
Observational Variables for Considering a Switch from a Normal to a Dysphagia Diet among Older Adults Requiring Long-Term Care: A One-Year Multicenter Longitudinal Study

 , , , , , , , , , and
, , , , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
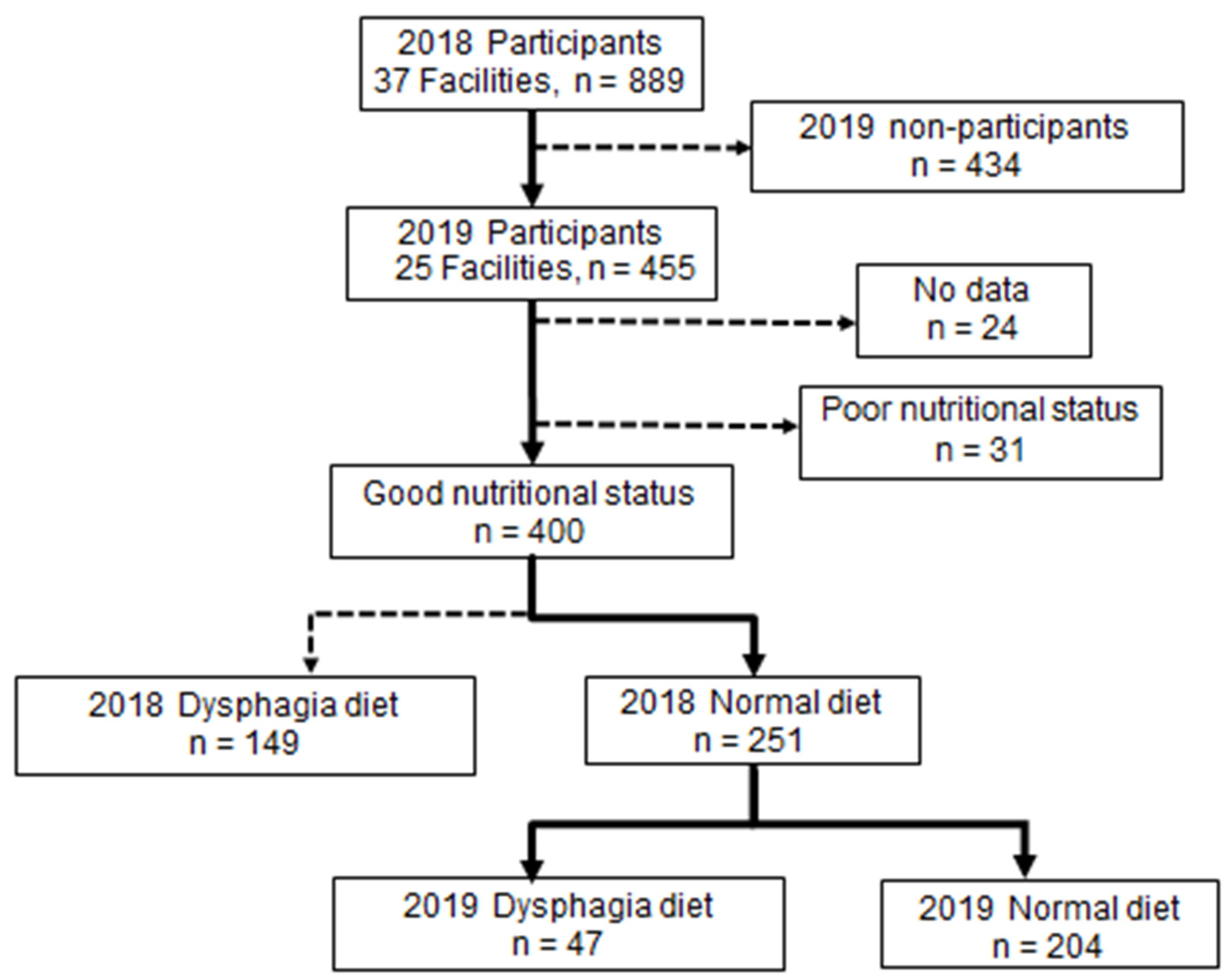
2.1. Study Design and Participants
2.2. Survey Items
2.2.1. Questionnaire Survey
Basic Information
Life and Cognitive Function Assessment
2.2.2. Oral Status
2.2.3. Measurements
Oral Status Assessment
Objective Assessment of the Oral Function
- Oral diadochokinesis (ODK)
- 2.
