
Emotions, Strategies, and Health: Examining the Impact of an Educational Program on Tanzanian Preschool Children



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants—Recruitment from Arusha, Tanzania
2.2. Survey Administration
2.3. The Intervention
2.4. Measures
2.4.1. Socio-Emotional
2.4.2. Health
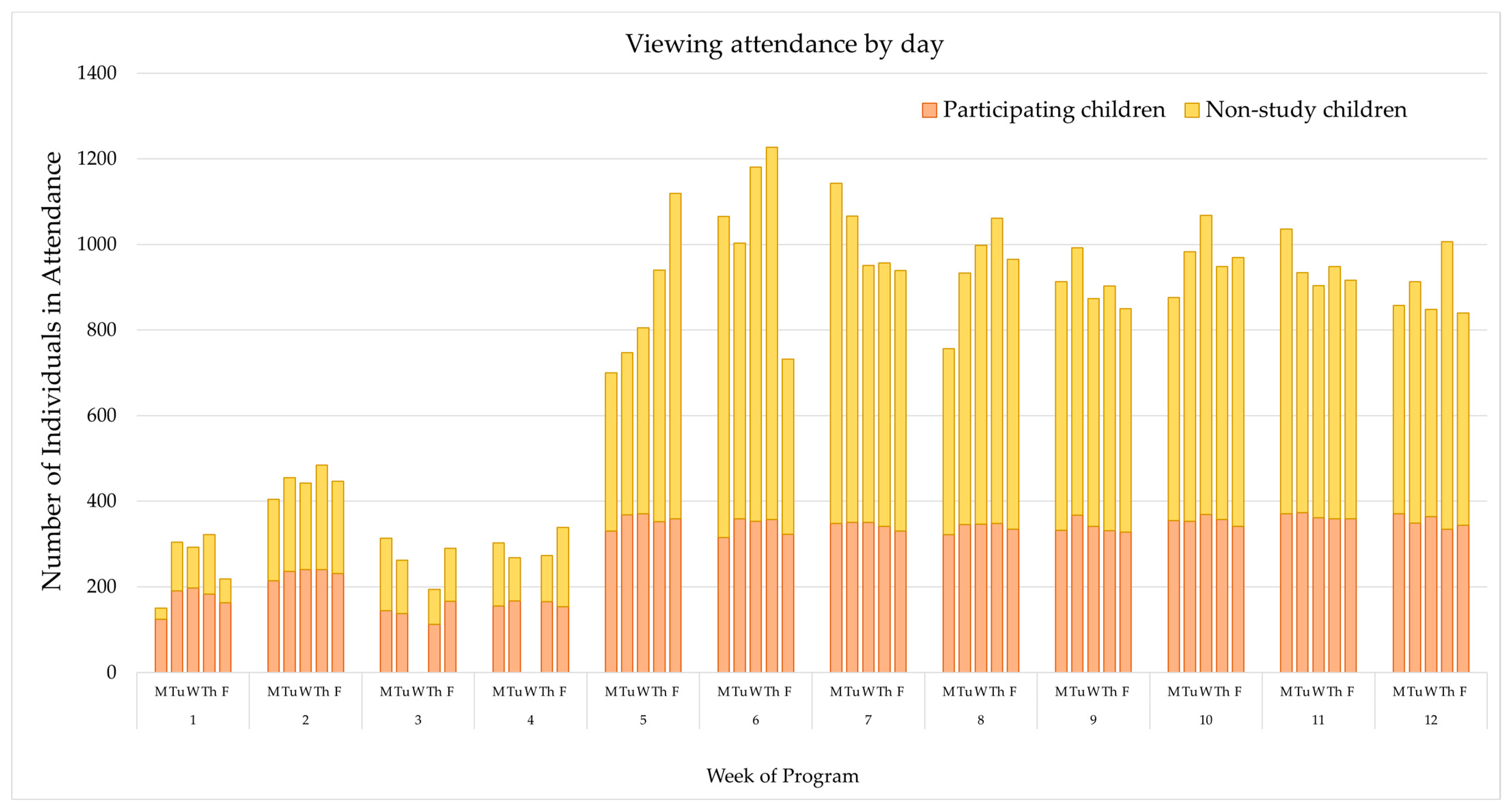
2.4.3. Receptivity and Attendance
2.5. Statistical Methods and Data Analyses
3. Results
3.1. Participants
3.2. Intervention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample Items | |
|---|---|
| Socio-Emotional | Prompt: (Picture card shown.) Glory is playing outside with her friends. She cannot find her teddy bear and begins to cry. Her friends want to make her feel better. |
| Emotions | S1.1 How does Glory feel? (Options: Happy, Sad, Sleepy, Angry) |
| Strategies | S1.2 What is the best thing for the friends to do? (Options: They should laugh at Glory; They should help Glory find her teddy bear; They could ignore/turn their backs on Glory; They could yell at Glory) |
| Health | |
| Health Behaviors | H10. What is a good way to exercise? (Show picture cards) (Options: Sitting, Dancing, Eating, Sleeping) |
| Food | H12. Some foods are good for you; others are unhealthy when you eat too much. Here is fish; it is healthy. This is ice candy; it is unhealthy. Can you help sort the healthy foods from unhealthy ones? (Presents child with 6 picture cards and has them sort accordingly) |

References
- Rogoff, B. Developmental transitions in children’s participation in sociocultural activities. In The Five to Seven Year Shift: The Age of Reason and Responsibility; Sameroff, A.J., Haith, M.M., Eds.; University of Chicago Press: Chicago, IL, USA, 1996; pp. 273–294. [Google Scholar]
- Witkower, Z.; Tracy, J.L.; Pun, A.; Baron, A.S. Can children recognize bodily expressions of emotion? J. Nonverbal Behav. 2021, 45, 505–518. [Google Scholar] [CrossRef]
