
Life-Space Mobility and Objectively Measured Movement Behavior in Older Adults with Hypertension after Receiving COVID-19 Vaccination

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Epidemiological Scenario before and after COVID-19 Vaccination
2.4. Study Procedures
2.5. Housing Characteristics
2.6. Objectively Measured Movement Behavior
2.7. Life-Space Mobility
2.8. Statistical Analysis
3. Results
3.1. Participant Characteristics
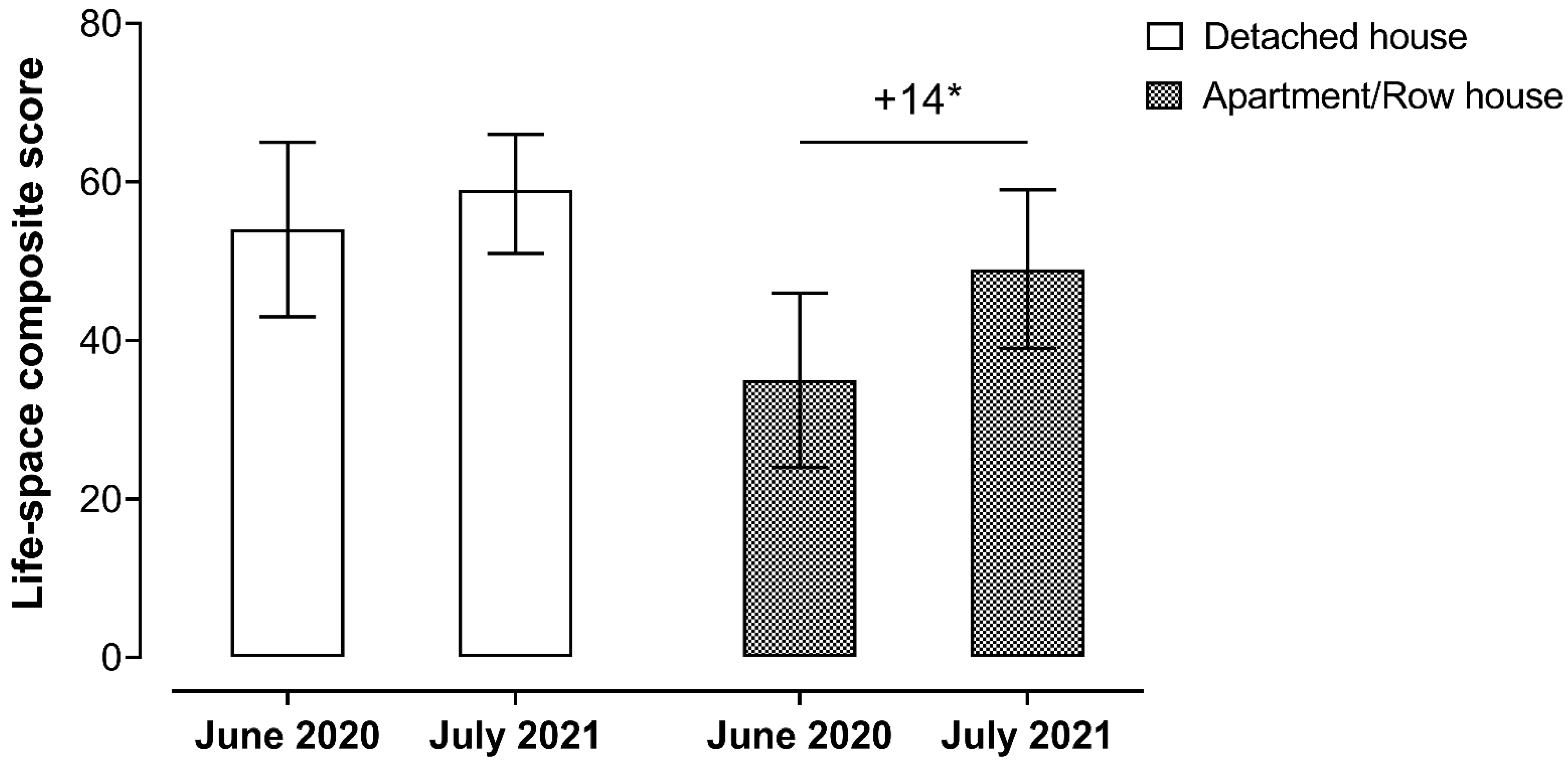
3.2. Changes in Life-Space Mobility after COVID-19 Vaccination
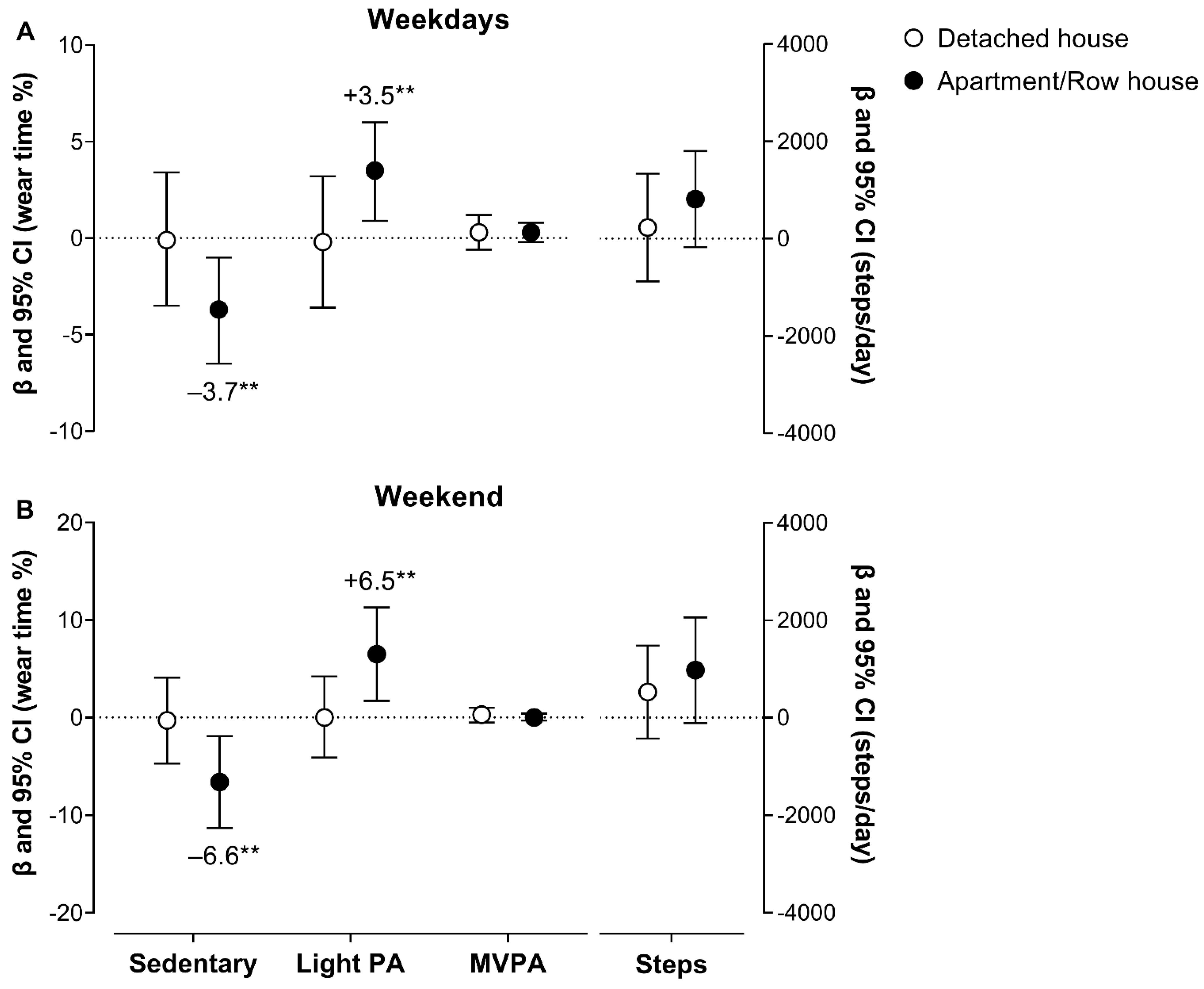
3.3. Moderating the Effect of Housing Type on Objectively Measured Changes in Movement Behavior after COVID-19 Vaccination
3.4. Objectively Measured Changes in the Volume of Movement Behavior after COVID-19 Vaccination
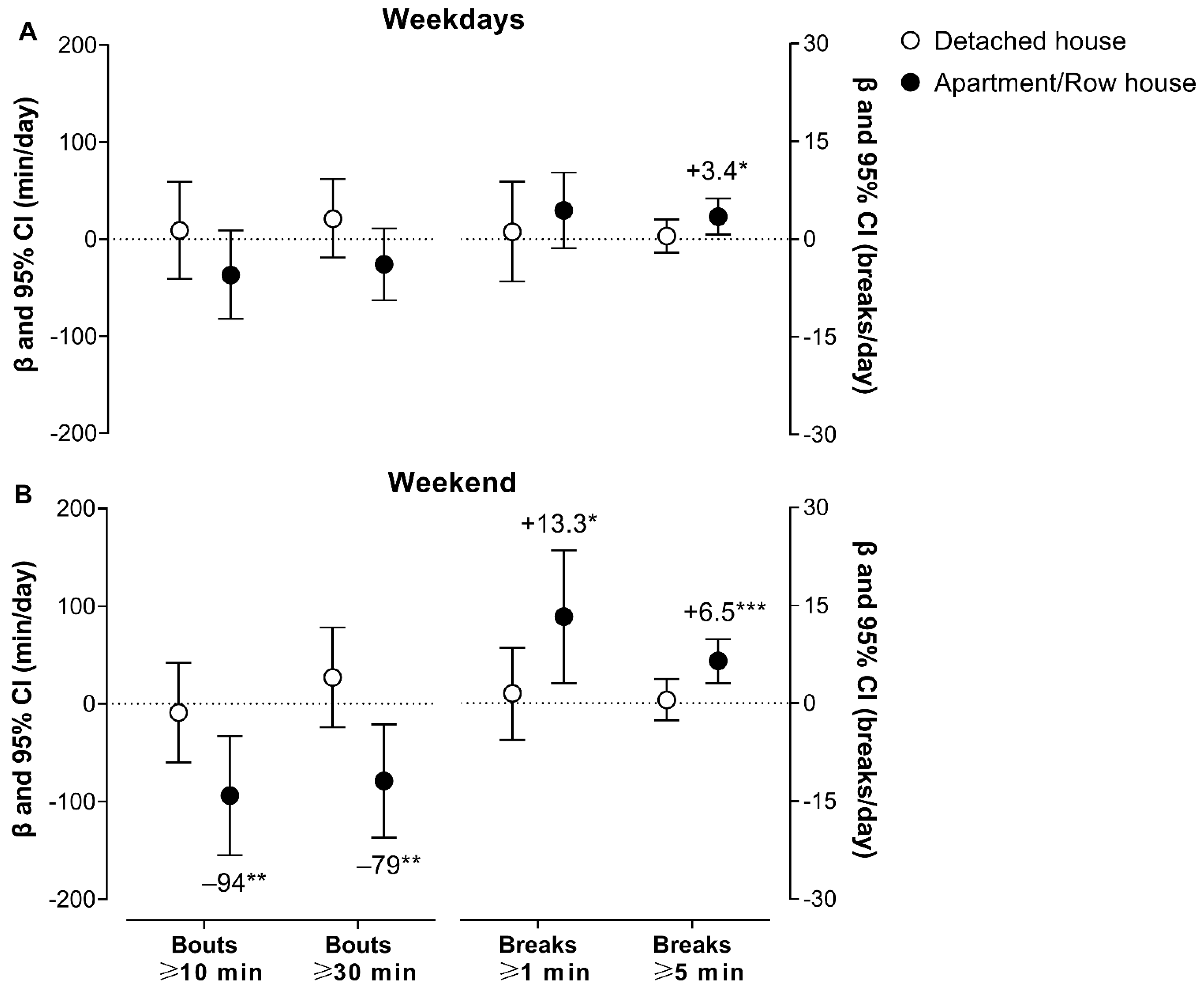
3.5. Objectively Measured Changes in the Movement Behavior Pattern after COVID-19 Vaccination
3.6. Associations of Changes in Life-Space Mobility with Objectively Measured Changes in Movement Behavior
4. Discussion
Practical Applications and Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19—31 August 2022; WHO: Geneva, Switzerland, 2022; p. 14. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---31-august-2022 (accessed on 5 September 2022).
