
Work Ability after Breast Cancer: Study of Healthcare Personnel Operating in a Hospital of South Italy

 , , ,
, , ,  ,
,  and
and 
Abstract
:1. Introduction
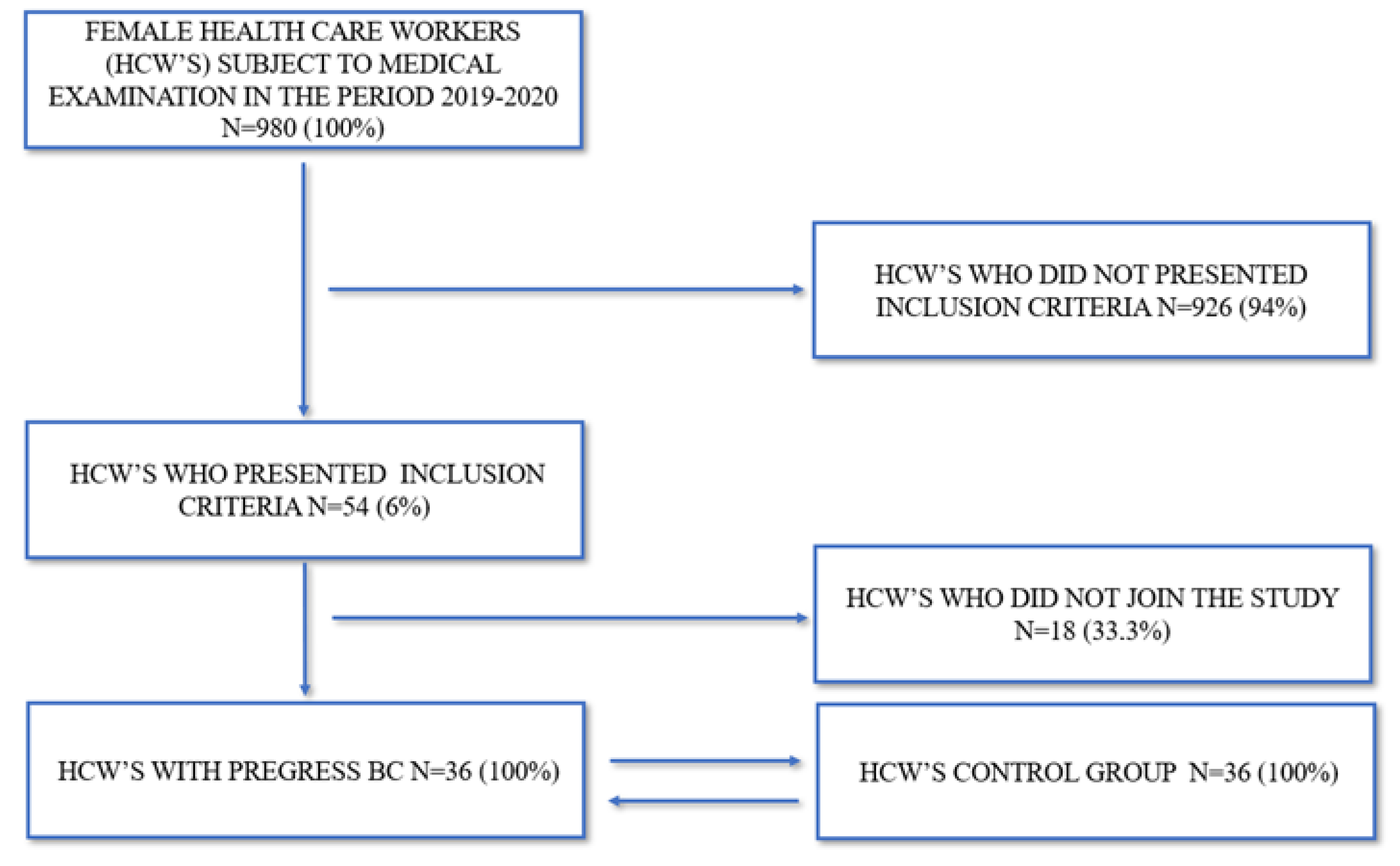
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Clegg, L.X.; Reichman, M.E.; Miller, B.A.; Hankey, B.F.; Singh, G.K.; Lin, Y.D. Impact of socioeconomic status on cancer incidence and stage at diagnosis: Selected findings from the surveillance, epidemiology, and end results: National longitudinal mortality study. Cancer Causes Control 2009, 20, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Shamshirian, A.; Heydari, K.; Shams, Z.; Aref, A.R.; Shamshirian, D.; Tamtaji, O.R.; Asemi, Z.; Shojaie, L.; Mirzaei, H.; Mohammadi, N.; et al. Breast cancer risk factors in Iran: A systematic review & meta-analysis. Horm. Mol. Biol. Clin. Investig. 2020, 41, 4. [Google Scholar]
- Harris, J.; Lippman, M.; Morrow, M.; Osborne, C. Diseases of the Breast, 5th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014. [Google Scholar]
- Fitzmaurice, C.; Dicker, D.; Pain, A.; Hamavid, H.; Moradi-Lakeh, M.; MacIntyre, M.F. The global burden of cancer. JAMA Oncol. 2015, 1, 505–527. [Google Scholar] [PubMed]
- Fondazione AIOM (Italian Association of Medical Oncology)–AIRTUM. 2019. Available online: https://www.fondazioneaiom.it/presentato-al-ministero-della-salute-il-volume-sui-numeri-del-cancro-frutto-della-collaborazione-tra-aiom-airtum-fondazione-aiom-passi-passi-dargento-e-siapec-iap/ (accessed on 15 May 2020).
