
Abdominal Aortic Screening Is a Priority for Health in Smoker Males: A Study on Central Italian Population

Abstract
:1. Introduction
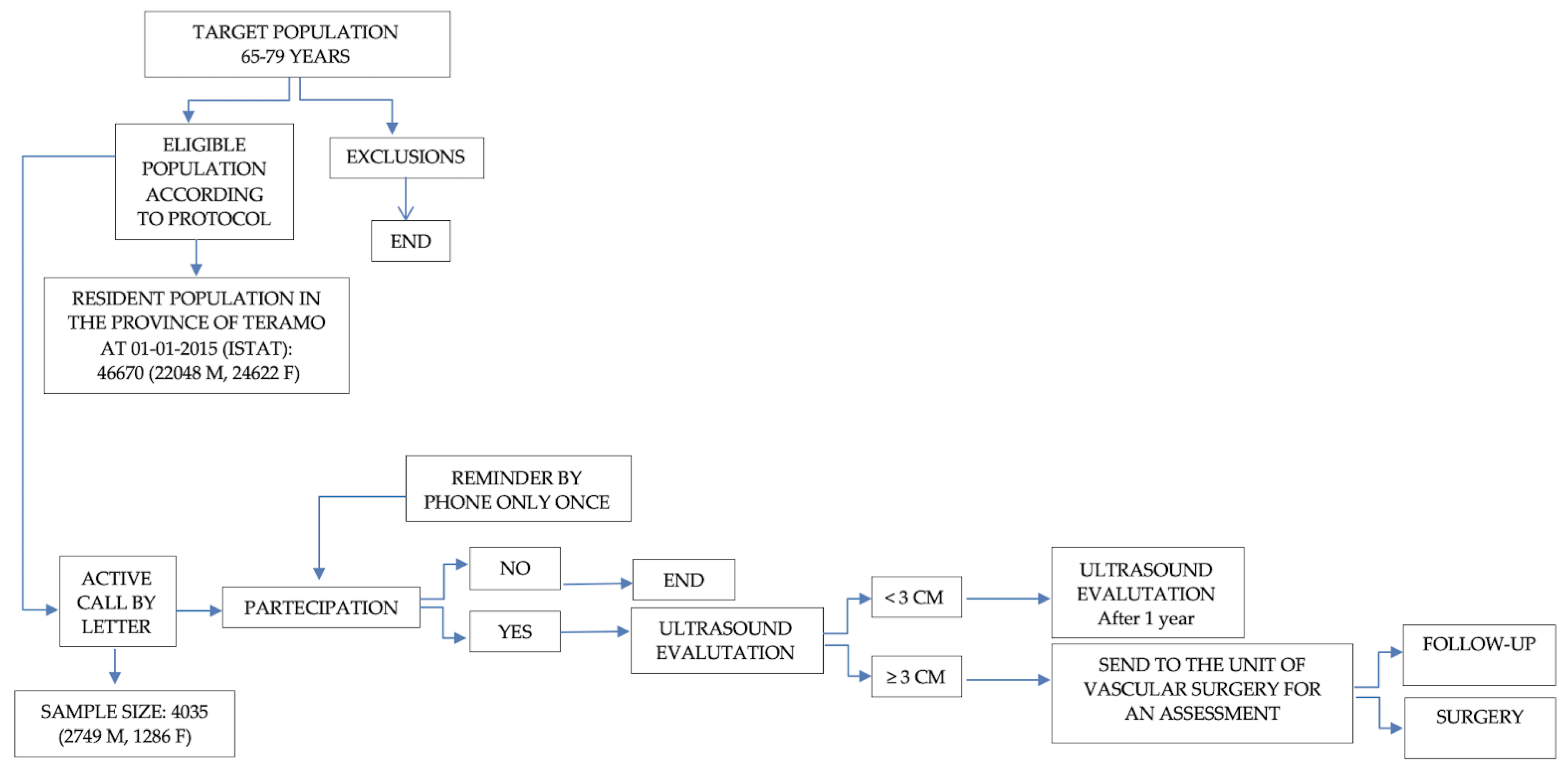
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AAA | Abdominal aortic aneurysm |
| DRG | disease related group |
| EVAR | Endovascular aneurysms repair |
References
- Moll, F.L.; Powell, J.T.; Fraedrich, G.; Verzini, F.; Haulon, S.; Waltham, M.; van Herwaarden, J.A.; Holt, P.J.E.; van Keulen, J.W.; Rantner, B.; et al. Management of Abdominal Aortic Aneurysms Clinical Practice Guidelines of the European Society for Vascular Surgery. Eur. J. Vasc. Endovasc. Surg. 2011, 41 (Suppl. 1), S1–S58. [Google Scholar] [CrossRef] [Green Version]
- Jongkind, V.; Yeung, K.K.; Akkersdijk, G.J.; Heidsieck, D.; Reitsma, J.B.; Tangelder, G.J.; Wisselink, W. Juxtarenal aortic aneurysm repair. J. Vasc. Surg. 2010, 52, 760–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindholt, J.S.; Juul, S.; Fasting, H.; Henneberg, E.W. Screening for abdominal aortic aneurysms: Single centre randomised controlled trial. BMJ 2005, 330, 750. [Google Scholar] [CrossRef] [Green Version]
- McCaul, K.A.; Lawrence-Brown, M.; Dickinson, J.A.; Norman, P.E. Long-term Outcomes of the Western Australian Trial of Screening for Abdominal Aortic Aneurysms: Secondary Analysis of a Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Benson, R.A.; Poole, R.; Murray, S.; Moxey, P.; Loftus, I.M. Screening results from a large United Kingdom abdominal aortic aneurysm screening center in the context of optimizing United Kingdom National Abdominal Aortic Aneurysm Screening Programme protocols. J. Vasc. Surg. 2016, 63, 301–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grøndal, N.; Søgaard, R.; Lindholt, J. Baseline prevalence of abdominal aortic aneurysm, peripheral arterial disease and hypertension in men aged 65–74 years from a population screening study (VIVA trial). BJS 2015, 102, 902–906. [Google Scholar] [CrossRef]
