
HOMA Index, Vitamin D Levels, Body Composition and Cardiorespiratory Fitness in Juvenile Obesity: Data from the CHILT III Programme, Cologne

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
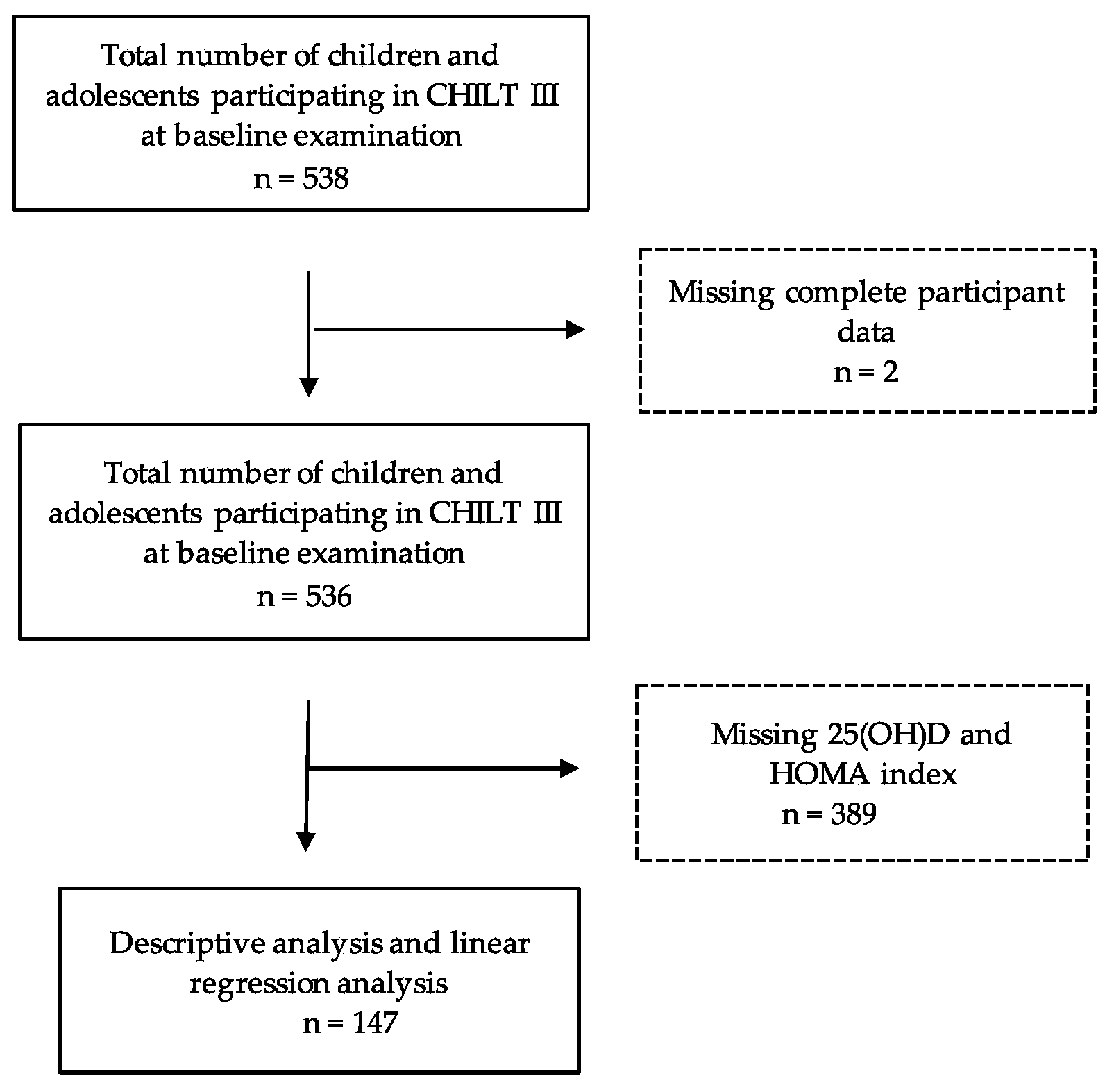
2.1. Study Population
2.2. Anthropometric Data
2.3. Laboratory Parameters
2.4. Determination of Cardiorespiratory Fitness
2.5. Statistical Analysis
3. Results
3.1. Anthropometric Data and Laboratory Parameters
3.2. Cardiorespiratory Fitness
3.3. Regression Analyses
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Levels and Trends in Child Malnutrition: Key Findings of the 2020 Edition. Available online: https://www.who.int/publications-detail-redirect/9789240003576 (accessed on 16 December 2021).
