
Modified Osteotome Sinus Floor Elevation Technique for Multiple Edentulous Spaces: A Non-Randomized Controlled Trial


Abstract
:1. Introduction
2. Methods and Materials
2.1. Patients’ Characteristics
2.2. Inclusion and Exclusion Criteria
- Partially edentulous patients at the maxillary posterior region, including the second premolar and first and second molar sites requiring dental implants.
- Bone width at the bony crest level sufficient to allow the insertion of regular-diameter (4.1 mm) and wide-diameter (4.8 mm) dental implants maintaining at least 1.0 mm of buccal and lingual bone. This requires at least 6–7 mm bone width at the bony crest level.
- Those with RBH in dentition defect area less than 5 mm should be included into modified OSFE group.
- Those with RBH in dentition defect area more than 5 mm should be included into traditional OSFE group.
- Patients with serious diseases (e.g., cardiovascular and cerebrovascular diseases, liver or kidney diseases).
- Patients who underwent major operations in recent 3 years.
- Patients with blood system diseases (e.g., blood coagulation disorder, anemia, the increase or decrease in leukocyte count or thrombocytopenia).
- Patients with diabetes, osteoporosis, hypertension, hyperthyroidism, rheumatism, allergies to medications or food.
- Female patients in menstrual period or pregnancy.
- Heavy smokers (more than 20 cigarettes daily).
- Patients with symptoms of sinus disease (e.g., maxillary sinusitis, antracele).
- Poor compliance, without regular subsequent visit.
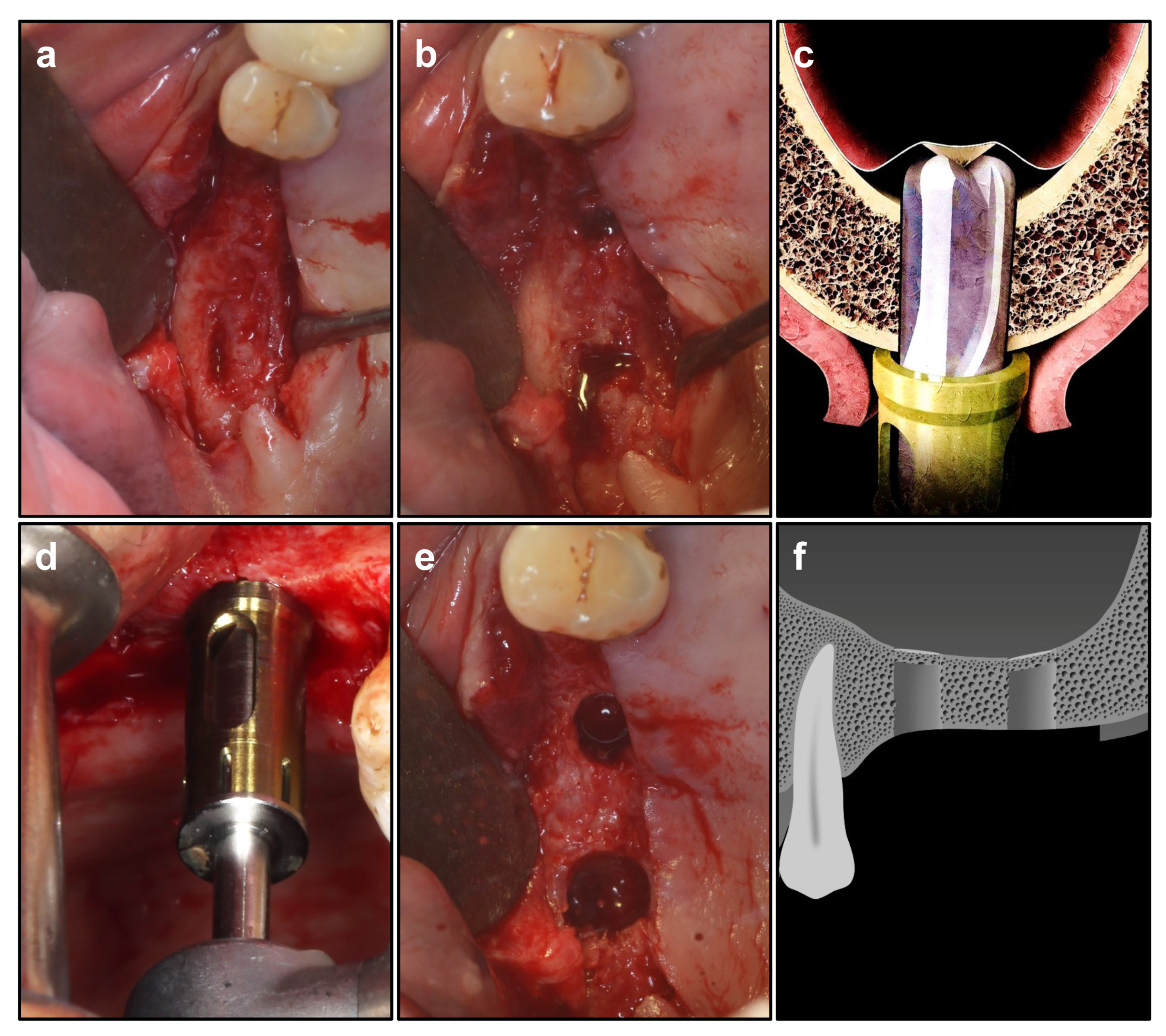
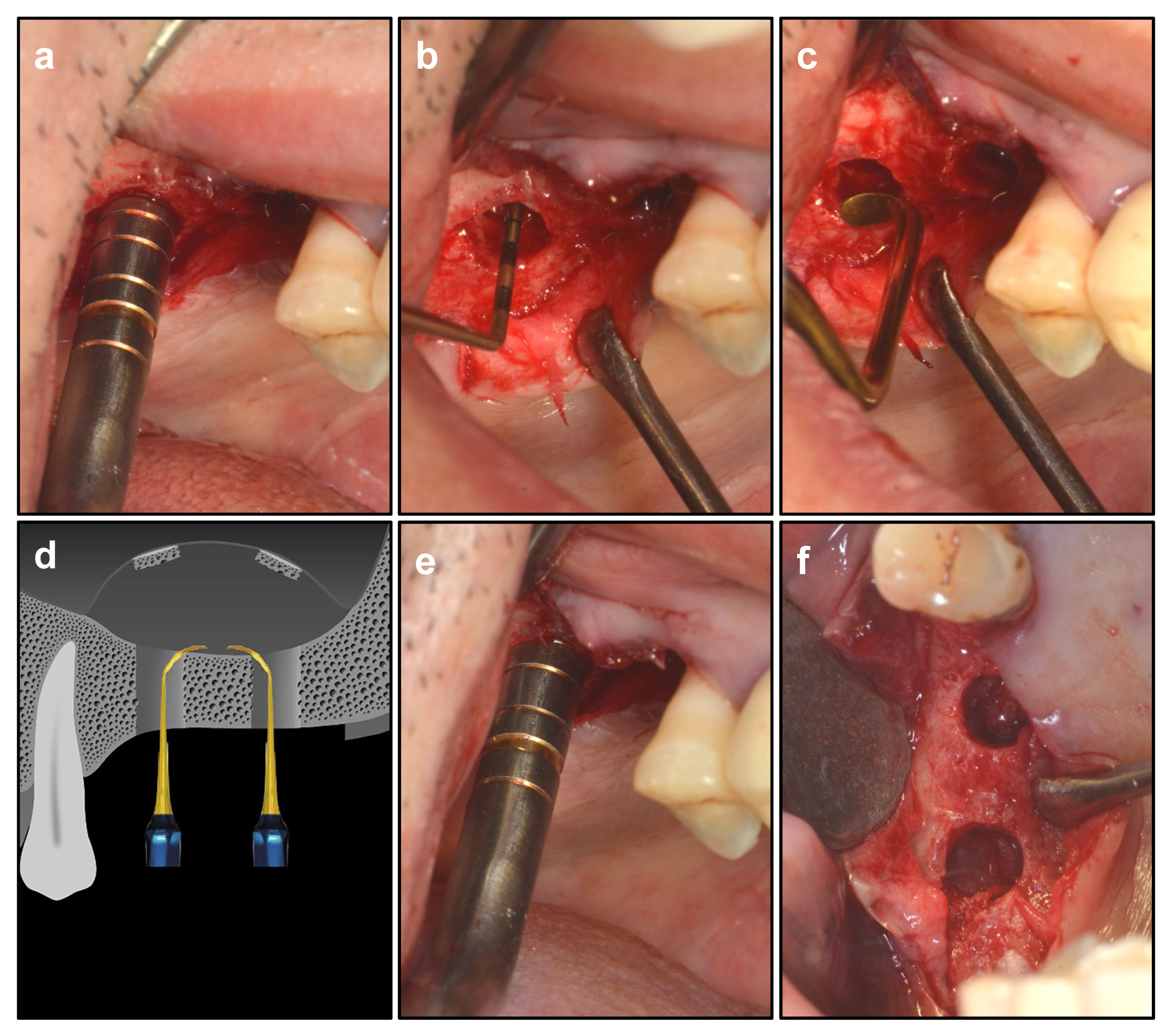
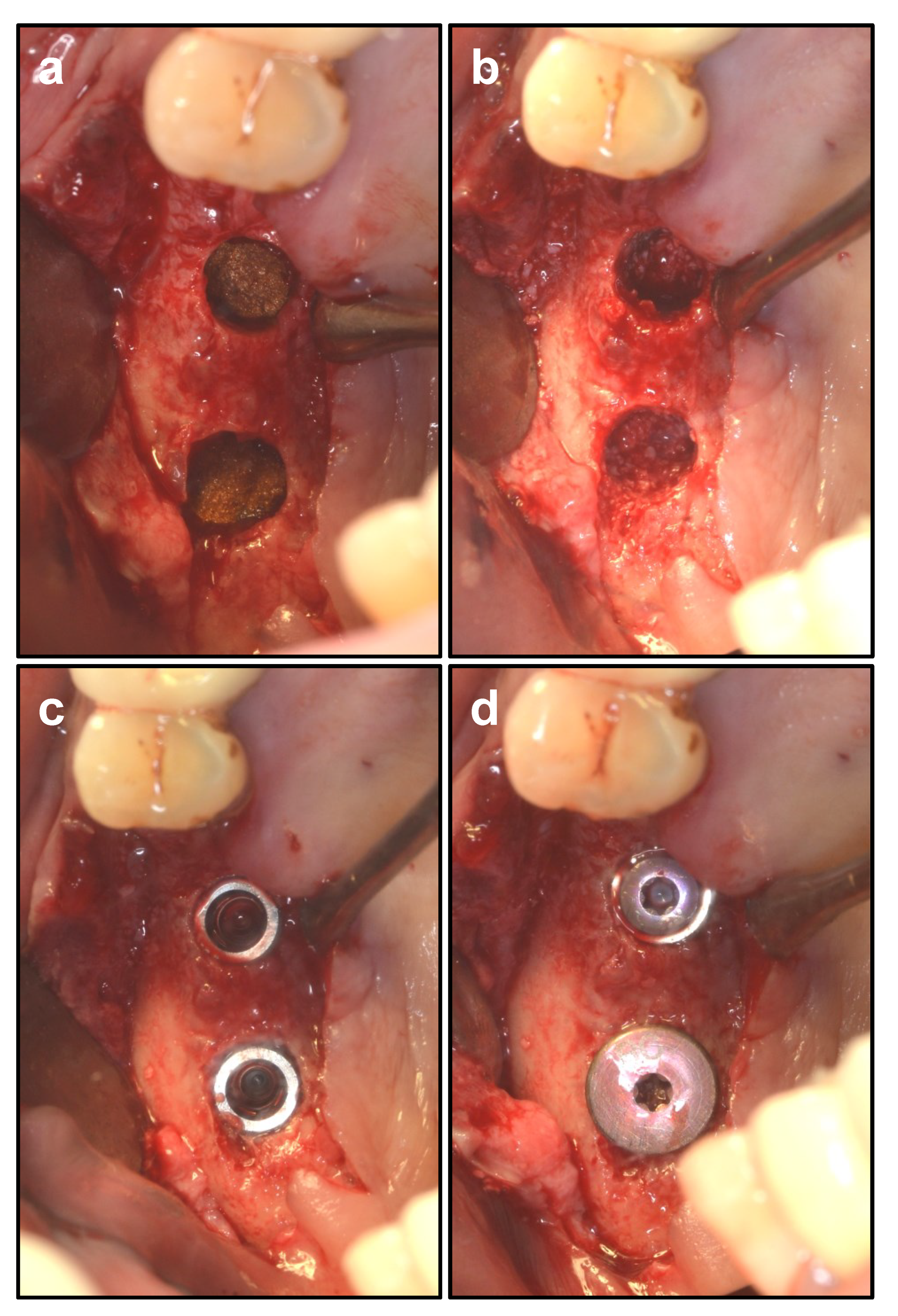
2.3. Surgical Procedure of Modified OSFE
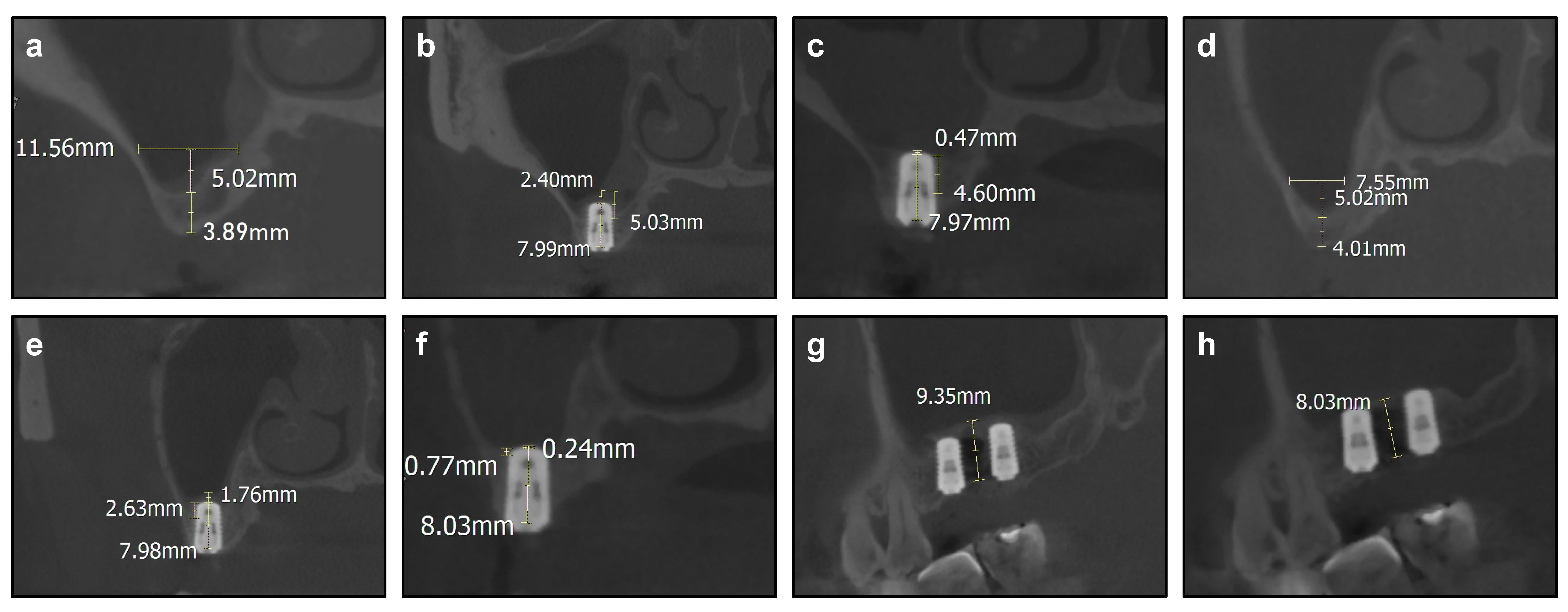
2.4. Cone-Beam Computed Tomography Evaluations
2.5. Statistical Analyses
3. Results
4. Discussion
4.1. Analysis of the Outcomes via Modified OSFE
4.2. Technique Essentials of Modified OSFE
4.3. Innovations and Advantages in Modified OSFE
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abi Najm, S.; Nurdin, N.; El Hage, M.; Bischof, M.; Nedir, R. Osteotome sinus floor elevation without grafting: A 10-year clinical and cone-beam sinus assessment. Implant Dent. 2018, 27, 1. [Google Scholar] [CrossRef] [PubMed]
- Niu, L.; Wang, J.; Yu, H.; Qiu, L. New classification of maxillary sinus contours and its relation to sinus floor elevation surgery. Clin. Implant Dent. Relat. Res. 2018, 20, 493–500. [Google Scholar] [CrossRef]
