
Long-Term Exposure to Fine Particulate Matter and the Risk of Chronic Liver Diseases: A Meta-Analysis of Observational Studies



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Study Selection and Eligibility
2.3. Data Extraction
2.4. Literature Quality Assessment
2.5. Statistical Analyses
3. Results
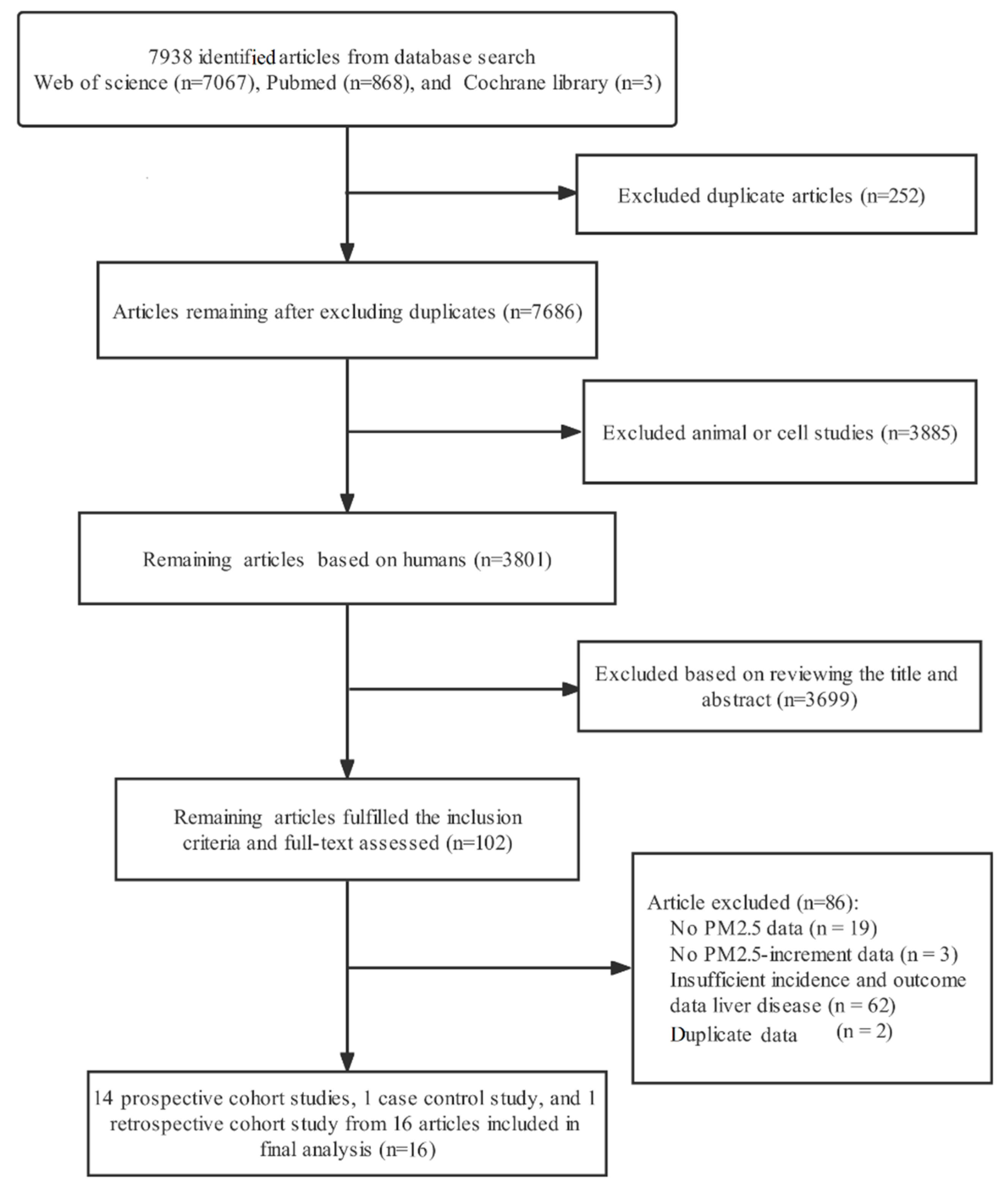
3.1. Eligible Studies
3.2. Characteristics of Studies Included in the Meta-Analysis
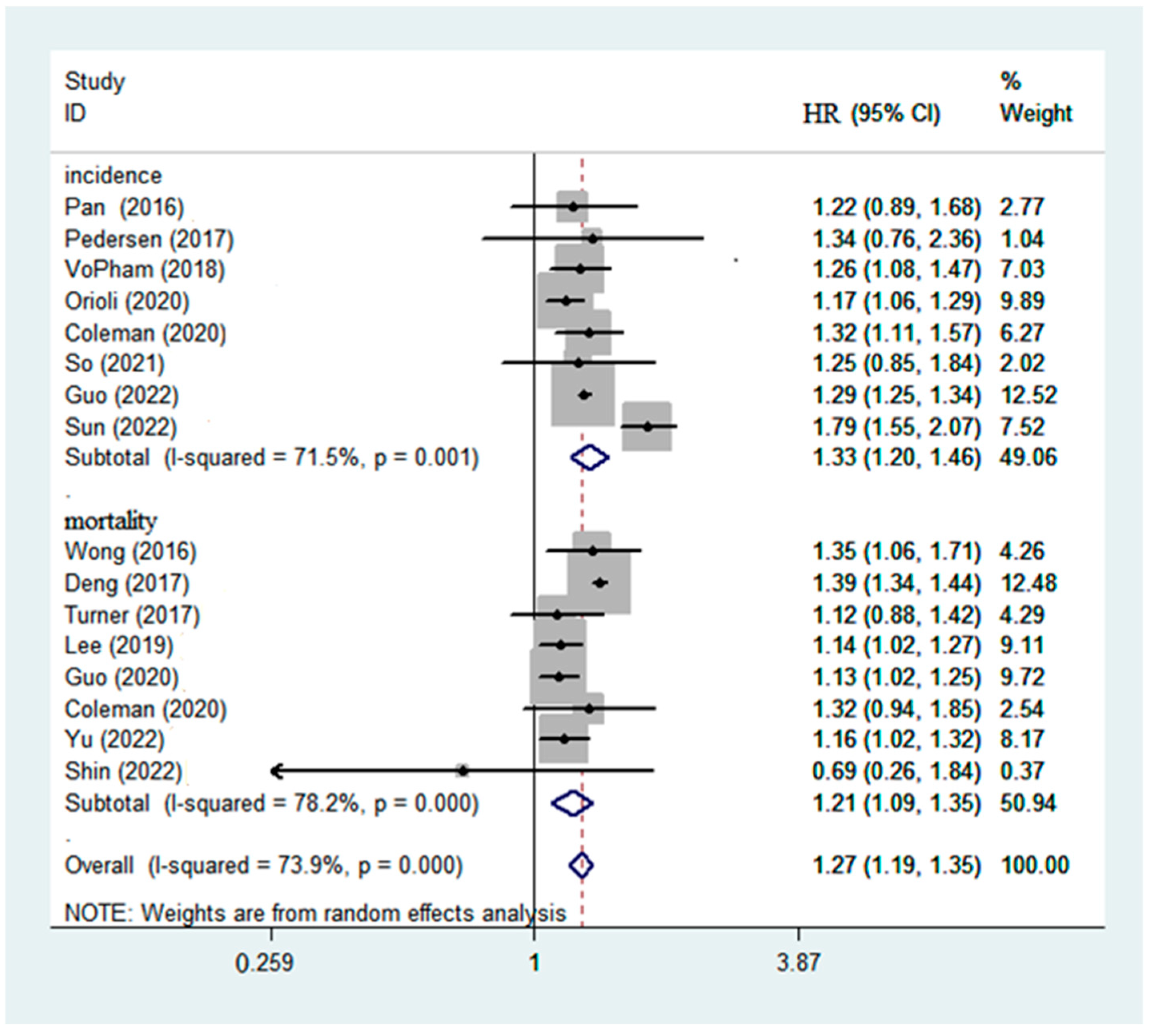
3.3. Overall Meta-Estimates and Publication Bias
3.4. Subgroup Analyses of Particulate Matter on Risk of Liver Diseases
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lu, X.; Li, R.; Yan, X. Airway hyperresponsiveness development and the toxicity of PM2.5. Environ. Sci. Pollut. Res. Int. 2021, 28, 6374–6391. [Google Scholar] [CrossRef] [PubMed]
- Shim, I.; Kim, W.; Kim, H.; Lim, Y.M.; Shin, H.; Park, K.S.; Yu, S.M.; Kim, Y.H.; Sung, H.K.; Eom, I.C.; et al. Comparative Cytotoxicity Study of PM2.5 and TSP Collected from Urban Areas. Toxics 2021, 9, 167. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhong, Y.; Liao, J.; Wang, G. PM2.5-related cell death patterns. Int. J. Med. Sci. 2021, 18, 1024–1029. [Google Scholar] [CrossRef] [PubMed]
- Shou, Y.; Huang, Y.; Zhu, X.; Liu, C.; Hu, Y.; Wang, H. A review of the possible associations between ambient PM2.5 exposures and the development of Alzheimer’s disease. Ecotoxicol. Environ. Saf. 2019, 174, 344–352. [Google Scholar] [CrossRef]
- Hamra, G.B.; Guha, N.; Cohen, A.; Laden, F.; Raaschou-Nielsen, O.; Samet, J.M.; Vineis, P.; Forastiere, F.; Saldiva, P.; Yorifuji, T.; et al. Outdoor particulate matter exposure and lung cancer: A systematic review and meta-analysis. Environ. Health Perspect. 2014, 122, 906–911. [Google Scholar] [CrossRef] [PubMed]
- Seen, S. Chronic liver disease and oxidative stress—A narrative review. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 1021–1035. [Google Scholar] [CrossRef]
- Albright, C.M.; Fay, E.E. Chronic Liver Disease in the Obstetric Patient. Clin. Obstet. Gynecol. 2020, 63, 193–210. [Google Scholar] [CrossRef] [PubMed]
- Saadati, S.; Sadeghi, A.; Mansour, A.; Yari, Z.; Poustchi, H.; Hedayati, M.; Hatami, B.; Hekmatdoost, A. Curcumin and inflammation in non-alcoholic fatty liver disease: A randomized, placebo controlled clinical trial. BMC Gastroenterol. 2019, 19, 133. [Google Scholar] [CrossRef]
- Chen, Z.; Tian, R.; She, Z.; Cai, J.; Li, H. Role of oxidative stress in the pathogenesis of nonalcoholic fatty liver disease. Free Radic. Biol. Med. 2020, 152, 116–141. [Google Scholar] [CrossRef]
- Tilg, H.; Cani, P.D.; Mayer, E.A. Gut microbiome and liver diseases. Gut 2016, 65, 2035–2044. [Google Scholar] [CrossRef]
- Tanase, D.M.; Gosav, E.M.; Costea, C.F.; Ciocoiu, M.; Lacatusu, C.M.; Maranduca, M.A.; Ouatu, A.; Floria, M. The Intricate Relationship between Type 2 Diabetes Mellitus (T2DM), Insulin Resistance (IR), and Nonalcoholic Fatty Liver Disease (NAFLD). J. Diabetes Res. 2020, 2020, 3920196. [Google Scholar] [CrossRef] [PubMed]
- Copeland, N.K.; Eller, M.A.; Kim, D.; Creegan, M.; Esber, A.; Eller, L.A.; Semwogerere, M.; Kibuuka, H.; Kiweewa, F.; Crowell, T.A.; et al. Brief Report: Increased Inflammation and Liver Disease in HIV/HBV-Coinfected Individuals. J. Acquir. Immune Defic. Syndr. 2021, 88, 310–313. [Google Scholar] [CrossRef] [PubMed]
