27–35. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, M.; Dhawan, P. “But I am fat”: The experiences of weight dissatisfaction in Indian adolescent girls and young women. Womens Stud. Int. Forum 2011, 34, 539–549. [Google Scholar] [CrossRef]
- López-Guimerà, G.; Levine, M.P.; Sánchez-carracedo, D.; Fauquet, J. Influence of mass media on body image and eating disordered attitudes and behaviors in females: A review of effects and processes. Media Psychol. 2010, 13, 387–416. [Google Scholar] [CrossRef]
- Añez, E.; Fornieles-Deu, A.; Fauquet-Ars, J.; López-Guimerà, G.; Puntí-Vidal, J.; Sánchez-Carracedo, D. Body image dissatisfaction, physical activity and screen-time in Spanish adolescents. J. Health Psychol. 2018, 23, 36–47. [Google Scholar] [CrossRef] [Green Version]
- Holmqvist, K.; Frisén, A. “I bet they aren’t that perfect in reality” Appearance ideals viewed from the perspective of adolescents with a positive body image. Body Image 2012, 9, 388–395. [Google Scholar] [CrossRef] [Green Version]
- Heidelberger, L.; Smith, C. Low-Income, African American and American Indian children’s viewpoints on body image assessment tools and body satisfaction: A mixed methods study. Matern. Child Health J. 2018, 22, 1327–1338. [Google Scholar] [CrossRef]
- Holmqvist, K.; Frisén, A. From negative to positive body image: Men’s and women’s journeys from early adolescence to emerging adulthood. Body Image 2019, 28, 53–65. [Google Scholar] [CrossRef]
- Deschamps, V.; Salanave, B.; Chan-Chee, C.; Vernay, M.; Castetbon, K. Body-Weight perception and related preoccupations in a large national sample of adolescents. Pediatr. Obes. 2015, 10, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Hart, L.M.; Damiano, S.R.; Cornell, C.; Paxton, S.J. What parents know and want to learn about healthy eating and body image in preschool children: A triangulated qualitative study with parents and early childhood professionals. BMC Public Health 2015, 15, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, S.B.; Nagata, J.M.; Griffiths, S.; Calzo, J.P.; Brown, T.A.; Mitchison, D.; Blashill, A.J.; Mond, J.M. The enigma of male eating disorders: A critical review and synthesis. Clin. Psychol. Rev. 2017, 57, 1–11. [Google Scholar] [CrossRef]
- Loth, K.; Wall, M.; Larson, N.; Neumark-Sztainer, D. Disordered eating and psychological well-being in overweight and nonoverweight adolescents: Secular trends from 1999 to 2010. Int. J. Eat. Disord. 2015, 48, 323–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lenardson, J.D.; Hansen, A.Y.; Hartley, D. Rural and remote food environments and obesity. Curr. Obes. Rep. 2015, 4, 46–53. [Google Scholar] [CrossRef]
- Jiménez Boraita, R.; Arriscado Alsina, D.; Gargallo Ibort, E.; Dalmau Torres, J.M. Quality of life related to health and habits: Differences between adolescents in rural and urban environments. An. Pediatr. 2021. [Google Scholar] [CrossRef]
- Vander Wal, J.S. Unhealthy weight control behaviors among adolescents. J. Health Psychol. 2012, 17, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Martínez, N.B.; Escoto, C.; Bosques, L.E.; Ibarra, J.E.; Juárez Lugo, C.S. Internalization of aesthetic ideals and body concern in males and females gym users. Rev. Mex. Trastor. Aliment. 2014, 5, 29–38. [Google Scholar] [CrossRef] [Green Version]