- Chiapasco, M.; Casentini, P.; Zaniboni, M. Bone augmentation procedures in implant dentistry. Int. J. Oral Maxillofac. Implant. 2009, 24, 237. [Google Scholar]
- O’Valle, F.; de Buitrago, J.; Hernández-Cortés, P.; Padial-Molina, M.; Crespo-Lora, V.; Cobo, M.; Aguilar, D.; Galindo-Moreno, P. Increased expression of musashi-1 evidences mesenchymal repair in maxillary sinus floor elevation. Sci. Rep. 2018, 8, 12243. [Google Scholar] [CrossRef] [PubMed]
- Hallman, M.; Sennerby, L.; Lundgren, S. A clinical and histologic evaluation of implant integration in the posterior maxilla after sinus floor augmentation with autogenous bone, bovine hydroxyapatite, or a 20:80 mixture. Int. J. Oral Maxillofac. Implant. 2002, 17, 635–643. [Google Scholar]
- Scott, A.R. ITI treatment guide, volume 5: Sinus floor elevation procedures. Br. Dent. J. 2012, 212, 512. [Google Scholar] [CrossRef]
- Anonymous. Proceedings of the 4th International team for Implantology (ITI) Consensus Conference, August 2008, Stuttgart, Germany. Int. J. Oral Maxillofac. Implant. 2009, 24, 7–278. [Google Scholar]
- Lazarin, R.; Ebenezer, S.; Benthaus, K.; Schimmel, M. The impact of the ITI international team for implantology on implant dentistry: A retrospective and descriptive analysis of 30 years of research support. Int. J. Oral Maxillofac. Implant. 2020, 35, e1–e13. [Google Scholar] [CrossRef]
- Rengo, C.; Fiorino, A.; Cucchi, A.; Nappo, A.; Randellini, E.; Calamai, P.; Ferrari, M. Patient-reported outcomes and complication rates after lateral maxillary sinus floor elevation: A prospective study. Clin. Oral Investig. 2021, 25, 4431–4444. [Google Scholar] [CrossRef]
- Zhou, Y.; Shi, Y.; Si, M.; Wu, M.; Xie, Z. The comparative evaluation of transcrestal and lateral sinus floor elevation in sites with residual bone height ≤ 6 mm: A two-year prospective randomized study. Clin. Oral Implant. Res. 2021, 32, 180–191. [Google Scholar] [CrossRef]
- Shao, Q.; Li, J.; Pu, R.; Feng, Y.; Jiang, Z.; Yang, G. Risk factors for sinus membrane perforation during lateral window maxillary sinus floor elevation surgery: A retrospective study. Clin. Implant Dent. Relat. Res. 2021, 23, 812–820. [Google Scholar] [CrossRef] [PubMed]
- Farina, R.; Franceschetti, G.; Travaglini, D.; Consolo, U.; Minenna, L.; Schincaglia, G.; Riccardi, O.; Bandieri, A.; Maietti, E.; Trombelli, L. Radiographic outcomes of transcrestal and lateral sinus floor elevation: One-year results of a bi-center, parallel-arm randomized trial. Clin. Oral Implant. Res. 2019, 30, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Thoma, D.S.; Yoon, S.R.; Cha, J.K.; Lim, H.C.; Lee, J.S.; Choi, S.H.; Jung, U.W. Sinus floor elevation using implants coated with recombinant human bone morphogenetic protein-2: Micro-computed tomographic and histomorphometric analyses. Clin. Oral Investig. 2018, 22, 829–837. [Google Scholar] [CrossRef] [PubMed]
