
PM2.5-Associated Hospitalization Risk of Cardiovascular Diseases in Wuhan: Cases Alleviated by Residential Greenness
 ,
,
Abstract
:1. Introduction
2. Method
2.1. Study Area and Population
2.2. Air Pollution Assessment
2.3. Residential Greenness Assessment
2.4. Study Design
2.5. Analytic Model
2.6. Sensitivity Analysis
3. Results
3.1. Study Population
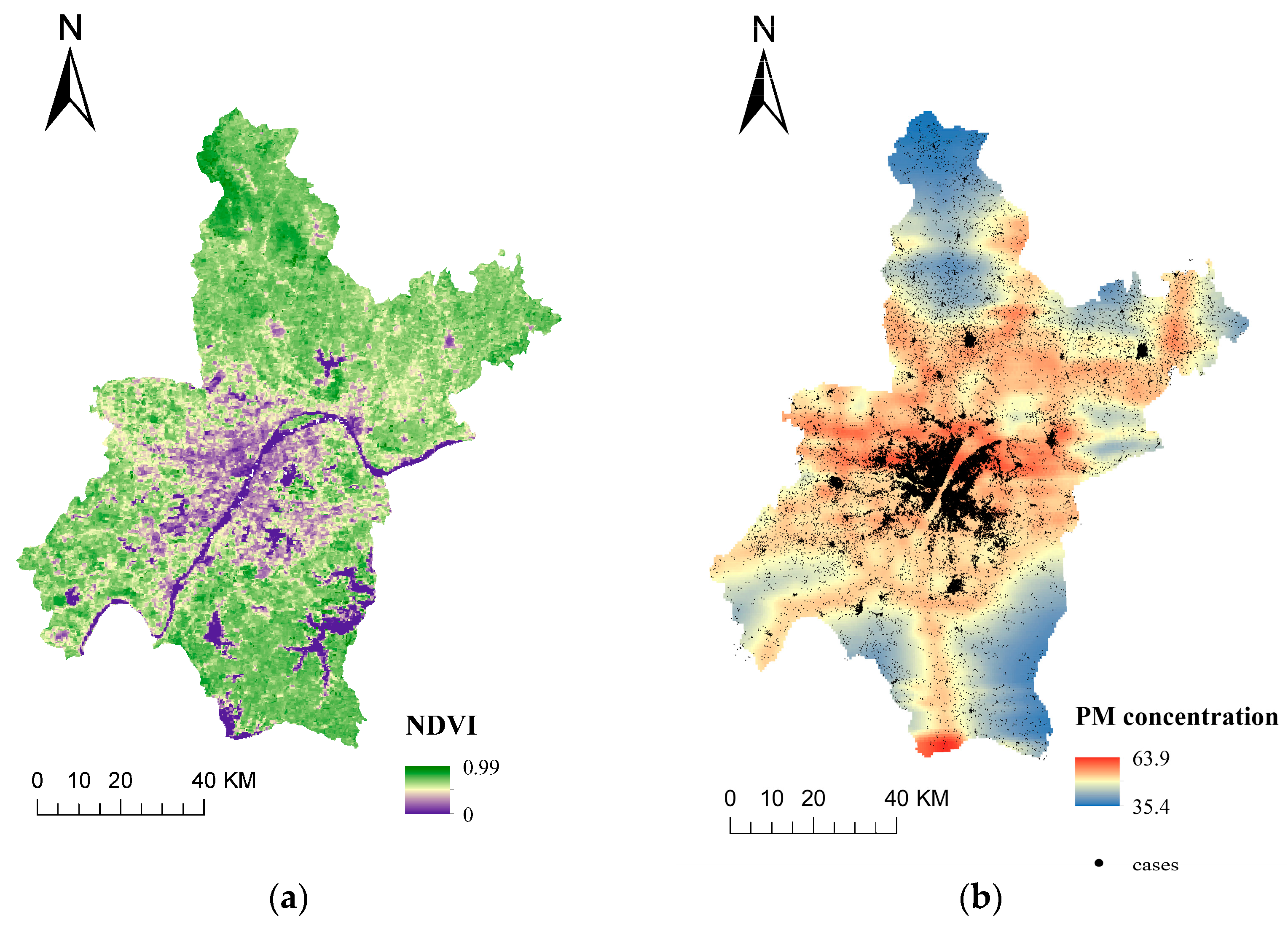
3.2. Residential Greenness and PM2.5 Assessment
3.3. Primary Model Results
3.4. Modification Effects of Greenness
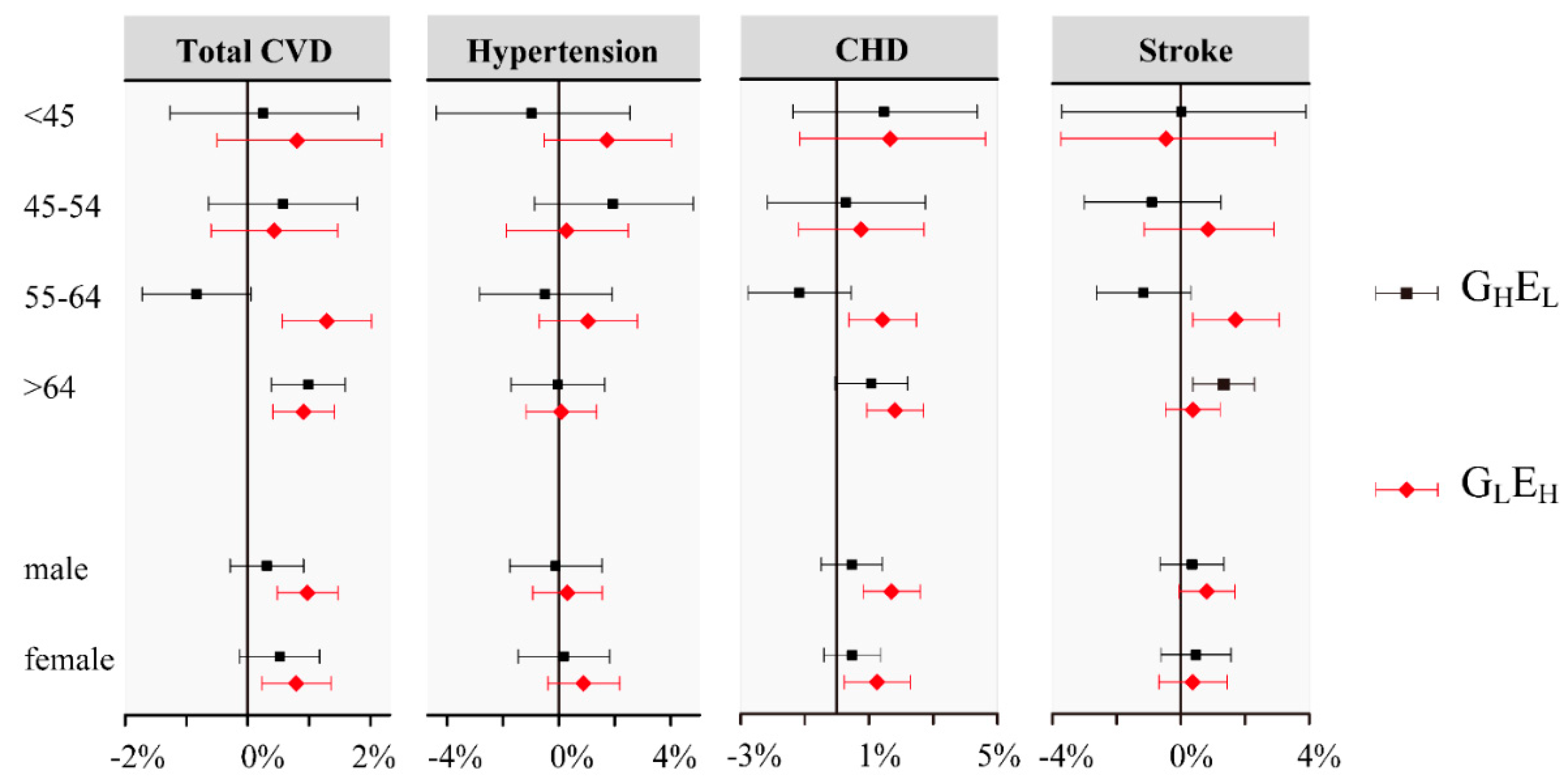
3.5. Stratification Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.; Liu, J.; Wang, M.; Zhang, X.; Zhou, M. Epidemiology of cardiovascular disease in China: Current features and implications. Nat. Rev. Cardiol. 2019, 16, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Moran, A.; Gu, D.; Zhao, D.; Coxson, P.; Wang, Y.C.; Chen, C.S.; Liu, J.; Cheng, J.; Bibbins-Domingo, K.; Shen, Y.M.; et al. Future cardiovascular disease in china: Markov model and risk factor scenario projections from the coronary heart disease policy model-china. Circ. Cardiovasc. Qual. Outcomes 2010, 3, 243–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holgate, S. Air pollution is a public health emergency. BMJ (Clin. Res. Ed.) 2022, 378, o1664. [Google Scholar] [CrossRef]
- Liu, C.; Chen, R.; Sera, F.; Vicedo-Cabrera, A.M.; Guo, Y.; Tong, S.; Coelho, M.; Saldiva, P.H.N.; Lavigne, E.; Matus, P.; et al. Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. N. Engl. J. Med. 2019, 381, 705–715. [Google Scholar] [CrossRef]
- Liu, C.; Chan, K.H.; Lv, J.; Lam, H.; Newell, K.; Meng, X.; Liu, Y.; Chen, R.; Kartsonaki, C.; Wright, N.; et al. Long-Term Exposure to Ambient Fine Particulate Matter and Incidence of Major Cardiovascular Diseases: A Prospective Study of 0.5 Million Adults in China. Environ. Sci. Technol. 2022, 56, 13200–13211. [Google Scholar] [CrossRef]
- Liang, F.; Liu, F.; Huang, K.; Yang, X.; Li, J.; Xiao, Q.; Chen, J.; Liu, X.; Cao, J.; Shen, C.; et al. Long-Term Exposure to Fine Particulate Matter and Cardiovascular Disease in China. J. Am. Coll. Cardiol. 2020, 75, 707–717. [Google Scholar] [CrossRef]
- Klompmaker, J.O.; Hart, J.E.; James, P.; Sabath, M.B.; Wu, X.; Zanobetti, A.; Dominici, F.; Laden, F. Air pollution and cardiovascular disease hospitalization—Are associations modified by greenness, temperature and humidity? Environ. Int. 2021, 156, 106715. [Google Scholar] [CrossRef]