- Bandura, A.; McDonald, F.J. Influence of social reinforcement and the behavior of models in shaping children’s moral judgment. J. Abnorm. Soc. Psychol. 1963, 67, 274–281. [Google Scholar] [CrossRef] [PubMed]
- Van Evra, J. Television and Child Development, 3rd ed.; Routledge: New York, NY, USA, 2004. [Google Scholar]
- Mitchell, A.E.; Kulasinghe, K.; Morawska, A. Establishing healthy personal hygiene habits with young children in Australia: A cross-sectional mixed methods study. Behav. Chang. 2021, 1–14. [Google Scholar] [CrossRef]
- Suyatmin, S.; Sukardi, S. Development of hygiene and healthy living habits learning module for early childhood education teachers. UJPH 2018, 7, 89–97. [Google Scholar] [CrossRef] [Green Version]
- Ngwaru, J.M. Promoting children’s sustainable access to early schooling in Africa: Reflections on the roles of parents in their children’s early childhood care and education. New Dir. Child Adolesc. Dev. 2014, 2014, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Bröder, J.; Okan, O.; Bauer, U.; Bruland, D.; Schlupp, S.; Bollweg, T.M.; Pinheiro, P. Health literacy in childhood and youth: A systematic review of definitions and models. BMC Public Health 2017, 17, 361. [Google Scholar] [CrossRef]
- Alderman, H.; Headey, D.D. How important is parental education for child nutrition? World Dev. 2017, 94, 448–464. [Google Scholar] [CrossRef]
- Engle, P.L.; Fernald, L.C.; Alderman, H.; Behrman, J.; O’Gara, C.; Yousafzai, A.; de Mello, M.C.; Hidrobo, M.; Ulkuer, N.; Global Child Development Steering Group; et al. Strategies for reducing inequalities and improving developmental outcomes for young children in low-income and middle-income countries. Lancet 2011, 378, 1339–1353. [Google Scholar] [CrossRef] [Green Version]
- Zosh, J.N.; Hopkins, E.J.; Jensen, H.; Liu, C.; Neale, D.; Hirsh-Pasek, K.; Whitebread, D. Learning through Play: A Review of the Evidence; LEGO Fonden: Billund, Denmark, 2017. [Google Scholar]
- Ligon, N. (Ubongo, Dar es Salaam, Tanzania). Personal communication, 2019.