- Boyacıgil, D.; Er, N.; Karaca, Ç.; Koç, O. The effect of residual bone height and membrane thickness on sinus membrane perforation in crestal sinus grafting: A prospective clinical study. Int. J. Oral Maxillofac. Surg. 2021, 50, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Andrés-García, R.; Ríos-Santos, J.; Herrero-Climent, M.; Bullón, P.; Fernández-Farhall, J.; Gómez-Menchero, A.; Fernández-Palacín, A.; Ríos-Carrasco, B. Sinus floor elevation via an osteotome technique without biomaterials. Int. J. Environ. Res. Public Health 2021, 18, 1103. [Google Scholar] [CrossRef] [PubMed]
- Munk, N.; Boulanger, K. Adaptation of the care guidelines for therapeutic massage and bodywork publications: Efforts to improve the impact of case reports. Int. J. Ther. Massage Bodyw. 2014, 7, 32. [Google Scholar]
- Sonoda, T.; Yamamichi, K.; Harada, T.; Yamamichi, N. Effect of staged crestal maxillary sinus augmentation: A case series. J. Periodontol. 2020, 91, 194–201. [Google Scholar] [CrossRef]
- Stacchi, C.; Lombardi, T.; Ottonelli, R.; Berton, F.; Perinetti, G.; Traini, T. New bone formation after transcrestal sinus floor elevation was influenced by sinus cavity dimensions: A prospective histologic and histomorphometric study. Clin. Oral Implant. Res. 2018, 29, 465–479. [Google Scholar] [CrossRef]
- Teng, M.; Liang, X.; Yuan, Q.; Nie, J.; Ye, J.; Cheng, Q.; Zhai, J.; Liao, J.; Sun, X.; Wen, C. The inlay osteotome sinus augmentation technique for placing short implants simultaneously with reduced crestal bone height. A short-term follow-up. Clin. Implant Dent. Relat. Res. 2013, 15, 918–926. [Google Scholar] [CrossRef]
- Aoki, N.; Baba, J.; Iwai, T.; Tohnai, I. Lateral bone window approach with micross mini bone scraper for sinus floor elevation. J. Maxillofac. Oral Surg. 2018, 17, 291–295. [Google Scholar] [CrossRef]
- Chandra, R.V.; Suvvari, N.; Reddy, A.A. Trephine core procedure versus bone-added osteotome sinus floor elevation in the augmentation of the sinus floor: A comparative clinical and radiographic study. Int. J. Oral Maxillofac. Implant. 2018, 33, 425–432. [Google Scholar] [CrossRef] [PubMed]
