
Feasibility and Acceptability of Personalized Breast Cancer Screening (DECIDO Study): A Single-Arm Proof-of-Concept Trial

 , , , , ,
on behalf of the DECIDO Group
, , , , ,
on behalf of the DECIDO Group
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Breast Cancer Risk Estimation, Risk Communication, and Screening Recommendations
2.5. Outcomes
2.6. Statistical Considerations
3. Results
3.1. Participants’ Characteristics
3.2. Risk of Breast Cancer and Screening Recommendations
3.3. Primary Outcomes
3.4. Secondary Outcomes
4. Discussion
4.1. Main Results
4.2. Comparison with Other Studies
4.2.1. Attitude towards Personalized Breast Cancer Screening and Intention to Participate
4.2.2. Breast Cancer Risk and Screening Recommendations
4.2.3. Risk Communication
4.3. Strengths and Limitations
5. Conclusions
6. Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Collaborators
Conflicts of Interest
References
- Chowdhury, S.; Dent, T.; Pashayan, N.; Hall, A.; Lyratzopoulos, G.; Hallowell, N.; Hall, P.; Pharoah, P.; Burton, H. Incorporating genomics into breast and prostate cancer screening: Assessing the implications. Genet. Med. 2013, 15, 423–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vilaprinyo, E.; Forné, C.; Carles, M.; Sala, M.; Pla, R.; Castells, X.; Domingo, L.; Rue, M.; The Interval Cancer (INCA) Study Group. Cost-effectiveness and harm-benefit analyses of risk-based screening strategies for breast cancer. PLoS ONE 2014, 9, e86858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Román, M.; Sala, M.; Domingo, L.; Posso, M.; Louro, J.; Castells, X. Personalized breast cancer screening strategies: A systematic review and quality assessment. PloS ONE 2019, 14, e0226352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mühlberger, N.; Sroczynski, G.; Gogollari, A.; Jahn, B.; Pashayan, N.; Steyerberg, E.; Widschwendter, M.; Siebert, U. Cost Effectiveness of Breast Cancer Screening and Prevention: A Systematic Review with a Focus on Risk-Adapted Strategies [Internet]; Springer: Berlin/Heidelberg, Germany, 2021; pp. 1311–1344. [Google Scholar] [CrossRef]
- Khan, S.A.; Hernandez-Villafuerte, K.V.; Muchadeyi, M.T.; Schlander, M. Cost-effectiveness of risk-based breast cancer screening: A systematic review. Int. J. Cancer 2021, 149, 790–810. [Google Scholar] [CrossRef]
- Esserman, L.J. The WISDOM Study: Breaking the deadlock in the breast cancer screening debate. Npj Breast Cancer 2017, 3, 34. [Google Scholar] [CrossRef] [Green Version]
- Delaloge, S.; Gorgio-Rossi, P.; Balleyguier, C.; Guindy, M.; Burrion, J.; Gilbert, F.; Román, M. My Personalized Breast Screening (MyPeBS)-ClinicalTrials.gov 2018; Identifier NCT03672331. Available online: https://clinicaltrials.gov/show/NCT03672331 (accessed on 17 August 2022).
- Brooks, J.D.; Nabi, H.H.; Andrulis, I.L.; Antoniou, A.C.; Chiquette, J.; Després, P.; Devilee, P.; Dorval, M.; Droit, A.; Easton, D.F.; et al. Personalized risk assessment for prevention and early detection of breast cancer: Integration and implementation (PERSPECTIVE I&I). J. Pers. Med 2021, 11, 511. [Google Scholar] [CrossRef]
- Evans, D.G.; Astley, S.; Stavrinos, P.; Harkness, E.; Donnelly, L.S.; Dawe, S.; Jacob, I.; Harvie, M.; Cuzick, J.; Brentnall, A.; et al. Improvement in risk prediction, early detection and prevention of breast cancer in the NHS Breast Screening Programme and Family History Clinic: A cohort study. In Programme Grants for Applied Research; NIHR Journals Library: Southampton, UK, 2016; pp. 1–299. [Google Scholar] [CrossRef] [Green Version]
- Pashayan, N.; Antoniou, A.C.; Ivanus, U.; Esserman, L.J.; Easton, D.F.; French, D.; Sroczynski, G.; Hall, P.; Cuzick, J.; Evans, D.G.; et al. Personalized early detection and prevention of breast cancer: Envision consensus statement. Nat. Rev. Clin. Oncol. 2020, 17, 687–705. [Google Scholar] [CrossRef]
- Antoniou, A.C.; Pharoah, P.P.D.; Smith, P.; Easton, D.F. The BOADICEA model of genetic susceptibility to breast and ovarian cancer. Br. J. Cancer 2004, 91, 1580–1590. [Google Scholar] [CrossRef] [Green Version]
- Tice, J.A.; Miglioretti, D.L.; Li, C.-S.; Vachon, C.M.; Gard, C.C.; Kerlikowske, K. Breast density and benign breast disease: Risk assessment to identify women at high risk of breast cancer. J. Clin. Oncol. 2015, 33, 3137–3143. [Google Scholar] [CrossRef] [Green Version]