- Modified water swallowing test (MWST)
- 3.
- Repetitive saliva swallowing test (RSST)
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kawashima, K.; Motohashi, Y.; Fujishima, I. Prevalence of Dysphagia Among Community-Dwelling Elderly Individuals as Estimated Using a Questionnaire for Dysphagia Screening. Dysphagia 2004, 19, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, K.; Kikutani, T.; Tamura, F. Survey of suspected dysphagia prevalence in home-dwelling older people using the 10-Item Eating Assessment Tool (EAT-10). PLoS ONE 2019, 14, e0211040. [Google Scholar] [CrossRef] [PubMed]
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clave, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons-from pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging 2016, 11, 189–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Williams, K.; Batchelor-Murphy, M.; Perkhounkova, Y.; Hein, M. Eating performance in relation to intake of solid and liquid food in nursing home residents with dementia: A secondary behavioral analysis of mealtime videos. Int. J. Nurs. Stud. 2019, 96, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Kocdor, P.; Ms, E.R.S.; Giese, R.; Tulunay-Ugur, O.E. Characteristics of dysphagia in older patients evaluated at a tertiary center. Laryngoscope 2014, 125, 400–405. [Google Scholar] [CrossRef]
- Park, W.Y.; Lee, T.H.; Ham, N.S.; Park, J.W.; Lee, Y.G.; Cho, S.J.; Lee, J.S.; Hong, S.J.; Jeon, S.R.; Kim, H.G.; et al. Adding Endoscopist-Directed Flexible Endoscopic Evaluation of Swallowing to the Videofluoroscopic Swallowing Study Increased the Detection Rates of Penetration, Aspiration, and Pharyngeal Residue. Gut Liver 2015, 9, 623–628. [Google Scholar] [CrossRef] [Green Version]
- Campbell-Taylor, I. Oropharyngeal Dysphagia in Long-Term Care: Misperceptions of Treatment Efficacy. J. Am. Med Dir. Assoc. 2008, 9, 523–531. [Google Scholar] [CrossRef]
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R. A Systematic Review of the Prevalence of Oropharyngeal Dysphagia in Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, and Pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef]
- Takeda, M.; Okada, K.; Kondo, M.; Taira, K.; Watanabe, Y.; Ito, K.; Nakajima, J.; Ozaki, Y.; Sasaki, R.; Nishi, Y.; et al. Factors Associated with Food Form in Long-Term Care Insurance Facilities. Dysphagia 2022. [Google Scholar] [CrossRef]
- Endo, A.; Watanabe, Y.; Matsushita, T.; Okada, K.; Ohara, Y.; Iwasaki, M.; Ito, K.; Nakajima, J.; Iwasa, Y.; Itoda, M.; et al. Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 10776. [Google Scholar] [CrossRef]
