
Results of a Qualitative Study Aimed at Building a Programme to Reduce Cardiovascular Risk in People with Severe Mental Illness

 ,
, {kind=link}
Abstract
:1. Background
2. Methods
2.1. COPsyCAT General Study Design
2.2. Design of the Qualitative Exploratory Study
2.3. Participant Recruitment
2.3.1. Patient Recruitment
2.3.2. Carer Recruitment
2.3.3. Psychiatric Health Professional and Primary Care Provider Recruitment
2.3.4. Inclusion Criteria
- For all participants:
- -
- Over 18 years old.
- -
- Consent to participate.
- Patients using psychiatric services:
- -
- PSMI followed in an inpatient or outpatient setting.
- Carers
- -
- Providing support to a PSMI with a long-term mental condition.
- -
- Consent needed from the PSMI receiving support.
- Psychiatric health professionals:
- -
- Psychiatrist or nurse working in a hospital or in a private setting.
- Primary care providers:
- -
- General practitioner, nurse, dietician, or pharmacist following at least one PSMI.
2.3.5. Exclusion Criteria
- For all participants:
- -
- Inability to participate in an FG for physical or psychological reasons.
- -
- Not affiliated with France’s health insurance system.
- -
- Under legal protection.
- -
- Pregnant, parturient or breastfeeding.
- -
- Did not speak or understand French.
2.4. Data Collection
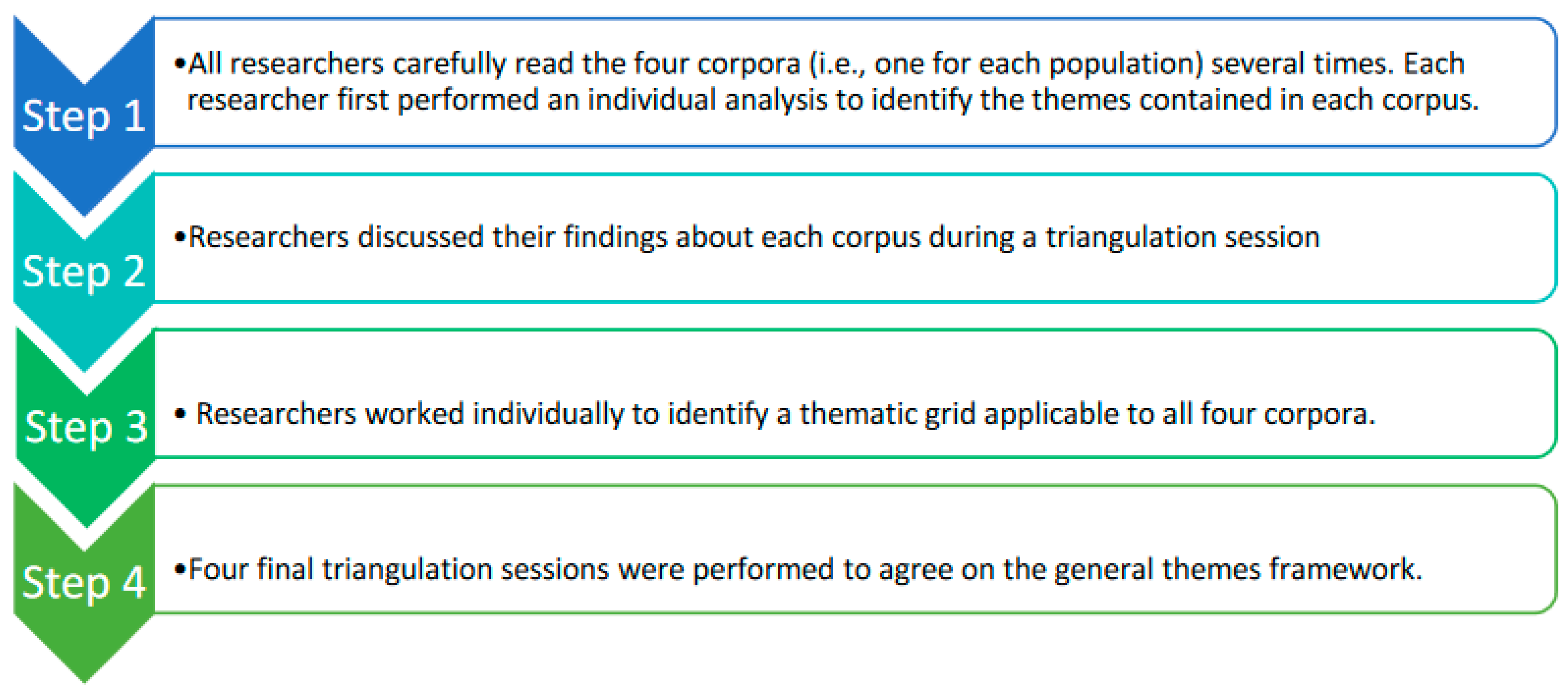
2.5. Analysis
3. Results
3.1. Description of Participants
3.1.1. Users of Psychiatric Services
3.1.2. Carers
3.1.3. Psychiatric Professionals
3.1.4. Primary Care Providers
3.2. Presentation of Themes
3.2.1. Theme 1—Communication
“Yes, communication, that’s it; what’s missing is communication, but the truth is, it’s up to us to create it.”Psychiatric Professional
Unfortunately, for most patients, we don’t know, we don’t have the diagnoses (…) we have to go and fish a bit for the information. And even if the doctors want to, it’s again a question of the time [needed to send us information]. There are many things that hinder communication between us and them. When we have very important concerns, we phone, but for the most part we now just try to send emails.”Primary care provider
“I think that we spend our time looking for information, especially with our patients. Therefore, I think it [shared patient medical record] would save time, a lot of time, because we have to call the secretary.”Psychiatric professional
“We don’t need to know the details. What we’re interested in is the pathologies (…) that the pathology is identified. Really, [having] a shared medical record would be a complete change in the relationship between all the professionals. The aim is for everyone to have access to the minimum amount of information they need.”Primary care provider
“(…) when you have cancer, the doctors hold multidisciplinary consultation meetings. (…) That is to say, no treatment is done without a whole bunch of specialists around the table saying ‘We’re going to do this’ and ‘We’re not going to do that’; they measure, they weigh up, they give the pros and the cons’, etc. I mean, there are enormous resources. (…) But for our relatives, it’s: “I’ll try this for you, oh that’ll make you fat, but well, it’s not serious”.Carer