- Dongo, V.; Krockow, N.V.; Weigl, P. Lateral sinus floor elevation without grafting materials. Individual- and aggregate-data meta-analysis. J. Cranio-Maxillofac. Surg. 2018, 46, 1616–1624. [Google Scholar] [CrossRef] [PubMed]
- Aludden, H.; Mordenfeld, A.; Hallman, M.; Christensen, A.E.; Starch-Jensen, T. Osteotome-mediated sinus floor elevation with or without a grafting material: A systematic review and meta-analysis of long-term studies (≥5-years). Implant Dent. 2018, 27, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Li, C.; Zhou, J.; Sun, X.; Li, X.; Qi, M.; Zhou, Y. Endoscopically controlled flapless transcrestal sinus floor elevation with platelet-rich fibrin followed by simultaneous dental implant placement. Medicine 2018, 97, e0608. [Google Scholar] [CrossRef]
- Zheng, X.; Teng, M.; Zhou, F.; Ye, J.; Li, G.; Mo, A. Influence of maxillary sinus width on transcrestal sinus augmentation outcomes: Radiographic evaluation based on cone beam ct. Clin. Implant Dent. Relat. Res. 2016, 18, 292–300. [Google Scholar] [CrossRef]
- Kim, Y.K.; Lee, J.Y.; Park, J.W.; Kim, S.G.; Oh, J.S. Sinus membrane elevation by the crestal approach using a novel drilling system. Implant Dent. 2017, 26, 351. [Google Scholar] [CrossRef]
- Kent, J.N.; Block, M.S. Simultaneous maxillary sinus floor bone grafting and placement of hydroxylapatite-coated implants. J. Oral Maxillofac. Surg. 1989, 47, 238. [Google Scholar] [CrossRef]
- Franceschetti, G.; Farina, R.; Minenna, L.; Riccardi, O.; Stacchi, C.; di Raimondo, R.; Maietti, E.; Trombelli, L. The impact of graft remodeling on peri-implant bone support at implants placed concomitantly with transcrestal sinus floor elevation: A multicenter, retrospective case series. Clin. Oral. Implant. Res. 2020, 31, 105–120. [Google Scholar] [CrossRef]
- Hernández-Alfaro, F.; Torradeflot, M.M.; Marti, C. Prevalence and management of schneiderian membrane perforations during sinus-lift procedures. Clin. Oral Implant. Res. 2010, 19, 91–98. [Google Scholar] [CrossRef]
- Zhai, M.; Cheng, H.; Yuan, J.; Wang, X.; Li, B.; Li, D. Nonlinear biomechanical characteristics of the schneiderian membrane: Experimental study and numerical modeling. BioMed Res. Int. 2018, 2018, 2829163. [Google Scholar] [CrossRef]
- Sakuma, S.; Ferri, M.; Imai, H.; Mesa, N.F.; Victorio, D.B.; Alccayhuaman, K.A.; Botticelli, D. Involvement of the maxillary sinus ostium (mso) in the edematous processes after sinus floor augmentation: A cone-beam computed tomographic study. Int. J. Implant Dent. 2020, 6, 35. [Google Scholar] [CrossRef] [PubMed]