- Golden, N.; Katzman, D.; Kreipe, R.; Stevens, S.; Sawyer, S.; Rees, J.; Nicholls, D.; Rome, E.S. Eating disorders in adolescentsposition paper of the Society for Adolescent Medicine. J. Adolesc. Health 2003, 33, 496–503. [Google Scholar] [CrossRef]
- Corominas, P.; Prats, R.; Coll, M. Health and School Program. Content and Implementation guide; Departament de Salut, Generalitat de Catalunya: Barcelona, Spain, 2008. [Google Scholar]
- Rodriguez Campayo, M.; Beato Fernández, L.; Rodriguez Cano, T.; Martínez-Sánchez, F. Spanish version of the Gardner body image validation scale in patients with eating behavior disorders. Actas Esp. Psiquiatr. 2003, 31, 59–64. [Google Scholar] [PubMed]
- De Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef]
- Cruz Sáez, M.; Pascual Jimeno, A.; Wlodarczyk, A.; Polo López, R.; Echeburúa Odriozola, E. Body dissatisfaction and weight control behaviors among overweight adolescent girls: Mediating role of anxiety and depression. Nutr. Hosp. 2016, 33, 935–940. [Google Scholar] [CrossRef] [Green Version]
- Feise, R.J. Do multiple outcome measures require p-value adjustment? BMC Med. Res. Methodol. 2002, 2, 1–4. [Google Scholar] [CrossRef] [Green Version]
- López-Guimerà, G.; Neumark-Sztainer, D.; Hannan, P.; Fauquet, J.; Loth, K.; Sánchez-Carracedo, D. Unhealthy weight-control behaviours, dieting and weight status: A cross-cultural comparison between North American and Spanish adolescents. Eur. Eat. Disord. Rev. 2013, 21, 276–283. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Sáez, S.; Pascual, A.; Salaberria, K.; Etxebarria, I.; Echeburúa, E. Risky eating behaviors and beliefs among adolescent girls. J. Health Psychol. 2015, 20, 154–163. [Google Scholar] [CrossRef] [PubMed]
- López Sánchez, G.F.; Suárez, A.D.; Smith, L. Analysis of body image and obesity by Stunkard’s silhouettes in 3- to 18-year-old Spanish children and adolescents. An. Psicol. 2018, 34, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Gómez Mármol, A.; Sánchez Alcaraz Martínez, B.; María del Pilar Mahedero, N. Insatisfacción y distorsión de la imagen corporal en adolescentes de doce a diecisiete años de edad. Ágora Educ. Fis. Deport. 2013, 15, 54–63. [Google Scholar]
- Ramos, P.; Pérez de Eulate, L.; Liberal, S.; Latorre, M. La imagen corporal en relación con los TCA en adolescentes vascos de 12 a 18 años. Rev. Psicodidact. 2003, 16, 65–73. [Google Scholar]
- Pocallet, M.P.; Ma, E.; Barberà, A.; Clapes, T.G.; Bonet, M.B.; Solé, T.P.; Solans, N.S.; Calvet, E.R.; Mora, J.; Bravo, M.O. Cross-Sectional study on body image and self-esteem among adolescents in Catalonia. Health Educ. Public Health 2019, 2, 164–169. [Google Scholar]
- Mazzurega, M.; Marisa, J.; Zampini, M.; Pavani, F. Thinner than yourself: Self-Serving bias in body size estimation. Psychol. Res. 2018, 84, 932–949. [Google Scholar] [CrossRef]
- Dey, R.; Clark, B.R.; Ackermann, N.; Racette, S.B. Weight status perception and weight loss intention among urban youth. Obes. Res. Clin. Pract. 2019, 13, 391–394. [Google Scholar] [CrossRef]