- Lugalla, L.P.; Ngwaru, M. (Eds.) Education in Tanzania in the Era of Globalisation: Challenges and Opportunities; Mkuki na Nyota Publishers: Dar Es Salaam, Tanzania, 2019. [Google Scholar]
- Mares, M.L.; Pan, Z. Effects of Sesame Street: A meta-analysis of children’s learning in 15 countries. J. Appl. Dev. Psychol. 2013, 34, 140–151. [Google Scholar] [CrossRef]
- Borzekowski, D.L.G. A quasi-experiment examining the impact of educational cartoons on Tanzanian children. J. Appl. Dev. Psychol. 2018, 54, 53–59. [Google Scholar] [CrossRef]
- Anderson, D.R.; Pempek, T.A. Television and very young children. ABS 2005, 48, 505–522. [Google Scholar] [CrossRef]
- Kirkorian, H.L.; Wartella, E.A.; Anderson, D.R. Media and young children’s learning. Future Child 2008, 18, 39–61. [Google Scholar] [CrossRef] [PubMed]
- Borzekowski, D.L.G.; Lando, A.L.; Olsen, S.H.; Giffen, L. The impact of an educational media intervention to support children’s early learning in Rwanda. Int. J. Early Child 2019, 51, 109–126. [Google Scholar] [CrossRef]
- Fisch, S.M. Children’s Learning from Educational Television: Sesame Street and Beyond; Routledge: London, UK, 2004. [Google Scholar]
- Fisch, S.M.; Truglio, R.T.; Cole, C.F. The impact of Sesame Street on preschool children: A review and synthesis of 30 years’ research. Media Psychol. 1999, 1, 165–190. [Google Scholar] [CrossRef]
- Kearney, M.S.; Levine, P.B. Early Childhood Education by MOOC: Lessons from Sesame Street (No. w21229); National Bureau of Economic Research: Cambridge, MA, USA, 2015. [Google Scholar]
- Anderson, D.R.; Huston, A.C.; Schmitt, K.L.; Linebarger, D.L.; Wright, J.C.; Larson, R. Early childhood television viewing and adolescent behavior: The recontact study. Monogr. Soc. Res. Child Dev. 2001, 66, I-147. [Google Scholar]
- Cole, C.; Arafat, C.; Tidhar, C.; Tafesh, W.Z.; Fox, N.; Killen, M.; Yung, F. The educational impact of Rechov Sumsum/Shara’a Simsim: A Sesame Street television series to promote respect and understanding among children living in Israel, the West Bank, and Gaza. Int. J. Behav. Dev. 2003, 27, 409–422. [Google Scholar] [CrossRef]
- Borzekowski, D.L.G.; Macha, J.E. The role of Kilimani Sesame in the healthy development of Tanzanian preschool children. J. Appl. Dev. Psychol. 2010, 31, 298–305. [Google Scholar] [CrossRef]
- Borzekowski, D.L.G.; Henry, H.K. The impact of Jalan Sesama on the educational and healthy development of Indonesian preschool children: An experimental study. Int. J. Behav. Dev. 2011, 35, 169–179. [Google Scholar] [CrossRef]
- Ubongo. Available online: https://www.ubongo.org/contact/ (accessed on 28 March 2022).
- National Bureau of Statistics (NBS) [Tanzania]; ICF Macro. Tanzania Demographic and Health Survey 2010; NBS: Dar es Salaam, Tanzania; ICF Macro: Calverton, MD, USA, 2011; Available online: https://dhsprogram.com/pubs/pdf/FR243/FR243%5B24June2011%5D.pdf (accessed on 28 March 2022).
- Tanzanian Human Development Report 2017: Social Policy in the Context of Economic Transformation; Economic and Social Research Foundation: Dar es Salaam, Tanzania; United Nations Development Programme: Dar es Salaam, Tanzania; Government of the United Republic of Tanzania: Dodoma, Tanzania, 2018.
- Ministry of Education, Science and Technology (MOEST); President’s Office, Regional and Local Government (PO-RALG). The United Republic of Tanzania: Education Sector Performance Report 2017/2018: Tanzania Mainland; United Nations International Children’s Emergency Fund (UNICEF): Tanzania, 2018; Available online: https://static1.squarespace.com/static/5ae8cdb955b02c7c455f14c5/t/5d27875c1c057b00019e8344/1562871658189/MOEST+Performance+Report+2018+Draft+15.9.2018+for+circulation.pdf (accessed on 28 March 2022).
- United Nations International Children’s Emergency Fund (UNICEF): United Republic of Tanzania. Education. Available online: https://www.unicef.org/tanzania/what-we-do/education (accessed on 28 March 2022).
- Borzekowski, D.L.G.; Singpurwalla, D.; Mehrotra, D.; Howard, D. The impact of Galli Galli Sim Sim on Indian preschoolers. J. Appl. Dev. Psychol. 2019, 64, 101054. [Google Scholar] [CrossRef]
- Pietrobelli, A.; Agosti, M.; The MeNu Group. Nutrition in the first 1000 days: Ten practices to minimize obesity emerging from published science. Int. J. Environ. Res. Public Health 2017, 14, 1491. [Google Scholar] [CrossRef] [Green Version]
- Birch, L.; Savage, J.S.; Ventura, A. Influences on the development of children’s eating behaviours: From infancy to adolescence. Can. J. Diet. Pract. Res. 2007, 68, s1-56. [Google Scholar] [PubMed]
- Manyengo, P.R. Background Report: Digitalization in Teaching and Education in the United Republic of Tanzania: Digitalization, the Future of Work and the Teaching Profession Project; International Labour Organization: Geneva, Switzerland, 2021; pp. 12–13. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_dialogue/---sector/documents/publication/wcms_783673.pdf (accessed on 28 March 2022).