- Parkinson, F.; Ferguson, S.; Lewis, P.; Williams, I.M.; Twine, C.P. Rupture rates of untreated large abdominal aortic aneurysms in patients unfit for elective repair. J. Vasc. Surg. 2015, 61, 1606–1612. [Google Scholar] [CrossRef] [Green Version]
- Kniemeyer, H.; Kessler, T.; Reber, P.; Ris, H.; Hakki, H.; Widmer, M. Treatment of Ruptured Abdominal Aortic Aneurysm, a Permanent Challenge or a Waste of Resources? Prediction of Outcome Using a Multi-organ-dysfunction Score. Eur. J. Vasc. Endovasc. Surg. 2000, 19, 190–196. [Google Scholar] [CrossRef] [Green Version]
- Fleming, C.; Whitlock, E.P.; Beil, T.L.; Lederle, F.A. Screening for Abdominal Aortic Aneurysm: A Best-Evidence Systematic Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2005, 142, 203–211. [Google Scholar] [CrossRef] [Green Version]
- Dimick, J.B.; Cowan, J.A., Jr.; Stanley, J.C.; Henke, P.K.; Pronovost, P.J.; Upchurch, G.R., Jr. Surgeon specialty and provider volumes are related to outcome of intact abdominal aortic aneurysm repair in the United States. J. Vasc. Surg. 2003, 38, 739–744. [Google Scholar] [CrossRef] [Green Version]
- Guirguis-Blake, J.M.; Beil, T.L.; Senger, C.A.; Whitlock, E.P. Ultrasonography Screening for Abdominal Aortic Aneurysms: A Systematic Evidence Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2014, 160, 321–329. [Google Scholar] [CrossRef] [Green Version]
- Corrado, G.; Durante, A.; Genchi, V.; Trabattoni, L.; Beretta, S.; Rovelli, E.; Foglia-Manzillo, G.; Ferrari, G. Prevalence of previously undiagnosed abdominal aortic aneurysms in the area of Como: The ComoCuore “looking for AAA” ultrasonography screening. Int. J. Cardiovasc. Imaging 2016, 32, 1213–1217. [Google Scholar] [CrossRef]
- Shaker, A.A.; Khairy, H.M.; Elkaffas, K.H.; Ghanem, A.A. Frequency of abdominal aortic aneurysm in persons who have been examined with ultrasound at Kasr Al-Ainy Hospitals: A single center pilot study. Acta Angiol. 2019, 25, 133–139. [Google Scholar] [CrossRef]