- Janner, S.; Dubach, P.; Suter, V.; Caversaccio, M.; Buser, D.; Bornstein, M. Sinus floor elevation or referral for further diagnosis and therapy: A comparison of maxillary sinus assessment by ent specialists and dentists using cone beam computed tomography. Clin. Oral Implant. Res. 2020, 31, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Testori, T.; Tavelli, L.; Yu, S.; Scaini, R.; Darnahal, A.; Wallace, S.; Wang, H. Maxillary sinus elevation difficulty score with lateral wall technique. Int. J. Oral Maxillofac. Implant. 2020, 35, 631–638. [Google Scholar] [CrossRef] [PubMed]
- Krennmair, S.; Malek, M.; Forstner, T.; Krennmair, G.; Weinländer, M.; Hunger, S. Risk factor analysis affecting sinus membrane perforation during lateral window maxillary sinus elevation surgery. Int. J. Oral Maxillofac. Implant. 2020, 35, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Tan, W.C.; Zwahlen, M.; Lang, N.P. A systematic review of the success of sinus floor elevation and survival of implants inserted in combination with sinus floor elevation. J. Clin. Periodontol. 2008, 35, 216–240. [Google Scholar] [CrossRef]
- Brignardellopetersen, R. Osteotome sinus floor elevation without bone graft seems to result in high survival rates and small amount of bone loss after 10 years. J. Am. Dent. Assoc. 2018, 149, e27. [Google Scholar] [CrossRef]
- Helder, M.N.; Fas, V.E.; Kwehandjaja, M.D.; Bruggenkate, C.M.T.; Klein-Nulend, J.; Eajm, S. Evaluation of a new biphasic calcium phosphate for maxillary sinus floor elevation: Micro-CT and histomorphometrical analyses. Clin. Oral Implant. Res. 2018, 29, 488–498. [Google Scholar] [CrossRef]
- Elian, S.; Barakat, K. Crestal endoscopic approach for evaluating sinus membrane elevation technique. Int. J. Implant Dent. 2018, 4, 15. [Google Scholar] [CrossRef]
- Vercellotti, T.; De, P.S.; Nevins, M. The piezoelectric bony window osteotomy and sinus membrane elevation: Introduction of a new technique for simplification of the sinus augmentation procedure. Int. J. Periodontics Restor. Dent. 2001, 21, 561–567. [Google Scholar]
- Wallace, S.S.; Tarnow, D.P.; Froum, S.J.; Cho, S.C.; Zadeh, H.H.; Stoupel, J.; Fabbro, M.D.; Testori, T. Maxillary sinus elevation by lateral window approach: Evolution of technology and technique. J. Evid. Based Dent. Pract. 2012, 12, 161–171. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group 0–4 mm | Sex | Age (Year) | Implant Site | RBH (mm) | Sinus Width (mm) | Implant Site’ | RBH’ (mm) | Sinus Width’ (mm) |
