
Dietary Diversity and Dietary Patterns in School-Aged Children in Western Kenya: A Latent Class Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Dietary Assessment
2.3. Anthropometric Assessment
2.4. Other Measures
2.5. Statistical Analysis
3. Results
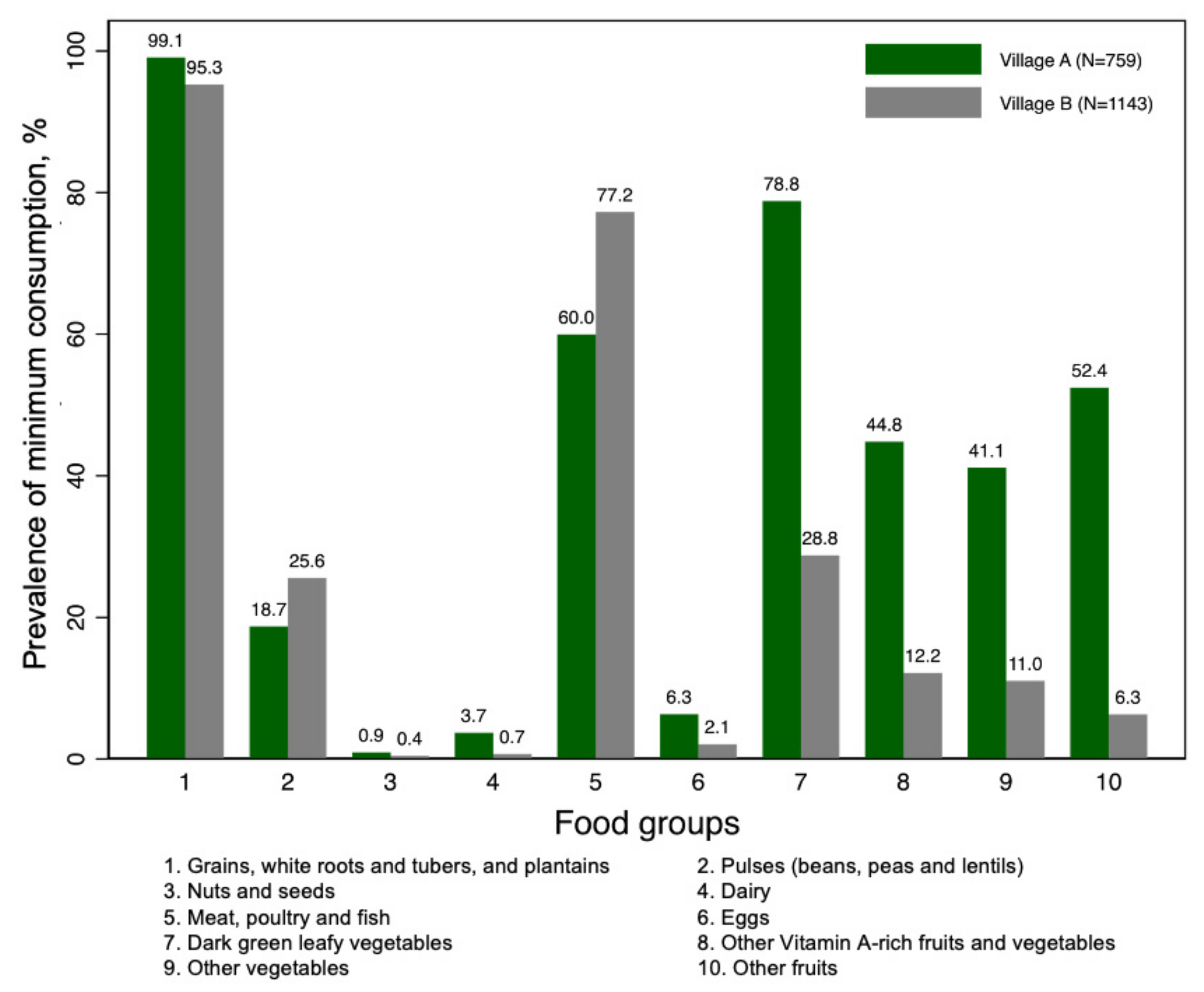
3.1. Dietary Diversity
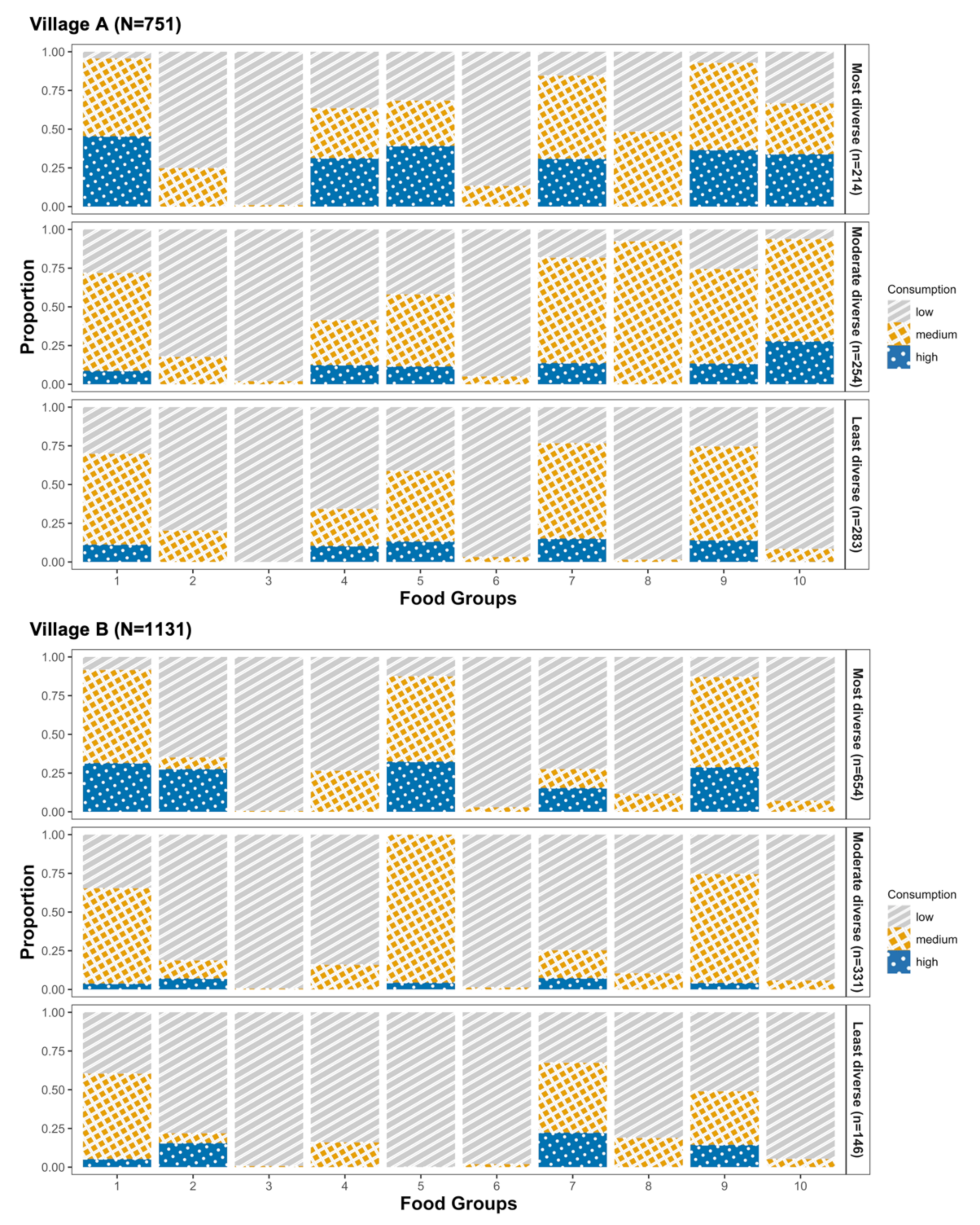
3.2. Dietary Patterns among Children in Village A
3.3. Dietary Patterns among Children in Village B
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Patton, G.C.; Sawyer, S.M.; Santelli, J.S.; Ross, D.A.; Afifi, R.; Allen, N.B.; Arora, M.; Azzopardi, P.; Baldwin, W.; Bonell, C.; et al. Our future: A Lancet commission on adolescent health and wellbeing. Lancet 2016, 387, 2423–2478. [Google Scholar] [CrossRef] [Green Version]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: Consequences for adult health and human capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef] [Green Version]
- Verger, E.O.; Le Port, A.; Borderon, A.; Bourbon, G.; Moursi, M.; Savy, M.; Mariotti, F.; Martin-Prevel, Y. Dietary Diversity Indicators and Their Associations with Dietary Adequacy and Health Outcomes: A Systematic Scoping Review. Adv. Nutr. 2021, 12, 1659–1672. [Google Scholar] [CrossRef]
- Popkin, B.M.; Corvalan, C.; Grummer-Strawn, L.M. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet 2020, 395, 65–74. [Google Scholar] [CrossRef]
- FAO. FHI 360. Minimum Dietary Diversity for Women: A Guide for Measurement; FAO: Rome, Italy, 2016. [Google Scholar]
- Martin-Prével, Y.; Allemand, P.; Wiesmann, D.; Arimond, M.; Ballard, T.; Deitchler, M.; Dop, M.-C.; Kennedy, G.; Lee, W.T.; Moursi, M. Moving forward on Choosing a Standard Operational Indicator of Women’s Dietary Diversity; FAO: Rome, Italy, 2015. [Google Scholar]