- Abenavoli, L.; Greco, M.; Milic, N.; Accattato, F.; Foti, D.; Gulletta, E.; Luzza, F. Effect of Mediterranean Diet and Antioxidant Formulation in Non-Alcoholic Fatty Liver Disease: A Randomized Study. Nutrients 2017, 9, 870. [Google Scholar] [CrossRef] [PubMed]
- Beelen, R.; Raaschou-Nielsen, O.; Stafoggia, M.; Andersen, Z.J.; Weinmayr, G.; Hoffmann, B.; Wolf, K.; Samoli, E.; Fischer, P.; Nieuwenhuijsen, M.; et al. Effects of long-term exposure to air pollution on natural-cause mortality: An analysis of 22 European cohorts within the multicentre ESCAPE project. Lancet 2014, 383, 785–795. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Butland, B.K.; Dimitroulopoulou, C.; Heal, M.R.; Stedman, J.R.; Carslaw, N.; Jarvis, D.; Heaviside, C.; Vardoulakis, S.; Walton, H.; et al. Long-term exposure to ambient ozone and mortality: A quantitative systematic review and meta-analysis of evidence from cohort studies. BMJ Open 2016, 6, e009493. [Google Scholar] [CrossRef]
- Stafoggia, M.; Oftedal, B.; Chen, J.; Rodopoulou, S.; Renzi, M.; Atkinson, R.W.; Bauwelinck, M.; Klompmaker, J.O.; Mehta, A.; Vienneau, D.; et al. Long-term exposure to low ambient air pollution concentrations and mortality among 28 million people: Results from seven large European cohorts within the ELAPSE project. Lancet Planet. Health 2022, 6, e9–e18. [Google Scholar] [CrossRef]
- Zare Sakhvidi, M.J.; Lequy, E.; Goldberg, M.; Jacquemin, B. Air pollution exposure and bladder, kidney and urinary tract cancer risk: A systematic review. Environ. Pollut. 2020, 267, 115328. [Google Scholar] [CrossRef]
- Stieb, D.M.; Berjawi, R.; Emode, M.; Zheng, C.; Salama, D.; Hocking, R.; Lyrette, N.; Matz, C.; Lavigne, E.; Shin, H.H. Systematic review and meta-analysis of cohort studies of long term outdoor nitrogen dioxide exposure and mortality. PLoS ONE 2021, 16, e0246451. [Google Scholar] [CrossRef]
- Kim, H.B.; Shim, J.Y.; Park, B.; Lee, Y.J. Long-Term Exposure to Air Pollutants and Cancer Mortality: A Meta-Analysis of Cohort Studies. Int. J. Environ. Res. Public Health 2018, 15, 2608. [Google Scholar] [CrossRef]
- Kim, H.B.; Shim, J.Y.; Park, B.; Lee, Y.J. Long-term exposure to air pollution and the risk of non-lung cancer: A meta-analysis of observational studies. Perspect. Public Health 2020, 140, 222–231. [Google Scholar] [CrossRef]
- Pritchett, N.; Spangler, E.C.; Gray, G.M.; Livinski, A.A.; Sampson, J.N.; Dawsey, S.M.; Jones, R.R. Exposure to Outdoor Particulate Matter Air Pollution and Risk of Gastrointestinal Cancers in Adults: A Systematic Review and Meta-Analysis of Epidemiologic Evidence. Environ. Health Perspect. 2022, 130, 36001. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.H.; Zhao, M.; Yu, H.; Li, H.D. The impact of particulate matter 2.5 on the risk of hepatocellular carcinoma: A meta-analysis. Int. Arch. Occup. Environ. Health 2022, 95, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Guo, B.; Guo, Y.; Nima, Q.; Feng, Y.; Wang, Z.; Lu, R.; Baimayangji; Ma, Y.; Zhou, J.; Xu, H.; et al. Exposure to air pollution is associated with an increased risk of metabolic dysfunction-associated fatty liver disease. J. Hepatol. 2022, 76, 518–525. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Yang, Q.; Zhou, Q.; Cao, W.; Yu, S.; Zhan, S.; Sun, F. Long-term exposure to air pollution, habitual physical activity and risk of non-alcoholic fatty liver disease: A prospective cohort study. Ecotoxicol. Environ. Saf. 2022, 235, 113440. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef]