- World Health Organization. Obesity. Available online: https://www.who.int/health-topics/obesity#tab=tab1 (accessed on 29 December 2021).
- Schienkiewitz, A.; Damerow, S.; Schaffrath Rosario, A. Prävalenz von Untergewicht, Übergewicht und Adipositas bei Kindern und Jugendlichen in Deutschland—Einordnung der Ergebnisse aus KiGGS Welle 2 nach internationalen Referenzsystemen. J. Health Monit. 2018, 3, 60–74. [Google Scholar] [CrossRef]
- Bogers, R.P.; Bemelmans, W.J.E.; Hoogenveen, R.T.; Boshuizen, H.C.; Woodward, M.; Knekt, P.; van Dam, R.M.; Hu, F.B.; Visscher, T.L.S.; Menotti, A.; et al. Association of Overweight with Increased Risk of Coronary Heart Disease Partly Independent of Blood Pressure and Cholesterol Levels: A Meta-Analysis of 21 Cohort Studies Including More than 300,000 Persons. Arch. Intern. Med. 2007, 167, 1720–1728. [Google Scholar] [CrossRef] [PubMed]
- Friedemann, C.; Heneghan, C.; Mahtani, K.; Thompson, M.; Perera, R.; Ward, A.M. Cardiovascular Disease Risk in Healthy Children and Its Association with Body Mass Index: Systematic Review and Meta-Analysis. BMJ 2012, 345, e4759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lifshitz, F. Obesity in Children. J. Clin. Res. Pediatr. Endocrinol. 2008, 1, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Lobstein, T.; Baur, L.; Uauy, R. IASO International Obesity TaskForce. Obesity in Children and Young People: A Crisis in Public Health. Obes. Rev. 2004, 5 (Suppl. 1), 4–104. [Google Scholar] [CrossRef] [PubMed]
- Litwin, S.E. Childhood Obesity and Adulthood Cardiovascular Disease. J. Am. Coll. Cardiol. 2014, 64, 1588–1590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dolinsky, D.H.; Armstrong, S.; Mangarelli, C.; Kemper, A.R. The Association between Vitamin D and Cardiometabolic Risk Factors in Children: A Systematic Review. Clin. Pediatr. (Phila) 2013, 52, 210–223. [Google Scholar] [CrossRef]
- RKI-Gesundheit A-Z—Antworten des Robert Koch-Instituts auf Häufig Gestellte Fragen zu Vitamin D. Available online: https://www.rki.de/SharedDocs/FAQ/Vitamin_D/Vitamin_D_FAQ-Liste.html#FAQId11855876 (accessed on 16 December 2021).