- Caswell, B.L.; Talegawkar, S.A.; Siamusantu, W.; West, K.P.; Palmer, A.C. A 10-Food Group Dietary Diversity Score Outperforms a 7-Food Group Score in Characterizing Seasonal Variability and Micronutrient Adequacy in Rural Zambian Children. J. Nutr. 2018, 148, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Bukania, Z.N.; Mwangi, M.; Karanja, R.M.; Mutisya, R.; Kombe, Y.; Kaduka, L.U.; Johns, T. Food Insecurity and Not Dietary Diversity Is a Predictor of Nutrition Status in Children within Semiarid Agro-Ecological Zones in Eastern Kenya. J. Nutr. Metab. 2014, 2014, 907153. [Google Scholar] [CrossRef] [PubMed]
- Amugsi, D.A.; Dimbuene, Z.T.; Kimani-Murage, E.W.; Mberu, B.; Ezeh, A.C. Differential effects of dietary diversity and maternal characteristics on linear growth of children aged 6–59 months in sub-Saharan Africa: A multi-country analysis. Public Health Nutr. 2017, 20, 1029–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- M’Kaibi, F.K.; Steyn, N.P.; Ochola, S.A.; Du Plessis, L. The relationship between agricultural biodiversity, dietary diversity, household food security, and stunting of children in rural Kenya. Food Sci. Nutr. 2017, 5, 243–254. [Google Scholar] [CrossRef]
- Muthini, D.; Nzuma, J.; Nyikal, R. Farm production diversity and its association with dietary diversity in Kenya. Food Secur. 2020, 12, 1107–1120. [Google Scholar] [CrossRef]
- Maseko, H.; Shackleton, C.M.; Nagoli, J.; Pullanikkatil, D. Children and Wild Foods in the Context of Deforestation in Rural Malawi. Hum. Ecol. Interdiscip. J. 2017, 45, 795–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berg, T.; Magala-Nyago, C.; Iversen, P.O. Nutritional status among adolescent girls in children’s homes: Anthropometry and dietary patterns. Clin. Nutr. 2018, 37, 926–933. [Google Scholar] [CrossRef]
- Zenebe, M.; Gebremedhin, S.; Henry, C.J.; Regassa, N. School feeding program has resulted in improved dietary diversity, nutritional status and class attendance of school children. Ital. J. Pediatr. 2018, 44, 16. [Google Scholar] [CrossRef] [Green Version]