- Twohig-Bennett, C.; Jones, A. The health benefits of the great outdoors: A systematic review and meta-analysis of greenspace exposure and health outcomes. Environ. Res 2018, 166, 628–637. [Google Scholar] [CrossRef]
- Heo, S.; Bell, M.L. The influence of green space on the short-term effects of particulate matter on hospitalization in the U.S. for 2000–2013. Environ. Res. 2019, 174, 61–68. [Google Scholar] [CrossRef]
- Zheng, C.; Tang, H.; Wang, X.; Chen, Z.; Zhang, L.; Kang, Y.; Yang, Y.; Chen, L.; Zhou, H.; Cai, J.; et al. Left ventricular diastolic dysfunction and cardiovascular disease in different ambient air pollution conditions: A prospective cohort study. Sci. Total Environ. 2022, 831, 154872. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Kan, H.; Chen, B.; Huang, W.; Bai, Z.; Song, G.; Pan, G.; Group, C.C. Association of particulate air pollution with daily mortality: The China Air Pollution and Health Effects Study. Am. J. Epidemiol. 2012, 175, 1173–1181. [Google Scholar] [CrossRef] [Green Version]
- Huang, Z.H.; Liu, X.Y.; Zhao, T.; Jiao, K.Z.; Ma, X.X.; Ren, Z.; Qiu, Y.F.; Liao, J.L.; Ma, L. Short-term effects of air pollution on respiratory diseases among young children in Wuhan city, China. World J. Pediatr. WJP 2022, 18, 333–342. [Google Scholar] [CrossRef] [PubMed]
- Ren, Z.; Liu, X.; Liu, T.; Chen, D.; Jiao, K.; Wang, X.; Suo, J.; Yang, H.; Liao, J.; Ma, L. Effect of ambient fine particulates (PM(2.5)) on hospital admissions for respiratory and cardiovascular diseases in Wuhan, China. Respir. Res. 2021, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Reid, C.E.; Kubzansky, L.D.; Li, J.; Shmool, J.L.; Clougherty, J.E. It’s not easy assessing greenness: A comparison of NDVI datasets and neighborhood types and their associations with self-rated health in New York City. Health Place 2018, 54, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Liu, C.; Chen, R.; Wang, W.; Li, W.; Kan, H.; Fu, C. Ambient air pollution and daily hospital admissions for mental disorders in Shanghai, China. Sci. Total Environ. 2018, 613–614, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.; Li, X.; Wang, S.; Wang, C.; Huang, F.; Gao, Q.; Wu, L.; Tao, L.; Guo, J.; Wang, W.; et al. Fine Particulate Air Pollution and Hospital Emergency Room Visits for Respiratory Disease in Urban Areas in Beijing, China, in 2013. PLoS ONE 2016, 11, e0153099. [Google Scholar] [CrossRef]