|---|---|---|---|---|---|---|---|---|
| No.1 | Male | 45 | 15 | 3.49 | 17.31 | 16 | 2.56 | 9.96 |
| No.2 | Female | 65 | 15 | 1.12 | 14.99 | 16 | 2.12 | 14.99 |
| No.3 | Female | 55 | 26 | 3.69 | 14.42 | 27 | 2.64 | 11.41 |
| No.4 | Male | 42 | 26 | 3.72 | 13.75 | 27 | 3.95 | 11.98 |
| No.5 | Male | 42 | 15 | 2.50 | 16.89 | 16 | 2.14 | 14.51 |
| No.6 | Male | 41 | 26 | 3.25 | 12.33 | 27 | 2.07 | 9.38 |
| No.7 | Male | 53 | 16 | 2.60 | 11.15 | 17 | 1.71 | 16.52 |
| No.8 | Female | 49 | 26 | 3.54 | 10.62 | 27 | 3.89 | 8.91 |
| No.9 | Male | 54 | 26 | 1.66 | 14.33 | 27 | 3.27 | 12.96 |
| Average ± SD | 49.6 ± 7.97 | - | 2.84 ± 0.94 | 13.98 ± 2.32 | - | 2.71 ± 0.82 | 12.29 ± 2.66 | |
| Group 4–5 mm | ||||||||
| No.10 | Female | 49 | 16 | 4.65 | 11.56 | 17 | 4.01 | 7.55 |
| No.11 | Male | 41 | 16 | 4.78 | 12.37 | 17 | 4.82 | 11.68 |
| No.12 | Male | 47 | 16 | 4.51 | 11.86 | 17 | 4.17 | 12.95 |
| No.13 | Male | 77 | 16 | 4.08 | 15.13 | 17 | 4.64 | 14.05 |
| No.14 | Female | 79 | 26 | 4.95 | 12.17 | 27 | 4.16 | 13.5 |
| No.15 | Female | 68 | 15 | 4.87 | 12.78 | 16 | 4.49 | 9.62 |
| No.16 | Female | 37 | 15 | 4.89 | 15.51 | 16 | 4.97 | 10.42 |
| No.17 | Female | 55 | 15 | 4.93 | 12.91 | 16 | 4.11 | 10.13 |
| No.18 | Female | 57 | 15 | 4.27 | 15.21 | 16 | 4.94 | 9.13 |
| Average ± SD | 56.7 ± 15.11 | - | 4.66 ± 0.31 | 13.28 ± 1.56 | - | 4.48 ± 0.38 | 12.29 ± 2.66 | |
| Group 5–7 mm | ||||||||
| No.19 | Male | 63 | 25 | 5.24 | 12.62 | 26 | 5.09 | 13.15 |
| No.20 | Female | 54 | 26 | 6.73 | 13.86 | 27 | 6.4 | 11.77 |
| No.21 | Female | 56 | 15 | 5.39 | 13.02 | 16 | 6.61 | 11.98 |
| No.22 | Female | 62 | 16 | 6.7 | 13.95 | 17 | 6.22 | 15.36 |
| No.23 | Male | 72 | 16 | 6.55 | 13.63 | 17 | 6.42 | 11.27 |
| No.24 | Male | 41 | 26 | 6.72 | 11.64 | 27 | 6.7 | 11.52 |
| No.25 | Male | 40 | 26 | 5.42 | 15.49 | 27 | 5.37 | 15.31 |
| No.26 | Female | 48 | 16 | 5.97 | 14.69 | 17 | 5.07 | 13.81 |
| No.27 | Female | 53 | 26 | 5.37 | 15.61 | 27 | 5.13 | 15.95 |
| No.28 | Male | 57 | 15 | 6.87 | 14.16 | 16 | 6.99 | 15.62 |
| No.29 | Female | 63 | 26 | 5.44 | 14.17 | 27 | 5.58 | 11.5 |
| No.30 | Male | 52 | 25 | 6.68 | 11.89 | 26 | 6.86 | 13.87 |
| Average ± SD | 55.1 ± 9.32 | - | 6.09 ± 0.67 | 13.73 ± 1.26 | - | 6.04 ± 0.74 | 13.43 ± 1.8 |
| Group 0–4 mm | Time of Surgery | Implant Size (mm) | Primary Stability (Ncm) | aGH1 (mm) | aGH2 (mm) | GR (mm) | Implant Size’ (mm) | Primary Stability’ (Ncm) | aGH1′ (mm) | aGH2′ (mm) | GR’ (mm) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| No.1 | 26 July 2017 | 4.8 × 8 | 20 | 2.43 | 1.23 | 1.2 | 4.8 × 8 | 5 | 1.97 | 0.44 | 1.53 |