- Darling, A.M.; Sunguya, B.; Ismail, A.; Manu, A.; Canavan, C.; Assefa, N.; Sie, A.; Fawzi, W.; Sudfeld, C.; Guwattude, D. Gender differences in nutritional status, diet and physical activity among adolescents in eight countries in sub-Saharan Africa. Trop. Med. Int. Health 2020, 25, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oniang’o, R.K.; Komokoti, A. Food habits in Kenya: The effects of change and attendant methodological problems. Appetite 1999, 32, 93–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steyn, N.P.; Nel, J.H.; Parker, W.; Ayah, R.; Mbithe, D. Urbanisation and the nutrition transition: A comparison of diet and weight status of South African and Kenyan women. Scand. J. Public Health 2012, 40, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Mbogori, T.; Kimmel, K.; Zhang, M.; Kandiah, J.; Wang, Y. Nutrition transition and double burden of malnutrition in Africa: A case study of four selected countries with different social economic development. AIMS Public Health 2020, 7, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Dossus, L.; Barquera, S.; Blottiere, H.M.; Franks, P.W.; Gunter, M.; Hwalla, N.; Hursting, S.D.; Leitzmann, M.; Margetts, B.; et al. Obesity, Energy balance and obesity: What are the main drivers? Cancer Causes Control 2017, 28, 247–258. [Google Scholar] [CrossRef] [Green Version]
- Kogo, B.K.; Kumar, L.; Koech, R. Climate change and variability in Kenya: A review of impacts on agriculture and food security. Environ. Dev. Sustain. 2020, 23, 23–43. [Google Scholar] [CrossRef]
- Wathome, D.M. The Relationship between Income and Food Consumption Patterns in Urban Nakuru. Ph.D. Thesis, University of Nairobi, Nairobi, Kenya, 1990. [Google Scholar]
- Ngatia, E.M.; Imungi, J.K.; Muita, J.W.; Nganga, P.M. Dietary patterns and dental caries in nursery school children in Nairobi, Kenya. East Afr. Med. J. 2001, 78, 673–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van’t Riet, H.; den Hartog, A.P.; Mwangi, A.M.; Mwadime, R.K.; Foeken, D.W.; van Staveren, W.A. The role of street foods in the dietary pattern of two low-income groups in Nairobi. Eur. J. Clin. Nutr. 2001, 55, 562–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ndiku, M.; Jaceldo-Siegl, K.; Sabaté, J. Dietary patterns of infant and preschool children in Mwingi and Makueni districts of Ukambani region, eastern Kenya. Afr. J. Food Agric. Nutr. Dev. 2010, 10. [Google Scholar] [CrossRef] [Green Version]