- Carracedo-Martínez, E.; Taracido, M.; Tobias, A.; Saez, M.; Figueiras, A. Case-crossover analysis of air pollution health effects: A systematic review of methodology and application. Environ. Health Perspect. 2010, 118, 1173–1182. [Google Scholar] [CrossRef] [Green Version]
- Hsu, W.H.; Hwang, S.A.; Kinney, P.L.; Lin, S. Seasonal and temperature modifications of the association between fine particulate air pollution and cardiovascular hospitalization in New York state. Sci. Total Environ. 2017, 578, 626–632. [Google Scholar] [CrossRef] [Green Version]
- Qiu, X.; Wei, Y.; Wang, Y.; Di, Q.; Sofer, T.; Awad, Y.A.; Schwartz, J. Inverse probability weighted distributed lag effects of short-term exposure to PM(2.5) and ozone on CVD hospitalizations in New England Medicare participants—Exploring the causal effects. Environ. Res. 2020, 182, 109095. [Google Scholar] [CrossRef]
- Andersen, Z.J.; Olsen, T.S.; Andersen, K.K.; Loft, S.; Ketzel, M.; Raaschou-Nielsen, O. Association between short-term exposure to ultrafine particles and hospital admissions for stroke in Copenhagen, Denmark. Eur. Heart J. 2010, 31, 2034–2040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sørensen, M.; Daneshvar, B.; Hansen, M.; Dragsted, L.O.; Hertel, O.; Knudsen, L.; Loft, S. Personal PM2.5 exposure and markers of oxidative stress in blood. Environ. Health Perspect. 2003, 111, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, J.; Xie, Y.; Qian, X.; Jiang, R.; Song, W. Acute effects of fine particles on cardiovascular system: Differences between the spontaneously hypertensive rats and wistar kyoto rats. Toxicol. Lett. 2010, 193, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Yitshak-Sade, M.; James, P.; Kloog, I.; Hart, J.E.; Schwartz, J.D.; Laden, F.; Lane, K.J.; Fabian, M.P.; Fong, K.C.; Zanobetti, A. Neighborhood Greenness Attenuates the Adverse Effect of PM2.5 on Cardiovascular Mortality in Neighborhoods of Lower Socioeconomic Status. Int. J. Environ. Res. Public Health 2019, 16, 814. [Google Scholar] [CrossRef] [Green Version]
- Xu, R.; Li, S.; Li, S.; Wong, E.M.; Southey, M.C.; Hopper, J.L.; Abramson, M.J.; Guo, Y. Residential surrounding greenness and DNA methylation: An epigenome-wide association study. Environ. Int. 2021, 154, 106556. [Google Scholar] [CrossRef]