- Gilbert-Diamond, D.; Baylin, A.; Mora-Plazas, M.; Marin, C.; Arsenault, J.E.; Hughes, M.D.; Willett, W.C.; Villamor, E. Vitamin D Deficiency and Anthropometric Indicators of Adiposity in School-Age Children: A Prospective Study. Am. J. Clin. Nutr. 2010, 92, 1446–1451. [Google Scholar] [CrossRef] [Green Version]
- Wortsman, J.; Matsuoka, L.Y.; Chen, T.C.; Lu, Z.; Holick, M.F. Decreased Bioavailability of Vitamin D in Obesity. Am. J. Clin. Nutr. 2000, 72, 690–693. [Google Scholar] [CrossRef]
- Mehmood, Z.-T.-N.H.; Papandreou, D. An Updated Mini Review of Vitamin D and Obesity: Adipogenesis and Inflammation State. Open Access Maced. J. Med. Sci. 2016, 4, 526–532. [Google Scholar] [CrossRef] [Green Version]
- Greco, E.A.; Lenzi, A.; Migliaccio, S. Role of Hypovitaminosis D in the Pathogenesis of Obesity-Induced Insulin Resistance. Nutrients 2019, 11, 1506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adikaram, S.G.S.; Samaranayake, D.B.D.L.; Atapattu, N.; Kendaragama, K.M.D.L.D.; Senevirathne, J.T.N.; Wickramasinghe, V.P. Prevalence of Vitamin D Deficiency and Its Association with Metabolic Derangements among Children with Obesity. BMC Pediatr. 2019, 19, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, S.J.; Edelman, M.; Uwaifo, G.I.; Freedman, R.J.; Semega-Janneh, M.; Reynolds, J.; Yanovski, J.A. The relationship between obesity and serum 1, 25-dihydroxy vitamin D concentrations in healthy adults. J. Clin. Endocrinol. Metab. 2004, 89, 1196–1199. [Google Scholar] [CrossRef] [Green Version]
- Szymczak-Pajor, I.; Śliwińska, A. Analysis of Association between Vitamin D Deficiency and Insulin Resistance. Nutrients 2019, 11, 794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Gong, J.; Hong, H.; Ha, C.; Kang, H. Serum Vitamin D Status and Its Relations to Body Fatness and Fitness and Risk Factors in Young Adults. J. Exerc. Nutr. Biochem. 2013, 17, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geirsdottir, O.G.; Chang, M.; Jonsson, P.V.; Thorsdottir, I.; Ramel, A. Associations of Physical Activity with Vitamin D Status Depends on Obesity Status in Old Adults. Clin. Nutr. ESPEN 2020, 39, 222–226. [Google Scholar] [CrossRef]
- Tarp, J.; Støle, A.P.; Blond, K.; Grøntved, A. Cardiorespiratory Fitness, Muscular Strength and Risk of Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diabetologia 2019, 62, 1129–1142. [Google Scholar] [CrossRef] [Green Version]
- Medrano, M.; Arenaza, L.; Migueles, J.H.; Rodríguez-Vigil, B.; Ruiz, J.R.; Labayen, I. Associations of Physical Activity and Fitness with Hepatic Steatosis, Liver Enzymes, and Insulin Resistance in Children with Overweight/Obesity. Pediatr. Diabetes 2020, 21, 565–574. [Google Scholar] [CrossRef]
- Bener, A.; Al-Hamaq, A.O.A.A.; Kurtulus, E.M.; Abdullatef, W.K.; Zirie, M. The Role of Vitamin D, Obesity and Physical Exercise in Regulation of Glycemia in Type 2 Diabetes Mellitus Patients. Diabetes Metab. Syndr. 2016, 10, 198–204. [Google Scholar] [CrossRef]
- Carson, E.L.; Pourshahidi, L.K.; Hill, T.R.; Cashman, K.D.; Strain, J.J.; Boreham, C.A.; Mulhern, M.S. Vitamin D, Muscle Function, and Cardiorespiratory Fitness in Adolescents From the Young Hearts Study. J. Clin. Endocrinol. Metab. 2015, 100, 4621–4628. [Google Scholar] [CrossRef] [Green Version]