- Hansen, A.W.; Christensen, D.L.; Larsson, M.W.; Eis, J.; Christensen, T.; Friis, H.; Mwaniki, D.L.; Kilonzo, B.; Boit, M.K.; Borch-Johnsen, K.; et al. Dietary patterns, food and macronutrient intakes among adults in three ethnic groups in rural Kenya. Public Health Nutr. 2011, 14, 1671–1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbochi, R.W.; Kuria, E.; Kimiywe, J.; Ochola, S.; Steyn, N.P. Predictors of overweight and obesity in adult women in Nairobi Province, Kenya. BMC Public Health 2012, 12, 823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelsen, L.; Alarcon, P.; Häsler, B.; Amendah, D.D.; Ferguson, E.; Fèvre, E.M.; Grace, D.; Dominguez-Salas, P.; Rushton, J. Cross-sectional study of drivers of animal-source food consumption in low-income urban areas of Nairobi, Kenya. BMC Nutr. 2016, 2, 70. [Google Scholar] [CrossRef] [Green Version]
- WHO Guideline: Implementing Effective Actions for Improving Adolescent Nutrition; World Health Organization: Geneva, Switzerland, 2018.
- Thorne-Lyman, A.L.; Shaikh, S.; Mehra, S.; Wu, L.S.; Ali, H.; Alland, K.; Schultze, K.J.; Mitra, M.; Hur, J.; Christian, P. Dietary patterns of >30,000 adolescents 9–15 years of age in rural Bangladesh. Ann. N. Y. Acad. Sci. 2020, 1468, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Shively, G.; Evans, A. Dietary Diversity in Nepal: A Latent Class Approach. Food Nutr. Bull. 2021, 42, 259–273. [Google Scholar] [CrossRef]
- Shorr, I.J. How to Weigh and Measure Children; United Nations: New York, NY, USA, 1986. [Google Scholar]
- UNICEF Mid-Upper Arm Circumference (MUAC) Measuring Tapes—Technical Bulletin. Available online: https://www.unicef.org/supply/documents/mid-upper-arm-circumference-muac-measuring-tapes-technical-bulletin (accessed on 27 July 2021).