- Dadvand, P.; de Nazelle, A.; Triguero-Mas, M.; Schembari, A.; Cirach, M.; Amoly, E.; Figueras, F.; Basagaña, X.; Ostro, B.; Nieuwenhuijsen, M. Surrounding greenness and exposure to air pollution during pregnancy: An analysis of personal monitoring data. Environ. Health Perspect. 2012, 120, 1286–1290. [Google Scholar] [CrossRef]
- Chen, J.; Yu, X.; Bi, H.; Fu, Y. Indoor simulations reveal differences among plant species in capturing particulate matter. PLoS ONE 2017, 12, e0177539. [Google Scholar] [CrossRef] [Green Version]
- Sæbø, A.; Popek, R.; Nawrot, B.; Hanslin, H.M.; Gawronska, H.; Gawronski, S.W. Plant species differences in particulate matter accumulation on leaf surfaces. Sci. Total Environ. 2012, 427–428, 347–354. [Google Scholar] [CrossRef]
- van den Berg, A.E.; Maas, J.; Verheij, R.A.; Groenewegen, P.P. Green space as a buffer between stressful life events and health. Soc. Sci. Med. 2010, 70, 1203–1210. [Google Scholar] [CrossRef] [Green Version]
- James, P.; Banay, R.F.; Hart, J.E.; Laden, F. A Review of the Health Benefits of Greenness. Curr. Epidemiol. Rep. 2015, 2, 131–142. [Google Scholar] [CrossRef]
- Aram, F.; Higueras García, E.; Solgi, E.; Mansournia, S. Urban green space cooling effect in cities. Heliyon 2019, 5, e01339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.; Tian, L.; Cao, W.; Lai, P.C.; Wong, P.P.Y.; Lee, R.S.; Mason, T.G.; Krämer, A.; Wong, C.M. Urban climate modified short-term association of air pollution with pneumonia mortality in Hong Kong. Sci. Total Environ. 2019, 646, 618–624. [Google Scholar] [CrossRef]
- Vienneau, D.; de Hoogh, K.; Faeh, D.; Kaufmann, M.; Wunderli, J.M.; Roosli, M.; Group, S.N.C.S. More than clean air and tranquillity: Residential green is independently associated with decreasing mortality. Environ. Int. 2017, 108, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Hao, T.; Rimm, E.B.; Willett, W.C.; Hu, F.B. Changes in diet and lifestyle and long-term weight gain in women and men. N. Engl. J. Med. 2011, 364, 2392–2404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuzeki, E.; Engeroff, T.; Banzer, W. Health Benefits of Light-Intensity Physical Activity: A Systematic Review of Accelerometer Data of the National Health and Nutrition Examination Survey (NHANES). Sports Med. 2017, 47, 1769–1793. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Cardiovascular Disease (n = 499,336) | ||||