- Aquino, E.M.L.; Silveira, I.H.; Pescarini, J.M.; Aquino, R.; De Souza-Filho, J.A.; Rocha, A.D.S.; Ferreira, A.; Victor, A.; Teixeira, C.; Machado, D.B.; et al. Social distancing measures to control the COVID-19 pandemic: Potential impacts and challenges in Brazil. Ciência Saúde Coletiva 2020, 25, 2423–2446. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities and its effects in patients infected with SARS-CoV-2: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, O.A.; Zanetti, A.D.S.; Antunes, E.F.; Longhi, F.G.; De Matos, T.A.; Battaglini, P.F. Prevalence of comorbidities in patients and mortality cases affected by SARS-CoV2: A systematic review and meta-analysis. Rev. Inst. Med. Trop. São Paulo 2020, 62, e43. [Google Scholar] [CrossRef] [PubMed]
- Perracini, M.R.; de Amorim, J.S.C.; Lima, C.A.; da Silva, A.; Trombini-Souza, F.; Pereira, D.S.; Pelicioni, P.H.S.; Duim, E.; Batista, P.P.; dos Santos, R.B.; et al. Impact of COVID-19 Pandemic on Life-Space Mobility of Older Adults Living in Brazil: REMOBILIZE Study. Front. Public Health 2021, 9, 643640. [Google Scholar] [CrossRef]
- Rantanen, T.; Eronen, J.; Kauppinen, M.; Kokko, K.; Sanaslahti, S.; Kajan, N.; Portegijs, E. Life-Space Mobility and Active Aging as Factors Underlying Quality of Life Among Older People Before and During COVID-19 Lockdown in Finland—A Longitudinal Study. J. Gerontol. Ser. A 2020, 76, e60–e67. [Google Scholar] [CrossRef]
- Saraiva, M.D.; Apolinario, D.; Avelino-Silva, T.J.; Tavares, C.D.A.M.; Gattás-Vernaglia, I.F.; Fernandes, C.M.; Rabelo, L.M.; Yamaguti, S.T.F.; Karnakis, T.; Kalil-Filho, R.; et al. The Impact of Frailty on the Relationship between Life-Space Mobility and Quality of Life in Older Adults during the COVID-19 Pandemic. J. Nutr. Health Aging 2020, 25, 440–447. [Google Scholar] [CrossRef]
- Taylor, J.K.; Buchan, I.E.; van der Veer, S.N. Assessing life-space mobility for a more holistic view on wellbeing in geriatric research and clinical practice. Aging Clin. Exp. Res. 2018, 31, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Browne, R.A.V.; Macêdo, G.A.D.; Cabral, L.L.P.; Oliveira, G.T.A.; Vivas, A.; Fontes, E.B.; Elsangedy, H.M.; Costa, E.C. Initial impact of the COVID-19 pandemic on physical activity and sedentary behavior in hypertensive older adults: An accelerometer-based analysis. Exp. Gerontol. 2020, 142, 111121. [Google Scholar] [CrossRef]
- Oliveira, M.R.; Sudati, I.P.; Konzen, V.D.M.; de Campos, A.C.; Wibelinger, L.M.; Correa, C.; Miguel, F.M.; Silva, R.N.; Borghi-Silva, A. Covid-19 and the impact on the physical activity level of elderly people: A systematic review. Exp. Gerontol. 2021, 159, 111675. [Google Scholar] [CrossRef]
- Pérez-Gisbert, L.; Torres-Sánchez, I.; Ortiz-Rubio, A.; Calvache-Mateo, A.; López-López, L.; Cabrera-Martos, I.; Valenza, M.C. Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12278. [Google Scholar] [CrossRef]