“I think that there should be more exchanges between doctors: Between psychiatrists and general practitioners, there should be exchanges, because at the end of the day, when we go to see the general practitioner, he’s not up to speed with everything, he asks us questions.”User of psychiatric services
3.2.2. Theme 2—Information
“So I think I’m going to go back. I was waiting to see if it would be reimbursed, because at that time it wasn’t. But now [it is reimbursed so] that’s good.”User of psychiatric services
“It took me four years to find out that there was a training programme for families and I only found out in October. It was supposed to start in September. It’s true that I waited [before looking for information]. They told me: “No, you have to wait until next year.”Carer
“There is the same thing in B.; they do cooking, eating behaviour, etc. It’s very interesting and it is not expensive (…). They have more and more requests [for this] but it’s from people who already know about it. It’s not the same. It’s not necessarily the people that need it the most who have the information. (…) likewise, we need to be informed, we are not necessarily informed.”Primary care provider
“I don’t have a brochure of the medical-psychological centre that shows me the pathway…. D. tells me that there is a dietician at the medical-psychological centre. I don’t know anything about it actually because… because… yes, I didn’t look for information.”Primary care provider
“(…) We invited all the general practitioners. There’s not a lot of them. We invited them to show them the services we offer, to present what we do, to talk about how you get to the medical-psychological centre, the reality on the ground…”Psychiatric professional
“Without discrimination, (…) without prescription, it needs to be a bit automatic. It must become natural to systematically talk about metabolic risk in the [psychiatric health] services, whether services are open or closed [i.e., patients cannot leave the premises], whether patients have good cognitive efficiency or not, and whatever the severity of their illness.”Psychiatric professional
“(…) If you screen for cardiovascular risks in schizophrenics, maybe you should do like you do for the general population…, I don’t know, we have screening for breast cancer at 50, screening for colon cancer, etc. Perhaps, we should do a more global cardiovascular risk campaign for vulnerable people…”Psychiatric professional
3.2.3. Theme 3—Training
“It’s difficult. I don’t know how to talk about it [mental disorder]. It would be nice to have more training about that, which is done (…) through talking with other people. I’d like that a lot. It would make me feel better.”User
Primary care providers expressed a lack of knowledge about mental disorders and their desire to learn how to manage them:
“There’s a big population of people who aren’t well [i.e., with mental disorders], but I don’t think they’re all the same.”