- Engmann, N.J.; Golmakani, M.K.; Miglioretti, D.L.; Sprague, B.L.; Kerlikowske, K. Population-attributable risk proportion of clinical risk factors for breast cancer. JAMA Oncology 2017, 3, 1228–1236. [Google Scholar] [CrossRef] [Green Version]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allweis, T.M.; Hermann, N.; Berenstein-Molho, R.; Guindy, M. Personalized Screening for Breast Cancer: Rationale, Present Practices, and Future Directions. Ann. Surg. Oncol. 2021, 28, 4306–4317. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, M.; Czene, K.; Strand, F.; Zackrisson, S.; Lindholm, P.; Lång, K.; Förnvik, D.; Sartor, H.; Mavaddat, N.; Easton, D.; et al. Identification of women at high risk of breast cancer who need supplemental screening. Radiology 2020, 297, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Yala, A.; Mikhael, P.G.; Strand, F.; Lin, G.; Satuluru, S.; Kim, T.; Banerjee, I.; Gichoya, J.; Trivedi, H.; Lehman, C.D.; et al. Multi-Institutional Validation of a Mammography-Based Breast Cancer Risk Model. J. Clin. Oncol. 2022, 40, 1732–1740. [Google Scholar] [CrossRef]
- Tice, J.A.; Cummings, S.R.; Smith-Bindman, R.; Ichikawa, L.; Barlow, W.E.; Kerlikowske, K. Using clinical factors and mammographic breast density to estimate breast cancer risk: Development and validation of a new predictive model. Ann. Intern. Med. 2008, 148, 337–347. [Google Scholar] [CrossRef] [Green Version]
- Yanes, T.; Young, M.A.; Meiser, B.; James, P.A. Clinical applications of polygenic breast cancer risk: A critical review and perspectives of an emerging field. Breast Cancer Res 2020, 22, 21. [Google Scholar] [CrossRef] [Green Version]
- Shieh, Y.; Hu, D.; Huntsman, S.; Gard, C.C.; Jessica, W.T.; Tice, J.A.; Ziv, E.; Kerlikowske, K.; Cummings, S.R. Joint relative risks for estrogen receptor-positive breast cancer from a clinical model, polygenic risk score, and sex hormones. Breast Cancer Res. Treat. 2017, 166, 603–612. [Google Scholar] [CrossRef]
- Hurson, A.N.; Choudhury, P.P.; Gao, C.; Hüsing, A.; Eriksson, M.; Shi, M.; Jones, M.E.; Evans, D.G.R.; Milne, R.L.; Gaudet, M.M.; et al. Prospective evaluation of a breast-cancer risk model integrating classical risk factors and polygenic risk in 15 cohorts from six countries. Int. J. Epidemiol. 2022, 50, 1897–1911. [Google Scholar] [CrossRef]
- Pérez-Lacasta, M.J.; Martínez-Alonso, M.; Garcia, M.; Sala, M.; Perestelo-Pérez, L.; Vidal, C.; Codern-Bové, N.; Feijoo-Cid, M.; Toledo-Chávarri, A.; Cardona, À.; et al. Effect of information about the benefits and harms of mammography on women’s decision making: The InforMa randomised controlled trial. PLoS ONE 2019, 14, e0214057. [Google Scholar] [CrossRef]
- McWilliams, L.; Woof, V.G.; Donnelly, L.S.; Howell, A.; Evans, D.G.; French, D.P. Extending screening intervals for women at low risk of breast cancer: Do they find it acceptable? BMC Cancer 2021, 21, 637. [Google Scholar] [CrossRef]
- Rainey, L.; van der Waal, D.; Donnelly, L.S.; Southworth, J.; French, D.P.; Evans, D.G.; Broeders, M.J.M. Women’s health behaviour change after receiving breast cancer risk estimates with tailored screening and prevention recommendations. BMC Cancer 2022, 22, 69. [Google Scholar] [CrossRef] [PubMed]
- Alarie, S.; Hagan, J.; Dalpé, G.; Faraji, S.; Mbuya-Bienge, C.; Nabi, H.; Pashayan, N.; Brooks, J.D.; Dorval, M.; Chiquette, J.; et al. Risk-stratified approach to breast cancer screening in canada: Women’s knowledge of the legislative context and concerns about discrimination from genetic and other predictive health data. J. Pers. Med. 2021, 11, 726. [Google Scholar] [CrossRef] [PubMed]
- Rainey, L.; van der Waal, D.; Jervaeus, A.; Donnelly, L.S.; Evans, D.G.; Hammarström, M.; Hall, P.; Wengström, Y.; Broeders, M.J.M. European women’s perceptions of the implementation and organisation of risk-based breast cancer screening and prevention: A qualitative study. BMC Cancer 2020, 20, 247. [Google Scholar] [CrossRef]
- Pons-Rodriguez, A.; Forné Izquierdo, C.; Vilaplana-Mayoral, J.; Cruz-Esteve, I.; Sánchez-López, I.; Reñé-Reñé, M.; Cazorla, C.; Hernández-Andreu, M.; Galindo-Ortego, G.; Gabandé, L.; et al. Feasibility and acceptability of personalised breast cancer screening (DECIDO study): Protocol of a single-arm proof-of-concept trial. BMJ Open 2020, 10, e044597. [Google Scholar] [CrossRef] [PubMed]
- Toledo-Chávarri, A.; Rué, M.; Codern-Bové, N.; Carles-Lavila, M.; Perestelo-Pérez, L.; Pérez-Lacasta, M.; Feijoo-Cid, M.; The InforMa Study Group. A qualitative study on a decision aid for breast cancer screening: Views from women and health professionals. Eur. J. Cancer Care 2017, 10, e12660. [Google Scholar] [CrossRef] [PubMed]
- American College of Radiology. Breast Imaging Reporting and Data System (BI-RADS) [Internet], 5th ed.; American College of Radiology: Silver Spring, MD, USA, 2013; Available online: https://www.acr.org/Clinical-Resources/Reporting-and-Data-Systems/Bi-Rads (accessed on 17 August 2022).
