
Association between Ultraviolet B Exposure Levels and Depression in Taiwanese Adults: A Nested Case–Control Study

 and
and
Abstract
:1. Introduction
2. Methods
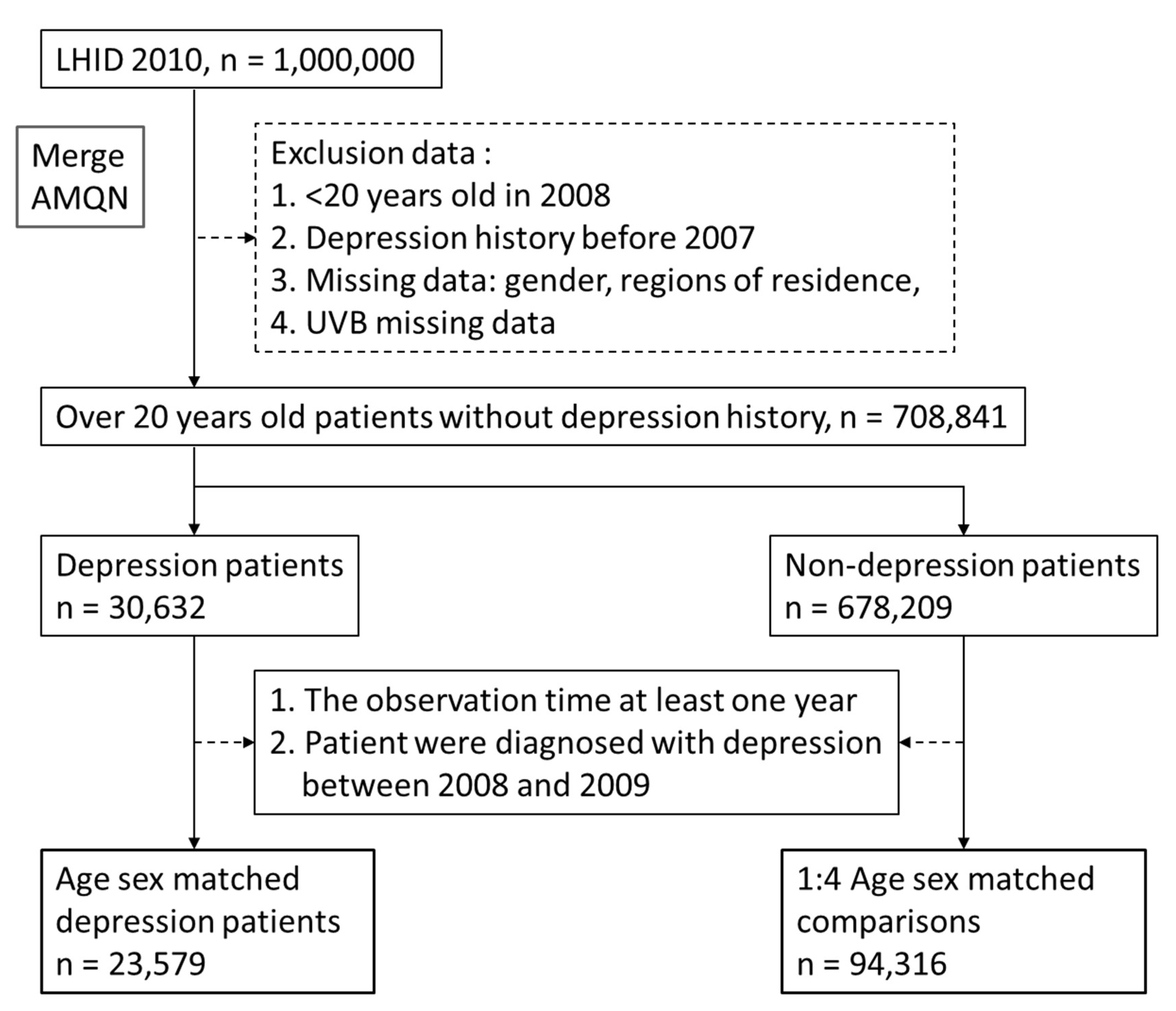
2.1. Data Source
2.2. Study Population
2.3. Comorbidities
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rastogi, R.P.; Richa, A.; Kumar, M.B.; Tyagi; Sinha, R.P. Molecular Mechanisms of Ultraviolet Radiation–Induced DNA Damage and Repair. J. Nucleic Acids 2010, 2010, 592980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akhter, K.F.; Mumin, A.; Lui, E.M.; Charpentier, P.A. Transdermal nanotherapeutics: Panax quinquefolium polysaccharide nanoparticles attenuate UVB–induced skin cancer. Int. J. Biol. Macromol. 2021, 181, 221–231. [Google Scholar] [CrossRef] [PubMed]
- WHO Depression. World Health Organization, Geneva 2021. Available online: https://www.who.int/news–room/fact–sheets/detail/depression (accessed on 13 September 2021).