- Yang, W.S.; Wang, X.; Deng, Q.; Fan, W.Y.; Wang, W.Y. An evidence-based appraisal of global association between air pollution and risk of stroke. Int. J. Cardiol. 2014, 175, 307–313. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Lee, C.H.; Hsieh, S.Y.; Huang, W.H.; Wang, I.K.; Yen, T.H. Association between Ambient Particulate Matter 2.5 Exposure and Mortality in Patients with Hepatocellular Carcinoma. Int. J. Environ. Res. Public Health 2019, 16, 2490. [Google Scholar] [CrossRef]
- Pan, W.C.; Wu, C.D.; Chen, M.J.; Huang, Y.T.; Chen, C.J.; Su, H.J.; Yang, H.I. Fine Particle Pollution, Alanine Transaminase, and Liver Cancer: A Taiwanese Prospective Cohort Study (REVEAL-HBV). J. Natl. Cancer Inst. 2016, 108, djv341. [Google Scholar] [CrossRef]
- Pedersen, M.; Andersen, Z.J.; Stafoggia, M.; Weinmayr, G.; Galassi, C.; Sorensen, M.; Eriksen, K.T.; Tjonneland, A.; Loft, S.; Jaensch, A.; et al. Ambient air pollution and primary liver cancer incidence in four European cohorts within the ESCAPE project. Environ. Res. 2017, 154, 226–233. [Google Scholar] [CrossRef] [PubMed]
- VoPham, T.; Bertrand, K.A.; Tamimi, R.M.; Laden, F.; Hart, J.E. Ambient PM(2.5) air pollution exposure and hepatocellular carcinoma incidence in the United States. Cancer Causes Control 2018, 29, 563–572. [Google Scholar] [CrossRef]
- Orioli, R.; Solimini, A.G.; Michelozzi, P.; Forastiere, F.; Davoli, M.; Cesaroni, G. A cohort study on long-term exposure to air pollution and incidence of liver cirrhosis. Environ. Epidemiol. 2020, 4, e109. [Google Scholar] [CrossRef] [PubMed]
- Coleman, N.C.; Burnett, R.T.; Ezzati, M.; Marshall, J.D.; Robinson, A.L.; Pope, C.A., 3rd. Fine Particulate Matter Exposure and Cancer Incidence: Analysis of SEER Cancer Registry Data from 1992–2016. Environ. Health Perspect. 2020, 128, 107004. [Google Scholar] [CrossRef] [PubMed]
- So, R.; Chen, J.; Mehta, A.J.; Liu, S.; Strak, M.; Wolf, K.; Hvidtfeldt, U.A.; Rodopoulou, S.; Stafoggia, M.; Klompmaker, J.O.; et al. Long-term exposure to air pollution and liver cancer incidence in six European cohorts. Int. J. Cancer 2021, 149, 1887–1897. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.M.; Tsang, H.; Lai, H.K.; Thomas, G.N.; Lam, K.B.; Chan, K.P.; Zheng, Q.; Ayres, J.G.; Lee, S.Y.; Lam, T.H.; et al. Cancer Mortality Risks from Long-term Exposure to Ambient Fine Particle. Cancer Epidemiol. Biomark. Prev. 2016, 25, 839–845. [Google Scholar] [CrossRef]
- Deng, H.; Eckel, S.P.; Liu, L.; Lurmann, F.W.; Cockburn, M.G.; Gilliland, F.D. Particulate matter air pollution and liver cancer survival. Int. J. Cancer 2017, 141, 744–749. [Google Scholar] [CrossRef]
- Turner, M.C.; Krewski, D.; Diver, W.R.; Pope, C.A., 3rd; Burnett, R.T.; Jerrett, M.; Marshall, J.D.; Gapstur, S.M. Ambient Air Pollution and Cancer Mortality in the Cancer Prevention Study II. Environ. Health Perspect. 2017, 125, 087013. [Google Scholar] [CrossRef]