“As a pharmacist, I don’t necessarily have a global vision of the person’s pathology when I receive a prescription.”
“I admit that I’m really interested. I know a bit about psychiatry, but in private practice, you’re a little afraid of their behaviours, precisely because of a lack of knowledge.”Primary care provider
“First, we need to train general practitioners in psychiatry so they can provide better follow-up to our patients”Psychiatric professional
“It would be perfect to (…) you prescribe a certain medicine, and you have a dedicated protocol.”Psychiatric professional
3.2.4. Theme 4—Support
“Yes, going to several [group-based activities] is motivating. I’m alone, at home. I’m reluctant to go walking because I’m alone. If I had support, maybe I would feel more motivated.”User
“(…) we each have a different disease. But we live very well with it. Every once in a while, you need to talk about it, sometimes just briefly, just five minutes, because it brings you back into line a little.”User
“When you get older—I mean, I think that I’m getting quite a bit older—I think you’d like someone to take over because you’re not here forever; you get older, you get tired and… You’d like to be helped more. We shouldn’t leave parents or carers like that.”Carer
“They would need stimulants and full-time educators, because, right, we trained ourselves, but we’re also emotional; we’re tired because we’re all alone; we’re isolated. When there’s a crisis to manage we’re all alone, there’s no help at time t. [I dream of] an ideal place, where he [her son] would be stimulated right from the start of the day with a good breakfast, and then we could go for a walk…”Carer
“(…) so they come, either with a nurse or with an educator or with a peer-health workers. That’s kind of gone now, but we used to have that, and it allowed us to at least be able to say ‘you need to go to the cardiologist’, and the peer-health worker would have helped to bring them. Like the educators can do to help them come to our office.”Primary care provider
“Above all, they need to be with someone, they’re so alone all the time; the times when they’re scared, [the times when] they go to have a medical exam or [when] they’re going to be given results that they might not be able to understand…”Psychiatric professional
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- L’etat de La Santé de La Popultion En France; Direction de la recherche de l’Evaluation des Etudes et des Statistiques: Paris, France, 2015.
- Wells, J.; Kennedy, C.; Bain, H.; Lee, S.H. The Experiences of Older Adults with a Diagnosed Functional Mental Illness, Their Carers and Healthcare Professionals in Relation to Mental Health Service Delivery: An Integrative Review. J. Clin. Nurs. 2020, 29, 31–52. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; Sullivan, L.M.; McEvoy, J.P.; Meyer, J.M.; Nasrallah, H.A.; Daumit, G.L.; Lamberti, S.; D’Agostino, R.B.; Stroup, T.S.; Davis, S.; et al. A Comparison of Ten-Year Cardiac Risk Estimates in Schizophrenia Patients from the CATIE Study and Matched Controls. Schizophr. Res. 2005, 80, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Gerhard, T.; Huang, C.; Crystal, S.; Stroup, T.S. Premature Mortality among Adults with Schizophrenia in the United States. JAMA Psychiatry 2015, 72, 1172–1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saha, S.; Chant, D.; McGrath, J. A Systematic Review of Mortality in Schizophrenia: Is the Differential Mortality Gap Worsening over Time? Arch. Gen. Psychiatry 2007, 64, 1123–1131. [Google Scholar] [CrossRef]