| No.2 | 14 December 2017 | 4.1 × 10 | 30 | 2.07 | 0.83 | 1.24 | 4.8 × 8 | 20 | 1.83 | 1.57 | 0.26 |
| No.3 | 17 February 2018 | 4.8 × 10 | 5 | 1.97 | 1.14 | 0.83 | 4.8 × 10 | 5 | 0.66 | 0.45 | 0.21 |
| No.4 | 25 January 2018 | 4.8 × 10 | 20 | 1.60 | 0.74 | 0.86 | 4.8 × 8 | 35 | 3.97 | 3.21 | 0.76 |
| No.5 | 29 January 2018 | 4.1 × 10 | 30 | 2.42 | 2.3 | 0.12 | 4.8 × 8 | 10 | 1.12 | 0.49 | 0.63 |
| No.6 | 11 July 2017 | 4.8 × 10 | 20 | 1.29 | 1.12 | 0.17 | 4.8 × 8 | 20 | 4.08 | 2.82 | 1.26 |
| No.7 | 13 April 2016 | 4.8 × 8 | 20 | 4.96 | 3.84 | 1.12 | 4.8 × 8 | 20 | 4.24 | 3.58 | 0.66 |
| No.8 | 3 November 2017 | 4.8 × 8 | 35 | 2.65 | 2.5 | 0.15 | 4.8 × 8 | 35 | 1.74 | 0.53 | 1.21 |
| No.9 | 31 August 2017 | 4.8 × 8 | 30 | 2.96 | 0.66 | 2.3 | 4.8 × 8 | 30 | 1.92 | 1.64 | 0.28 |
| Average ± SD | - | - | 23.33 ± 9.01 | 2.48 ± 1.06 | 1.6 ± 1.07 | 0.89 ± 0.7 | - | 20 ± 11.73 | 2.39 ± 1.35 | 1.64 ± 1.28 | 0.76 ± 0.48 |
| Group 4–5 mm | |||||||||||
| No.10 | 15 November 2017 | 4.8 × 8 | 35 | 2.4 | 0.47 | 1.93 | 4.8 × 8 | 35 | 1.76 | 0.24 | 1.52 |
| No.11 | 11 July 2018 | 4.8 × 10 | 20 | 1.87 | 1.53 | 0.34 | 4.8 × 8 | 10 | 2.13 | 1.47 | 0.66 |
| No.12 | 1 April 2019 | 4.8 × 10 | 30 | 1.68 | 0.99 | 0.69 | 4.8 × 10 | 25 | 2.92 | 2.27 | 0.65 |
| No.13 | 12 April 2019 | 4.8 × 10 | 25 | 2.36 | 1.51 | 0.85 | 4.8 × 10 | 35 | 1.53 | 1.05 | 0.48 |
| No.14 | 12 April 2019 | 4.8 × 10 | 20 | 2.75 | 1.42 | 1.33 | 4.8 × 10 | 30 | 2.56 | 2.24 | 0.32 |
| No.15 | 19 April 2019 | 4.1 × 10 | 20 | 1.65 | 1.42 | 0.23 | 4.8 × 10 | 25 | 2.44 | 1.31 | 1.13 |
| No.16 | 23 April 2019 | 4.1 × 8 | 15 | 1.9 | 1.02 | 0.88 | 4.8 × 10 | 35 | 2.18 | 1.01 | 1.17 |
| No.17 | 20 June 2019 | 4.1 × 10 | 20 | 1.76 | 1.38 | 0.38 | 4.8 × 10 | 5 | 1.13 | 1.13 | 0 |
| No.18 | 21 June 2019 | 4.1 × 10 | 25 | 2.9 | 1.71 | 1.19 | 4.8 × 10 | 25 | 2.75 | 1.59 | 1.16 |
| Average ± SD | - | - | 23.33 ± 6.12 | 2.14 ± 0.47 | 1.27 ± 0.38 | 0.87 ± 0.55 | - | 25 ± 10.9 | 2.16 ± 0.9 | 1.37 ± 0.63 | 0.79 ± 0.49 |
| Group 5–7 mm | |||||||||||
| No.19 | 27 December 2018 | 4.1 × 10 | 35 | 1.77 | 1.35 | 0.12 | 4.8 × 10 | 30 | 2.17 | 1.17 | 1 |
| No.20 | 11 January 2019 | 4.8 × 10 | 30 | 2.13 | 0.86 | 0.97 | 4.8 × 10 | 35 | 1.97 | 1.31 | 0.66 |
| No.21 | 31 January2019 | 4.1 × 8 | 10 | 2.08 | 1.02 | 0.76 | 4.8 × 8 | 10 | 2.88 | 1.66 | 1.22 |
| No.22 | 2 February 2019 | 4.8 × 10 | 15 | 1.69 | 0.9 | 0.49 | 4.8 × 10 | 30 | 2.07 | 1.23 | 0.84 |