- Reddy, M. Depression: The Disorder and the Burden. Indian J. Psychol. Med. 2010, 32, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, A.; Je, L.S. Understanding comorbidity with depression and anxiety disorders. J. Osteopath. Med. 2006, 106 (Suppl. S2), S9–S14. [Google Scholar]
- Huang, B.; Huang, Z.; Tan, J.; Xu, H.; Deng, K.; Cheng, J.; Ren, Z.; Gong, X.; Gao, Y. The mediating and interacting role of physical activity and sedentary behavior between diabetes and depression in people with obesity in United States. J. Diabetes Its Complicat. 2020, 35, 107764. [Google Scholar] [CrossRef]
- Kessler, R.C.; Sampson, N.A.; Berglund, P.; Gruber, M.J.; Al–Hamzawi, A.; Andrade, L.; Bunting, B.; Demyttenaere, K.; Florescu, S.; De Girolamo, G.; et al. Anxious and non–anxious major depressive disorder in the World Health Organization World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 2015, 24, 210–226. [Google Scholar] [CrossRef] [Green Version]
- Kalin, N.H. The Critical Relationship Between Anxiety and Depression. Am. J. Psychiatry 2020, 177, 365–367. [Google Scholar] [CrossRef]
- Miulescu, R.D.; Calarasu, M.; Rosca, R.; Danoiu, S. P02–25–The prevalence of depression in patients with cushing’s syndrome. Eur. Psychiatry 2011, e26, 620. [Google Scholar] [CrossRef]
- Tang, A.; O’Sullivan, A.J.; Diamond, T.; Gerard, A.; Campbell, P. Psychiatric symptoms as a clinical presentation of Cushing’s syndrome. Ann. Gen. Psychiatry 2013, 12, 23. [Google Scholar] [CrossRef] [Green Version]
- Cummings, J.L. Depression and Parkinson’s disease: A review. Am. J. Psychiatry 1992, 149, 443–454. [Google Scholar] [CrossRef]
- Wragg, R.E.; Jeste, D.V. Overview of depression and psychosis in Alzheimer’s disease. Am. J. Psychiatry 1989, 146, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Sultzer, D.L.; Levin, H.S.; Mahler, M.E.; High, W.M.; Cummings, J.L. A comparison of psychiatric symptoms in vascular dementia and Alzheimer’s disease. Am. J. Psychiatry 1993, 150, 1806–1812. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Krishnan, R.R.K.; O’Connor, C.M. Depression and Heart Disease: Evidence of a link, and its therapeutic implications. CNS Drugs 2002, 16, 111–127. [Google Scholar] [CrossRef] [PubMed]
- Zweig, R.M.; Ross, C.A.; Hedreen, J.C.; Steele, C.; Cardillo, J.E.; Whitehouse, P.J.; Folstein, M.F.; Price, N.L. The neuropathology of aminergic nuclei in Alzheimer’s disease. Ann. Neurol. 1988, 24, 233–242. [Google Scholar] [CrossRef]
- Mayeux, R.; Stern, Y.; Williams, J.B.; Cote, L.; Frantz, A.; Dyrenfurth, I. Clinical and biochemical features of depression in Parkinson’s disease. Am. J. Psychiatry 1986, 143, 756–759. [Google Scholar] [CrossRef]
- Starkstein, S.E.; Preziosi, T.J.; Bolduc, P.L.; Robinson, R.G. Depression in Parkinson’s Disease. J. Nerv. Ment. Dis. 1990, 178, 27–31. [Google Scholar] [CrossRef]
- Krishnan, K.R.; Delong, M.; Kraemer, H.; Carney, R.; Spiegel, D.; Gordon, C.; McDonald, W.; Dew, M.A.; Alexopoulos, G.; Buckwalter, K.; et al. Comorbidity of depression with other medical diseases in the elderly. Biol. Psychiatry 2002, 52, 559–588. [Google Scholar] [CrossRef]
- Slominski, A.T.; Zmijewski, M.A.; Plonka, P.M.; Szaflarski, J.P.; Paus, R. How UV Light Touches the Brain and Endocrine System Through Skin, and Why. Endocrinology 2018, 159, 1992–2007. [Google Scholar] [CrossRef] [Green Version]