- Hortobagyi, G.N.; de la Garza Salazar, J.; Pritchard, K.; Amadori, D.; Haidinger, R.; Hudis, C.A. The global breast cancer burden: Variations in epidemiology and survival. Clin. Breast Cancer 2005, 6, 391–401. [Google Scholar] [CrossRef]
- Gregorowitsch, M.L.; van den Bongard, H.J.G.D.; Couwenberg, A.M.; Young-Afat, D.A.; Haaring, C.; Van Dalen, T.; Schoenmaeckers, E.J.P.; Agterof, M.J.; Baas, I.O.; Sier, M.F.; et al. Self-reported work ability in breast cancer survivors; a prospective cohort study in The Netherlands. Breast 2019, 48, 45–53. [Google Scholar] [CrossRef]
- ISTAT-The Italian Institute of Statistics. Available online: www.demo.istat.it (accessed on 20 June 2020).
- Lee, H.E.; Lee, J.; Jang, T.W.; Kim, I.A.; Park, J.; Song, J. The relationship between night work and breast cancer. Ann. Occup. Environ. Med. 2018, 30, 11. [Google Scholar] [CrossRef]
- Bachelet, D.; Verner, M.A.; Neri, M.; Duverger, É.C.; Charlier, C.; Arveux, P.; Haddad, S.; Guénel, P. Breast Cancer and Exposure to Organochlorines in the CECILE Study: Associations with Plasma Levels Measured at the Time of Diagnosis and Estimated during Adolescence. Int. J. Environ. Res. Public Health 2019, 16, 271. [Google Scholar] [CrossRef]
- Cordina-Duverger, E.; Menegaux, F.; Popa, A.; Rabstein, S.; Harth, V.; Pesch, B.; Brüning, T.; Fritschi, L.; Glass, D.C.; Heyworth, J.S.; et al. Night shift work and breast cancer: A pooled analysis of population-based case-control studies with complete work history. Eur. J. Epidemiol. 2018, 33, 369–379. [Google Scholar] [CrossRef]
- IARC Monografie Volume 60. Some Industrial Chemicals; IARC: Lyon, France, 1994.
- IARC Monografie Volume 75. Ionizing Radiation, Part 1: X- and Gamma (γ)-Radiation, and Neutrons; IARC: Lyon, France, 2000.
- IARC Monografie Volume 97. 1,3-Butadiene, Ethylene Oxide and Vinyl Halides (Vinyl Fluoride, Vinyl Chloride and Vinyl Bromide); IARC: Lyon, France, 2008.
- IARC Monografie Volume 100F. Chemical Agents and Related Occupations; IARC: Lyon, France, 2012.
- IARC Monographs Volume 124. Carcinogenicity of Night Shift Work; IARC: Lyon, France, 2019.