- Valtueña, J.; Gracia-Marco, L.; Huybrechts, I.; Breidenassel, C.; Ferrari, M.; Gottrand, F.; Dallongeville, J.; Sioen, I.; Gutierrez, A.; Kersting, M.; et al. Cardiorespiratory Fitness in Males, and Upper Limbs Muscular Strength in Females, Are Positively Related with 25-Hydroxyvitamin D Plasma Concentrations in European Adolescents: The HELENA Study. QJM 2013, 106, 809–821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Pollock, N.; Stallmann-Jorgensen, I.S.; Gutin, B.; Lan, L.; Chen, T.C.; Keeton, D.; Petty, K.; Holick, M.F.; Zhu, H. Low 25-Hydroxyvitamin D Levels in Adolescents: Race, Season, Adiposity, Physical Activity, and Fitness. Pediatrics 2010, 125, 1104–1111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lier, L.M.; Breuer, C.; Ferrari, N.; Friesen, D.; Maisonave, F.; Schmidt, N.; Graf, C. Individual Physical Activity Behaviour and Group Composition as Determinants of the Effectiveness of a Childhood Obesity Intervention Program. OFA 2021, 14, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Eisenburger, N.; Friesen, D.; Haas, F.; Klaudius, M.; Schmidt, L.; Vandeven, S.; Joisten, C. Predicting Psychosocial Health of Children and Adolescents with Obesity in Germany: The Underappreciated Role of Physical Fitness. Int. J. Environ. Res. Public Health 2021, 18, 11188. [Google Scholar] [CrossRef]
- Kromeyer-Hauschild, K.; Wabitsch, M.; Kunze, D.; Geller, F.; Geiß, H.C.; Hesse, V.; von Hippel, A.; Jaeger, U.; Johnsen, D.; Korte, W.; et al. Perzentile für den Body-mass-Index für das Kindes- und Jugendalter unter Heranziehung verschiedener deutscher Stichproben. Mon. Kinderheilkd 2001, 149, 807–818. [Google Scholar] [CrossRef] [Green Version]
- Wabitsch, M.; Kunze, D. Konsensbasierte AGA S2-Leitlinie zur Diagnostik, Therapie und Prävention von Übergewicht und Adipositas im Kindes- und Jugendalter.: Version 15.10.2015. Available online: https://www.a-g-a.de (accessed on 21 November 2021).
- Lohman, T.G.; Roche, A.F.; Martorel, R. Anthropometric Standardization Reference Manual; Human Kinetics Books: Champaign, IL, USA, 1988; ISBN 978-087-322-121-4. [Google Scholar]
- Slaughter, M.H.; Lohman, T.G.; Boileau, R.A.; Horswill, C.A.; Stillman, R.J.; van Loan, M.D.; Bemben, D.A. Skinfold equations for estimation of body fatness in children and youth. Human Biol. 1988, 60, 709–723. [Google Scholar]
- Rodríguez, G.; Moreno, L.A.; Blay, M.G.; Blay, V.A.; Fleta, J.; Sarría, A.; Bueno, M.; AVENA-Zaragoza Study Group. Body Fat Measurement in Adolescents: Comparison of Skinfold Thickness Equations with Dual-Energy X-Ray Absorptiometry. Eur. J. Clin. Nutr. 2005, 59, 1158–1166. [Google Scholar] [CrossRef]
- Data Input. Nutriguard-MS Gebrauchsanleitung: Version 2.0. Available online: https://www.data-input.de/media/pdf_deutsch_2018/Gebrauchsanleitung_Nutriguard%20MS_2019.pdf (accessed on 29 November 2021).
- Data Input. Nutri Plus Gebrauchsanleitung: Software zur Bestimmung von Körperzusammensetzung und Ernährungszustand aus BIA-Messungen. Available online: https://data-input.de/media/pdf_deutsch_2018/Data_Input_NutriPlus_Gebrauchsanleitung_DE.pdf (accessed on 21 November 2021).