- Shieh, Y.; Hu, D.; Ma, L.; Huntsman, S.; Gard, C.C.; Leung, J.W.T.; Tice, J.A.; Vachon, C.M.; Cummings, S.R.; Kerlikowske, K.; et al. Breast cancer risk prediction using a clinical risk model and polygenic risk score. Breast Cancer Res. Treat. 2016, 159, 513–525. [Google Scholar] [CrossRef]
- Mavaddat, N.; Pharoah, P.D.P.; Michailidou, K.; Tyrer, J.; Brook, M.N.; Bolla, M.K.; Wang, Q.; Dennis, J.; Dunning, A.M.; Shah, M.; et al. Prediction of breast cancer risk based on profiling with common genetic variants. J. Natl. Cancer Inst 2015, 107, djv036. [Google Scholar] [CrossRef]
- Gail, M.H.; Brinton, L.A.; Byar, D.P.; Donald, K.; Green, S.B.; Schairer, C.; Mutvihill, J.J. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J. Natl. Cancer Inst. 1989, 81, 1879–1886. [Google Scholar] [CrossRef] [PubMed]
- Hersch, J.; Barratt, A.; Jansen, J.; Irwig, L.; McGeechan, K.; Jacklyn, G.; Thornton, H.; Dhillon, H.; Houssami, N.; Hersch, J.; et al. Use of a decision aid including information on overdetection to support informed choice about breast cancer screening: A randomised controlled trial. Lancet 2015, 385, 1642–1652. [Google Scholar] [CrossRef]
- Sekhon, M.; Cartwright, M.; Francis, J.J. Acceptability of healthcare interventions: An overview of reviews and development of a theoretical framework. BMC Health Serv. Res. 2017, 17, 88. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 17 August 2022).
- RStudio Team. RStudio: Integrated Development Environment for R.; RStudio, PBC.: Boston, MA, USA, 2020; Available online: http://www.rstudio.com/ (accessed on 17 August 2022).
- Heiberger, R.M. Statistical Analysis and Data Display: Heiberger and Holland. 2020. Available online: https://cran.r-project.org/web/packages/HH/HH.pdf (accessed on 17 August 2022).
- Dunlop, K.; Rankin, N.M.; Smit, A.K.; Salgado, Z.; Newson, A.J.; Keogh, L.; Cust, A.E. Acceptability of risk-stratified population screening across cancer types: Qualitative interviews with the Australian public. Health Expect. 2021, 24, 1326–1336. [Google Scholar] [CrossRef]
- Evans, D.G.R.; Donnelly, L.S.; Harkness, E.F.; Astley, S.M.; Stavrinos, P.; Dawe, S.; Watterson, D.; Fox, L.; Sergeant, J.C.; Ingham, S.; et al. Breast cancer risk feedback to women in the UK NHS breast screening population. Br. J. Cancer 2016, 114, 1045–1052. [Google Scholar] [CrossRef] [PubMed]
- Laza-Vásquez, C.; Codern-Bové, N.; Cardona-Cardona, À.; Hernández-Leal, M.J.; Pérez-Lacasta, M.J.; Carles-Lavila, M.; Rué, M. Views of health professionals on risk-based breast cancer screening and its implementation in the Spanish National Health System: A qualitative discussion group study. PLoS ONE 2022, 17, e0263788. [Google Scholar] [CrossRef] [PubMed]
- Woof, V.G.; McWilliams, L.; Donnelly, L.S.; Howell, A.; Evans, D.G.; Maxwell, A.J.; French, D.P. Introducing a low-risk breast screening pathway into the NHS Breast Screening Programme: Views from healthcare professionals who are delivering risk-stratified screening. Women’s Health 2021, 17, 17455065211009746. [Google Scholar] [CrossRef]
- He, X.; Schifferdecker, K.E.; Ozanne, E.M.; Tosteson, A.N.A.; Woloshin, S.; Schwartz, L.M. How do women view risk-based mammography screening? A qualitative study. J. Gen. Intern. Med. 2018, 33, 1905–1912. [Google Scholar] [CrossRef] [Green Version]