- Guo, C.; Chan, T.C.; Teng, Y.C.; Lin, C.; Bo, Y.; Chang, L.Y.; Lau, A.K.H.; Tam, T.; Wong, M.C.S.; Lao, X.Q. Long-term exposure to ambient fine particles and gastrointestinal cancer mortality in Taiwan: A cohort study. Environ. Int. 2020, 138, 105640. [Google Scholar] [CrossRef]
- Coleman, N.C.; Burnett, R.T.; Higbee, J.D.; Lefler, J.S.; Merrill, R.M.; Ezzati, M.; Marshall, J.D.; Kim, S.Y.; Bechle, M.; Robinson, A.L.; et al. Cancer mortality risk, fine particulate air pollution, and smoking in a large, representative cohort of US adults. Cancer Causes Control 2020, 31, 767–776. [Google Scholar] [CrossRef]
- Yu, P.; Xu, R.; Li, S.; Coelho, M.; Saldiva, P.H.N.; Sim, M.R.; Abramson, M.J.; Guo, Y. Associations between long-term exposure to PM(2.5) and site-specific cancer mortality: A nationwide study in Brazil between 2010 and 2018. Environ. Pollut. 2022, 302, 119070. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.; Kim, O.J.; Yang, S.; Choe, S.A.; Kim, S.Y. Different Mortality Risks of Long-Term Exposure to Particulate Matter across Different Cancer Sites. Int. J. Environ. Res. Public Health 2022, 19, 3180. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Li, Y.; Li, G.; Zhang, Y.; Li, J.; Haosheng, C. Fluorescent reconstitution on deposition of PM2.5 in lung and extrapulmonary organs. Proc. Natl. Acad. Sci. USA 2019, 116, 2488–2493. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.J.; Tan, H.Y.; Lee, C.Y.; Cho, H. An Air Particulate Pollutant Induces Neuroinflammation and Neurodegeneration in Human Brain Models. Adv. Sci. 2021, 8, e2101251. [Google Scholar] [CrossRef] [PubMed]
- Ran, Z.; An, Y.; Zhou, J.; Yang, J.; Zhang, Y.; Yang, J.; Wang, L.; Li, X.; Lu, D.; Zhong, J.; et al. Subchronic exposure to concentrated ambient PM2.5 perturbs gut and lung microbiota as well as metabolic profiles in mice. Environ. Pollut. 2021, 272, 115987. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Zhang, C.; Zhao, J.; Li, D.; Chen, J. Exposure to concentrated ambient PM2.5 (CAPM) induces intestinal disturbance via inflammation and alternation of gut microbiome. Environ. Int. 2022, 161, 107138. [Google Scholar] [CrossRef]
- Ma, X.N.; Li, R.Q.; Xie, J.L.; Li, S.H.; Li, J.W.; Yan, X.X. PM2.5-induced inflammation and myocardial cell injury in rats. Eur. Rev. Med. Pharm. Sci. 2021, 25, 6670–6677. [Google Scholar] [CrossRef]
- Zhang, Z.; Hu, S.; Fan, P.; Li, L.; Feng, S.; Xiao, H.; Zhu, L. The Roles of Liver Inflammation and the Insulin Signaling Pathway in PM2.5 Instillation-Induced Insulin Resistance in Wistar Rats. Dis. Markers 2021, 2021, 2821673. [Google Scholar] [CrossRef]
- Xu, M.X.; Ge, C.X.; Qin, Y.T.; Gu, T.T.; Lou, D.S.; Li, Q.; Hu, L.F.; Feng, J.; Huang, P.; Tan, J. Prolonged PM2.5 exposure elevates risk of oxidative stress-driven nonalcoholic fatty liver disease by triggering increase of dyslipidemia. Free Radic. Biol. Med. 2019, 130, 542–556. [Google Scholar] [CrossRef]
- Song, L.; Jiang, S.; Pan, K.; Du, X.; Zeng, X.; Zhang, J.; Zhou, J.; Sun, Q.; Xie, Y.; Zhao, J. AMPK activation ameliorates fine particulate matter-induced hepatic injury. Environ. Sci. Pollut. Res. Int. 2020, 27, 21311–21319. [Google Scholar] [CrossRef]