| Characteristic | Subcategory | n (%) |
|---|---|---|
| Sex | Male | 221 (54%) |
| Female | 190 (46%) | |
| Age | 3–4 years old | 47 (11%) |
| 5 years old | 200 (49%) | |
| 6–9 years old | 164 (40%) | |
| Electricity | Yes | 69 (17%) |
| No | 310 (75%) | |
| N/A | 32 (8%) | |
| Regular access to television | Yes | 86 (21%) |
| No | 230 (56%) | |
| N/A | 95 (23%) |
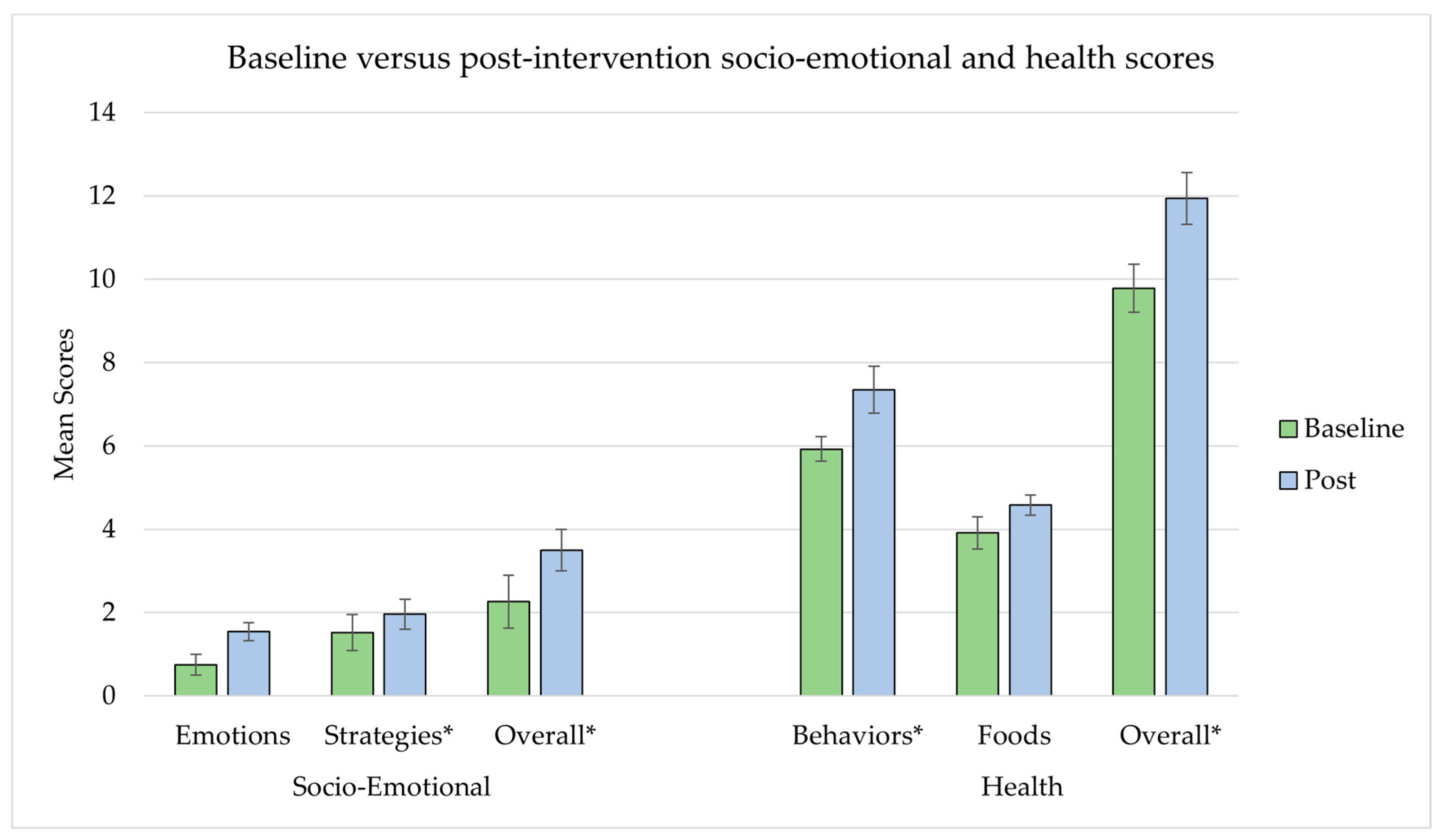
| Variables | Maximum Possible Score | Baseline Score | Post-Intervention Score | Bivariate Multi-Level Model |
|---|---|---|---|---|
| Mean (95% CL) | Mean (95% CL) | p-Value | ||
| Socio-Emotional | ||||
| Emotions | 6 | 0.74 (0.50, 0.99) | 1.54 (1.33, 1.75) | 0.2232 |
| Strategies | 6 | 1.52 (1.09, 1.95) | 1.96 (1.60, 2.32) | <0.0001 |
| OVERALL | 12 | 2.26 (1.63, 2.89) | 3.50 (3.00, 3.99) | <0.0001 |
| Health | ||||
| Behaviors | 19 * | 5.92 (5.63, 6.22) | 7.35 (6.79, 7.91) | <0.0001 |
| Foods | 8 | 3.91 (3.52, 4.30) | 4.58 (4.34, 4.82) | 0.5420 |
| OVERALL | 27 | 9.78 (9.21, 10.36) | 11.94 (11.32, 12.56) | <0.0001 |
| Emotions | Strategies | Overall Socio- Emotional | |
|---|---|---|---|
| Estimate | Estimate | Estimate | |
| Intercept | 0.43 | −0.22 | −0.2 |
| Sex: Male (vs. Female) | 0.36 * | 0.01 | 0.39 |
| Age | 0.02 | 0.11 | 0.18 |
| Baseline score | 0.13 ~ | 0.49 *** | 0.47 *** |
| General Media Receptivity | −0.53 | 0.05 | −0.52 |
| Akili and Me Receptivity | 0.25 *** | 0.29 *** | 0.50 *** |
| AIC fit statistic | 1503.5 | 1677.9 | 2002.6 |
| % gain for knowing all four Akili and Me characters | 16.66% | 19.13% | 16.74% |
| Health Behaviors | Foods | Overall Health | |
|---|---|---|---|
| Estimate | Estimate | Estimate | |
| Intercept | 4.20 *** | 3.29 *** | 6.48 *** |
| Sex: Male (vs. Female) | 0.14 | 0.24 | 0.48 ~ |
| Age | 0.04 | 0.1 | 0.19 |
| Baseline score | 0.29 *** | 0.03 | 0.26 *** |
| General media receptivity | 0.49 | −0.55 | −0.06 |
| Akili and Me receptivity | 0.40 *** | 0.17 ** | 0.57 *** |