- Pujades-Rodriguez, M.; George, J.; Shah, A.D.; Rapsomaniki, E.; Denaxas, S.; West, R.; Smeeth, L.; Timmis, A.; Hemingway, H. Heterogeneous associations between smoking and a wide range of initial presentations of cardiovascular disease in 1 937 360 people in England: Lifetime risks and implications for risk prediction. Int. J. Epidemiol. 2015, 44, 129–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazquez, C.; Sakalihasan, N.; D’Harcour, J.-B.; Limet, R. Routine Ultrasound Screening for Abdominal Aortic Aneurysm among 65- and 75-Year-Old Men in a City of 200,000 Inhabitants. Ann. Vasc. Surg. 1998, 12, 544–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gianfagna, F.; Veronesi, G.; Tozzi, M.; Tarallo, A.; Borchini, R.; Ferrario, M.M.; Bertù, L.; Montonati, A.; Castelli, P.; Mara, L.; et al. Prevalence of Abdominal Aortic Aneurysms in the General Population and in Subgroups at High Cardiovascular Risk in Italy. Results of the RoCAV Population Based Study. Eur. J. Vasc. Endovasc. Surg. 2018, 55, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Cornuz, J.; Pinto, C.S.; Tevaearai, H.; Egger, M. Risk factors for asymptomatic abdominal aortic aneurysm: Systematic review and meta-analysis of population-based screening studies. Eur. J. Public Health 2004, 14, 343–349. [Google Scholar] [CrossRef] [Green Version]
- Altobelli, E.; Rapacchietta, L.; Profeta, V.F.; Fagnano, R. Risk Factors for Abdominal Aortic Aneurysm in Population-Based Studies: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, M.U.; Fitzpatrick-Lewis, D.; Kenny, M.; Miller, J.; Raina, P.; Sherifali, D. A systematic review of short-term vs long-term effectiveness of one-time abdominal aortic aneurysm screening in men with ultrasound. J. Vasc. Surg. 2018, 68, 612–623. [Google Scholar] [CrossRef] [PubMed]
- A Benson, R.; Meecham, L.; Fisher, O.; Loftus, I.M. Ultrasound screening for abdominal aortic aneurysm: Current practice, challenges and controversies. Br. J. Radiol. 2018, 91, 20170306. [Google Scholar] [CrossRef] [PubMed]
- Bollettino Ufficiale Regione Abruzzo, Decreto Tariffe Ospedaliere. Available online: https://www.regione.abruzzo.it/system/files/dgr/2017/DGR305_2017.pdf (accessed on 22 October 2021).