- Lai, K.-Y.; Wu, T.-H.; Liu, C.-S.; Lin, C.-H.; Lin, C.-C.; Lai, M.-M.; Lin, W.-Y. Body mass index and albumin levels are prognostic factors for long-term survival in elders with limited performance status. Aging 2020, 12, 1104–1113. [Google Scholar] [CrossRef] [PubMed]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.C. The Clinical Dementia Rating (cdr): Current Version and Scoring Rules. Neurology 1991, 41, 1588–1592. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Fujishima, I. Textural Changes by Mastication and Proper Food Texture for Patients with Oropharyngeal Dysphagia. Nutrients 2020, 12, 1613. [Google Scholar] [CrossRef]
- Watanabe, E.; Yamagata, Y.; Fujitani, J.; Fujishima, I.; Takahashi, K.; Uyama, R.; Ogoshi, H.; Kojo, A.; Maeda, H.; Ueda, K.; et al. The Criteria of Thickened Liquid for Dysphagia Management in Japan. Dysphagia 2017, 33, 26–32. [Google Scholar] [CrossRef]
- Tanaka, T.; Takahashi, K.; Hirano, H.; Kikutani, T.; Watanabe, Y.; Ohara, Y.; Furuya, H.; Tetsuo, T.; Akishita, M.; Iijima, K. Oral Frailty as a Risk Factor for Physical Frailty and Mortality in Community-Dwelling Elderly. J. Gerontol. A Biol Sci. Med. Sci. A 2018, 73, 1661–1667. [Google Scholar] [CrossRef]
- Zenner, P.M.; Losinski, D.S.; Mills, R.H. Using cervical auscultation in the clinical dysphagia examination in long-term care. Dysphagia 1995, 10, 27–31. [Google Scholar] [CrossRef]
- Tohara, H.; Saitoh, E.; Mays, K.A.; Kuhlemeier, K.; Palmer, J.B. Three Tests for Predicting Aspiration without Videofluorography. Dysphagia 2003, 18, 126–134. [Google Scholar] [CrossRef]
- Persson, E.; Wårdh, I.; Östberg, P. Repetitive Saliva Swallowing Test: Norms, Clinical Relevance and the Impact of Saliva Secretion. Dysphagia 2018, 34, 271–278. [Google Scholar] [CrossRef]
- Ott, A.; Senger, M.; Lötzbeyer, T.; Gefeller, O.; Sieber, C.C.; Volkert, D. Effects of a Texture-Modified, Enriched, and Reshaped Diet on Dietary Intake and Body Weight of Nursing Home Residents with Chewing and/or Swallowing Problems: An Enable Study. J. Nutr. Gerontol. Geriatr. 2019, 38, 361–376. [Google Scholar] [CrossRef]
- Suzuki, R.; Kikutani, T.; Yoshida, M.; Yamashita, Y.; Hirayama, Y. Prognosis-related factors concerning oral and general conditions for homebound older adults in Japan. Geriatr. Gerontol. Int. 2015, 15, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Leopold, N.A.; Kagel, M.C. Swallowing, ingestion and dysphagia: A reappraisal. Arch. Phys. Med. Rehabilitation 1983, 64, 371–373. [Google Scholar]
- Dziewas, R.; auf dem Brinke, M.; Birkmann, U.; Bräuer, G.; Busch, K.; Cerra, F.; Damm-Lunau, R.; Dunkel, J.; Fellgiebel, A.; Garms, E.; et al. Safety and clinical impact of FEES-results of the FEES-registry. Neurol. Res. Pract. 2019, 1, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Leder, S.B.; Murray, J.T. Fiberoptic Endoscopic Evaluation of Swallowing. Phys. Med. Rehabil. Clin. N Am. 2008, 19, 787–801. [Google Scholar] [CrossRef]