- Rapisarda, V.; Ledda, C., 3rd. Etnean Occupational Medicine Workshop-Breast Cancer and Work. Cancers 2020, 12, 1925. [Google Scholar] [CrossRef]
- Leonardi, G.C.; Rapisarda, V.; Marconi, A.; Scalisi, A.; Catalano, F.; Proietti, L.; Travali, S.; Libra, M.; Fenga, C. Correlation of the risk of breast cancer and disruption of the circadian rhythm (Review). Oncol. Rep. 2012, 28, 418–428. [Google Scholar] [CrossRef]
- Bracci, M.; Copertaro, A.; Ciarapica, V.; Barbaresi, M.; Esposito, S.; Albanesi, A.; Valentino, M.; Ledda, C.; Rapisarda, V.; Santarelli, L. NOCTURNIN Gene Diurnal Variation in Healthy Volunteers and Expression Levels in Shift Workers. Biomed. Res. Int. 2019, 2019, 7582734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bracci, M.; Ciarapica, V.; Zabaleta, M.E.; Tartaglione, M.F.; Pirozzi, S.; Giuliani, L.; Piva, F.; Valentino, M.; Ledda, C.; Rapisarda, V.; et al. BRCA1 and BRCA2 Gene Expression: Diurnal Variability and Influence of Shift Work. Cancers 2019, 11, 1146. [Google Scholar] [CrossRef]
- Manzella, N.; Bracci, M.; Strafella, E.; Staffolani, S.; Ciarapica, V.; Copertaro, A.; Rapisarda, V.; Ledda, C.; Amati, M.; Valentino, M.; et al. Circadian Modulation of 8-Oxoguanine DNA Damage Repair. Sci. Rep. 2015, 5, 13752. [Google Scholar] [CrossRef]
- Manzella, N.; Bracci, M.; Ciarapica, V.; Staffolani, S.; Strafella, E.; Rapisarda, V.; Valentino, M.; Amati, M.; Copertaro, A.; Santarelli, L. Circadian gene expression and extremely low-frequency magnetic fields: An in vitro study. Bioelectromagnetics 2015, 36, 294–301. [Google Scholar] [CrossRef] [PubMed]
- Bracci, M.; Manzella, N.; Copertaro, A.; Staffolani, S.; Strafella, E.; Barbaresi, M.; Copertaro, B.; Rapisarda, V.; Valentino, M.; Santarelli, L. Rotating-shift nurses after a day off: Peripheral clock gene expression, urinary melatonin, and serum 17-β-estradiol levels. Scand. J. Work Environ. Health 2014, 40, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Bracci, M.; Copertaro, A.; Manzella, N.; Staffolani, S.; Strafella, E.; Nocchi, L.; Barbaresi, M.; Copertaro, B.; Rapisarda, V.; Valentino, M.; et al. Influence of night-shift and napping at work on urinary melatonin, 17-β-estradiol and clock gene expression in pre-menopausal nurses. J. Biol. Regul. Homeost. Agents 2013, 27, 267–274. [Google Scholar]
- Moo, T.A.; Sanford, R.; Dang, C.; Morrow, M. Overview of Breast Cancer Therapy. PET Clin. 2018, 13, 339–354. [Google Scholar] [CrossRef]
- Campagna, M.; Loscerbo, R.; Pilia, I.; Meloni, F. Return to Work of Breast Cancer Survivors: Perspectives and Challenges for Occupational Physicians. Cancers 2020, 12, 355. [Google Scholar] [CrossRef]
- Ramaci, T.; Rapisarda, V.; Bellini, D.; Mucci, N.; De Giorgio, A.; Barattucci, M. Mindfulness as a Protective Factor for Dissatisfaction in HCWs: The Moderating Role of Mindful Attention between Climate Stress and Job Satisfaction. Int. J. Environ. Res. Public Health 2020, 17, 3818. [Google Scholar] [CrossRef]
- Pellerone, M.; Rapisarda, V.; Trischitta, M.C.A.; Vitale, E.; Ramaci, T. Burnout and Self-Perceived Instructional Competence: An Exploratory Study of a Group of Italian Female Elementary School Teachers. Int. J. Environ. Res. Public Health 2020, 17, 1356. [Google Scholar] [CrossRef]