- Stanley, S.; Laugharne, J. The Impact of Lifestyle Factors on the Physical Health of People with a Mental Illness: A Brief Review. Int. J. Behav. Med. 2014, 21, 275–281. [Google Scholar] [CrossRef]
- Scott, D.; Happell, B. The High Prevalence of Poor Physical Health and Unhealthy Lifestyle Behaviours in Individuals with Severe Mental Illness. Issues Ment. Health Nurs. 2011, 32, 589–597. [Google Scholar] [CrossRef]
- Callaghan, R.C.; Veldhuizen, S.; Jeysingh, T.; Orlan, C.; Graham, C.; Kakouris, G.; Remington, G.; Gatley, J. Patterns of Tobacco-Related Mortality among Individuals Diagnosed with Schizophrenia, Bipolar Disorder, or Depression. J. Psychiatr. Res. 2014, 48, 102–110. [Google Scholar] [CrossRef]
- Codony, M.; Alonso, J.; Almansa, J.; Bernert, S.; de Girolamo, G.; de Graaf, R.; Haro, J.M.; Kovess, V.; Vilagut, G.; Kessler, R.C. Perceived Need for Mental Health Care and Service Use among Adults in Western Europe: Results of the ESEMeD Project. Psychiatr. Serv. 2009, 60, 1051–1058. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Mittal, D.; Reaves, C.M.; Haynes, T.F.; Han, X.; Morris, S.; Sullivan, G. Mental Health Stigma and Primary Health Care Decisions. Psychiatry Res. 2014, 218, 35–38. [Google Scholar] [CrossRef] [Green Version]
- Recommandation de Bonne Pratique en Psychiatrie: Comment Améliorer la Prise en Charge Somatique des Patients Ayant Une Pathologie Psychiatrique Sévère et Chronique; Fédération Française de Psychiatrie: Paris, France, 2015; p. 32.
- Druss, B.G.; Rohrbaugh, R.M.; Levinson, C.M.; Rosenheck, R.A. Integrated Medical Care for Patients with Serious Psychiatric Illness: A Randomized Trial. Arch. Gen. Psychiatry 2001, 58, 861–868. [Google Scholar] [CrossRef]
- Santé, O. Mondiale de la Plan D’action Global Pour La Santé Mentale 2013–2020; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- United Nations. Resolution Adopted by the General Assembly on 25 September 2015 70/1. Transforming Our World: The 2030 Agenda for Sustainable Development—A/RES/70/1; United Nations General Assembly: New York, NY, USA, 2015. [Google Scholar]
- Shanghai Declaration on Promoting Health in the 2030 Agenda for Sustainable Development. In Proceedings of the 9th Global Conference on Health Pormotion, Shanghai, China, 21–24 November 2016.
- Kokorelias, K.M.; Gignac, M.A.M.; Naglie, G.; Cameron, J.I. Towards a Universal Model of Family Centered Care: A Scoping Review. BMC Health Serv. Res. 2019, 19, 564. [Google Scholar] [CrossRef] [PubMed]
- Brodaty, H.; Donkin, M. Family Caregivers of People with Dementia. Dialogues Clin. Neurosci. 2009, 11, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Leischik, R.; Dworrak, B.; Strauss, M.; Przybylek, B.; Schöne, D.; Horlitz, M.; Mügge, A.; Dworrak, T. Plasticity of Health. Ger. J. Med. 2016, 1, 1–17. [Google Scholar] [CrossRef]
- Musacchio, N.; Lovagnini Scher, A.; Giancaterini, A.; Pessina, L.; Salis, G.; Schivalocchi, F.; Nicolucci, A.; Pellegrini, F.; Rossi, M.C.E. Impact of a Chronic Care Model Based on Patient Empowerment on the Management of Type 2 Diabetes: Effects of the SINERGIA Programme. Diabet. Med. J. Br. Diabet. Assoc. 2011, 28, 724–730. [Google Scholar] [CrossRef]