- Stephen, I.D.; Hunter, K.; Sturman, D.; Mond, J.; Stevenson, R.J.; Brooks, K.R. Experimental manipulation of visual attention affects body size adaptation but not body dissatisfaction. Int. J. Eat. Disord. 2019, 52, 79–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guadarrama Guadarrama, R.; Henández Navor, J.C.; Veytia López, M. “How do I perceive myself and how I would like to be”: A study on the body image of Mexican adolescents. Rev. Psicol. Clin. Niños Adolesc. 2018, 5, 37–43. [Google Scholar] [CrossRef]
- Ramos Valverde, P.; Rivera de los Santos, F.; Moreno Rodríguez, C. Diferencias de sexo en imagen corporal, control de peso e índice de masa corporal de los adolescentes españoles. Psicothema 2010, 22, 77–83. [Google Scholar] [PubMed]
- Strauss, R.S. Self-Reported weight status and dieting in a cross-sectional sample of young adolescents. Arch. Pediatr. Adolesc. Med. 1999, 153, 741. [Google Scholar] [CrossRef] [PubMed]
- Talamayan, K.S.; Springer, A.E.; Kelder, S.H.; Gorospe, E.C.; Joye, K.A. Prevalence of overweight misperception and weight control behaviors among normal weight adolescents in the United States. Sci. World J. 2006, 6, 365–373. [Google Scholar] [CrossRef] [Green Version]
- Corno, G.; Serino, S.; Cipresso, P.; Baños, R.M.; Riva, G. Assessing the relationship between attitudinal and perceptual component of body image disturbance using virtual reality. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Pope, H.; Phillips, K.; Olivardia, R. The Adonis Complex; Free Press: New York, NY, USA, 2002. [Google Scholar]
- Levine, M.; Smolak, L. Cultural influences on body image and eating disorders. In Oxford Handbook of Eating Disorders; Agras, W., Ed.; Oxford University Press: New York, NY, USA, 2010; p. 493. [Google Scholar]
- Meier, E.P.; Gray, J. Facebook photo activity associated with body image disturbance in adolescent girls. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 199–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiggemann, M.; Miller, J. The internet and adolescent girls’ weight satisfaction and drive for thinness. Sex Roles 2010, 63, 79–90. [Google Scholar] [CrossRef]
- Calado, M.; Lameiras, M.; Sepulveda, A.R.; Rodriguez, Y.; Carrera, M.V. The association between exposure to mass media and body dissatisfaction among spanish adolescents. Womens Health Issues 2011, 21, 390–399. [Google Scholar] [CrossRef]
- Fardouly, J.; Vartanian, L. Negative comparisons about one’s appearance mediate the relationship between Facebook usage and body image concerns. Body Image 2015, 12, 82–88. [Google Scholar] [CrossRef]
- Ramos Vidal, I. The role of relationships and life satisfaction on body image perceptual disturbance in a sample of Mexican students. Arch. Med. 2019, 19, 111–123. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Education. Royal Decree 132/2010, from February 12th, Establishing the Minimum Requirements of the Centers that Teach the Second Cycle of Childhood Education, Primary Education and Secondary Education; Ministry of Education: Madrid, Spain, 2010.
- Chapuis-de-Andrade, S.; de Araujo, R.M.; Lara, D.R. Association of weight control behaviors with body mass index and weight-based self-evaluation. Rev. Bras. Psiquiatr. 2017, 39, 237–243. [Google Scholar] [CrossRef] [Green Version]