- Runacres, A.; Mackintosh, K.A.; Knight, R.L.; Sheeran, L.; Thatcher, R.; Shelley, J.; McNarry, M.A. Impact of the COVID-19 Pandemic on Sedentary Time and Behaviour in Children and Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11286. [Google Scholar] [CrossRef] [PubMed]
- Browne, R.A.V.; Cabral, L.L.P.; Freire, Y.A.; Macêdo, G.A.D.; Oliveira, G.T.A.; Vivas, A.; Elsangedy, H.M.; Fontes, E.B.; Costa, E.C. Housing type is associated with objectively measured changes in movement behavior during the COVID-19 pandemic in older adults with hypertension: An exploratory study. Arch. Gerontol. Geriatr. 2021, 94, 104354. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.-J.; Chan, K.-H.; Hung, I.F.-N. Safety and Efficacy of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Different Vaccines at Phase 3. Vaccines 2021, 9, 989. [Google Scholar] [CrossRef] [PubMed]
- Pormohammad, A.; Zarei, M.; Ghorbani, S.; Mohammadi, M.; Razizadeh, M.; Turner, D.; Turner, R. Efficacy and Safety of COVID-19 Vaccines: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Vaccines 2021, 9, 467. [Google Scholar] [CrossRef] [PubMed]
- Xing, K.; Tu, X.-Y.; Liu, M.; Liang, Z.-W.; Chen, J.-N.; Li, J.-J.; Jiang, L.-G.; Xing, F.-Q.; Jiang, Y. Efficacy and safety of COVID-19 vaccines: A systematic review. Chin. J. Contemp. Pediatrics 2021, 23, 221–228. [Google Scholar]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- González, S.; Olszevicki, S.; Salazar, M.; Calabria, A.; Regairaz, L.; Marín, L.; Campos, P.; Varela, T.; Martínez, V.V.G.; Ceriani, L.; et al. Effectiveness of the first component of Gam-COVID-Vac (Sputnik V) on reduction of SARS-CoV-2 confirmed infections, hospitalisations and mortality in patients aged 60-79: A retrospective cohort study in Argentina. eClinicalMedicine 2021, 40, 101126. [Google Scholar] [CrossRef]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Hitchings, M.D.T.; Ranzani, O.T.; Torres, M.S.S.; de Oliveira, S.B.; Almiron, M.; Said, R.; Borg, R.; Schulz, W.L.; de Oliveira, R.D.; da Silva, P.V.; et al. Effectiveness of CoronaVac among healthcare workers in the setting of high SARS-CoV-2 Gamma variant transmission in Manaus, Brazil: A test-negative case-control study. Lancet Reg. Health Am. 2021, 1, 100025. [Google Scholar] [CrossRef]
- Ranzani, O.T.; Hitchings, M.D.T.; Dorion, M.; D’Agostini, T.L.; de Paula, R.C.; de Paula, O.F.P.; Villela, E.F.D.M.; Torres, M.S.S.; de Oliveira, S.B.; Schulz, W.; et al. Effectiveness of the CoronaVac vaccine in older adults during a gamma variant associated epidemic of covid-19 in Brazil: Test negative case-control study. BMJ 2021, 374, n2015. [Google Scholar] [CrossRef]
- Victora, C.G.; Castro, M.C.; Gurzenda, S.; Medeiros, A.C.; França, G.V.; Barros, A.J. Estimating the early impact of vaccination against COVID-19 on deaths among elderly people in Brazil: Analyses of routinely-collected data on vaccine coverage and mortality. eClinicalMedicine 2021, 38, 101036. [Google Scholar] [CrossRef] [PubMed]