- Halabi, I.O.; Scholtes, B.; Voz, B.; Gillain, N.; Durieux, N.; Odero, A.; Baumann, M.; Ziegler, O.; Gagnayre, R.; Guillaume, M.; et al. “Patient Participation” and Related Concepts: A Scoping Review on Their Dimensional Composition. Patient Educ. Couns. 2020, 103, 5–14. [Google Scholar] [CrossRef]
- Papathanasiou, J.; Troev, T.; Ferreira, A.S.; Tsekoura, D.; Elkova, H.; Kyriopoulos, E.; Ilieva, E. Advanced Role and Field of Competence of the Physical and Rehabilitation Medicine Specialist in Contemporary Cardiac Rehabilitation. Hell. J. Cardiol. HJC Hell. Kardiologike Epitheorese 2016, 57, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Çelik Ince, S.; Partlak Günüşen, N.; Serçe, Ö. Perception of Physical Health by Patients with Severe Mental Illness and Their Family Caregivers: A Qualitative Study. Perspect. Psychiatr. Care 2019, 55, 718–727. [Google Scholar] [CrossRef]
- van Hasselt, F.M.; Oud, M.J.T.; Loonen, A.J.M. Improvement of Care for the Physical Health of Patients with Severe Mental Illness: A Qualitative Study Assessing the View of Patients and Families. BMC Health Serv. Res. 2013, 13, 426. [Google Scholar] [CrossRef] [Green Version]
- Happell, B.; Wilson, K.; Platania-Phung, C.; Stanton, R. Physical Health and Mental Illness: Listening to the Voice of Carers. J. Ment. Health 2017, 26, 127–133. [Google Scholar] [CrossRef]
- Butler, J.; de Cassan, S.; Turner, P.; Lennox, B.; Hayward, G.; Glogowska, M. Attitudes to Physical Healthcare in Severe Mental Illness; a Patient and Mental Health Clinician Qualitative Interview Study. BMC Fam. Pract. 2020, 21, 243. [Google Scholar] [CrossRef]
- Clancy, R.; Lewin, T.J.; Bowman, J.A.; Kelly, B.J.; Mullen, A.D.; Flanagan, K.; Hazelton, M.J. Providing Physical Health Care for People Accessing Mental Health Services: Clinicians’ Perceptions of Their Role. Int. J. Ment. Health Nurs. 2019, 28, 256–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, S.; Heinkel, S.; Burton, A.; Blackburn, R.; McCloud, T.; Ross, J.; Osborn, D.; Walters, K. A Qualitative Study Exploring the Barriers and Facilitators of Implementing a Cardiovascular Disease Risk Reducing Intervention for People with Severe Mental Illness into Primary Care Contexts across England: The “PRIMROSE” Trial. BMC Health Serv. Res. 2020, 20, 753. [Google Scholar] [CrossRef] [PubMed]
- Baleige, A.; Besnard, J.-F.; Meunier-Beillard, N.; Demassiet, V.; Monnier, A.; Ouezini, A.; Lambert, O.; Charrel, C.; Mazas, O.; Oberlin, J.; et al. A Collaboration between Service Users and Professionals for the Development and Evaluation of a New Program for Cardiovascular Risk Management in Persons with a Diagnosis of Severe Mental Illness: French Multicenter Qualitative and Feasibility Studies. Int. J. Ment. Health Syst. 2019, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Paillé, P.; Mucchielli, A. Chapitre 11—L’analyse thématique. In L’analyse Qualitative en Sciences Humaines et Sociales; Armand Colin: Paris, France, 2012; pp. 231–314. ISBN 978-2-200-24904-5. [Google Scholar]
- Pullen, I.M.; Yellowless, A.J. Is Communication Improving between General Practitioners and Psychiatrists? Br. Med. J. Clin. Res. Ed 1985, 290, 31–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milleret, G.; Benradia, I.; Guicherd, W.; Roelandt, J.-L. National Action Research “The Place of Mental Health in General Practice”. Inf. Psychiatr. 2014, 90, 311–317. [Google Scholar]
- Merlière, Y. The shared medical record, a digital health record for all. Soins Rev. Ref. Infirm. 2020, 65, 29–32. [Google Scholar] [CrossRef]