- Martin-Harris, B.; Jones, B. The Videofluorographic Swallowing Study. Phys. Med. Rehabilitation Clin. N Am. 2008, 19, 769–785. [Google Scholar] [CrossRef] [Green Version]
- Easterling, C.S.; Robbins, E. Dementia and Dysphagia. Geriatr. Nurs. 2008, 29, 275–285. [Google Scholar] [CrossRef]
- Edahiro, A.; Hirano, H.; Yamada, R.; Chiba, Y.; Watanabe, Y. Comparative study of eating behavior in elderly patients with Alzheimer’s disease and vascular dementia: A first report. -Comparison of disturbed eating behavior-. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2013, 50, 651–660. [Google Scholar] [CrossRef] [Green Version]
- Saitoh, E. Dysphagia rehabilitation. Rinsho Shinkeigaku 2008, 48, 875–879. [Google Scholar] [CrossRef] [Green Version]
- Keller, H.H.; Carrier, N.; Slaughter, S.E.; Lengyel, C.; Steele, C.; Duizer, L.; Morrison, J.; Brown, K.S.; Chaudhury, H.; Yoon, M.; et al. Prevalence and Determinants of Poor Food Intake of Residents Living in Long-Term Care. J. Am. Med Dir. Assoc. 2017, 18, 941–947. [Google Scholar] [CrossRef] [Green Version]
- Kuzuya, M. [Nutritional assessment and nutritional management for the elderly]. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2003, 40, 199–203. [Google Scholar] [CrossRef]
- Dietitians Association of Australia; The Speech Pathology Association of Australia Limited Texture-modified foods and thickened fluids as used for individuals with dysphagia: Australian standardised labels and definitions. Nutr. Diet. 2007, 64, S53–S76. [CrossRef]


{kind=link}
| Variable | 2018 Dysphagia Diet (n = 149) | 2018 Normal Diet (n = 251) | Good Nutritional Status (n = 400) | p-Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median, [Q1, Q3] | Mean ± SD | Median, [Q1, Q3] | Mean ± SD | Median, [Q1, Q3] | ||||||||
| n (%) | n (%) | n (%) | |||||||||||
| Age | 87.5 | ± | 7.6 | 89.0 [83.0, 93.0] | 85.9 | ± | 7.8 | 86.5 [81.0, 92.0] | 86.5 | ± | 7.7 | 87.0 [82.0, 92.0] | 0.042 |
| Sex (female), n (%) | 120 | (80.5) | 201 | (80.1) | 321 | (80.3) | 0.912 | ||||||
| Body mass index | 19.4 | ± | 2.7 | 19.4 [17.4, 21.3] | 21.9 | ± | 3.7 | 21.6 [19.5, 24.1] | 21.0 | ± | 3.6 | 20.8 [18.5, 22.9] | <0.001 |
| Barthel Index (Total points) | 17.7 | ± | 19.4 | 10.0 [0.0, 30.0] | 44.0 | ± | 24.8 | 45.0 [25.0, 60.0] | 34.2 | ± | 26.2 | 35.0 [10.0, 55.0] | <0.001 |
| Clinical dementia rating (Total points) | |||||||||||||
| 0, 0.5 | 4 | (2.7) | 40 | (15.9) | 44 | (11.0) | <0.001 | ||||||
| 1 | 14 | (9.4) | 70 | (27.9) | 84 | (21.0) | |||||||
| 2 | 36 | (24.2) | 84 | (33.5) | 120 | (30.0) | |||||||
| 3 | 90 | (60.2) | 56 | (22.3) | 146 | (36.5) | |||||||
| Simple evaluations (Oral conditions) | |||||||||||||
| Language (possible) | 80 | (53.7) | 203 | (80.9) | 283 | (70.8) | <0.001 | ||||||