- Stice, E.; Davis, K.; Miller, N.P.; Marti, C.N. Fasting increases risk for onset of binge eating and bulimic pathology: A 5-year prospective study. J. Abnorm. Psychol. 2008, 117, 941–946. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, K.M.; Whelan, D.R.; Sandler, D.P.; Hall, J.E.; Weinberg, C.R. Predictors and long-term health outcomes of eating disorders. PLoS ONE 2017, 12, e0181104. [Google Scholar] [CrossRef] [Green Version]
- Smink, F.R.E.; Van Hoeken, D.; Hoek, H.W. Epidemiology, course, and outcome of eating disorders. Curr. Opin. Psychiatry 2013, 26, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Raevuori, A.; Keski-Rahkonen, A.; Hoek, H.W. A review of eating disorders in males. Curr. Opin. Psychiatry 2014, 27, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Marti, C.N.; Rohde, P. Prevalence, incidence, impairment, and course of the proposed DSM-5 eating disorder diagnoses in an 8-year prospective community study of young women. J. Abnorm. Psychol. 2013, 122, 445–457. [Google Scholar] [CrossRef] [Green Version]
- Calado, M.; Lameiras, M.; Sepulveda, A.R.; Rodríguez, Y.; Carrera, M.V. The mass media exposure and disordered eating behaviours in Spanish secondary students. Eur. Eat. Disord. Rev. 2010, 18, 417–427. [Google Scholar] [CrossRef]
- Essau, C.A.; Lewinsohn, P.M.; Lim, J.X.; Ho, M.R.; Rohde, P. Incidence, recurrence and comorbidity of anxiety disorders in four major developmental stages. J. Affect. Disord. 2018, 228, 248–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burcusa, S.L.; Iacono, W.G. Risk for recurrence in depression. Clin. Psychol. Rev. 2007, 27, 959–985. [Google Scholar] [CrossRef] [Green Version]
- Bertha, E.A.; Balázs, J. Subthreshold depression in adolescence: A systematic review. Eur. Child Adolesc. Psychiatry 2013, 22, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Tort-Nasarre, G.; Pollina Pocallet, M.; Artigues-Barberà, E. The meaning and factors that influence the concept of body image: Systematic review and meta-ethnography from the perspectives of adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1140. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | All Participants (n = 2496) |
|---|---|
| Age, mean (SD) | 14.1 (1.61) |
| Age group, n (%) | |
| <15 | 1593 (63.8%) |
| ≥15 | 903 (36.2%) |
| Sex, n (%) | |
| Female | 1278 (51.2%) |
| Male | 1218 (48.8%) |
| Body Mass Index z-score, mean (SD) | 0.31 (1.02) |
| Item | All Participants (n = 2496) | Female (n = 1278) | Male (n = 1218) | p-Value (Male vs Female) | <15 (n = 1593) | ≥15 (n = 903) | p-Value (<15 vs ≥15) |
|---|---|---|---|---|---|---|---|
| Perceptual dimension | |||||||
| Real image (n = 2496) | 1.05 (3.64) * | 0.82 (3.58) * | 1.30 (3.68) * | <0.001 | 1.35 (3.71) * | 0.52 (3.45) * | <0.001 |
| Perceived image (n = 2474) | −2.42 (2.42) * | −2.61 (2.37) * | −2.22 (2.47) * | <0.001 | −2.42 (2.42) * | −2.42 (2.43) * | 0.834 |
| Body distortion score (n = 2474) | −3.47 (2.92) * | −3.41 (2.88) * | −3.53 (2.97) * | 0.161 | −3.77 (3.00) * | −2.94 (2.71) * | <0.001 |
| Cognitive-affective dimension | |||||||
| Desired image (n = 2473) | −2.79 (2.01) * | −3.57 (1.60) * | −1.98 (2.07) * | <0.001 | −2.86 (1.95) * | −2.67 (2.10) * | 0.053 |
| Body dissatisfaction score (n = 2473) | 0.37 (2.22) * | 0.96 (1.90) * | −0.25 (2.35) * | <0.001 | 0.44 (2.26) * | 0.25 (2.13) * | 0.021 |
| Behavioral dimension | |||||||