- Veleva, B.I.; Van Bezooijen, R.L.; Chel, V.G.M.; Numans, M.E.; Caljouw, M.A.A. Effect of ultraviolet light on mood, depressive disorders and well–being. Photodermatol. Photoimmunol. Photomed. 2018, 34, 288–297. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the omega-3 fatty acids control serotonin synthesis and action, part 2: Relevance for ADHD, bipolar disorder, schizophrenia, and impulsive behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef] [Green Version]
- Caldwell, J.D.; Londe, K.; Ochs, S.D.; Hajdu, Z.; Rodewald, A.; Gebhart, V.M. Three steroid–binding globulins, their localiza–tion in the brain and nose, and what they might be doing there. Steroids 2019, 142, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Kaviani, M.; Nikooyeh, B.; Zand, H.; Yaghmaei, P.; Neyestani, T.R. Effects of vitamin D supplementation on depression and some involved neurotransmitters. J. Affect. Disord. 2020, 269, 28–35. [Google Scholar] [CrossRef] [PubMed]
- El–Mallakh, R.S.; Ali, Z. Therapeutic implications of the serotonin transporter gene in depression. Biomark. Neuropsychiatry 2019, 1, 100004. [Google Scholar] [CrossRef]
- Azmitia, E.C. Chapter 1–Evolution of Serotonin: Sunlight to Suicide. Handb. Behav. Neurosci. 2010, 31, 3–22. [Google Scholar] [CrossRef]
- Carney, R.M.; Rich, M.W.; Tevelde, A.; Saini, J.; Clark, K.; Jaffe, A.S. Major depressive disorder in coronary artery disease. Am. J. Cardiol. 1987, 60, 1273–1275. [Google Scholar] [CrossRef]
- Dew, M.A.; Becker, J.T.; Sanchez, J.; Caldararo, R.; Lopez, O.L.; Wess, J.; Dorst, S.K.; Banks, G. Prevalence and predictors of depressive, anxiety and substance use disorders in HIV–infected and uninfected men: A longitudinal evaluation. Psychol. Med. 1997, 27, 395–409. [Google Scholar] [CrossRef] [PubMed]
- Baldewicz, T.T.; Goodkin, K.; Blaney, N.T.; Shor–Posner, G.; Kumar, M.; Wilkie, F.L.; Baum, M.K.; Eisdorfer, C. Cobalamin level is related to self–reported and clinically rated mood and to syndromal depression in bereaved HIV–1+ and HIV–1− homosexual men. J. Psychosom. Res. 2000, 48, 177–185. [Google Scholar] [CrossRef]
- Watson, R.; Gibbs, N.K.; Griffiths, C.; Sherratt, M. Damage to Skin Extracellular Matrix Induced by UV Exposure. Antioxid. Redox Signal. 2014, 21, 1063–1077. [Google Scholar] [CrossRef]
- Wagener, F.A.; Carels, C.E.; Lundvig, D. Targeting the redox balance in inflammatory skin conditions. Int. J. Mol. Sci. 2013, 14, 9126–9167. [Google Scholar] [CrossRef]
- Smith, H.R. Depression in cancer patients: Pathogenesis, implications and treatment (Review). Oncol. Lett. 2015, 9, 1509–1514. [Google Scholar] [CrossRef] [Green Version]
- Beesley, V.L.; Hughes, M.C.B.; Smithers, B.M.; Khosrotehrani, K.; Malt, M.K.; Von Schuckmann, L.A.; Green, A.C. Anxiety and depression after diagnosis of high–risk primary cutaneous melanoma: A 4–year longitudinal study. J. Cancer Surviv. 2020, 14, 712–719. [Google Scholar] [CrossRef] [PubMed]
- Zhao, G.; Okoro, C.A.; Li, J.; White, A.; Dhingra, S.; Li, C. Current depression among adult cancer survivors: Findings from the 2010 Behavioral Risk Factor Surveillance System. Cancer Epidemiol. 2014, 38, 757–764. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.-Y.; Su, C.-C.; Shao, S.-C.; Sung, S.-F.; Lin, S.-J.; Kao Yang, Y.-H.; Lai, E.C.-C. Taiwan’s National Health Insurance Research Database: Past and future. Clin. Epidemiol. 2019, 11, 349–358. [Google Scholar] [CrossRef] [Green Version]
- Taiwan Air Quality Monitoring Network. 2019 TAQMN Site. Available online: http://taqm.epa.gov.tw/taqm/en/b0101.aspx (accessed on 11 August 2019).