- Landwehr, C. Zusammenhang zwischen dem mütterlichen Lebensstil, ausgewählten Gesundheits- und Laborparametern sowie dem Einfluss auf die frühkindliche Entwicklung-die “MAMA”-Studie. Ph.D. Dissertation, Deutsche Sporthochschule, Köln, Germany, 2017. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Arellano-Ruiz, P.; García-Hermoso, A.; Cavero-Redondo, I.; Pozuelo-Carrascosa, D.; Martínez-Vizcaíno, V.; Solera-Martinez, M. Homeostasis Model Assessment Cut-off Points Related to Metabolic Syndrome in Children and Adolescents: A Systematic Review and Meta-Analysis. Eur. J. Pediatr. 2019, 178, 1813–1822. [Google Scholar] [CrossRef]
- Menrath, I.; Graf, C.; Granacher, U.; Kriemler, S. Pädiatrische Sportmedizin; Springer: Berlin/Heidelberg, Germany, 2021. [Google Scholar] [CrossRef]
- Orysiak, J.; Mazur-Rozycka, J.; Fitzgerald, J.; Starczewski, M.; Malczewska-Lenczowska, J.; Busko, K. Vitamin D Status and Its Relation to Exercise Performance and Iron Status in Young Ice Hockey Players. PLoS ONE 2018, 13, e0195284. [Google Scholar] [CrossRef]
- Milani, G.P.; Simonetti, G.D.; Edefonti, V.; Lava, S.A.G.; Agostoni, C.; Curti, M.; Stettbacher, A.; Bianchetti, M.G.; Muggli, F. Seasonal Variability of the Vitamin D Effect on Physical Fitness in Adolescents. Sci. Rep. 2021, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Trecroci, A.; Invernizzi, P.L.; Monacis, D.; Colella, D. Actual and Perceived Motor Competence in Relation to Body Mass Index in Primary School-Aged Children: A Systematic Review. Sustainability 2021, 13, 9994. [Google Scholar] [CrossRef]
- Chee, W.S.S.; Chang, C.Y.; Arasu, K.; Wong, S.Y.; Ong, S.H.; Yang, W.Y.; Chong, M.H.Z.; Mavinkurve, M.; Khoo, E.J.; Chinna, K.; et al. Vitamin D Status Is Associated with Modifiable Lifestyle Factors in Pre-Adolescent Children Living in Urban Kuala Lumpur, Malaysia. Nutrients 2021, 13, 2175. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.A.; Dalskov, S.-M.; Sørensen, L.B.; Hjorth, M.F.; Andersen, R.; Tetens, I.; Krarup, H.; Ritz, C.; Astrup, A.; Michaelsen, K.F.; et al. Vitamin D Status Is Associated with Cardiometabolic Markers in 8-11-Year-Old Children, Independently of Body Fat and Physical Activity. Br. J. Nutr. 2015, 114, 1647–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalba-Heredia, L.; Comeras-Chueca, C.; González-Agüero, A.; Domingo-Del-Val, D.; Calmarza, P.; Vicente-Rodríguez, G.; Casajús, J.A.; Matute-Llorente, Á. 25-Hydroxyvitamin D and Cardiorespiratory Fitness in Prepubertal Overweight and Obese Children. Nutrients 2021, 13, 1597. [Google Scholar] [CrossRef] [PubMed]