- Ramaci, T.; Barattucci, M.; Vella, F.; Senia, P.; Cannizzaro, E.; Scorciapino, A.; Ledda, C.; De Giorgio, A.; Rapisarda, V. Straining at Work and Its Relationship with Personality Profiles and Individual Consequences in Healthcare Workers (HCWs). Int. J. Environ. Res. Public Health 2020, 17, 610. [Google Scholar] [CrossRef] [PubMed]
- Barattucci, M.; Padovan, A.M.; Vitale, E.; Rapisarda, V.; Ramaci, T.; De Giorgio, A. Mindfulness-Based IARA Model® Proves Effective to Reduce Stress and Anxiety in Health Care Professionals. A Six-Month Follow-Up Study. Int. J. Environ. Res. Public Health 2019, 16, 4421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kullberg, C.; Selander, J.; Albin, M.; Bourgquist, S.; Manjer, J.; Gustavsson, P. Female white-collar workers remain at higher risk of breast cancer after adjustments for individual risk factors related to reproduction and lifestyle. Occup. Environ. Med. 2017, 74, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Suur-Uski, J.; Pekkala, J.; Blomgren, J.; Pietiläinen, O.; Rahkonen, O.; Mänty, M. Occupational Class Differences in Long-Term Sickness Absence Due to Breast Cancer during 2005–2013: A Population-Based Study among Finnish Women. Int. J. Environ. Res. Public Health 2019, 16, 3477. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, P.; Maglia, M.; Floresta, D.; Ledda, C.; Vitale, E.; Polosa, R.; Rapisarda, V. A randomized controlled trial to compare group motivational interviewing to very brief advice for the effectiveness of a workplace smoking cessation counseling intervention. J. Addict. Dis. 2020, 38, 465–474. [Google Scholar] [CrossRef]
- Rapisarda, V.; Ledda, C.; Maltezou, H.C. Vaccination in healthcare workers: Risk assessment, planning, strategy of intervention and legal implications. Future Microbiol. 2019, 14, 1–3. [Google Scholar] [CrossRef]
- Ledda, C.; Cinà, D.; Matera, S.; Mucci, N.; Bracci, M.; Rapisarda, V. High HOMA-IR Index in Healthcare Shift Workers. Medicina 2019, 55, 186. [Google Scholar] [CrossRef]
- Ilmarinen, J. The Work Ability Index (WAI). Occup. Med. 2007, 57, 160. [Google Scholar] [CrossRef]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Work, T.A. Ability Index. Finnish Institute of Occupational Health, Helsinki. Occup. Health Care 1998, 19, 17–19. [Google Scholar]
- Gamperiene, M.; Nygård, J.F.; Sandanger, I.; Lau, B.; Bruusgaard, D. Self-reported work ability of Norwegian women in relation to physical and mental health, and to the work environment. J. Occup. Med. Toxicol. 2008, 3, 8. [Google Scholar] [CrossRef]
- Bresić, J.; Knezević, B.; Milosević, M.; Tomljanović, T.; Golubić, R.; Mustajbegović, J. Stress and work ability in oil industry workers. Arh. Hig. Rada Toksikol. 2007, 58, 399–405. [Google Scholar] [CrossRef] [PubMed]
- de Zwart, B.C.; Frings-Dresen, M.H.; van Duivenbooden, J.C. Test-retest reliability of the Work Ability Index questionnaire. Occup. Med. 2002, 52, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Kiss, P.; Walgraeve, M.; Vanhoorne, M. Assessment of work ability in aging fire fighters by means of the Work Ability Index: Preliminary results. Arch. Public Health 2002, 60, 233–243. [Google Scholar]
- Hortobagyi, G.N.; Edge, S.B.; Giuliano, A. New and Important Changes in the TNM Staging System for Breast Cancer. Am. Soc. Clin. Oncol. Educ. Book 2018, 38, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Broggi, G.; Filetti, V.; Ieni, A.; Rapisarda, V.; Ledda, C.; Vitale, E.; Varricchio, S.; Russo, D.; Lombardo, C.; Tuccari, G.; et al. MacroH2A1 Immunoexpression in Breast Cancer. Front. Oncol. 2020, 10, 1519. [Google Scholar] [CrossRef]