- Hsu, W.-T.; Hsu, C.-C.; Wen, M.-H.; Lin, H.-C.; Tsai, H.-T.; Su, P.; Sun, C.-T.; Lin, C.-L.; Hsu, C.-Y.; Chang, K.-H.; et al. Increased risk of depression in patients with acquired sensory hearing loss. Medicine 2016, 95, e5312. [Google Scholar] [CrossRef] [PubMed]
- Menza, M.A.; Robertson–Hoffman, D.E.; Bonapace, A.S. Parkinson’s disease and anxiety: Comorbidity with depression. Biol. Psychiatry 1993, 34, 465–470. [Google Scholar] [CrossRef]
- Han, W.; Wei, Z.; Dang, R.; Guo, Y.; Zhang, H.; Geng, C.; Wang, C.; Feng, Q.; Jiang, P. Angiotensin–Ⅱ and angiotensin–(1–7) imbalance affects comorbidity of depression and coronary heart disease. Peptides 2020, 131, 170353. [Google Scholar] [CrossRef] [PubMed]
- Perez–Tejada, J.; Labaka, A.; Vegas, O.; Larraioz, A.; Pescador, A.; Arregi, A. Anxiety and depression after breast cancer: The predictive role of monoamine levels. Eur. J. Oncol. Nurs. 2021, 52, 101953. [Google Scholar] [CrossRef]
- Defrancesco, M.; Pechlaner, R.; Kiechl, S.; Willeit, J.; Deisenhammer, E.A.; Hinterhuber, H.; Rungger, G.; Gasperi, A.; Marksteiner, J. What Characterizes Depression in Old Age? Results from the Bruneck Study. Pharmacopsychiatry 2017, 51, 153–160. [Google Scholar] [CrossRef]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta–analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef]
- Sun, H.-Y.; Luo, C.-W.; Chiang, Y.-W.; Li, K.-L.; Ho, Y.-C.; Lee, S.-S.; Chen, W.-Y.; Chen, C.-J.; Kuan, Y.-H. Association Between PM2.5 Exposure Level and Primary Open–Angle Glaucoma in Taiwanese Adults: A Nested Case–control Study. Int. J. Environ. Res. Public Heal. 2021, 18, 1714. [Google Scholar] [CrossRef]
- Bracke, P.; Delaruelle, K.; Dereuddre, R.; Van de Velde, S. Depression in women and men, cumulative disadvantage and gender inequality in 29 European countries. Soc. Sci. Med. 2020, 267, 113354. [Google Scholar] [CrossRef] [PubMed]
- Anguzu, R.; Nagavally, S.; Dawson, A.Z.; Walker, R.J.; Egede, L.E. Age and Gender Differences in Trends and Impact of Depression on Quality of Life in the United States, 2008 to 2016. Women’s Health Issues 2021, 31, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Onuh, J.C.; Mbah, P.O.; Ajaero, C.K.; Orjiakor, C.T.; Igboeli, E.E.; Ayogu, C.K. Rural–urban appraisal of the prevalence and factors of depression status in South Africa. J. Affect. Disord. Rep. 2021, 4, 100082. [Google Scholar] [CrossRef]
- Kim, Y.; Woo, H.; Withers, E. Low income dynamics and depression over the life course in South Korea. Adv. Life Course Res. 2020, 48, 100400. [Google Scholar] [CrossRef]
- Huang, Y.; Su, Y.; Chen, H.; Liu, H.; Hu, J. Serum Levels of CRP are Associated with Depression in a Middle–aged and Elderly Population with Diabetes Mellitus: A Diabetes Mellitus–Stratified Analysis in a Population–Based Study. J. Affect. Disord. 2020, 281, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Lin, K.Y.-H.; Chou, C.-Y.; Chang, C.Y.-Y.; Lin, W.-C.; Wan, L. Association between oophorectomy and depression in patients with comorbidities: A nationwide cohort study in Taiwan. Taiwan. J. Obstet. Gynecol. 2020, 59, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Mead, M.N. Benefits of Sunlight: A Bright Spot for Human Health. Environ. Heal. Perspect. 2008, 116, A160–A167. [Google Scholar] [CrossRef] [Green Version]