- Altobelli, E.; Rapacchietta, L.; Angeletti, P.M.; Barbante, L.; Profeta, F.V.; Fagnano, R. Breast Cancer Screening Programmes across the WHO European Region: Differences among Countries Based on National Income Level. Int. J. Environ. Res. Public Health 2017, 14, 452. [Google Scholar] [CrossRef]
- Altobelli, E.; Rapacchietta, L.; Marziliano, C.; Campagna, G.; Profeta, V.F.; Fagnano, R. Differences in colorectal cancer surveillance epidemiology and screening in the WHO European Region. Oncol. Lett. 2018, 17, 2531–2542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altobelli, E.; Rapacchietta, L.; Profeta, F.V.; Fagnano, R. HPV-vaccination and cancer cervical screening in 53 WHO European Countries: An update on prevention programs according to income level. Cancer Med. 2019, 8, 2524–2534. [Google Scholar] [CrossRef]
- NHS Overview Abdominal Aortic Screening. Available online: https://www.nhs.uk/conditions/abdominal-aortic-aneurysm-screening/ (accessed on 1 November 2021).
- Carnevale, M.L.; Koleilat, I.; Lipsitz, E.C.; Friedmann, P.; Indes, J.E. Extended screening guidelines for the diagnosis of abdominal aortic aneurysm. J. Vasc. Surg. 2020, 72, 1917–1926. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, M.; Thompson, S.G.; Brown, L.C.; Powell, J.T. Meta-analysis of individual patient data to examine factors affecting growth and rupture of small abdominal aortic aneurysms. Br. J. Surg. 2012, 99, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Schmitz-Rixen, T.; Keese, M.; Hakimi, M.; Peters, A.; Böckler, D.; Nelson, K.; Grundmann, R.T. Ruptured abdominal aortic aneurysm—epidemiology, predisposing factors, and biology. Langenbecks Arch. Für Chir. 2016, 401, 275–288. [Google Scholar] [CrossRef]
- Sampilvanjil, A.; Karasawa, T.; Yamada, N.; Komada, T.; Higashi, T.; Baatarjav, C.; Watanabe, S.; Kamata, R.; Ohno, N.; Takahashi, M. Cigarette smoke extract induces ferroptosis in vascular smooth muscle cells. Am. J. Physiol. Circ. Physiol. 2020, 318, H508–H518. [Google Scholar] [CrossRef]
- Anzai, T. Inflammatory Mechanisms of Cardiovascular Remodeling. Circ. J. 2018, 82, 629–635. [Google Scholar] [CrossRef] [Green Version]
- Cochrane, A.L. Effectiveness and Efficiency: Random Reflections on Health Services; Nuffield Provincial Hospitals Trust: London, UK, 1972. [Google Scholar]
- Giardina, S.; Pane, B.; Spinella, G.; Cafueri, G.; Corbo, M.; Brasseur, P.; Orengo, G.; Palombo, D. An economic evaluation of an abdominal aortic aneurysm screening program in Italy. J. Vasc. Surg. 2011, 54, 938–946. [Google Scholar] [CrossRef] [Green Version]
- Ying, A.J.; Affan, E.T. Abdominal Aortic Aneurysm Screening: A Systematic Review and Meta-analysis of Efficacy and Cost. Ann. Vasc. Surg. 2019, 54, 298–303. [Google Scholar] [CrossRef]
- Agenzia Nazionale per i Servizi Sanitari Regionali (AGENAS), Piano Nazionale Esiti. Available online: https://pne.agenas.it/ (accessed on 22 October 2021).