- Leilei, L.; Wenke, Q.; Yuyuan, L.; Sihang, L.; Xue, S.; Weiqiang, C.; Lianbao, Y.; Ying, W.; Yan, L.; Ming, L. Oleanolic acid-loaded nanoparticles attenuate activation of hepatic stellate cells via suppressing TGF-β1 and oxidative stress in PM2.5-exposed hepatocytes. Toxicol. Appl. Pharmacol. 2022, 437, 115891. [Google Scholar] [CrossRef] [PubMed]
- Ding, S.; Yuan, C.; Si, B.; Wang, M.; Da, S.; Bai, L.; Wu, W. Combined effects of ambient particulate matter exposure and a high-fat diet on oxidative stress and steatohepatitis in mice. PLoS ONE 2019, 14, e0214680. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Li, Z.; Ye, Y.; Xie, L.; Li, W. Oxidative Stress and Liver Cancer: Etiology and Therapeutic Targets. Oxid. Med. Cell. Longev. 2016, 2016, 7891574. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.W.; Dai, C.M.; Chen, X.H.; Feng, J.F. The Relationship between Serum Trace Elements and Oxidative Stress of Patients with Different Types of Cancer. Oxid. Med. Cell. Longev. 2021, 2021, 4846951. [Google Scholar] [CrossRef]
- Wang, W.; Zhou, J.; Chen, M.; Huang, X.; Xie, X.; Li, W.; Cao, Q.; Kan, H.; Xu, Y.; Ying, Z. Exposure to concentrated ambient PM2.5 alters the composition of gut microbiota in a murine model. Part. Fibre Toxicol. 2018, 15, 17. [Google Scholar] [CrossRef]
- Shan, S.; Xiong, Y.; Guo, J.; Liu, M.; Gao, X.; Fu, X.; Zeng, D.; Song, C.; Zhang, Y.; Cheng, D.; et al. Effect of an inulin-type fructan from Platycodon grandiflorum on the intestinal microbiota in rats exposed to PM2.5. Carbohydr. Polym. 2022, 283, 119147. [Google Scholar] [CrossRef]
- Wu, Y.; Pei, C.; Wang, X.; Wang, M.; Huang, D.; Wang, F.; Xiao, W.; Wang, Z. Effect of probiotics on nasal and intestinal microbiota in people with high exposure to particulate matter ≤ 2.5 mum (PM2.5): A randomized, double-blind, placebo-controlled clinical study. Trials 2020, 21, 850. [Google Scholar] [CrossRef]
- Zhao, L.; Fang, J.; Tang, S.; Deng, F.; Liu, X.; Shen, Y.; Liu, Y.; Kong, F.; Du, Y.; Cui, L.; et al. PM2.5 and Serum Metabolome and Insulin Resistance, Potential Mediation by the Gut Microbiome: A Population-Based Panel Study of Older Adults in China. Environ. Health Perspect. 2022, 130, 27007. [Google Scholar] [CrossRef]
- Jones, R.M.; Neish, A.S. Gut Microbiota in Intestinal and Liver Disease. Annu. Rev. Pathol. 2021, 16, 251–275. [Google Scholar] [CrossRef]
- Zhang, X.; Coker, O.O.; Chu, E.S.; Fu, K.; Lau, H.C.H.; Wang, Y.X.; Chan, A.W.H.; Wei, H.; Yang, X.; Sung, J.J.Y.; et al. Dietary cholesterol drives fatty liver-associated liver cancer by modulating gut microbiota and metabolites. Gut 2021, 70, 761–774. [Google Scholar] [CrossRef]
- Haberzettl, P.; O’Toole, T.E.; Bhatnagar, A.; Conklin, D.J. Exposure to Fine Particulate Air Pollution Causes Vascular Insulin Resistance by Inducing Pulmonary Oxidative Stress. Environ. Health Perspect. 2016, 124, 1830–1839. [Google Scholar] [CrossRef] [PubMed]
- Muzurovic, E.; Mikhailidis, D.P.; Mantzoros, C. Non-alcoholic fatty liver disease, insulin resistance, metabolic syndrome and their association with vascular risk. Metabolism 2021, 119, 154770. [Google Scholar] [CrossRef] [PubMed]