- Holick, M.F. Vitamin D Status: Measurement, Interpretation, and Clinical Application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [Green Version]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Zhao, Y.; Fan, X.; Wang, J.; Lu, W.; Zheng, X. Independent Associations of Serum 25–hydroxyvitamin D3 and D2 with Depressive Symptoms in Females. J. Affect. Disord. 2021, 296, 342–349. [Google Scholar] [CrossRef]
- Gowda, U.; Mutowo, M.P.; Smith, B.J.; Wluka, A.E.; Renzaho, A.M.N. Vitamin D supplementation to reduce depression in adults: Meta–analysis of randomized controlled trials. Nutrition 2015, 31, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Urbanski, A.; Schwarz, T.; Neuner, P.; Krutmann, J.; Kirnbauer, R.; Luger, T.A.; Köck, A. Ultraviolet Light Induces Increased Circulating Interleukin–6 in Humans. J. Investig. Dermatol. 1990, 94, 808–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansel, J.C.; Luger, T.A.; Green, I. The Effect of In Vitro and In Vivo UV Irradiation on the Production of ETAF Activity by Human and Murine Keratinocytes. J. Investig. Dermatol. 1983, 81, 519–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, N.; Tohyama, C.; Satoh, M.; Reeve, V. Defective immune response and severe skin damage following UVB irradiation in interleukin-6-deficient mice. Immunology 1999, 97, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Dantzer, R.; Wollman, E.; Vitkovic, L.; Yirmiya, R. Cytokines and depression: Fortuitous or causative association? Mol. Psychiatry 1999, 4, 328–332. [Google Scholar] [CrossRef] [Green Version]
- Licinio, J.; Wong, M.-L. The role of inflammatory mediators in the biology of major depression: Central nervous system cytokines modulate the biological substrate of depressive symptoms, regulate stress–responsive systems, and contribute to neurotoxicity and neuroprotection. Mol. Psychiatry 1999, 4, 317–327. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S.-J. Effects of interleukin–1beta polymorphisms on brain function and behavior in healthy and psychiatric disease conditions. Cytokine Growth Factor Rev. 2017, 37, 89–97. [Google Scholar] [CrossRef]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta–Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Howren, M.B.; Lamkin, D.M.; Suls, J. Associations of Depression With C–Reactive Protein, IL–1, and IL–6: A Meta–Analysis. Psychosom. Med. 2009, 71, 171–186. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Ho, R.C.-M.; Mak, A. Interleukin (IL)–6, tumour necrosis factor alpha (TNF–α) and soluble interleukin–2 receptors (sIL–2R) are elevated in patients with major depressive disorder: A meta–analysis and meta–regression. J. Affect. Disord. 2012, 139, 230–239. [Google Scholar] [CrossRef]