- Ashton, H.A.; Buxton, M.; Day, N.E.; Kim, L.G.; Marteau, T.M.; Scott, R.A.; Thompson, S.G.; Walker, N.M.; Multicentre Aneurysm Screening Study Group. The Multicentre Aneurysm Screening Study (MASS) into the effect of abdominal aortic aneurysm screening on mortality in men: A randomised controlled trial. Lancet 2002, 360, 1531–1539. [Google Scholar] [PubMed]
- Nair, N.; Kvizhinadze, G.; Jones, G.T.; Rush, R.; Khashram, M.; Roake, J.; Blakely, A. Health gains, costs and cost-effectiveness of a population-based screening programme for abdominal aortic aneurysms. BJS 2019, 106, 1043–1054. [Google Scholar] [CrossRef] [PubMed]
- Wild, J.; Stather, P.; Biancari, F.; Choke, E.; Earnshaw, J.; Grant, S.; Hafez, H.; Holdsworth, R.; Juvonen, T.; Lindholt, J.; et al. A Multicentre Observational Study of the Outcomes of Screening Detected Sub-aneurysmal Aortic Dilatation. Eur. J. Vasc. Endovasc. Surg. 2013, 45, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altobelli, E.; Angeletti, P.M.; Rapacchietta, L.; Petrocelli, R. Overview of meta-analyses: The impact of dietary lifestyle on stroke risk. Int. J. Environ. Res. Public Health 2019, 16, 3582. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
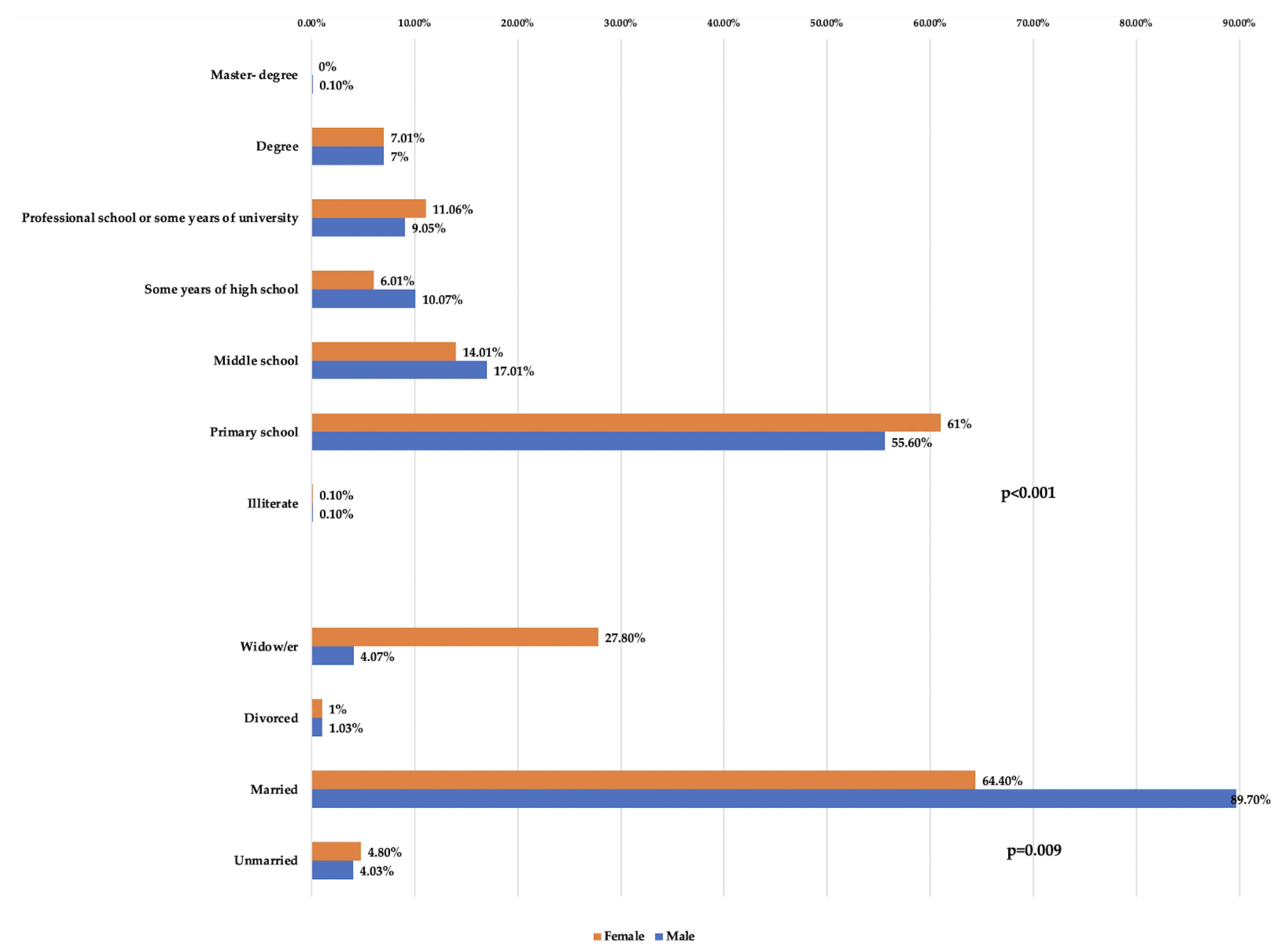
| Variables | Responders | Gender | ||
|---|---|---|---|---|
| No. (%) Males | No. (%) Females | p-Values | ||
| Marital status | <0.000 Χ2 = 263.4 | |||
| Unmarried | 92 | 59 (4.3) | 33 (4.8) | |
| Married | 1684 | 1241 (89.7) | 443 (64.4) | |
| Divorced | 27 | 20 (1.3) | 7 (1.0) | |
| Widow/er | 268 | 63 (4.7) | 205 (27.8) | |