- Clair, H.B.; Pinkston, C.M.; Rai, S.N.; Pavuk, M.; Dutton, N.D.; Brock, G.N.; Prough, R.A.; Falkner, K.C.; McClain, C.J.; Cave, M.C. Liver Disease in a Residential Cohort with Elevated Polychlorinated Biphenyl Exposures. Toxicol. Sci. 2018, 164, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Niehoff, N.M.; Zabor, E.C.; Satagopan, J.; Widell, A.; O’Brien, T.R.; Zhang, M.; Rothman, N.; Grimsrud, T.K.; Van Den Eeden, S.K.; Engel, L.S. Prediagnostic serum polychlorinated biphenyl concentrations and primary liver cancer: A case-control study nested within two prospective cohorts. Environ. Res. 2020, 187, 109690. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.; Pahkala, K.; Juonala, M.; Jaakkola, J.; Rovio, S.P.; Lehtimaki, T.; Sabin, M.A.; Jula, A.; Hutri-Kahonen, N.; Laitinen, T.; et al. Childhood and Adulthood Passive Smoking and Nonalcoholic Fatty Liver in Midlife: A 31-year Cohort Study. Am. J. Gastroenterol. 2021, 116, 1256–1263. [Google Scholar] [CrossRef]
- Lee, S.; Lee, H.A.; Park, B.; Han, H.; Park, B.H.; Oh, S.Y.; Hong, Y.S.; Ha, E.H.; Park, H. A prospective cohort study of the association between bisphenol A exposure and the serum levels of liver enzymes in children. Environ. Res. 2018, 161, 195–201. [Google Scholar] [CrossRef]
- Park, E.; Kim, J.; Kim, B.; Park, E.Y. Association between environmental exposure to cadmium and risk of suspected non-alcoholic fatty liver disease. Chemosphere 2021, 266, 128947. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Studies | Study Design | Location | Years Enrolled | Age Range (Years) | Gender | Sample Size | Health Effects | Adjustment Variables | NOS |
|---|---|---|---|---|---|---|---|---|---|
| Pan et al. [30] (2016) | Prospective Cohort Study | Taiwan | 1991–1992 | 30–65 | Male/female | 464 | Increased incidence of liver cancer | Age 40 to 49 years, males, positive for HBsAg serostatus, positive for anti-HCV serostatus, and had alcohol consumption habit | 9 |
| Pedersen et al. [31] (2017) | Prospective Cohort Study | Denmark, Austria and Italy | 1985–2005 | 42–57 | Male/female | 279 | Increased incidence of liver cancer | Age (time scale), sex, calendar time smoking status, alcohol, occupational exposure, employment status, education, area-level SES | 9 |
| VoPham et al. [32] (2018) | Prospective Cohort Study | USA | 2000–2014 | 50–74 | Male/female | 56,245 | Increased incidence of liver cancer | Age at diagnosis, sex, race, year of diagnosis, SEER registry, prevalence of heavy alcohol consumption, smoking, obesity, diabetes; population density; median household income; percentage with a bachelor’s degree or higher; percentage unemployed; percentage of individuals below the poverty level; percentage foreign born; urbanicity; and ambient UV exposure | 9 |
| Orioli et al. [33] (2020) | Prospective Cohort Study | Italy | 2001–2005 | ≥30 | Male/female | 10,111 | Increased incidence of liver cirrhosis | Sex, age, educational level, occupational status, marital status, place of birth, and area-level SEP | 9 |