| Presence of unhealthy behavior (n = 2484) | 257 (10.3%) | 160 (12.6%) | 97 (7.98%) | <0.001 | 161 (10.1%) | 96 (10.7%) | 0.712 |
| Self-induced vomiting (n = 2489) | 65 (2.61%) | 43 (3.38%) | 22 (1.81%) | 0.020 | 43 (2.70%) | 22 (2.45%) | 0.803 |
| Laxatives intake (n = 2490) | 23 (0.92%) | 11 (0.86%) | 12 (0.99%) | 0.914 | 17 (1.07%) | 6 (0.67%) | 0.429 |
| Diuretics intake (n = 2488) | 11 (0.44%) | 6 (0.47%) | 5 (0.41%) | 1.000 | 10 (0.63%) | 1 (0.11%) | 0.111 |
| Weight loss pills intake (n = 2492) | 11 (0.44%) | 7 (0.55%) | 4 (0.33%) | 0.598 | 8 (0.50%) | 3 (0.33%) | 0.756 |
| Fasting (n = 2491) | 205 (8.23%) | 135 (10.6%) | 70 (5.75%) | <0.001 | 122 (7.67%) | 83 (9.22%) | 0.201 |
| Variable | Presence of UWCB | Self-Induced Vomiting | Fasting | |||
|---|---|---|---|---|---|---|
| Predictor | aOR (95% CI) | p-value | aOR (95% CI) | p-value | aOR (95% CI) | p-value |
| Age | 1.070 (0.979–1.170) | 0.136 | 0.977 (0.825–1.148) | 0.780 | 1.154 (1.048–1.269) | 0.003 |
| Sex (Male) | 0.808 (0.476–1.371) | 0.430 | 1.233 (0.453–3.389) | 0.681 | 0.632 (0.338–1.157) | 0.142 |
| Body dissatisfaction (linear component) | 1.406 (1.174–1.682) | <0.001 | 1.965 (1.352–3.021) | 0.001 | 1.291 (1.101–1.565) | 0.005 |
| Body dissatisfaction (quadratic component) | 1.008 (0.979–1.037) | 0.605 | 0.964 (0.905–1.015) | 0.209 | 1.020 (0.991–1.046) | 0.155 |
| Body distortion (linear component) | 1.056 (0.919–1.212) | 0.443 | 1.041 (0.837–1.276) | 0.709 | 1.056 (0.907–1.224) | 0.471 |
| Body distortion (quadratic component) | 1.019 (1.004–1.035) | 0.016 | 1.029 (1.006–1.052) | 0.009 | 1.019 (1.002–1.036) | 0.024 |
| Sex (Male): Body dissatisfaction (linear component) | 0.804 (0.669–0.967) | 0.021 | 0.538 (0.345–0.797) | 0.004 | 0.868 (0.713–1.029) | 0.132 |
| Sex (Male): Body dissatisfaction (quadratic component) | 1.025 (0.994–1.058) | 0.119 | 1.048 (0.984–1.122) | 0.154 | 1.018 (0.989–1.052) | 0.249 |
| Sex (Male): Body distortion (linear component) | 0.991 (0.829–1.184) | 0.918 | 1.000 (0.772–1.278) | 0.998 | 0.968 (0.790–1.182) | 0.750 |
| Sex (Male): Body distortion (quadratic component) | 0.997 (0.975–1.019) | 0.781 | 0.996 (0.965–1.028) | 0.815 | 0.993 (0.969–1.018) | 0.592 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pollina-Pocallet, M.; Artigues-Barberà, E.; Tort-Nasarre, G.; Sol, J.; Azlor, L.; Foguet-Boreu, Q.; Ortega-Bravo, M. Self-Perception and Self-Acceptance Are Related to Unhealthy Weight Control Behaviors in Catalan Adolescents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 4976. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094976
Pollina-Pocallet M, Artigues-Barberà E, Tort-Nasarre G, Sol J, Azlor L, Foguet-Boreu Q, Ortega-Bravo M. Self-Perception and Self-Acceptance Are Related to Unhealthy Weight Control Behaviors in Catalan Adolescents: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(9):4976. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094976
Chicago/Turabian StylePollina-Pocallet, Mercè, Eva Artigues-Barberà, Glòria Tort-Nasarre, Joaquim Sol, Laura Azlor, Quintí Foguet-Boreu, and Marta Ortega-Bravo. 2021. "Self-Perception and Self-Acceptance Are Related to Unhealthy Weight Control Behaviors in Catalan Adolescents: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 9: 4976. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094976