| Total responders | 2071 | 1383 | 688 | |
| Education | 0.009 Χ2 = 18.7 | |||
| Illiterate | 3 | 2 (0.1) | 1 (0.1) | |
| Primary school | 1188 | 769 (55.6) | 419 (61.0) | |
| Middle school | 333 | 236 (17.1) | 97 (14.1) | |
| Some years of high school | 190 | 148 (10.7) | 42 (6.1) | |
| Professional school or some years of university | 211 | 131 (9.5) | 80 (11.6) | |
| Degree | 146 | 97 (7.0) | 49 (7.1) | |
| Master’s degree | 1 | 1 (0.1) | 0 (0.0) | |
| Total responders | 2072 | 1384 | 688 | |
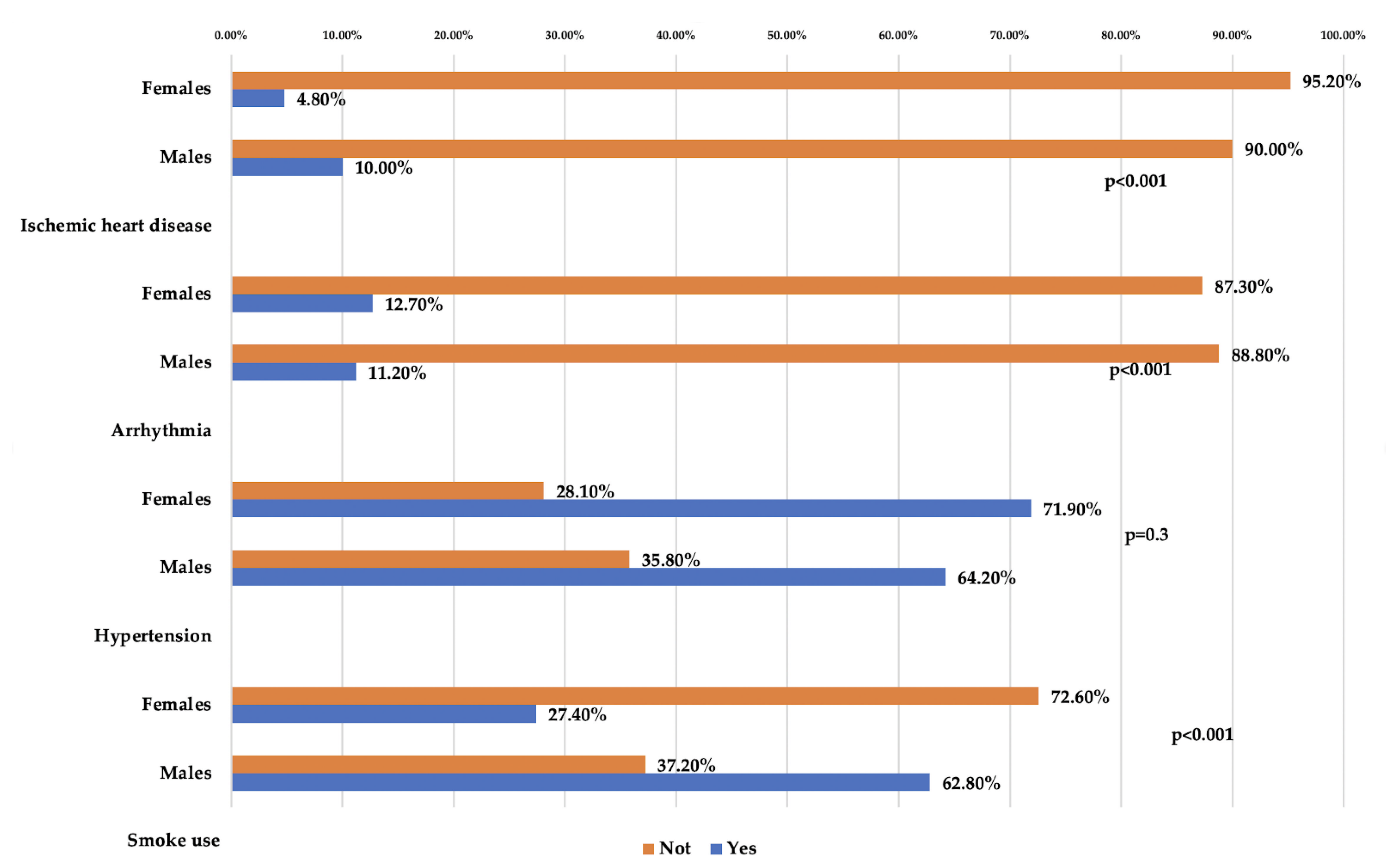
| Gender | Responders | No. (%) Yes | No. (%) Not | p-Values |
|---|---|---|---|---|
| Smoke Use | ||||
| Males | 1523 | 956 (62.8) | 567 (37.2) | <0.000 Χ2 = 256.7 |
| Females | 771 | 211 (27.4) | 560 (72.6) | |
| Total responders | 2294 | 1167 | 1127 | |
| Hypertension | ||||
| No. (%) Yes | No. (%) Not | <0.000 Χ2 = 12.3 | ||
| Males | 1380 | 886 (64.2) | 494 (35.8) | |
| Females | 684 | 492 (71.9) | 192 (28.1) | |
| Total responders | 2064 | 1378 | 686 | |
| Arrhythmia | 0.3 Χ2 = 1.1 | |||
| No. (%) Yes | No. (%) Not | |||
| Males | 1378 | 154 (11.2) | 1224 (88.8) | |
| Females | 684 | 87 (12.7) | 597 (87.3) | |
| Total responders | 2062 | 241 | 1821 | |
| Ischemic heart disease | <0.000 Χ2 = 16.2 | |||
| No. (%) Yes | No. (%) Not | |||
| Males | 1379 | 138 (10.0) | 1241 (90.0) | |
| Females | 684 | 33 (4.8) | 651 (95.2) | |
| Total responders | 2063 | 171 | 1892 | |
| Gender and Abdominal Aortic Diameter | ||||
| Diameter | ||||
| Gender | No. (%) < 3 cm | No. (%) ≥ 3 cm | Total | Χ2 = 18.6 p ≤ 0.000 OR: 5.94 (2.37–14.88) |