- Björk, J.; Inghammar, M.; Moghaddassi, M.; Rasmussen, M.; Malmqvist, U.; Kahn, F. High level of protection against COVID-19 after two doses of BNT162b2 vaccine in the working age population—First results from a cohort study in Southern Sweden. Infect. Dis. 2021, 54, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Hall, V.J.; Foulkes, S.; Saei, A.; Andrews, N.; Oguti, B.; Charlett, A.; Wellington, E.; Stowe, J.; Gillson, N.; Atti, A.; et al. COVID-19 vaccine coverage in health-care workers in England and effectiveness of BNT162b2 mRNA vaccine against infection (SIREN): A prospective, multicentre, cohort study. Lancet 2021, 397, 1725–1735. [Google Scholar] [CrossRef]
- Dagan, N.; Barda, N.; Kepten, E.; Miron, O.; Perchik, S.; Katz, M.A.; Hernán, M.A.; Lipsitch, M.; Reis, B.; Balicer, R.D. BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Mass Vaccination Setting. N. Engl. J. Med. 2021, 384, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.L.; Andrews, N.; Gower, C.; Robertson, C.; Stowe, J.; Tessier, E.; Simmons, R.; Cottrell, S.; Roberts, R.; O’Doherty, M.; et al. Effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines on covid-19 related symptoms, hospital admissions, and mortality in older adults in England: Test negative case-control study. BMJ 2021, 373, n1088. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). Interim Public Health Recommendations for Fully Vaccinated People. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated-guidance.html (accessed on 3 October 2021).
- Brazil Ministry of Health. Painel Coronavírus. 2021. Available online: https://covid.saude.gov.br (accessed on 17 October 2020).
- Brazil Ministry of Health. Secretariat of Health Surveillance. Special Epidemiological Bulletin 18. Coronavirus Disease—COVID-19. 2020; p. 42. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2020/boletim-epidemiologico-no-18-boletim-coe-coronavirus.pdf/view (accessed on 5 September 2022).
- State Department of Public Health of Rio Grande do Norte. Epidemiological Bulletin 76—Coronavirus Disease (COVID-19). 2020; p. 14. Available online: https://portalcovid19.saude.rn.gov.br/wp-content/uploads/2020/04/76_boletim_covid-19-1.pdf (accessed on 5 September 2022).
- Laboratory of Technological Innovation in Health. Regulatory of Intensive Care Unit Beds of Rio Grande do Norte, Brazil. In: Federal University of Rio Grande do Norte. 2021. Available online: https://regulacao.saude.rn.gov.br/sala-situacao/sala_publica/ (accessed on 17 October 2021).
- Brazil Ministry of Health. Secretariat of Health Surveillance. Special Epidemiological Bulletin 71. Coronavirus Disease—COVID-19. 2021; p. 108. Available online: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/covid-19/2021/boletim_epidemiologico_covid_71.pdf/view (accessed on 5 September 2022).
- State Department of Public Health of Rio Grande do Norte. Coronavirus Epidemiological Report (COVID-19). Special Edition—Epidemiological Week 27. 2021; p. 36. Available online: https://portalcovid19.saude.rn.gov.br/wp-content/uploads/2020/04/boletim-especial-SE-27.pdf (accessed on 5 September 2022).