| Coleman et al. [34] (2020) | Prospective Cohort Study | USA | 1992–2016 | 18–84 | Male/female | 185,012 | Increased incidence of liver cancer | percentage of the county in various age buckets; percentage male; percentage White, Black, Hispanic, and other; percentage who did not graduate high school, graduated high school, or obtained more education than high school; median income, rent, and home value; percentage below 150% poverty; percentage working class; percentage unemployed; percentage living in a rural area; percentage smokers; percentage who consume alcohol; percentage who are physically active; and percentage of individuals in a county who are obese using LOESS models with 3 df. | 9 |
| Guo et al. [23] (2022) | a Cross-Sectional Study | China | 2018–2019 | 41–64 | Male/female | 17,951 | Increased incidence of metabolic dysfunction-associated fatty liver disease | Age, sex, ethnicity, education attainment, annual household income, study region, alcohol consumption, smoking status, second-hand smoke, high fat intake, low fruit and vegetable intake, physical activity, and indoor air pollution | 9 |
| So et al. [35] (2021) | Prospective Cohort Study | Sweden, Denmark, Netherland, France, Austria | 1985–2015 | 34–62 | Male/female | 512 | Increased incidence of liver cancer | Age (time scale), sex (strata), subcohort (strata), calendar year of baseline, smoking status, employment status, and mean income at the neighborhood level in 2001 | 9 |
| Sun et al. [24] (2022) | Prospective Cohort Study | Taiwan | 2001–2016 | 46–65 | Male/female | 35,614 | Increased incidence of non-alcoholic fatty liver disease | Age, year of enrollment, season of measurement, gender, smoking status, alcohol consumption, occupational exposure, educational attainment, vegetable intake, fruit intake, sugar drink intake, fried food intake, habitual physical activity, physical activity at work, cancer, long-term use of hyperlipidemia drugs, cardiovascular disease, and hypertension | 9 |
| Wong et al. [36] (2016) | Prospective Cohort Study | Hong Kong | 1998–2011 | ≥65 | Male/female | 676 | Increased mortality of liver cancer | Age (year), Gender, BMI quartiles, Smoking, Exercise (days/week), Education, Monthly expenditure (USD) | 9 |
| Deng et al. [37] (2017) | Prospective Cohort Study | USA | 2000–2009 | 51–77 | Male/female | 20,221 | Increased mortality of liver cancer | Age, sex, race/ethnicity, marital status, socioeconomic status, rural–urban commuting area, distance to primary interstate highway, distance to primary US and state highways, month of diagnosis, year of diagnosis and initial treatments | 9 |
| Turner et al. [38] (2017) | Prospective Cohort Study | Canada | 1982–2004 | Majority: 40–69 | Male/female | 1003 | Increased mortality of liver cancer | Age, race/ethnicity, gender stratified and adjusted for baseline values of education; marital status; body mass index; body mass index squared; smoking status; cigarettes per day; cigarettes per day squared; duration of smoking; duration of smoking squared; age started smoking; passive smoking, vegetable/fruit/fiber consumption; fat consumption; beer, wine, liquor consumption; industrial exposures; occupation dirtiness index; and 1990 ecological covariates | 9 |
| Lee et al. [29] (2019) | Retrospective Cohort Study | Taiwan | 2000–2009 | 49–74 | Male/female | 1003 | Increased mortality of liver cancer | Child–Pugh score, macrovascular invasion | 8 |