| Males | 1472 (96.3) | 57 (3.7) | 1529 | |
| Females | 767 (99.4) | 5 (0.6) | 772 | |
| Total | 2239 | 62 | 2301 | |
| Current smokers or former smokers (≥10 cigarettes/day) | ||||
| Diameter | ||||
| Smoke use | No. (%) < 3 cm | No. (%) ≥ 3 cm | Total | Χ2 = 27.8 p ≤ 0.000 OR: 5.21 (2.63–10.30) |
| Yes | 1115 (95.5) | 52 (4.5) | 1167 | |
| Not | 1117 (99.1) | 10 (0.9) | 1127 | |
| Total responders | 2232 | 62 | 2294 | |
| Cardiac arrhythmia and abdominal aortic diameter | ||||
| Diameter | ||||
| Arhythmia | No. (%) < 3 cm | No. (%) ≥ 3 cm | Total | Χ2 = 12.8 p ≤ 0.000 OR: 2.81 (1.53–5.15) |
| Yes | 226 (93.8) | 15 (6.2) | 241 | |
| Not | 1779 (99.1) | 42 (2.3) | 1821 | |
| Total responders | 2005 | 57 | 2062 | |
| Ischemic heart disease and abdominal aortic diameter | ||||
| Diameter | ||||
| Ischemic heart disease | No. (%) < 3 cm | No. (%) ≥ 3 cm | Total | Χ2 = 27.8 p = 0.006 OR: 2.76 (1.40–5.43) |
| Yes | 160 (96.3) | 11 (6.4) | 171 | |
| Not | 1846 (97.6) | 46 (2.4) | 1892 | |
| Total responders | 2006 | 57 | 2063 | |
| Hypertension and abdominal aortic diameter | ||||
| Diameter | ||||
| Hypertension | No. (%) < 3 cm | No. (%) ≥ 3 cm | Total | Χ2 = 2.1 p = 0.149 OR: 0.68 (0.40–1.15) |
| Yes | 1345 (97.6) | 33 (2.4) | 1378 | |
| Not | 662 (96.5) | 24 (3.5) | 686 | |
| Total responders | 2007 | 57 | ||
| Emergency | Planned | Costs of Emergency Euro | Costs Planned Euro | Screening Coasts/Year Euro | Ratio Emergency/ Planned | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Evar | Open | TOT | Costs Drg 110 Euro | Evar | Open | Tot | Costs DRG 111 Euro | |||||