- Orces, C.H. The Association between 25-Hydroxyvitamin D Levels and Muscle Strength in Adolescents. Nutr. Hosp. 2021, 38, 1169–1174. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sánchez, C.; Oses, M.; Villanueva, A.; Cabeza, R.; Idoate, F.; Sanz, A.; Rodríguez-Vigil, B.; Ortega, F.B.; Ruiz, J.R.; et al. Associations of Fitness and Physical Activity with Specific Abdominal Fat Depots in Children with Overweight/Obesity. Scand J. Med. Sci. Sports 2022, 32, 211–222. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Total | Boys | Girls | p-Value | |
|---|---|---|---|---|---|
| Percentile | Obese | 133 (90.5%) | 62 (88%) | 71 (96%) | 0.096 † |
| Overweight | 11 (7.5%) | 8 (12%) | 3 (4%) | ||
| Physical Variables | Age (years) | 12.3 ± 2.3 (n = 147) | 12.5 ± 2.1 (n= 70) | 12.0 ± 2.4 (n = 77) | 0.191 ‡ |
| Height (m) | 1.57 ± 0.1 (n = 144) | 1.59 ± 0.1 (n = 70) | 1.55 ± 0.1 (n = 74) | 0.058 ‡ | |
| Weight (kg) | 76.4 ± 19.9 (n = 144) | 79.9 ± 23.1 (70) | 73.1 ± 15.8 (n = 74) | 0.043 ‡ | |
| Waist circumference | 95.2 ± 13.6 (n = 136) | 99.0 ± 16.0 (n = 68) | 91.3 ± 9.2 (n = 68) | <0.001 ‡ | |
| BMI (kg/m2) | 30.5 ± 5.2 (n = 144) | 31.1 ± 6.2 (n = 70) | 29.9 ± 3.9 (n = 74) | 0.188 ‡ | |
| BMI SDS | 2.52 ± 0.5 (n = 144) | 2.49 ± 0.5 (n = 70) | 2.55 ± 0.4 (n = 74) | 0.478 ‡ | |
| Body fat (kg) | 19.8 ± 6.3 (n = 137) | 20.8 ± 7.4 (n = 68) | 18.8 ± 4.9 (n = 69) | 0.065 ‡ | |
| Body fat (%) | 25.4 ± 2.2 (n = 137) | 25.5 ± 2.3 (n = 68) | 25.3 ± 2.1 (n = 69) | 0.609 ‡ | |
| Muscle mass (kg) | 23.1 ± 7.2 (n = 73) | 24.0 ± 8.7 (n = 37) | 22.3 ± 5.1 (n = 36) | 0.324 ‡ | |
| Muscle mass (%) | 30.8 ± 4.2 (n = 73) | 30.4 ± 5.1 (n = 37) | 31.3 ± 2.9 (n = 36) | 0.361 ‡ | |
| Fitness parameter | Absolute cardiorespiratory Fitness (W) | 120.0 ± 33.9 (n = 135) | 124.5 ± 38.4 (n = 68) | 115.4 ± 28.2 (n = 67) | 0.188 ‡ |
| Relative cardiorespiratory Fitness (W/kg) | 1.6 ± 0.4 (n = 135) | 1.6 ± 0.4 (n = 68) | 1.6 ± 0.4 (n = 67) | 0.404 ‡ | |
| Laboratory parameters | 25(OH)D (ng/mL) | 23.29 ± 9.8 (n = 147) | 24.88 ± 10.9 (n = 70) | 21.85 ± 8.6 (n = 77) | 0.062 ‡ |
| Blood glucose (mg/dL) | 90.76 ± 7.9 (n = 147) | 91.72 ± 7.8 (n = 70) | 89.89 ± 7.9 (n= 77) | 158 ‡ | |
| Insulin (µU/mL) | 22.27 ± 11.8 (n = 147) | 23.00 ± 12.7 (n = 70) | 21.61 ± 10.9 (n= 77) | 0.478 ‡ | |
| HOMA index | 5.01 ± 2.7 (n = 147) | 5.20 ± 2.8 (n = 70) | 4.84 ± 2.5 (n = 77) | 0.419 ‡ |
| Variable | Vitamin D (ng/mL) | HOMA Index | |||||
|---|---|---|---|---|---|---|---|
| Lowered Vitamin D Level | Sufficient Vitamin D Level | p-Value | Insulin Resistance | Absence of Insulin Resistance | p-Value | ||
| Physical Variables | Age (years) | 12.9 ± 2.2 | 12.2 ± 2.3 | 0.276 ‡ | 12.4 ± 2.2 | 11.6 ± 2.4 | 0.078 ‡ |
| Height (m) | 1.56 ± 0.1 | 1.57 ± 0.1 | 0.747 ‡ | 1.56 ± 0.1 | 1.52 ± 0.1 | 0.004 ‡ | |
| Weight (kg) | 78.3 ± 21.8 | 76.2 ± 19.8 | 0.701 ‡ | 79.0 ± 20.3 | 66.0 ± 14.7 | 0.001 ‡ | |
| Waist circumference (cm) | 100.3 ± 15.4 | 94.7 ± 13.4 | 0.195 ‡ | 97.2 ± 13.8 | 86.9 ± 8.8 | <0.001 ‡ | |
| BMI (kg/m2) | 31.6 ± 6.4 | 30.4 ± 5.0 | 0.395 ‡ | 31.0 ± 5.4 | 28.3 ± 3.6 | 0.010 ‡ | |