- Bertani, D.E.; De Novellis, A.M.P.; Farina, R.; Latella, E.; Meloni, M.; Scala, C.; Valeo, L.; Galeazzi, G.M.; Ferrari, S. “Shedding Light on Light”: A Review on the Effects on Mental Health of Exposure to Optical Radiation. Int. J. Environ. Res. Public Heal. 2021, 18, 1670. [Google Scholar] [CrossRef] [PubMed]
- Jukic, A.M.Z.; Hoofnagle, A.N.; Lutsey, P.L. Measurement of Vitamin D for Epidemiologic and Clinical Research: Shining Light on a Complex Decision. Am. J. Epidemiol. 2017, 187, 879–890. [Google Scholar] [CrossRef]
- Heck, D.E.; Vetrano, A.M.; Mariano, T.M.; Laskin, J.D. UVB Light Stimulates Production of Reactive Oxygen Species: Unexpected role for catalase. J. Biol. Chem. 2003, 278, 22432–22436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- He, Y.-Y.; Häder, D.-P. Involvement of reactive oxygen species in the UV–B damage to the cyanobacterium Anabaena sp. J. Photochem. Photobiol. B Biol. 2002, 66, 73–80. [Google Scholar] [CrossRef]
- Su, Y.; Wang, S.-B.; Zheng, H.; Tan, W.-Y.; Li, X.; Huang, Z.-H.; Hou, C.-L.; Jia, F.-J. The role of anxiety and depression in the relationship between physical activity and sleep quality: A serial multiple mediation model. J. Affect. Disord. 2021, 290, 219–226. [Google Scholar] [CrossRef]
- Liu, X.; Wang, C.; Qiao, X.; Si, H.; Jin, Y. Sleep quality, depression and frailty among Chinese community–dwelling older adults. Geriatr. Nurs. 2021, 42, 714–720. [Google Scholar] [CrossRef]


{kind=link}
| Comparison | Depression | p-Value | |||
|---|---|---|---|---|---|
| (n = 94,316) | (n = 23,579) | ||||
| Gender | |||||
| Female | 57,884 | (61.37%) | 14,471 | (61.37%) | 1.0000 |
| Male | 36,432 | (38.63%) | 9108 | (38.63%) | |
| Age | |||||
| Mean ± SD | 47.81 ± 16.78 | 47.96 ± 17.03 | 0.2180 | ||
| Low income | |||||
| Yes | 58,336 | (61.85%) | 15,150 | (64.25%) | <0.0001 |
| No | 35,980 | (38.15%) | 8429 | (35.75%) | |
| Urbanization level | |||||
| Highly urbanized | 28,730 | (30.46%) | 7816 | (33.15%) | <0.0001 |
| Moderate urbanization | 28,273 | (29.98%) | 7330 | (31.09%) | |
| Emerging town | 18,369 | (19.48%) | 3684 | (15.62%) | |
| General town | 11,410 | (12.1%) | 2815 | (11.94%) | |
| Aged Township | 1563 | (1.66%) | 398 | (1.69%) | |
| Agricultural town | 2765 | (2.93%) | 806 | (3.42%) | |
| Remote township | 3206 | (3.4%) | 730 | (3.1%) | |
| Comorbidities | |||||
| Diabetes | 11,466 | (12.16%) | 3755 | (15.93%) | <0.0001 |
| Anxiety | 8665 | (9.19%) | 9674 | (41.03%) | <0.0001 |
| Cushing’s disease | 50 | (0.05%) | 30 | (0.13%) | <0.0001 |
| Parkinson’s disease | 723 | (0.77%) | 533 | (2.26%) | <0.0001 |
| Alzheimer’s disease | 263 | (0.28%) | 222 | (0.94%) | <0.0001 |
| Coronary heart disease | 8568 | (9.08%) | 3319 | (14.08%) | <0.0001 |
| Breast cancer | 689 | (0.73%) | 256 | (1.09%) | <0.0001 |
| Human immunodeficiency virus | 41 | (0.04%) | 58 | (0.25%) | <0.0001 |
| Comparison | Depression | Two-Tailed Test p-Value | Chi-Square p-Value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (%) | Average Monthly UVB Exposure (UVI) | N (%) | Average Monthly UVB Exposure (UVI) | |||||||||||