- Rainey, L.; Jervaeus, A.; Donnelly, L.S.; Evans, D.; Hammarström, M.; Hall, P.; Wengström, Y.; Broeders, M.J.M.; van der Waal, D. Women’s perceptions of personalized risk-based breast cancer screening and prevention: An international focus group study. Psycho-Oncology 2019, 28, 1056–1062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laza-Vásquez, C.; Hernández-Leal, M.J.; Carles-Lavila, M.; Pérez-Lacasta, M.J.; Cruz-Esteve, I.; Rué, M.; The DECIDO Group. Barriers and facilitators to the implementation of a personalized breast cancer screening program: Views of Spanish health professionals. Int. J. Environ. Res. Public Health 2022, 19, 1406. [Google Scholar] [CrossRef] [PubMed]
- Long, H.; Brooks, J.M.; Harvie, M.; Maxwell, A.; French, D.P. How do women experience a false-positive test result from breast screening? A systematic review and thematic synthesis of qualitative studies. Br. J. Cancer 2019, 121, 351–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, J.; Dodd, R.H.; Hersch, J.; McCaffery, K.J.; Naganathan, V.; Cvejic, E.; Jansen, J. Psychosocial and clinical predictors of continued cancer screening in older adults. Patient Educ. Couns. 2021, 104, 3093–3096. [Google Scholar] [CrossRef]
- Hersch, J.; McGeechan, K.; Barratt, A.; Jansen, J.; Irwig, L.; Jacklyn, G.; Houssami, N.; Dhillon, H.; McCaffery, K. How information about overdetection changes breast cancer screening decisions: A mediation analysis within a randomised controlled trial. BMJ Open 2017, 7, e01624. [Google Scholar] [CrossRef]
- Clift, A.K.; Dodwell, D.; Lord, S.; Petrou, S.; Brady, S.M.; Collins, G.S.; Hippisley-Cox, J. The current status of risk-stratified breast screening. Br. J. Cancer 2022, 126, 533–550. [Google Scholar] [CrossRef] [PubMed]
- Houssami, N.; Kerlikowske, K. AI as a new paradigm for risk-based screening for breast cancer. Nat. Med. 2022, 28, 29–30. [Google Scholar] [CrossRef] [PubMed]
- Vachon, C.M.; Pankratz, V.S.; Scott, C.G.; Haeberle, L.; Ziv, E.; Jensen, M.R.; Brandt, K.R.; Whaley, D.H.; Olson, E.; Heusinger, K.; et al. The contributions of breast density and common genetic variation to breast cancer risk. J. Natl. Cancer Inst. 2015, 107, dju397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saghatchian, M.; Abehsera, M.; Yamgnane, A.; Geyl, C.; Gauthier, E.; Hélin, V.; Bazire, M.; Villoing-Gaudé, L.; Reyes, C.; Gentien, D.; et al. Feasibility of personalized screening and prevention recommendations in the general population through breast cancer risk assessment: Results from a dedicated risk clinic. Breast Cancer Res. Treat. 2022, 192, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.; van Veen, E.M.; Byers, H.; Roberts, E.; Howell, A.; Howell, S.J.; Harkness, E.F.; Brentnall, A.; Cuzick, J.; Newman, W.G. The importance of ethnicity: Are breast cancer polygenic risk scores ready for women who are not of White European origin? Int. J. Cancer 2022, 150, 73–79. [Google Scholar] [CrossRef]
- Baccolini, V.; Isonne, C.; Salerno, C.; Giffi, M.; Migliara, G.; Mazzalai, E.; Turatto, F.; Sinopoli, A.; Rosso, A.; De Vito, C.; et al. The association between adherence to cancer screening programs and health literacy: A systematic review and meta-analysis. Prev. Med. 2022, 155, 106927. [Google Scholar] [CrossRef]
- Hoffmann, T.C.; del Mar, C. Patients’ expectations of the benefits and harms of treatments, screening, and tests. JAMA Intern. Med. 2015, 175, 274. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; del Mar, C. Clinicians’ expectations of the benefits and harms of treatments, screening, and tests. A systematic review. JAMA Intern. Med. 2017, 177, 407–419. [Google Scholar] [CrossRef]
- Seaman, K.; Dzidic, P.L.; Castell, E.; Saunders, C.; Breen, L.J. A systematic review of women’s knowledge of screening mammography. Breast 2018, 42, 81–93. [Google Scholar] [CrossRef]