- Svensson, A.C.; Forsberg, J.S.; Seblova, D.; Lager, A. Residential area and physical activity: A multi-level study of 68,000 adults in Stockholm County. Scand. J. Public Health 2016, 45, 25–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKee, G.; Kearney, P.; Kenny, R.A. The factors associated with self-reported physical activity in older adults living in the community. Age Ageing 2015, 44, 586–592. [Google Scholar] [CrossRef] [Green Version]
- Saidj, M.; Jørgensen, T.; Jacobsen, R.K.; Linneberg, A.; Aadahl, M. The influence of housing characteristics on leisure-time sitting. A prospective cohort study in Danish adults. Prev. Med. 2015, 81, 58–62. [Google Scholar] [CrossRef]
- Pettigrew, S.; Rai, R.; Jongenelis, M.I.; Jackson, B.; Beck, B.; Newton, R.U. The Potential Importance of Housing Type for Older People’s Physical Activity Levels. J. Appl. Gerontol. 2019, 39, 285–291. [Google Scholar] [CrossRef]
- Choi, L.; Liu, Z.; Matthews, C.E.; Buchowski, M.S. Validation of Accelerometer Wear and Nonwear Time Classification Algorithm. Med. Sci. Sports Exerc. 2011, 43, 357–364. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Mciver, K.L.; Pate, R.R. Conducting Accelerometer-Based Activity Assessments in Field-Based Research. Med. Sci. Sports Exerc. 2005, 37, S531–S543. [Google Scholar] [CrossRef] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of Time Spent in Sedentary Behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875–881. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Boerema, S.T.; Van Velsen, L.; Vollenbroek, M.; Hermens, H.J. Pattern measures of sedentary behaviour in adults: A literature review. Digit. Health 2020, 6, 2055207620905418. [Google Scholar] [CrossRef]
- Simões, M.D.S.M.; Garcia, I.F.; Costa, L.D.C.; Lunardi, A.C. Life-Space Assessment questionnaire: Novel measurement properties for Brazilian community-dwelling older adults. Geriatr. Gerontol. Int. 2018, 18, 783–789. [Google Scholar] [CrossRef]
- Peel, C.; Baker, P.S.; Roth, D.L.; Brown, C.J.; Brodner, E.V.; Allman, R.M. Assessing mobility in older adults: The UAB Study of Aging Life-Space Assessment. Phys. Ther. 2005, 85, 1008–1119. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, P.; Allman, R.M. Resilience in mobility in the context of chronic disease and aging. In New Frontiers in Resilient Aging; Fry, P.S., Keyes, C.L.M., Eds.; Cambridge University Press: Cambridge, UK, 2010; pp. 310–339. [Google Scholar] [CrossRef]
- Baker, P.S.; Bodner, E.V.; Allman, R.M. Measuring Life-Space Mobility in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2003, 51, 1610–1614. [Google Scholar] [CrossRef]
- Kennedy, R.E.; Sawyer, P.; Mph, C.P.W.; Lo, A.X.; Ritchie, C.S.; Roth, D.L.; Allman, R.M.; Brown, C.J. Life-Space Mobility Change Predicts 6-Month Mortality. J. Am. Geriatr. Soc. 2017, 65, 833–838. [Google Scholar] [CrossRef] [Green Version]
- Kammerlind, A.-S.C.; Fristedt, S.; Bravell, M.E.; Fransson, E. Test–retest reliability of the Swedish version of the Life-Space Assessment Questionnaire among community-dwelling older adults. Clin. Rehabil. 2014, 28, 817–823. [Google Scholar] [CrossRef]