| Mean (SD) | Q1 | Median | Q3 | Mean (SD) | Q1 | Median | Q3 | |||||||
| Total participants Ultra–violet Index WHO standard level | ||||||||||||||
| Low level | 87,700 | (92.99%) | 1.37 (0.26) | 1.21 | 1.29 | 1.53 | 21,486 | (32.65%) | 1.43 (0.28) | 1.22 | 1.38 | 1.56 | <0.0001 | <0.0001 |
| Moderate level | 3937 | (4.17%) | 4.60 (0.73) | 3.99 | 4.67 | 5.16 | 1236 | (5.91%) | 4.51 (0.80) | 3.88 | 4.60 | 5.11 | ||
| High level | 1223 | (1.3%) | 6.86 (0.55) | 6.45 | 6.82 | 7.23 | 381 | (2.78%) | 6.88 (0.57) | 6.45 | 6.87 | 7.31 | ||
| Very high level | 763 | (0.81%) | 9.20 (0.81) | 8.51 | 9.16 | 9.69 | 246 | (2.43%) | 9.32 (0.84) | 8.54 | 9.40 | 10.00 | ||
| Extreme level | 693 | (0.73%) | 13.87 (2.14) | 12.02 | 13.63 | 15.15 | 230 | (3.39%) | 13.91 (2.31) | 12.09 | 13.40 | 15.15 | ||
| Observed | Incidence Density (95% CI) | Adjusted IRR (95%CI) | |
|---|---|---|---|
| Person-Months | Per 100 Person-Months | ||
| UVB WHO level (reference: Low level) | |||
| Low level | 866,325 | 2.48 (2.47–2.49) | Reference |
| Moderate level | 66,201 | 1.87 (1.84–1.89) | 0.889 (0.835–0.947) |
| High level | 15,396 | 2.47 (2.44–2.51) | 1.134 (1.022–1.260) |
| Very high level | 6845 | 3.59 (3.53–3.66) | 1.711 (1.505–1.945) |
| Extreme level | 4112 | 5.59 (5.47–5.73) | 2.785 (2.439–3.180) |
| Low-income (reference: No) | |||
| Yes | 613,820 | 2.47 (2.45–2.48) | 1.080 (1.052–1.110) |
| No | 345,059 | 2.44 (2.42–2.46) | Reference |
| Urbanization level (reference: Highly urbanized) | |||
| Highly urbanized | 309,804 | 2.52 (2.50–2.55) | Reference |
| Moderate urbanization | 297,639 | 2.46 (2.44–2.48) | 0.891 (0.863–0.920) |
| Emerging town | 151,564 | 2.43 (2.40–2.46) | 0.733 (0.705–0.762) |
| General town | 118,742 | 2.37 (2.34–2.40) | 0.799 (0.764–0.835) |
| Aged Township | 16,233 | 2.45 (2.36–2.55) | 0.839 (0.756–0.931) |
| Agricultural town | 33,880 | 2.38 (2.32–2.44) | 0.892 (0.824–0.966) |
| Remote township | 31,017 | 2.35 (2.29–2.42) | 0.748 (0.693–0.808) |
| Comorbidities (reference: without) | |||
| Diabetes | 156,293 | 2.40 (2.37–2.43) | 1.138 (1.096–1.181) |
| Anxiety | 398,918 | 2.43 (2.41–2.44) | 3.685 (3.587–3.785) |
| Cushing’s disease | 1169 | 2.57 (2.23–3.01) | 1.374 (0.960–1.966) |
| Parkinson’s disease | 21,716 | 2.45 (2.38–2.54) | 1.648 (1.509–1.799) |
| Alzheimer’s disease | 9631 | 2.31 (2.20–2.42) | 1.685 (1.473–1.927) |
| Coronary heart disease | 132,622 | 2.50 (2.47–2.54) | 1.205 (1.159–1.254) |
| Breast cancer | 10,417 | 2.46 (2.35–2.57) | 1.280 (1.131–1.449) |
| Human immunodeficiency virus | 2458 | 2.36 (2.16–2.60) | 2.283 (1.763–2.955) |
| UVB WHO Level (Reference: Low Level) | ||||
|---|---|---|---|---|
| Adjusted IRR (95%CI) | ||||
| Moderate Level | High Level | Very High Level | Extreme Level | |
| Gender | ||||
| Female | 0.885 (0.816–0.959) | 1.030 (0.896–1.184) | 1.697 (1.439–2.000) | 2.825 (2.381–3.352) |
| Male | 0.899 (0.814–0.993) | 1.305 (1.113–1.531) | 1.731 (1.411–2.123) | 2.749 (2.227–3.393) |
| Low income | ||||
| Yes | 0.888 (0.817–0.966) | 1.120 (0.968–1.297) | 1.823 (1.529–2.174) | 2.780 (2.300–3.359) |