| No.23 | 12 February 2019 | 4.8 × 10 | 30 | 2.67 | 1.77 | 0.6 | 4.8 × 10 | 30 | 2.7 | 1.32 | 1.38 |
| No.24 | 14 February2019 | 4.8 × 10 | 15 | 2.06 | 1.29 | 0.47 | 4.8 × 10 | 30 | 1.87 | 1.2 | 0.67 |
| No.25 | 14 February2019 | 4.1 × 8 | 35 | 2.55 | 1.07 | 1.18 | 4.1 × 8 | 15 | 2.83 | 1.79 | 1.04 |
| No.26 | 21 February2019 | 4.1 × 8 | 20 | 2.64 | 1.48 | 0.86 | 4.8 × 8 | 25 | 1.82 | 1.35 | 0.47 |
| No.27 | 5 March 2019 | 4.1 × 10 | 15 | 2.54 | 1.37 | 0.87 | 4.8 × 10 | 30 | 2.74 | 1.31 | 1.43 |
| No.28 | 18 March 2019 | 4.8 × 8 | 30 | 2.53 | 0.88 | 1.35 | 4.8 × 10 | 30 | 2.26 | 1.23 | 1.03 |
| No.29 | 26 March 2019 | 4.8 × 10 | 10 | 2.11 | 1.61 | 0.2 | 4.8 × 8 | 25 | 2.21 | 1.38 | 0.83 |
| No.30 | 7 April 2019 | 4.8 × 8 | 25 | 2.61 | 1.64 | 0.67 | 4.8 × 10 | 35 | 1.7 | 1.58 | 0.12 |
| Average ± SD | - | - | 22.5 ± 9.41 | 2.28 ± 0.35 | 1.27 ± 0.32 | 0.71 ± 0.37 | - | 27.08 ± 7.53 | 2.27 ± 0.42 | 1.38 ± 0.2 | 0.89 ± 0.38 |
| Group 0–4 mm | aGH between Implants (mm) | aGH between Implants (mm) | GR between Implants (mm) |
|---|---|---|---|
| No.1 | 10.25 | 8.12 | 2.13 |
| No.2 | 11.21 | 10.14 | 1.07 |
| No.3 | 12.50 | 10.83 | 1.67 |
| No.4 | 11.77 | 9.72 | 2.05 |
| No.5 | 10.18 | 5.92 | 4.26 |
| No.6 | 12.26 | 10.37 | 1.89 |
| No.7 | 10.65 | 9.26 | 1.39 |
| No.8 | 10.69 | 9.72 | 0.97 |
| No.9 | 6.91 | 6.58 | 0.33 |
| Average ± SD | 10.71 ± 1.66 | 8.96 ± 1.72 | 1.75 ± 1.11 |
| Group 4–5 mm | |||
| No.10 | 9.35 | 8.03 | 1.32 |
| No.11 | 10.26 | 8.87 | 1.39 |
| No.12 | 11.22 | 8.94 | 2.28 |
| No.13 | 9.92 | 9.12 | 0.8 |
| No.14 | 9.86 | 7.71 | 2.15 |
| No.15 | 10.26 | 9.93 | 0.33 |
| No.16 | 11.68 | 9.35 | 2.33 |
| No.17 | 9.96 | 9.51 | 0.45 |
| No.18 | 11.36 | 8.41 | 2.95 |
| Average ± SD | 10.43 ± 0.8 | 8.87 ± 0.72 | 1.56 ± 0.92 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, N.; Liu, C. Modified Osteotome Sinus Floor Elevation Technique for Multiple Edentulous Spaces: A Non-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 8019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19138019
Kang N, Liu C. Modified Osteotome Sinus Floor Elevation Technique for Multiple Edentulous Spaces: A Non-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(13):8019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19138019
Chicago/Turabian StyleKang, Ning, and Caojie Liu. 2022. "Modified Osteotome Sinus Floor Elevation Technique for Multiple Edentulous Spaces: A Non-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 13: 8019. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19138019