| 2014 | 4 | 16 | 20 | 13,874.36 | 16 | 10,253.09 | 277,487.20 | 164,049.44 | Inactive screening | 1.69 | ||
| 2015 | 2 | 4 | 6 | 21 | 83,246.16 | 215,314.89 | 14,726.40 | 0.39 | ||||
| 2016 | 2 | 8 | 10 | 20 | 138,743.60 | 205,061.80 | 14,726.40 | 0.68 | ||||
| 2017 | 1 | 0 | 1 | 12 | 7 | 19 | 13,874.36 | 194,808.71 | 14,726.40 | 0.07 | ||
| 2018 | 0 | 0 | 0 | 8 | 3 | 11 | - | 112,783.99 | 14,726.40 | 0.00 | ||
| 2019 | 2 | 0 | 2 | 6 | 1 | 7 | 27,748.72 | 71,771.63 | 14,726.40 | 0.39 | ||
| 541,100.04 | 963,790.46 | 73,632.00 | 0.56 | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Altobelli, E.; Gianfelice, F.; Angeletti, P.M.; Petrocelli, R. Abdominal Aortic Screening Is a Priority for Health in Smoker Males: A Study on Central Italian Population. Int. J. Environ. Res. Public Health 2022, 19, 591. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010591
Altobelli E, Gianfelice F, Angeletti PM, Petrocelli R. Abdominal Aortic Screening Is a Priority for Health in Smoker Males: A Study on Central Italian Population. International Journal of Environmental Research and Public Health. 2022; 19(1):591. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010591
Chicago/Turabian StyleAltobelli, Emma, Filippo Gianfelice, Paolo Matteo Angeletti, and Reimondo Petrocelli. 2022. "Abdominal Aortic Screening Is a Priority for Health in Smoker Males: A Study on Central Italian Population" International Journal of Environmental Research and Public Health 19, no. 1: 591. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010591