|---|---|---|---|---|---|
| All | a Low Greenness | High Greenness | b High Long-Term PM2.5 | Low Long-Term PM2.5 | |
| (n = 499,336) | (n = 249,438) | (n = 249,898) | (n = 249,337) | (n = 249,999) | |
| Age [mean ± SD (years)] | 65.13 ± 14.84 | 65.48 ± 14.84 | 64.79 ± 14.84 | 65.03 ± 14.74 | 65.24 ± 14.95 |
| Age group [n (%)] | |||||
| <45 years | 41,027 (8.2) | 19,573 (7.9) | 21,454 (8.6) | 20,460 (8.2) | 20,567 (8.2) |
| 45–54 years | 65,386 (13.1) | 31,981 (12.8) | 33,405 (13.4) | 32,181 (12.9) | 33,205 (13.3) |
| 55–64 years | 124,713 (24.9) | 63,972 (25.7) | 60,741 (24.3) | 61,983 (24.9) | 62,730 (25.1) |
| 65–74 years | 128,791 (25.8) | 61,506 (24.7) | 67,285 (26.9) | 67,633 (27.1) | 61,158 (24.5) |
| >74 years | 139,419 (27.9) | 72,406 (29.0) | 67,013 (26.8) | 67,080 (26.9) | 72,339 (28.9) |
| Sex [n (%)] | |||||
| Male | 273,082 (54.6) | 136,711 (54.8) | 136,371 (54.6) | 135,572 (54.4) | 137,510 (55.1) |
| Female | 226,254 (46.4) | 112,727 (46.2) | 113,527 (45.4) | 113,765 (45.6) | 112,489 (44.9) |
| c Sub-diagnoses [n (%)] | |||||
| Hypertension | 76,965 (15.4) | 39,688 (15.9) | 37,277 (14.9) | 36,234 (14.5) | 40,731 (16.3) |
| CHD | 144,536 (28.9) | 75,069 (30.1) | 69,467 (27.8) | 69,780 (28.0) | 74,756 (29.9) |
| Stroke | 164,390 (32.9) | 79,737 (32.0) | 84,653 (33.9) | 86,573 (34.7) | 77,817 (31.1) |
| Lag | Total CVD | Hypertension | CHD | Stroke |
|---|---|---|---|---|
| lag0–3 | 0.64(0.42,0.86) | 0.29(−0.26,0.84) | 0.9(0.48,1.31) | 0.58(0.18,0.97) |
| lag0–2 | 0.78 (0.58, 0.99) | 0.53 (0.03, 1.04) | 1.01 (0.62, 1.39) | 0.69 (0.32, 1.06) |
| lag0–1 | 0.57 (0.38, 0.75) | 0.26 (−0.19, 0.72) | 0.75 (0.41, 1.10) | 0.58 (0.25, 0.91) |
| lag3 | −0.07(−0.23,0.08) | −0.17(−0.56,0.23) | 0.05(−0.25,0.34) | −0.07(−0.35,0.22) |
| lag2 | 0.48 (0.32, 0.64) | 0.57 (0.17, 0.98) | 0.62 (0.32, 0.92) | 0.23 (−0.06, 0.53) |
| lag1 | 0.45 (0.29, 0.61) | 0.34 (−0.06, 0.75) | 0.64 (0.34, 0.95) | 0.32 (0.03, 0.61) |
| lag0 | 0.34 (0.18, 0.50) | 0.10 (−0.29, 0.49) | 0.42 (0.13, 0.72) | 0.45 (0.16, 0.73) |
| Residential Exposure Factors | a Level of Residential Exposure | Total CVD | Hypertension | CHD | Stroke |
|---|---|---|---|---|---|
| Greenness | Low | 0.99 (0.71, 1.28) | 0.87 (0.16, 1.59) | 1.36 (0.84, 1.89) | 0.84 (0.31, 1.37) |