- Gencay Can, A.; Can, S.S.; Ekşioğlu, E.; Çakcı, F.A. Is kinesiophobia associated with lymphedema, upper extremity function, and psychological morbidity in breast cancer survivors? Turk. J. Phys. Med. Rehabil. 2018, 65, 139–146. [Google Scholar] [CrossRef]
- Bracci, M.; Ciarapica, V.; Copertaro, A.; Barbaresi, M.; Manzella, N.; Tomasetti, M.; Gaetani, S.; Monaco, F.; Amati, M.; Valentino, M.; et al. Peripheral Skin Temperature and Circadian Biological Clock in Shift Nurses after a Day off. Int. J. Mol. Sci. 2016, 17, 623. [Google Scholar] [CrossRef]
- O’Shaughnessy, J. Extending survival with chemotherapy in metastatic breast cancer. Oncologist 2005, 10, 20–29. [Google Scholar] [CrossRef]
- Erol, T.; İmamoğlu, N.E.; Aydin, B.; Taşkiran, Z.E.; Esendağli, G.; Kösemehmetoğlu, K.; Baykal, A. Primary tumor resection for initially staged IV breast cancer: An emphasis on programmed death-ligand 1 expression, promoter methylation status, and survival. Medicine 2019, 98, e16773. [Google Scholar] [CrossRef]
- Nesvold, I.L.; Reinertsen, K.V.; Fosså, S.D.; Dahl, A.A. The relation between arm/shoulder problems and quality of life in breast cancer survivors: A cross-sectional and longitudinal study. J Cancer Surviv 2011, 5, 62–72. [Google Scholar] [CrossRef]
- Goss, C.; Leverment, I.M.; de Bono, A.M. Breast cancer and work outcomes in health care workers. Occup. Med. 2014, 64, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Stubblefield, M.D.; Keole, N. Upper body pain and functional disorders in patients with breast cancer. PM R 2014, 6, 170–183. [Google Scholar] [CrossRef] [PubMed]
- de Boer, A.G.E.M.; Verbeek, J.H.A.M.; Spelten, E.R.; Uitterhoeve, A.L.J.; Ansink, A.C.; de Reijke, T.M.; Kammeijer, M.; Sprangers, M.A.G.; van Dijk, F.J.H. Work ability and return-to-work in cancer patients. Br. J. Cancer 2008, 98, 1342–1347. [Google Scholar] [CrossRef]
- Malaguarnera, R.; Ledda, C.; Filippello, A.; Frasca, F.; Francavilla, V.C.; Ramaci, T.; Parisi, M.C.; Rapisarda, V.; Piro, S. Thyroid Cancer and Circadian Clock Disruption. Cancers 2020, 12, E3109. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, V.; Marconi, A.; Candido, S.; Nicolosi, D.; Salmeri, M.; Gangemi, P.; Proietti, L.; Spandidos, D.A.; Bracci, M.; Fenga, C.; et al. A tailored health surveillance program unveils a case of MALT lymphoma in an HCV-positive health-care worker. Oncol. Lett. 2013, 5, 651–654. [Google Scholar] [CrossRef]
- Barchitta, M.; Maugeri, A.; Magnano San Lio, R.; Quattrocchi, A.; Degrassi, F.; Catalano, F.; Basile, G.; Agodi, A. The Effects of Diet and Dietary Interventions on the Quality of Life among Breast Cancer Survivors: A Cross-Sectional Analysis and a Systematic Review of Experimental Studies. Cancers 2020, 12, 322. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Cases with Prior BrC 36 (100%) | Control Group 36 (100%) | p-Value | |
|---|---|---|---|
| Average age (yrs) | 52.9 ± 7.29 | 53.7 ± 7 | n.s. |
| Age (at the time of diagnosis) | 45.2 ± 7.2 | - | n.c. |
| Menarche (age) | 11.8 ± 1.09 | 11.7 ± 1.2 | n.s. |
| Menopause (age) | 44.7 ± 4.9 | 44.2 ±4.7 | n.s. |
| Service duration (yrs) | 26.1 ± 7.5 | 25.9 ± 6.7 | n.s. |
| Job time (yrs–at diagnosis) | 17.7 ± 8.8 | 15.7 ± 7.1 | n.s. |
| Shift workers | 28 (78%) | 20 (55.6%) | n.s. |
| BMI mean (kg/m2) | 25.3 ± 4.8 | 25.1 ± 2.7 | n.s. |
| BMI < 18.5 | 5 (14%) | 7 (19% | n.s. |