- Gunn, C.M.; Maschke, A.; Paasche-Orlow, M.K.; Kressin, N.R.; Schonberg, M.A.; Battaglia, T.A. Engaging women with limited health literacy in mammography decision-making: Perspectives of patients and primary care providers. J. Gen. Intern. Med. 2020, 36, 12–15. [Google Scholar] [CrossRef]
- Ahmed, S.; Lévesque, E.; Garland, R.; Knoppers, B.; Dorval, M.; Simard, J.; Loiselle, C.G. Women’s perceptions of perspective: A breast cancer risk stratification e-platform. Hered. Cancer Clin. Pract. 2022, 20, 8. [Google Scholar] [CrossRef] [PubMed]
- Puzhko, S.; Gagnon, J.; Simard, J.; Knoppers, B.M.; Siedlikowski, S.; Bartlett, G. Health professionals’ perspectives on breast cancer risk stratification: Understanding evaluation of risk versus screening for disease. Public Health Rev 2019, 40, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghanouni, A.; Sanderson, S.C.; Pashayan, N.; Renzi, C.; von Wagner, C.; Waller, J. Attitudes towards risk-stratified breast cancer screening among women in England: A cross-sectional survey. J. Med. Screen 2020, 27, 138–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blouin-Bougie, J.; Amara, N.; Simard, J. Toward a population-based breast cancer risk stratification approach? The needs and concerns of healthcare providers. J. Pers. Med. 2021, 11, 540. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographics and Health | Median (Q1; Q3) or n (%) | n |
|---|---|---|
| Age (years) | 48.4 (43.8; 50.1) | 387 |
| Body mass index | 25.4 (22.7; 29.4) | 387 |
| Source: | 387 | |
| Primary care | 211 (54.5%) | |
| Screening program | 176 (45.5%) | |
| Birth place: | 387 | |
| Catalonia | 268 (69.3%) | |
| Other places in Spain | 39 (10.1%) | |
| Other countries | 80 (20.7%) | |
| Education: | 387 | |
| Less than secondary school graduation | 45 (11.6%) | |
| Secondary school diploma or equivalent | 53 (13.7%) | |
| High school | 125 (32.3%) | |
| University degree | 164 (42.4%) | |
| Employment: | 383 | |
| Working | 306 (79.9%) | |
| No paid job | 77 (20.1%) | |
| Had previous mammograms | 218 (56.3%) | 387 |
| Age at first menstruation | 13.0 (11.5; 14.0) | 387 |
| Number of children | 2 (1; 2) | 387 |
| Age at first childbirth | 28.0 (22.0; 32.0) | 297 |
| Breast feeding | 192 (64.6%) | 297 |
| Peri- or postmenopausal | 66 (17.1%) | 387 |
| Oral contraceptives | 387 | |
| Never | 116 (30.0%) | |
| <1 year | 43 (11.1%) | |
| 1–2 years | 55 (14.2%) | |
| 3+ years | 173 (44.7%) | |
| Perceived risk of being diagnosed with breast cancer during lifetime | 383 | |
| Very low | 73 (19.1%) | |
| Low | 160 (41.8%) | |
| Moderate | 132 (34.5%) | |
| High | 18 (4.7%) | |
| Perceived risk of being diagnosed with breast cancer compared to other women | 382 | |
| Much lower | 33 (8.64%) | |
| A little lower | 63 (16.5%) | |
| The same | 239 (62.6%) | |
| A little higher | 46 (12.0%) | |
| Much higher | 1 (0.3%) | |
| Perceived knowledge on benefits of breast screening | 5 (4; 5) | 384 |
| Perceived knowledge on harms of breast screening | 4 (3; 5) | 380 |
| Attitudes towards knowing benefits and harms of breast screening and knowing risk-based screening Not at all important (1) to very much important (5) | ||
| For you, knowing the benefits is important | 5 (5; 5) | 384 |
| For you, knowing the harms is important | 5 (4; 5) | 382 |
| For you, knowing risk-based screening is important | 5 (5; 5) | 383 |
| General intentions of risk-based breast screening | ||
| For you, being involved in risk-based screening would be… Not at all right (1) to very much right (5) | 5 (5; 5) | 384 |
| For you, being involved in risk-based screening would be… Not at all important (1) to very much important (5) | 5 (5; 5) | 377 |