| High | 0.45 (0.13, 0.77) | 0.14 (−0.58, 0.87) | 0.63 (0.09, 1.17) | 0.55 (0.04, 1.06) | |
| Long-term PM2.5 | Low | 0.73 (0.41, 1.06) | 0.69 (−0.14, 1.53) | 0.67 (0.05, 1.29) | 0.56 (0.01, 1.12) |
| High | 0.70 (0.43, 0.97) | 0.32 (−0.33, 0.97) | 1.11 (0.61, 1.61) | 0.66 (0.16, 1.16) |
| Admissions | a Long-Term PM2.5 Level | b Residential Greenness | |||
|---|---|---|---|---|---|
| Quartile 1 (Least Green) | Quartile 2 | Quartile 3 | Quartile 4 (Greenest) | ||
| Total CVD | Low | 1.61 (0.95, 2.27) | 0.87 (0.23, 1.52) | 0.35 (−0.30, 1.00) | 0.39 (−0.30, 1.09) |
| High | 0.58 (0.04, 1.11) | 1.19 (0.66, 1.73) | 0.66 (0.13, 1.20) | 0.01 (−0.56, 0.59) | |
| Hypertension | Low | 1.98 (0.39, 3.60) | −0.03 (−1.62, 1.58) | 0.47 (−1.09, 2.05) | 0.26 (−1.56, 2.12) |
| High | 0.27 (−1.01, 1.56) | 1.10 (−0.19, 2.40) | 0.44 (−0.84, 1.74) | −0.70 (−2.17, 0.80) | |
| CHD | Low | 1.23 (0.03, 2.44) | 0.79 (−0.40, 2.00) | 0.66 (−0.52, 1.85) | 0.74 (−0.62, 2.12) |
| High | 1.17 (0.20, 2.15) | 1.84 (0.87, 2.82) | 1.04 (0.08, 2.02) | −0.44 (−1.55, 0.68) | |
| Stroke | Low | 1.32 (0.15, 2.50) | 0.94 (0.10, 1.78) | 0.77 (−0.39, 1.94) | 0.51 (−0.65, 1.69) |
| High | 0.38 (−0.58, 1.34) | 0.69 (−0.27, 1.66) | −0.79 (−1.95, 0.38) | 0.80 (−0.17, 1.77) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, H.; Liao, J.; Wang, J.; Yang, C.; Jiao, K.; Wang, X.; Huang, Z.; Ma, X.; Liu, X.; Liao, J.; et al. PM2.5-Associated Hospitalization Risk of Cardiovascular Diseases in Wuhan: Cases Alleviated by Residential Greenness. Int. J. Environ. Res. Public Health 2023, 20, 746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010746
Yang H, Liao J, Wang J, Yang C, Jiao K, Wang X, Huang Z, Ma X, Liu X, Liao J, et al. PM2.5-Associated Hospitalization Risk of Cardiovascular Diseases in Wuhan: Cases Alleviated by Residential Greenness. International Journal of Environmental Research and Public Health. 2023; 20(1):746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010746
Chicago/Turabian StyleYang, Haomin, Jianpeng Liao, Jing Wang, Can Yang, Kuizhuang Jiao, Xiaodie Wang, Zenghui Huang, Xuxi Ma, Xingyuan Liu, Jingling Liao, and et al. 2023. "PM2.5-Associated Hospitalization Risk of Cardiovascular Diseases in Wuhan: Cases Alleviated by Residential Greenness" International Journal of Environmental Research and Public Health 20, no. 1: 746. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20010746