| BMI SDS | 2.54 ± 0.6 | 2.52 ± 0.4 | 0.861 ‡ | 2.55 ± 0.5 | 2.39 ± 0.4 | 0.098 ‡ | |
| Body fat (kg); Caliper | 20.8 ± 7.3 | 19.7 ± 6.2 | 0.564 ‡ | 20.4 ± 6.6 | 17.0 ± 4.2 | 0.002 ‡ | |
| Body fat (%); Caliper | 25.5 ± 2.6 | 25.4 ± 2.1 | 0.870 ‡ | 25.6 ± 2.2 | 24.9 ± 1.9 | 0.161 ‡ | |
| Muscle mass (kg) | 21.0 ± 6.3 | 23.3 ± 7.3 | 0.225 ‡ | 18.7 ± 3.4 | 23.9 ± 7.4 | 0.026 ‡ | |
| Muscle mass (%) | 29.1 ± 2.4 | 31.0 ± 4.3 | 0.148 ‡ | 29.9 ± 3.9 | 31.0 ± 4.2 | 0.422 ‡ | |
| Fitness parameter | Absolute cardiorespiratory fitness (W) | 100.0 ± 16.7 | 121.6 ± 34.5 | 0.003 ‡ | 121.7 ± 34.5 | 112.5 ± 30.7 | 0.460 ‡ |
| Relative cardiorespiratory fitness (W/kg) | 1.3 ± 0.3 | 1.6 ± 0.4 | 0.004 ‡ | 1.6 ± 0.4 | 1.7 ± 0.3 | 0.529 ‡ | |
| Laboratory parameters | Vitamin D (ng/mL) | 22.6 ± 9.3 | 25.97 ± 11.5 | 0.095 ‡ | |||
| Blood glucose (mg/dL) | 5.13 ± 0.5 | 5.02 ± 0.43 | 0.148 ‡ | ||||
| Insulin (µU/mL) | 27.00 ± 8.8 | 21.78 ± 8.6 | 0.115 ‡ | ||||
| HOMA index | 6.19 ± 2.2 | 4.88 ± 2.7 | 0.082 ‡ | ||||
| Model | Beta (s.e.) | p-Value | R2 (corr.) | |
|---|---|---|---|---|
| Baseline | Age (years) | 0.047 (0.226) | 0.799 | 0.205 |
| Sex | −0.033 (0.476) | 0.717 | ||
| BMI (kg/m2) | −0.789 (0.203) | 0.047 | ||
| BMI-SDS | 0.325 (1.564) | 0.235 | ||
| Absolute body fat (kg); Caliper | 1.315 (0.172) | 0.002 | ||
| Relative body fat (%); Caliper | −0.296 (0.197) | 0.067 | ||
| Absolute physical fitness (W) | −0.282 (0.019) | 0.254 | ||
| Relative physical fitness (W/kg) | 0.188 (1.261) | 0.323 | ||
| Vitamin D (ng/mL) | −0.149 (0.023) | 0.079 | ||
| Final | Vitamin D (ng/mL) | −0.154 (0.022) | 0.058 | 0.210 |
| Absolute body fat (kg); Caliper | 0.403 (0.033) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fraemke, A.; Ferrari, N.; Friesen, D.; Haas, F.; Klaudius, M.; Mahabir, E.; Schmidt, L.; Joisten, C. HOMA Index, Vitamin D Levels, Body Composition and Cardiorespiratory Fitness in Juvenile Obesity: Data from the CHILT III Programme, Cologne. Int. J. Environ. Res. Public Health 2022, 19, 2442. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042442
Fraemke A, Ferrari N, Friesen D, Haas F, Klaudius M, Mahabir E, Schmidt L, Joisten C. HOMA Index, Vitamin D Levels, Body Composition and Cardiorespiratory Fitness in Juvenile Obesity: Data from the CHILT III Programme, Cologne. International Journal of Environmental Research and Public Health. 2022; 19(4):2442. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042442
Chicago/Turabian StyleFraemke, Annika, Nina Ferrari, David Friesen, Fabiola Haas, Marlen Klaudius, Esther Mahabir, Lisa Schmidt, and Christine Joisten. 2022. "HOMA Index, Vitamin D Levels, Body Composition and Cardiorespiratory Fitness in Juvenile Obesity: Data from the CHILT III Programme, Cologne" International Journal of Environmental Research and Public Health 19, no. 4: 2442. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042442