| Variable | Median (Q1; Q3) or n (%) | n | |
|---|---|---|---|
| Previous benign lesion | 387 | ||
| Non-proliferative disease | 23 (5.9%) | ||
| Unspecified benign lesion | 31 (8.0%) | ||
| None | 333 (86.1%) | ||
| Breast density (BI-RADS) | 381 | ||
| A: almost entirely fatty | 56 (14.7%) | ||
| B: scattered areas of fibroglandular density | 117 (30.7%) | ||
| C: heterogeneously dense | 170 (44.6%) | ||
| D: extremely dense | 38 (10.0%) | ||
| Family history of breast cancer | 38 (9.8%) | 387 | |
| Risk estimation | 372 | ||
| Relative risk a | 2.80 (1.85; 3.38) | ||
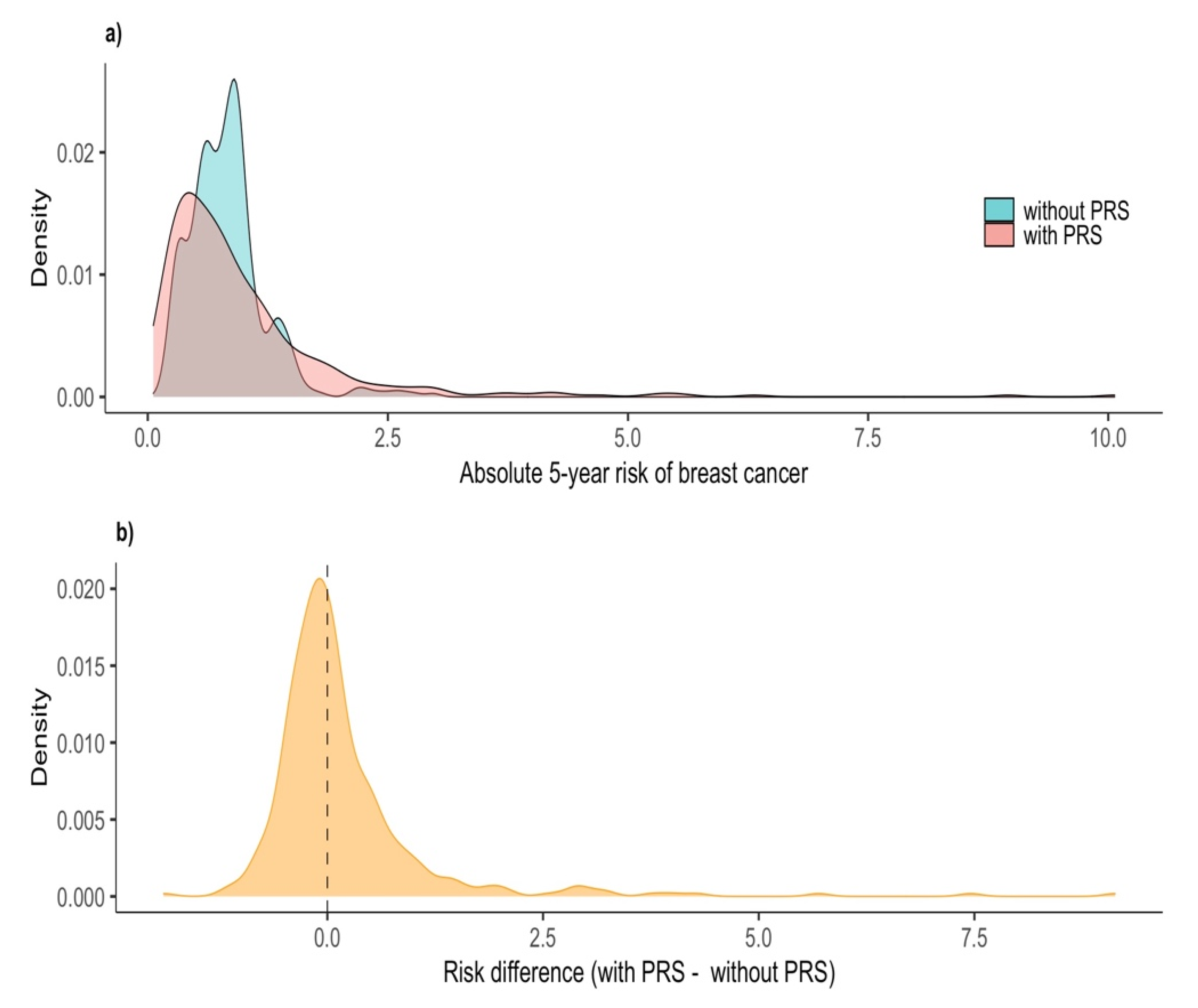
| Absolute risk (%) (without PRS) | 0.80 (0.58; 0.96) | ||
| Polygenic risk score | 0.95 (0.62; 1.51) | ||
| Final risk (%) (with PRS) | 0.72 (0.41; 1.19) | ||
| Risk difference (with PRS minus without PRS, %) | −0.03 (−0.28; 0.34) | ||
| Recommendations b | |||
| Age < 50 years n = 204 | Age 50 years n = 168 | All n = 372 | |
| Referral to the hospital breast unit | 1 (0.5%) | 2 (1.2%) | 3 (0.8%) |
| Annual screening | 51 (25%) | 39 (23.2%) | 90 (24.2%) |
| Biennial screening | 20 (9.8%) | 32 (19.0%) | 52 (14.0%) |
| Triennial screening | 7 (3.4%) | 95 (56.5%) | 102 (27.4%) |
| Watch and wait until the screening program invitation | 125 (61.3%) | 0 (0.0%) | 125 (33.6%) |
| Risk estimation by screening recommendations | Annual screening/referral to breast unit (n = 93) | Biennial screening (n = 52) | Triennial/wait until screening program invitation (n = 227) |
| Relative risk | 3.35 (2.80; 4.03) | 2.80 (1.85; 4.01) | 2.08 (1.85; 2.96) |
| Absolute risk (%) | 0.94 (0.82; 1.28) | 0.92 (0.62; 1.16) | 0.62 (0.48; 0.91) |
| Polygenic risk score | 1.89 (1.44; 2.67) | 1.13 (0.87; 1.56) | 0.70 (0.50; 1.01) |
| Final risk (%) | 1.73 (1.36; 2.48) | 1.03 (0.89; 1.11) | 0.46 (0.31; 0.67) |
| Risk difference (with PRS minus without PRS, %) | 0.80 (0.47; 1.39) | 0.12 (−0.15; 0.34) | −0.17 (−0.39; 0.00) |
| Primary Outcomes | Median (Q1; Q3) or n (%) | n |
|---|---|---|
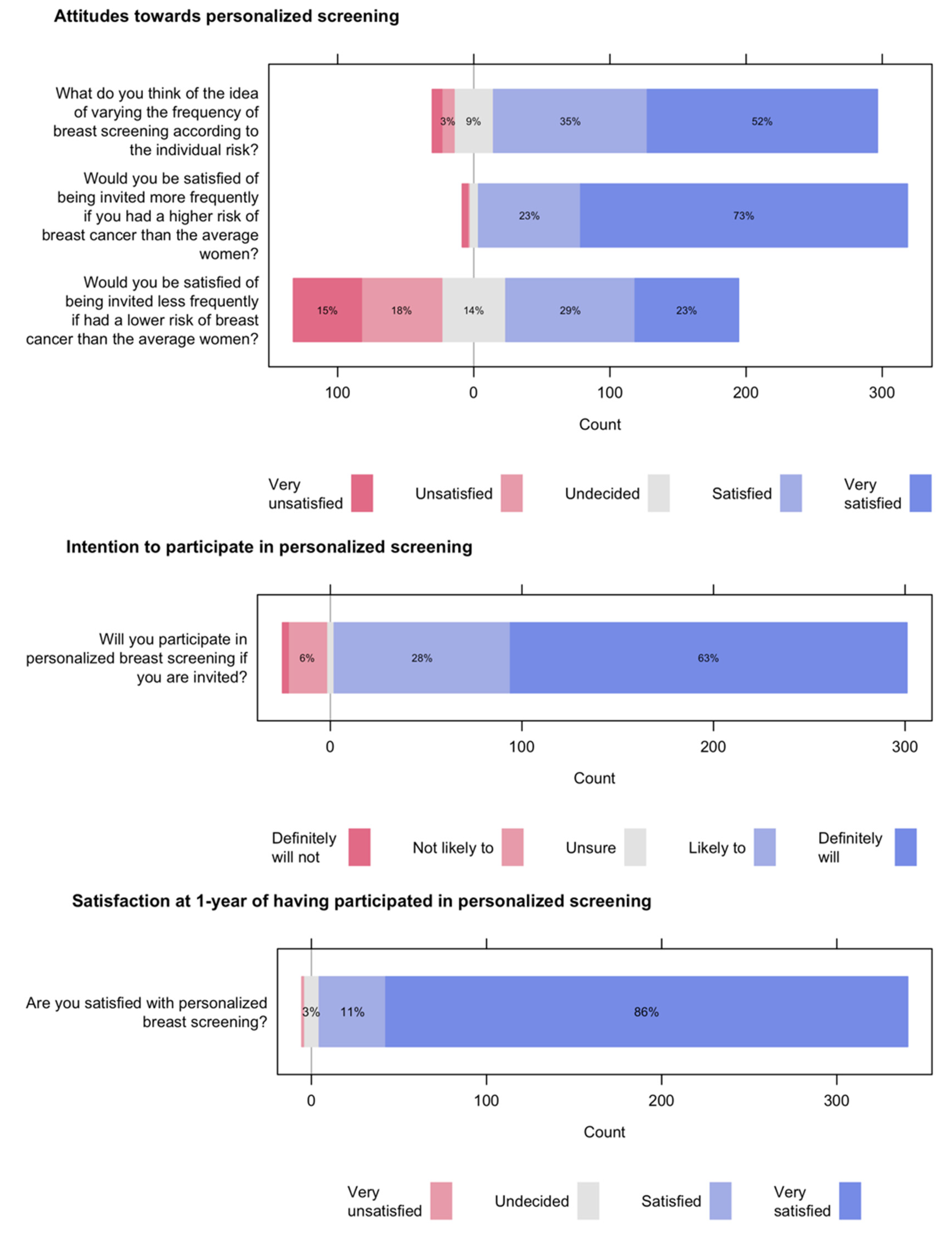
| Attitudes towards personalized breast screening What do you think of the idea of varying the frequency of breast screening according to individual risk? Very bad idea (1) to very good idea (5) | 5 (4; 5) | 327 |
| Would you be personally pleased to be invited more often for screening mammograms if you were found to have a higher risk of breast cancer than the average woman of your age? Not at all satisfied (1) to very satisfied (5) | 5 (4; 5) | 327 |
| Would you be personally pleased to be invited less often for screening mammograms if you were found to have a lower risk of breast cancer than the average woman of your age? Not at all satisfied (1) to very satisfied (5) | 4 (2; 4) | 327 |
| Overall attitudes score From 3 to 15; higher scores indicate more positive attitude | 12 (11; 14) | 327 |
| Positive attitudes to personalized screening (scores ≥ 12) and 95% confidence interval | 205 (62.7%) | 327 |
| (57.2%, 67.9%) | ||
| Intentions to participate in personalized breast screening | 326 | |
| Intending to participate (definitely or likely) | 299 (91.7%) | |
| 95% confidence interval | (88.2%, 94.5%) | |
| Definitely will | 207 (63.5%) | |
| Likely to | 92 (28.2%) | |
| Unsure | 20(6.1%) | |
| Not likely to or definitely will not | 7 (2.2%) | |
| Satisfaction with personalized screening (at 1 year) | 5 (5; 5) | 346 |
| Not at all satisfied | 1 (0.3%) | |
| Dissatisfied | 0 (0%) | |
| Neither satisfied nor dissatisfied | 9 (2.60%) | |
| Satisfied | 38 (11.0%) | |
| Extremely satisfied | 298 (86.1%) |