| Guo et al. [39] (2020) | Prospective Cohort Study | Taiwan | 2001–2014 | ≥18 | Male/female | 611 | Increased mortality of liver cancer | Age, sex, education, BMI, cigarette smoking, alcohol drinking, physical activity, vegetable and fruit intake, occupational exposure, season and year of enrolment | 9 |
| Coleman et al. [40] (2020) | Prospective Cohort Study | USA | 1987–2014. | 18–84 | Male/female | 761 | Increased mortality of liver cancer | buckets) and categorical variables for BMI, income, education, marital status, rural versus urban, region, and survey year | 9 |
| Yu et al. [41] (2022) | Prospective Cohort Study | Brazil | 2010–2018 | ≥20 | Male/female | 82,297 | Increased mortality of liver cancer | The result was estimated by random effect meta-analysis with no statistical adjustment, because those models were based on the same sample. | 8 |
| Shin et al. [42] (2022) | Prospective Cohort Study | Korea | 2007–2015 | Mean age: 46.58 | Male/female | 651 | Increased mortality of liver cancer | Age, sex, Health insurance premium, Employment status, Cigarette smoking status, Cigarette smoking amount (pack per day), Cigarette smoking period (year), Alcohol consumption, Physical activity, Nutrition, BMI, Family history of cancer, district-level of Elderly population, completeness of high school graduates, Gross Regional Domestic Product, and Population density, Area type, Health screening participation | 9 |
| Total Studies | Incidence | Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No. of Study | Pooled HR (95% CI) | I2 (%) | No. of Study | Pooled HR (95% CI) | I2(%) | No. of Study | Pooled HR (95% CI) | I2 (%) | |
| Region | |||||||||
| Asia | 7 | 1.29 (1.14–1.45) | 82.3 | 3 | 1.43 (1.11–1.84) | 89.6 | 4 | 1.15 (1.07–1.23) | 0 |
| Europe | 4 | 1.17 (1.09–1.26) | 0 | 3 | 1.18 (1.08–1.29) | 0 | 1 | 1.16 (1.02–1.32) | NA |
| North America | 5 | 1.35 (1.27–1.43) | 15 | 2 | 1.29 (1.15–1.46) | 0 | 3 | 1.32 (1.16–1.50) | 36.9 |
| Type of disease | |||||||||
| Liver cancer | 13 | 1.23 (1.14–1.33) | 63.4 | 5 | 1.28 (1.15–1.42) | 0 | 8 | 1.21 (1.09–1.35) | 78.2 |
| Liver cirrhosis | 1 | 1.17 (1.06–1.29) | NA | 1 | 1.17 (1.06–1.29) | NA | 0 | NA | NA |
| Fatty liver disease | 2 | 1.51 (1.09–2.08) | 94.7 | 2 | 1.51 (1.09–2.08) | 94.7 | 0 | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sui, J.; Xia, H.; Zhao, Q.; Sun, G.; Cai, Y. Long-Term Exposure to Fine Particulate Matter and the Risk of Chronic Liver Diseases: A Meta-Analysis of Observational Studies. Int. J. Environ. Res. Public Health 2022, 19, 10305. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610305
Sui J, Xia H, Zhao Q, Sun G, Cai Y. Long-Term Exposure to Fine Particulate Matter and the Risk of Chronic Liver Diseases: A Meta-Analysis of Observational Studies. International Journal of Environmental Research and Public Health. 2022; 19(16):10305. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610305
Chicago/Turabian StyleSui, Jing, Hui Xia, Qun Zhao, Guiju Sun, and Yinyin Cai. 2022. "Long-Term Exposure to Fine Particulate Matter and the Risk of Chronic Liver Diseases: A Meta-Analysis of Observational Studies" International Journal of Environmental Research and Public Health 19, no. 16: 10305. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610305