| Drooling (none) | 87 | (58.4) | 222 | (88.4) | 309 | (77.3) | <0.001 | ||||||
| Halitosis (none) | 88 | (59.1) | 178 | (70.9) | 266 | (66.5) | 0.015 | ||||||
| Masticatory movement (move) | 116 | (77.9) | 241 | (96.0) | 357 | (89.3) | <0.001 | ||||||
| Tongue movement (move) | 76 | (51.0) | 207 | (82.5) | 283 | (70.8) | <0.001 | ||||||
| Perioral muscle function (move) | 102 | (68.5) | 221 | (88.0) | 323 | (80.8) | <0.001 | ||||||
| Left–right asymmetric movement of the mouth angle (not) | 116 | (77.9) | 229 | (91.2) | 345 | (86.3) | <0.001 | ||||||
| Swallowing (possible) | 91 | (61.1) | 235 | (93.6) | 326 | (81.5) | <0.001 | ||||||
| Coughing (not) | 57 | (38.3) | 201 | (80.1) | 258 | (64.5) | <0.001 | ||||||
| Changes in voice quality after swallowing (not) | 115 | (77.2) | 237 | (94.4) | 352 | (88.0) | <0.001 | ||||||
| Respiratory observation after swallowing (No abnormality) | 140 | (94.0) | 247 | (98.4) | 387 | (96.8) | 0.015 | ||||||
| Rinsing (possible) | 48 | (32.2) | 196 | (78.1) | 244 | (61.0) | <0.001 | ||||||
| Oral residue (none) | 53 | (35.6) | 137 | (54.6) | 190 | (47.5) | <0.001 | ||||||
| Objective evaluation of oral function | |||||||||||||
| Remaining Teeth | 6.0 | ± | 7.7 | 3.0 [0.0, 10.8] | 10.1 | ± | 9.5 | 7.0 [0.0, 19.0] | 8.6 | ± | 9.1 | 5.0 [0.0, 17.0] | <0.001 |
| Functional teeth | 16.4 | ± | 11.5 | 21.5 [3.3, 28.0] | 23.3 | ± | 7.5 | 28.0 [21.0, 28.0] | 20.7 | ± | 9.8 | 27.0 [15.5, 28.0] | <0.002 |
| ODK (ta) | 2.9 | ± | 2.9 | 3.0 [0.95, 3.8] | 3.9 | ± | 2.0 | 4.0 [2.4, 5.0] | 3.6 | ± | 2.3 | 3.6 [2.2, 5.0] | <0.003 |
| RSST | 1.9 | ± | 1.2 | 2.0 [1.0, 3.0] | 2.7 | ± | 1.4 | 3.0 [2.0, 4.0] | 2.6 | ± | 1.4 | 3.0 [2.0, 3.0] | <0.004 |
| MWST | 2.0 | ± | 2.1 | 0.0 [0.0, 4.0] | 3.8 | ± | 1.7 | 4.0 [4.0, 5.0] | 3.1 | ± | 2.1 | 4.0 [0.0, 5.0] | <0.005 |
| Variable | 2019 Dysphagia Diet (n = 47) | 2019 Normal Diet Maintained (n = 204) | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median, [Q1, Q3] | Mean ± SD | Median, [Q1, Q3] | ||||||
| n (%) | n (%) | ||||||||
| Age | 86.3 | ± | 7.6 | 86.0 [81.0, 93.0] | 85.8 | ± | 7.8 | 87.0 [81.0, 92.0] | 0.853 |
| Sex (female), n (%) | 35 | (74.5) | 166 | (81.4) | 0.285 | ||||
| Body mass index | 20.8 | ± | 3.7 | 20.7 [18.3, 23.0] | 22.1 | ± | 3.6 | 21.8 [19.7, 24.3] | 0.029 |
| Barthel Index (Total points) | 35.5 | ± | 20.0 | 35.0 [25.0, 50.0] | 46.0 | ± | 25.4 | 45.0 [25.0, 65.0] | 0.009 |
| Clinical Dementia Rating (Total points) | |||||||||
| 0, 0.5 | 1 | (2.1) | 39 | (19.1) | 0.036 | ||||
| 1 | 14 | (29.8) | 56 | (27.5) | |||||
| 2 | 20 | (42.6) | 64 | (31.4) | |||||
| 3 | 11 | (23.4) | 45 | (22.1) | |||||
| Simple evaluations (oral conditions) | |||||||||
| Language (possible) | 33 | (70.2) | 170 | (83.3) | 0.039 | ||||
| Drooling (none) | 39 | (83.0) | 183 | (89.7) | 0.16 | ||||