- Linzer, D.A.; Lewis, J.B. poLCA: An R Package for Polytomous Variable Latent Class Analysis. J. Stat. Softw. 2011, 42, 1–29. [Google Scholar] [CrossRef] [Green Version]
- FAO. Minimum Dietary Diversity for Women; FAO: Rome, Italy, 2021. [Google Scholar]
- Deloitte The Lake Region Economic Blueprint: A Better Life. Available online: https://www2.deloitte.com/content/dam/Deloitte/ke/Documents/public-sector/PS_Lake%20Basin_DeloitteKenya.pdf (accessed on 21 June 2021).
- Thuita, F.; Mwadime, K.; Wang’ombe, J.; Thuita, F.M. Influence of access to microfinance credit by women on household food consumption patterns in an urban low income setting in Nairobi, Kenya. Eur. Int. J. Sci. Technol. 2013, 2, 79–88. [Google Scholar]
- Rousham, E.K.; Pradeilles, R.; Akparibo, R.; Aryeetey, R.; Bash, K.; Booth, A.; Muthuri, S.K.; Osei-Kwasi, H.; Marr, C.M.; Norris, T.; et al. Dietary behaviours in the context of nutrition transition: A systematic review and meta-analyses in two African countries. Public Health Nutr. 2020, 23, 1948–1964. [Google Scholar] [CrossRef]
- FEWS NET. Food Security Primarily Remains Stable with the Early End of the Long Rains in May. Available online: https://fews.net/sites/default/files/documents/reports/Kenya_OL_07_2013.pdf (accessed on 31 July 2020).
- FEWS NET. Food Security to Remain Stable Despite Likely Normal to Below Normal October to December Rains. Available online: https://fews.net/sites/default/files/documents/reports/Kenya_OL_10_2013.pdf (accessed on 31 July 2020).
- WHO Children’s Diet. Available online: https://www.who.int/dietphysicalactivity/childhood_diet/en/ (accessed on 17 February 2021).
- Gidding, S.S.; Dennison, B.A.; Birch, L.L.; Daniels, S.R.; Gillman, M.W.; Lichtenstein, A.H.; Rattay, K.T.; Steinberger, J.; Stettler, N.; Van Horn, L.; et al. Dietary recommendations for children and adolescents: A guide for practitioners. Pediatrics 2006, 117, 544–559. [Google Scholar]
- Wrottesley, S.V.; Pedro, T.M.; Fall, C.H.; Norris, S.A. A review of adolescent nutrition in South Africa: Transforming adolescent lives through nutrition initiative. South Afr. J. Clin. Nutr. 2020, 33, 94–132. [Google Scholar] [CrossRef]
- WHO Diet, Nutrition and the Prevention of Chronic Diseases: Report of a WHO Study Group; World Health Organization: Geneva, Switzerland, 1990.