| BMI 18.5–24.9 | 12 (33%) | 6 (17%) | n.s. |
| BMI 25–29.9 | 15 (42%) | 17 (47%) | n.s. |
| BMI > 30 | 4 (11%) | 6 (17%) | n.s |
| Smokers | 7 (19.4%) | 5 (13.8%) | n.s. |
| Cigarette packages/year | 14.5 ± 2.5 | 15.1 ± 2.1 | n.s. |
| Daily alcohol intake (1 glass per day) | 2 (5.5%) | 3 (8.3%) | n.s. |
| Medical Doctors/biologists | 15 (41.6%) | 14 (38.8%) | n.s. |
| Nurses/technicians | 21 (58.4%) | 22 (61.1%) | n.s. |
| Surgical area | 10 (28%) | 9 (25%) | n.s. |
| Medical area | 14 (39%) | 16 (44.4%) | n.s. |
| Service area | 12 (33.3%) | 11 (30.6%) | n.s. |
| Nulliparous | 11(30.5%) | 9 (25%) | n.s. |
| BrC family history | 11 (30.5%) | 2 (5.5%) | p < 0.05 |
| Hormonal contraception | 13 (36.1%) | 0 | p < 0.05 |
| Breastfeeding | 22/25 (61.1%) | 18/27 (50%) | n.s. |
| Luminal-A | Luminal-B | Her 2+ | |
|---|---|---|---|
| N° cases | 24 (67%) | 4 (11%) | 8 (22%) |
| MCT | 5 (21%) | 0 | 5 (62.5%) |
| QDCT | 19 (79%) | 4 (100%) | 3 (37.5%) |
| LMCT | 12 (50%) | 4 (100%) | 6 (75%) |
| CTP | / | / | / |
| RDT | 4 (16%) | / | / |
| CTP and RDT | 20 (84%) | 4 (100%) | 8 (100%) |
| STAGE 0 | Tis | N0 | M0 | 4 (11%) |
| STAGE I | T1 | N0 | M0 | 11 (30.5%) |
| STAGE II A | T0 | N1 | M0 | / |
| T1 | N1 | M0 | 8 (22%) | |
| T2 | N0 | M0 | 2 (5%) | |
| STAGE IIB | T2 | N1 | M0 | 4 (11%) |
| T3 | N0 | M0 | 3 (8.3%) | |
| STAGE III A | T0 | N2 | M0 | / |
| T1 | N2 | M0 | 2 (5%) | |
| T2 | N2 | M0 | 1 (2.7%) | |
| T3 | N1, N2 | M0 | 1 (2.7%) | |
| STAGE III B | T4 | N1, N2, N3 | M0 | / |
| STAGE III C | Any T | N3 | M0 | / |
| STAGE IV | Any T | Any N | M1 | 1 (2.7%) |
| WAI Score | 7–27 (Low) | 28–36 (Moderate) | 37–43 (Good) | 44–49 (Excellent) |
|---|---|---|---|---|
| QDCT + CTP/RDT | - | 2 (6%) | 3 (8%) | 4 (11%) |
| QDCT + RDT | - | 2 (6%) | 2 (6%) | |
| QDCT + CTP | - | - | - | - |
| QDCT + CTP/RDT + LMCT | 4 (11%) | 5 (14%) | 4 (11%) | - |
| QDCT + RDT + LMCT | - | - | - | - |
| MCT + CTP | - | - | - | - |
| MCT + CTP/RDT + LMCT | 3 (8%) | 6(16%) | - | - |
| MCT + LMTC | - | - | - | - |
| MCT + CTP/RDT | 1 (3%) | - | - | - |
| MCT + RDT | - | - | - | - |
| MCT + LMCT + RDT | - | - | - | - |
| TOTAL STUDY GROUP | 8 (22%) * | 13 (33%) * | 9 (23%) * | 8 (22%) * |
| CONTROL GROUP | 2 (6%) * | 6 (16%) * | 20 (51%) * | 9 (23%) * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vella, F.; Filetti, V.; Cirrincione, L.; Rapisarda, V.; Matera, S.; Skerjanc, A.; Cannizzaro, E.; Vitale, E. Work Ability after Breast Cancer: Study of Healthcare Personnel Operating in a Hospital of South Italy. Int. J. Environ. Res. Public Health 2022, 19, 10835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710835
Vella F, Filetti V, Cirrincione L, Rapisarda V, Matera S, Skerjanc A, Cannizzaro E, Vitale E. Work Ability after Breast Cancer: Study of Healthcare Personnel Operating in a Hospital of South Italy. International Journal of Environmental Research and Public Health. 2022; 19(17):10835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710835
Chicago/Turabian StyleVella, Francesca, Veronica Filetti, Luigi Cirrincione, Venerando Rapisarda, Serena Matera, Alenka Skerjanc, Emanuele Cannizzaro, and Ermanno Vitale. 2022. "Work Ability after Breast Cancer: Study of Healthcare Personnel Operating in a Hospital of South Italy" International Journal of Environmental Research and Public Health 19, no. 17: 10835. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191710835