| Secondary Outcomes | Median (Q1; Q3) or n (%) | n |
|---|---|---|
| Attitudes towards having breast screening | ||
| Overall attitudes score | ||
| From 5 to 25; higher scores indicate more positive attitude | 22 (21; 25) | 286 |
| Positive attitudes to screening (scores ≥ 20) | 251 (87.8%) | 286 |
| Based on what you know, do you think measuring breast cancer risk will do | 325 | |
| More good than harm | 241 (74.2%) | |
| More harm than good | 12 (3.7%) | |
| It depends | 43 (13.2%) | |
| I don’t know | 29 (8.9%) | |
| Information on the individual risk of breast cancer provides reassurance | ||
| Strongly disagree (1) to strongly agree (5) | 4 (4; 5) | 327 |
| Receiving information about risks leads to anxiety | ||
| Strongly disagree (1) to strongly agree (5) | 3 (2; 4) | 327 |
| The information about the individual risk of breast cancer makes me worried | ||
| Strongly disagree (1) to strongly agree (5) | 3 (2; 4) | 326 |
| Preference with regard to the current screening (biennial exams between 50 and 69 years) | 326 | |
| Would choose personalized screening | 215 (66.0%) | |
| Would choose the current screening | 87 (26.7%) | |
| Don’t know | 24 ( 7.3%) | |
| Adequate knowledge (conceptual and numerical items combined) | ||
| Breast-cancer-mortality benefit | 56 (18.1%) | 310 |
| False positives | 21 (6.5%) | 324 |
| Overdiagnosis | 24 (8.3%) | 290 |
| Adequate knowledge across all three subscales | 5 (1.5%) | 328 |
| Adequate knowledge (conceptual items individually) | ||
| Screening is for women without symptoms | 283 (89.6%) | 316 |
| Screening reduces breast cancer deaths (benefit) | 264 (95.7%) | 276 |
| Screening will not find every breast cancer (benefit) | 130 (49.4%) | 263 |
| Screening may lead to false positive results (false positives) | 275 (96.5%) | 285 |
| Screening increases breast cancer diagnoses (overdiagnosis) | 225 (77.3%) | 291 |
| Overdiagnosis vs. false positives distinction (overdiagnosis) | 101 (39.6%) | 255 |
| Not all breast cancers cause illness and death (overdiagnosis) | 83 (34.3%) | 242 |
| Cannot predict if a cancer will cause harm (overdiagnosis) | 182 (77.8%) | 234 |
| Cancer that might not cause problems is treated (overdiagnosis) | 60 (25.3%) | 237 |
| Some women receive treatment they do not need (overdiagnosis) | 92 (43.0%) | 214 |
| Screening overdiagnoses more often than prevents deaths (overdiagnosis) | 60 (22.8%) | 263 |
| Decisional conflict | 247 | |
| Score: no decisional conflict (0) to extreme decisional conflict (100) | 10 (0; 25) | |
| 0 | 93 (37.6%) | |
| 1–24 | 78 (31.6%) | |
| ≥25 | 76 (30.8%) | |
| Confidence in decision making | ||
| Not at all confident (1) to very confident (5) | 4.7 (4.0; 5.0) | 322 |
| Anxiety about screening participation | ||
| Score, from 20 to 80, with higher scores indicating more anxiety | 30 (20; 40) | 297 |
| Worry about breast cancer | 308 | |
| Not worried at all | 119 (38.6%) | |
| A bit worried | 124 (40.3%) | |
| Quite worried or very worried | 65 (21.1%) | |
| Perceived significance of the benefits and the adverse effects of screening | ||
| In deciding whether to have screening, how important is it for you to consider the chance of… | ||
| Avoiding breast cancer death | 323 | |
| Very important | 273 (84.5%) | |
| Quite important | 32 (9.9%) | |
| A bit important | 8 (2.5%) | |
| Not at all important | 10 (3.1%) | |
| Being diagnosed and treated for a cancer that is not harmful | 321 | |
| Very important | 159 (49.5%) | |
| Quite important | 90 (28.1%) | |
| A bit important | 44 (13.7%) | |
| Not at all important | 28 (8.7%) | |
| Having a false positive. | 322 | |