| AIC fit statistic | 1822.4 | 1505.9 | 2053 |
| % gain for knowing all four Akili and Me characters | 8.45% | 8.39% | 8.44% |
| Emotions | Strategies | Overall Socio- Emotional | |
|---|---|---|---|
| Estimate | Estimate | Estimate | |
| Intercept | 0.43 | 0.32 | 0.34 |
| Sex: Male (vs. Female) | 0.38 * | 0.04 | 0.42 |
| Age | 0.05 | 0.14 | 0.24 |
| Baseline score | 0.12 ~ | 0.53 *** | 0.53 *** |
| General media receptivity | −0.47 | 0.08 | −0.46 |
| Thursday attendance (days) | 0.07 * | 0.01 | 0.06 |
| AIC fit statistic | 1520.7 | 1693.6 | 2024.4 |
| Health Behaviors | Foods | Overall Health | |
|---|---|---|---|
| Estimate | Estimate | Estimate | |
| Intercept | 4.09 ** | 3.39 *** | 6.51 *** |
| Sex: Male (vs. Female) | 0.09 | 0.24 | 0.44 |
| Age | 0.05 | 0.12 | 0.21 |
| Baseline score | 0.33 *** | 0.04 | 0.30 *** |
| General media receptivity | 0.4 | −0.54 | −0.17 |
| Friday attendance (days) | 0.12 * | 0.03 | 0.14 * |
| AIC fit statistic | 1837.5 | 1514.4 | 2072.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kauffman, L.E.; Dura, E.A.; Borzekowski, D.L.G. Emotions, Strategies, and Health: Examining the Impact of an Educational Program on Tanzanian Preschool Children. Int. J. Environ. Res. Public Health 2022, 19, 5884. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105884
Kauffman LE, Dura EA, Borzekowski DLG. Emotions, Strategies, and Health: Examining the Impact of an Educational Program on Tanzanian Preschool Children. International Journal of Environmental Research and Public Health. 2022; 19(10):5884. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105884
Chicago/Turabian StyleKauffman, Lauren E., Elizabeth A. Dura, and Dina L. G. Borzekowski. 2022. "Emotions, Strategies, and Health: Examining the Impact of an Educational Program on Tanzanian Preschool Children" International Journal of Environmental Research and Public Health 19, no. 10: 5884. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19105884