- Ferguson, E.L.; Gibson, R.S.; Opare-Obisaw, C.; Osei-Opare, F.; Lamba, C.; Ounpuu, S. Seasonal food consumption patterns and dietary diversity of rural preschool Ghanaian and Malawian children23. Ecol. Food Nutr. 1993, 29, 219–234. [Google Scholar] [CrossRef]
- Ndekha, M.; Kulmala, T.; Vaahtera, M.; Cullinan, T.; Salin, M.L.; Ashorn, P. Seasonal variation in the dietary sources of energy for pregnant women in Lungwena, rural Malawi. Ecol. Food Nutr. 2000, 38, 605–622. [Google Scholar] [CrossRef]
- Patterson, K.; Berrang-Ford, L.; Lwasa, S.; Namanya, D.B.; Ford, J.; Twebaze, F.; Clark, S.; Donnelly, B.; Harper, S.L. Seasonal variation of food security among the Batwa of Kanungu, Uganda. Public Health Nutr. 2017, 20, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Village A (n = 759) | Village B (n = 1143) | |
|---|---|---|
| Percentage (Number) | ||
| Gender, male | 53.6 (407) | 52.2 (596) |
| Did not go to bed hungry last night | 99.1 (752) | 92.6 (1058) |
| Not orphan | 65.1 (494) | -- |
| Mean (SD) | ||
| Age, years | 11.6 (2.2) | 12.6 (2.2) |
| Height, cm | 147.0 (12.4) | 148.5 (13.0) |
| Weight, kg | 38.2 (10.3) | 39.3 (10.6) |
| BMI, kg/m2 | 17.3 (2.2) | 17.5 (2.2) |
| MUAC, cm | 21.2 (2.9) | 21.0 (2.8) |
| Village A (n = 759) | Village B (n = 1143) | |
|---|---|---|
| Mean (SD) | ||
| Total daily calories | 966.1 (447.8) | 726.0 (414.3) |
| Percentage calories from fat, % | 19.4 (9.5) | 17.0 (9.5) |
| Percentage calories from carbohydrates, % | 65.1 (13.3) | 62.3 (15.6) |
| Percentage calories from protein, % | 15.5 (9.8) | 20.6 (12.5) |
| WDDS | 4.1 (1.4) | 2.6 (0.9) |
| Percentage (number) | ||
| WDDS component scores | ||
| 0 | 0.8 (6) | 0.4 (5) |
| 1 | 0.5 (4) | 6.6 (76) |
| 2 | 11.9 (90) | 43.0 (491) |
| 3 | 23.5 (178) | 36.5 (417) |
| 4 | 24.5 (186) | 10.1 (116) |
| 5 | 23.7 (180) | 3.0 (34) |
| 6 | 11.6 (88) | 0.3 (4) |
| 7· | 3.4 (26) | 0.0 |
| 8 | 0.1 (1) | 0.0 |
| 9 | 0.0 | 0.0 |
| 10 | 0.0 | 0.0 |
| Odds Ratio (95% CI) | |||
|---|---|---|---|
| Most Diverse | Moderately Diverse | Least Diverse | |
| Village A (n = 751) | n = 214 | n = 254 | n = 283 |
| Age, years | reference | 1.13 (0.87, 1.49) | 1.15 (0.88, 1.50) |
| Gender a | reference | 2.44 (1.89, 3.15) | 5.66 (4.58, 6.98) |
| Orphan status b | reference | 4.19 (2.66, 6.59) | 3.58 (2.50, 5.13) |
| BMI, kg/m2 | reference | 1.50 (1.20, 1.86) | 1.57 (1.26, 1.96) |
| Per 100 kcal/d energy | reference | 0.42 (0.32, 0.55) | 0.33 (0.26, 0.43) |
| Village B (n = 1131) | n = 654 | n = 331 | n = 146 |
| Age, years | reference | 1.13 (0.91, 1.41) | 1.00 (0.78, 1.27) |
| Gender a | reference | 0.95 (0.39, 2.28) | 1.34 (0.52, 3.47) |
| BMI, kg/m2 | reference | 1.50 (1.15, 1.96) | 1.71 (1.29, 2.26) |
| Per 100 kcal/d energy | reference | 0.22 (0.11, 0.41) | 0.14 (0.07, 0.28) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, T.; Broverman, S.; Puffer, E.S.; Zaltz, D.A.; Thorne-Lyman, A.L.; Benjamin-Neelon, S.E. Dietary Diversity and Dietary Patterns in School-Aged Children in Western Kenya: A Latent Class Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159130
Liu T, Broverman S, Puffer ES, Zaltz DA, Thorne-Lyman AL, Benjamin-Neelon SE. Dietary Diversity and Dietary Patterns in School-Aged Children in Western Kenya: A Latent Class Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159130
Chicago/Turabian StyleLiu, Tiange, Sherryl Broverman, Eve S. Puffer, Daniel A. Zaltz, Andrew L. Thorne-Lyman, and Sara E. Benjamin-Neelon. 2022. "Dietary Diversity and Dietary Patterns in School-Aged Children in Western Kenya: A Latent Class Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9130. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19159130