| Halitosis (none) | 30 | (62.8) | 148 | (72.5) | 0.235 | ||||
| Masticatory movement (move) | 44 | (93.6) | 197 | (96.6) | 0.351 | ||||
| Tongue movement (move) | 30 | (63.8) | 177 | (86.8) | <0.001 | ||||
| Perioral muscle function (move) | 35 | (74.5) | 186 | (91.2) | 0.003 | ||||
| Left–right asymmetric movement of the mouth angle (not) | 42 | (89.4) | 187 | (91.7) | 0.936 | ||||
| Swallowing (possible) | 41 | (87.2) | 194 | (95.1) | 0.047 | ||||
| Coughing (not) | 34 | (72.3) | 167 | (81.9) | 0.141 | ||||
| Changes in voice quality after swallowing (not) | 42 | (89.4) | 195 | (95.6) | 0.094 | ||||
| Respiratory observation after swallowing (No abnormality) | 45 | (95.7) | 202 | (99.0) | 0.106 | ||||
| Rinsing (possible) | 29 | (61.7) | 167 | (81.9) | 0.003 | ||||
| Oral residue (none) | 23 | (48.9) | 114 | (55.9) | 0.37 | ||||
| Objective evaluation of oral function | |||||||||
| Remaining teeth | 9.0 | ± | 9.2 | 5.0 [0.0, 18.3] | 10.3 | ± | 9.5 | 8.0 [0.0, 19.0] | 0.475 |
| Functional teeth | 20.9 | ± | 9.5 | 25.0 [16.3, 28.0] | 23.8 | ± | 6.9 | 28.0 [22.0, 28.0] | 0.08 |
| ODK (ta) | 4.4 | ± | 1.4 | 4.6 [3.4, 5.4] | 3.8 | ± | 2.1 | 3.8 [2.4, 5.0] | 0.03 |
| RSST | 2.0 | ± | 1.2 | 2.0 [1.0, 3.0] | 3.0 | ± | 1.4 | 3.0 [2.0, 4.0] | 0.003 |
| MWST | 3.3 | ± | 1.9 | 4.0 [2.3, 5.0] | 4.0 | ± | 1.6 | 4.0 [4.0, 5.0] | 0.011 |
| Model 1 | Model 2 | Model 3 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Oral Status | OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||||||
| Language (1: good, 2: bad) | 1.02 | * | 0.02 | – | 0.25 | 0.93 | −0.08 | – | 0.17 | 0.93 | −0.07 | – | 0.17 | ||
| Drooling (1: no, 2: yes) | 0.94 | −0.06 | – | 0.24 | 0.89 | −0.12 | – | 0.18 | 0.89 | −0.12 | – | 0.18 | |||
| Halitosis (1: no, 2: yes) | 0.94 | −0.06 | – | 0.15 | 0.88 | −0.13 | – | 0.08 | 0.88 | −0.13 | – | 0.08 | |||
| Masticatory movement (1: good, 2: bad) | 0.97 | −0.03 | – | 0.45 | 0.93 | −0.07 | – | 0.39 | 0.93 | −0.07 | – | 0.40 | |||
| Tongue movement (1: good, 2: bad) | 1.14 | ** | 0.13 | – | 0.38 | 1.06 | * | 0.06 | – | 0.31 | 1.06 | * | 0.06 | – | 0.31 |
| Perioral muscle function (1: good, 2: bad) | 1.13 | ** | 0.12 | – | 0.42 | 1.06 | * | 0.06 | – | 0.36 | 1.05 | * | 0.05 | – | 0.36 |
| Left–right asymmetric movement of the mouth angle (1: good, 2: bad) | 0.80 | −0.22 | – | 0.11 | 0.77 | −0.26 | – | 0.05 | 0.77 | −0.26 | – | 0.05 | |||
| Swallowing (1: good, 2: bad) | 1.01 | * | 0.01 | – | 0.40 | 0.91 | −0.09 | – | 0.29 | 0.91 | −0.09 | – | 0.29 | ||
| Coughing (1: no, 2: yes) | 1.00 | * | 0.00 | – | 0.24 | 0.94 | −0.07 | – | 0.17 | 0.94 | −0.06 | – | 0.18 | ||
| Changes in voice quality after swallowing (1: no abnormality, 2: abnormality) | 0.92 | −0.08 | – | 0.33 | 0.84 | −0.17 | – | 0.23 | 0.84 | −0.17 | – | 0.24 | |||