| No | 0.884 (0.805–0.972) | 1.153 (0.992–1.340) | 1.593 (1.321–1.921) | 2.808 (2.331–3.383) |
| Urbanization level | ||||
| Highly urbanized | ||||
| Yes | – | – | – | – |
| No | 0.895 (0.844–0.949) | 1.151 (1.040–1.275) | 1.742 (1.536–1.976) | 2.828 (2.482–3.223) |
| Comorbidities | ||||
| Diabetes | ||||
| Yes | 0.881 (0.765–1.015) | 1.17 (0.917–1.494) | 1.639 (1.204–2.231) | 2.683 (1.971–3.652) |
| No | 0.887 (0.827–0.951) | 1.122 (0.999–1.26) | 1.730 (1.503–1.993) | 2.828 (2.441–3.276) |
| Anxiety | ||||
| Yes | 0.804 (0.730–0.885) | 1.159 (0.999–1.344) | 1.699 (1.407–2.052) | 2.821 (2.323–3.426) |
| No | 0.956 (0.881–1.038) | 1.118 (0.964–1.296) | 1.734 (1.457–2.065) | 2.806 (2.339–3.365) |
| Cushing’s disease | ||||
| Yes | 0.792 (0.122–5.16) | – | – | 2.245 (0.094–53.642) |
| No | 0.889 (0.835–0.947) | 1.138 (1.025–1.264) | 1.717 (1.511–1.952) | 2.781 (2.435–3.177) |
| Parkinson’s disease | ||||
| Yes | 0.728 (0.501–1.06) | 1.017 (0.585–1.77) | 1.062 (0.38–2.97) | 2.157 (1.179–3.945) |
| No | 0.896 (0.84–0.954) | 1.139 (1.024–1.268) | 1.727 (1.518–1.965) | 2.844 (2.482–3.259) |
| Alzheimer’s disease | ||||
| Yes | 0.623 (0.357–1.088) | 0.803 (0.343–1.879) | 1.274 (0.436–3.725) | – |
| No | 0.895 (0.84–0.953) | 1.142 (1.027–1.269) | 1.714 (1.506–1.95) | 2.788 (2.441–3.184) |
| Coronary heart disease | ||||
| Yes | 0.824 (0.707–0.960) | 1.078 (0.830–1.400) | 1.727 (1.294–2.304) | 2.108 (1.479–3.004) |
| No | 0.901 (0.841–0.965) | 1.137 (1.015–1.275) | 1.701 (1.474–1.962) | 2.929 (2.538–3.381) |
| Breast cancer | ||||
| Yes | 0.933 (0.43–2.023) | – | 1.058 (0.243–4.598) | 4.894 (1.414–16.936) |
| No | 0.889 (0.835–0.947) | 1.140 (1.026–1.266) | 1.717 (1.509–1.952) | 2.770 (2.424–3.165) |
| Human immunodeficiency virus | ||||
| Yes | 0.536 (0.071–4.070) | – | 9.134 (1.196–69.763) | 5.557 (0.161–191.663) |
| No | 0.889 (0.835–0.947) | 1.134 (1.021–1.259) | 1.709 (1.503–1.943) | 2.777 (2.431–3.172) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luo, C.-W.; Chen, S.-P.; Chiang, C.-Y.; Wu, W.-J.; Chen, C.-J.; Chen, W.-Y.; Kuan, Y.-H. Association between Ultraviolet B Exposure Levels and Depression in Taiwanese Adults: A Nested Case–Control Study. Int. J. Environ. Res. Public Health 2022, 19, 6846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116846
Luo C-W, Chen S-P, Chiang C-Y, Wu W-J, Chen C-J, Chen W-Y, Kuan Y-H. Association between Ultraviolet B Exposure Levels and Depression in Taiwanese Adults: A Nested Case–Control Study. International Journal of Environmental Research and Public Health. 2022; 19(11):6846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116846
Chicago/Turabian StyleLuo, Ci-Wen, Shih-Pin Chen, Chen-Yu Chiang, Wen-Jun Wu, Chun-Jung Chen, Wen-Ying Chen, and Yu-Hsiang Kuan. 2022. "Association between Ultraviolet B Exposure Levels and Depression in Taiwanese Adults: A Nested Case–Control Study" International Journal of Environmental Research and Public Health 19, no. 11: 6846. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116846