- Saberi, P.; Catz, S.L.; Leyden, W.A.; Stewart, C.; Ralston, J.D.; Horberg, M.A.; Grothaus, L.; Silverberg, M.J. Antiretroviral Therapy Adherence and Use of an Electronic Shared Medical Record among People Living with HIV. AIDS Behav. 2015, 19 (Suppl. 2), 177–185. [Google Scholar] [CrossRef]
- Abed, R.; Teodorczuk, A. Danger Ahead: Challenges in Undergraduate Psychiatry Teaching and Implications for Community Psychiatry. Br. J. Psychiatry J. Ment. Sci. 2015, 206, 89–90. [Google Scholar] [CrossRef] [Green Version]
- Piot, M.-A.; Dechartres, A.; Attoe, C.; Jollant, F.; Lemogne, C.; Layat Burn, C.; Rethans, J.-J.; Michelet, D.; Cross, S.; Billon, G.; et al. Simulation in Psychiatry for Medical Doctors: A Systematic Review and Meta-Analysis. Med. Educ. 2020, 54, 696–708. [Google Scholar] [CrossRef]
- Lang, J.-P.; Jurado, N.; Herdt, C.; Sauvanaud, F.; Lalanne Tongio, L. Education care in patients with psychiatric disorders in France: Psychoeducation or therapeutic patient education? Rev. Epidemiol. Sante Publique 2019, 67, 59–64. [Google Scholar] [CrossRef]
- Lequimener-de Lorgeril, V.; Chirio-Espitalier, M.; Grall-Bronnec, M. Influence of a therapeutic patient education (TPE) program on quality of life in bipolar disorder: Preliminary results. L’Encephale 2019, 45, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.M.; Tribe, R.H.; Stott, J.C.H.; Pilling, S. Open Dialogue: A Review of the Evidence. Psychiatr. Serv. 2019, 70, 46–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- von Peter, S.; Aderhold, V.; Cubellis, L.; Bergström, T.; Stastny, P.; Seikkula, J.; Puras, D. Open Dialogue as a Human Rights-Aligned Approach. Front. Psychiatry 2019, 10, 387. [Google Scholar] [CrossRef] [PubMed]
- Hude, W.; Pinet, E. Les Médiateurs de Santé Pair: Une Profession En Devenir. Inf. Psychiatr. 2020, 96, 527–532. [Google Scholar]
- CCOMS Programme «Médiateur de Santé/Pair». Available online: https://www.solidarites-usagerspsy.fr/s-engager/les-pairs-aidants/les-mediateurs-de-sante-pairs-en-france/ (accessed on 2 June 2022).
- Stępnicki, P.; Kondej, M.; Kaczor, A.A. Current Concepts and Treatments of Schizophrenia. Molecules 2018, 23, 2087. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa, M.; Meunier-Beillard, N.; Guillermet, E.; Cros, L.; Demassiet, V.; Hude, W.; Baleige, A.; Besnard, J.-F.; Roelandt, J.-L.; Denis, F. Results of a Qualitative Study Aimed at Building a Programme to Reduce Cardiovascular Risk in People with Severe Mental Illness. Int. J. Environ. Res. Public Health 2022, 19, 6847. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116847
Costa M, Meunier-Beillard N, Guillermet E, Cros L, Demassiet V, Hude W, Baleige A, Besnard J-F, Roelandt J-L, Denis F. Results of a Qualitative Study Aimed at Building a Programme to Reduce Cardiovascular Risk in People with Severe Mental Illness. International Journal of Environmental Research and Public Health. 2022; 19(11):6847. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116847
Chicago/Turabian StyleCosta, Marie, Nicolas Meunier-Beillard, Elise Guillermet, Lucie Cros, Vincent Demassiet, Wendy Hude, Anna Baleige, Jean-François Besnard, Jean-Luc Roelandt, and Frédéric Denis. 2022. "Results of a Qualitative Study Aimed at Building a Programme to Reduce Cardiovascular Risk in People with Severe Mental Illness" International Journal of Environmental Research and Public Health 19, no. 11: 6847. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19116847