| Respiratory observation after swallowing (1: good, 2: bad) | 0.88 | −0.13 | – | 0.60 | 0.84 | −0.17 | – | 0.52 | 0.85 | −0.16 | – | 0.54 | |||
| Rinsing (1: possible, 2: impossible) | 1.11 | ** | 0.10 | – | 0.32 | 1.01 | * | 0.01 | – | 0.25 | 1.01 | * | 0.01 | – | 0.25 |
| Oral residue (1: no, 2: yes) | 0.99 | −0.01 | – | 0.19 | 0.93 | −0.08 | – | 0.13 | 0.93 | −0.07 | – | 0.14 | |||
| Objective evaluation of oral function | OR | 95% CI | OR | 95% CI | OR | 95% CI | |||||||||
| Remaining teeth | 1.00 | 0.00 | – | 0.01 | 1.00 | 0.00 | – | 0.01 | 1.00 | 0.00 | – | 0.01 | |||
| Functional teeth | 1.00 | * | 0.00 | – | 0.02 | 1.00 | * | 0.00 | – | 0.01 | 1.00 | * | 0.00 | – | 0.01 |
| ODK (ta) male | 0.73 | −0.32 | – | 0.26 | 0.66 | −0.42 | – | 0.23 | 0.66 | −0.42 | – | 0.24 | |||
| ODK (ta) female | 0.78 | −0.24 | 0.04 | 0.78 | −0.25 | 0.04 | 0.77 | −0.26 | 0.04 | ||||||
| RSST | 0.70 | −0.36 | – | 0.18 | 0.84 | −0.18 | – | 0.03 | 0.93 | −0.08 | – | 0.15 | |||
| MWST | 0.93 | −0.07 | – | 0.22 | 0.94 | −0.06 | – | 0.16 | 0.94 | −0.06 | – | 0.16 | |||
| Variable | OR | 95% CI | |||
|---|---|---|---|---|---|
| Age | 1.00 | −0.01 | – | 0.01 | |
| Sex (1: male, 2: female) | 0.92 | −0.08 | – | 0.15 | |
| Body mass index | 0.97 | * | −0.03 | – | 0.00 |
| Barthel Index | 0.99 | ** | −0.01 | – | 0.00 |
| Clinical Dementia Rating | |||||
| 0, 0.5 | Reference | ||||
| 1 | 1.09 | * | 0.08 | – | 0.36 |
| 2 | 1.16 | ** | 0.15 | – | 0.43 |
| 3 | 1.14 | ** | 0.13 | – | 0.45 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeda, M.; Watanabe, Y.; Matsushita, T.; Taira, K.; Miura, K.; Ohara, Y.; Iwasaki, M.; Ito, K.; Nakajima, J.; Iwasa, Y.; et al. Observational Variables for Considering a Switch from a Normal to a Dysphagia Diet among Older Adults Requiring Long-Term Care: A One-Year Multicenter Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 6586. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116586
Takeda M, Watanabe Y, Matsushita T, Taira K, Miura K, Ohara Y, Iwasaki M, Ito K, Nakajima J, Iwasa Y, et al. Observational Variables for Considering a Switch from a Normal to a Dysphagia Diet among Older Adults Requiring Long-Term Care: A One-Year Multicenter Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6586. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116586
Chicago/Turabian StyleTakeda, Maaya, Yutaka Watanabe, Takae Matsushita, Kenshu Taira, Kazuhito Miura, Yuki Ohara, Masanori Iwasaki, Kayoko Ito, Junko Nakajima, Yasuyuki Iwasa, and et al. 2022. "Observational Variables for Considering a Switch from a Normal to a Dysphagia Diet among Older Adults Requiring Long-Term Care: A One-Year Multicenter Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 11: 6586. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116586