| Very important | 166 (51.6%) | |
| Quite important | 83 (25.8%) | |
| A bit important | 41 (12.7%) | |
| Not at all important | 32 (9.9%) | |
| Self-efficacy | ||
| Strongly disagree (1) to strongly agree (5) | ||
| Breast cancer risk information makes me feel empowered as I have more knowledge | 4 (3; 5) | 322 |
| Information about the risks of screening increases my autonomy | 4 (3; 5) | 322 |
| Receiving and commenting on risk information from a healthcare professional makes me feel safer | 5 (4; 5) | 323 |
| Receiving and commenting on risk information from a healthcare professional makes me feel better about making decisions that affect my health | 5 (4; 5) | 324 |
| Overall self-efficacy score | ||
| From 4 to 20; higher scores indicate higher self-efficacy. | 17 (15; 19) | 321 |
| Experience assessment | ||
| Overall experience score | 22 (21; 25) | 309 |
| Positive experience to personalized screening (scores ≥ 20) | 256 (82.8%) | |
| Confidence in personalized screening Not at all confident (1) to very confident (5) | 5 (4; 5) | 321 |
| Understanding of the individual risk and the screening recommendations | ||
| Strongly disagree (1) to strongly agree (5) | ||
| I have understood the information I received about my risk for breast cancer in relation to women of my age | 5 (4; 5) | 319 |
| I have understood the recommendations given to me about the screening of breast cancer in the coming years based on my risk of breast cancer | 5 (4; 5) | 320 |
| Intention to follow the recommendations about breast cancer screening | 321 | |
| Definitely will | 244 (76.0%) | |
| Likely to | 59 (18.4%) | |
| Unsure | 11 (3.4%) | |
| Not likely to or definitely will not | 7 (2.2%) | |
| Time spent on risk communication (minutes) | 4.6 (3.2; 7.0) | 370 |
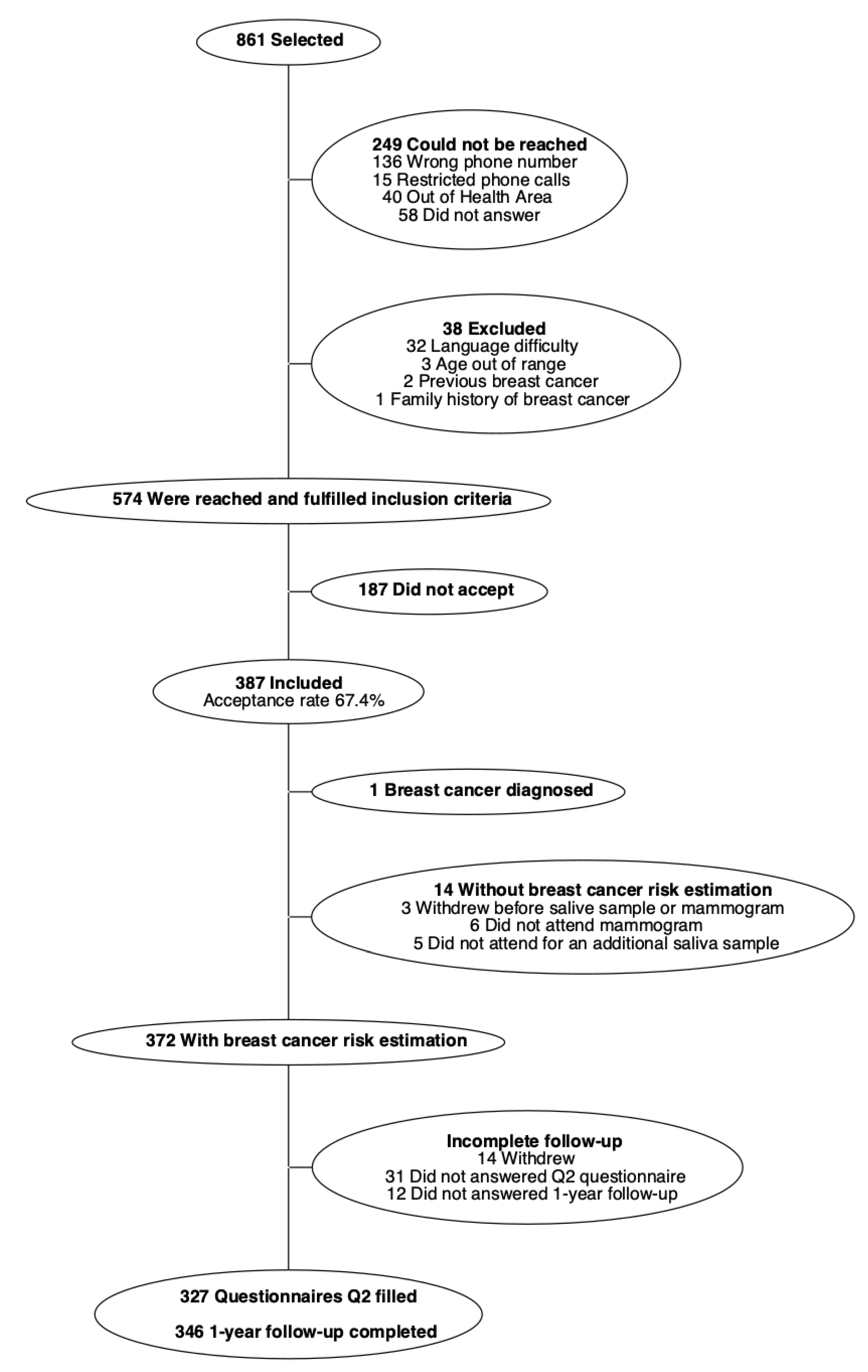
| Proportion of women who agreed to participate in the study | 387 (67.4%) | 574 |
| Proportion of participating women who completed the different phases of the study | 387 | |
| Risk estimation | 372 (96.1%) | |
| Follow-up questionnaire | 327 (84.5%) | |
| Assessment of satisfaction at 1-year | 349 (90.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laza-Vásquez, C.; Martínez-Alonso, M.; Forné-Izquierdo, C.; Vilaplana-Mayoral, J.; Cruz-Esteve, I.; Sánchez-López, I.; Reñé-Reñé, M.; Cazorla-Sánchez, C.; Hernández-Andreu, M.; Galindo-Ortego, G.; et al. Feasibility and Acceptability of Personalized Breast Cancer Screening (DECIDO Study): A Single-Arm Proof-of-Concept Trial. Int. J. Environ. Res. Public Health 2022, 19, 10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610426
Laza-Vásquez C, Martínez-Alonso M, Forné-Izquierdo C, Vilaplana-Mayoral J, Cruz-Esteve I, Sánchez-López I, Reñé-Reñé M, Cazorla-Sánchez C, Hernández-Andreu M, Galindo-Ortego G, et al. Feasibility and Acceptability of Personalized Breast Cancer Screening (DECIDO Study): A Single-Arm Proof-of-Concept Trial. International Journal of Environmental Research and Public Health. 2022; 19(16):10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610426
Chicago/Turabian StyleLaza-Vásquez, Celmira, Montserrat Martínez-Alonso, Carles Forné-Izquierdo, Jordi Vilaplana-Mayoral, Inés Cruz-Esteve, Isabel Sánchez-López, Mercè Reñé-Reñé, Cristina Cazorla-Sánchez, Marta Hernández-Andreu, Gisela Galindo-Ortego, and et al. 2022. "Feasibility and Acceptability of Personalized Breast Cancer Screening (DECIDO Study): A Single-Arm Proof-of-Concept Trial" International Journal of Environmental Research and Public Health 19, no. 16: 10426. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191610426