- Babicki, M.; Malchrzak, W.; Hans-Wytrychowska, A.; Mastalerz-Migas, A. Impact of Vaccination on the Sense of Security, the Anxiety of COVID-19 and Quality of Life among Polish. A Nationwide Online Survey in Poland. Vaccines 2021, 9, 1444. [Google Scholar] [CrossRef] [PubMed]
- Boto-García, D.; Pino, J.F.B. Propelled: Evidence on the impact of vaccination against COVID-19 on travel propensity. Curr. Issues Tour. 2022, 25, 1–20. [Google Scholar] [CrossRef]
- Portegijs, E.; Rantakokko, M.; Viljanen, A.; Sipila, S.; Rantanen, T. Is frailty associated with life-space mobility and perceived autonomy in participation outdoors? A longitudinal study. Age Ageing 2016, 45, 550–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, C.J. Trajectories of Life-Space Mobility After Hospitalization. Ann. Intern. Med. 2009, 150, 372–378. [Google Scholar] [CrossRef] [PubMed]
- Galmes-Panades, A.M.; Varela-Mato, V.; Konieczna, J.; Wärnberg, J.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Schröder, H.; Vioque, J.; Alonso-Gómez, Á.M.; et al. Isotemporal substitution of inactive time with physical activity and time in bed: Cross-sectional associations with cardiometabolic health in the PREDIMED-Plus study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Pozo-Cruz, J.; García-Hermoso, A.; Alfonso-Rosa, R.M.; Alvarez-Barbosa, F.; Owen, N.; Chastin, S.; del Pozo-Cruz, B. Replacing Sedentary Time: Meta-analysis of Objective-Assessment Studies. Am. J. Prev. Med. 2018, 55, 395–402. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Owen, N.; Yates, T.; Kingwell, B.A.; Dunstan, D.W. Sitting Less and Moving More: Improved Glycaemic Control for Type 2 Diabetes Prevention and Management. Curr. Diabetes Rep. 2016, 16, 114. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Larsen, R.N.; Dunstan, D.W.; Owen, N.; Kingwell, B.A. Sitting Less and Moving More: Implications for hypertension. Hypertension 2018, 72, 1037–1046. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Detached House | Apartment/ Row House | p a | Overall | |
|---|---|---|---|---|
| n (%) | 17 (53.1) | 15 (46.9) | 32 | |
| Age, yrs | 67.5 ± 4.5 | 66.5 ± 3.5 | 0.467 | 67.0 ± 4.0 |
| Female, (%) | 9 (52.9) | 12 (80.0) | 0.147 | 21 (65.6) |
| Living with a partner, (%) | 9 (52.9) | 7 (46.7) | 1.000 | 16 (50.0) |
| Living with grandchildren, (%) | 5 (29.4) | 2 (13.3) | 0.402 | 7 (21.9) |
| Post-secondary education, (%) | 4 (23.5) | 3 (20.0) | 1.000 | 7 (21.9) |
| Employment status, (%) | ||||
| Employed (home office) | 4 (23.5) | 6 (40.0) | 0.450 | 10 (31.3) |
| Retired | 13 (76.5) | 9 (60.0) | 22 (68.8) | |
| Per capita income, (%) | ||||
| <1 MWS | 4 (23.5) | 4 (26.7) | 0.906 | 8 (25.0) |
| 1–2 MWS | 7 (41.2) | 7 (46.7) | 14 (43.8) | |
| >2 MWS | 6 (35.3) | 4 (26.7) | 10 (31.3) | |
| Income sufficiency (suitable/very good), (%) | 12 (70.6) | 8 (53.3) | 0.467 | 20 (62.5) |
| Ex-smoker, (%) | 6 (35.3) | 2 (13.3) | 0.229 | 8 (25.0) |
| Physically inactive, (%) | 12 (70.6) | 13 (86.7) | 0.402 | 25 (78.1) |
| Type 2 diabetes, (%) | 9 (52.9) | 4 (26.7) | 0.166 | 13 (40.6) |
| Dyslipidemia, (%) | 7 (41.2) | 6 (40.0) | 1.000 | 13 (40.6) |
| Hypertension diagnosis, yrs | 15.4 ± 11.9 | 10.8 ± 4.0 | 0.121 | 13.3 ± 9.3 |
| COVID-19 infected, (%) | 6 (35.3) | 4 (26.7) | 0.712 | 10 (31.3) |
| COVID-19 vaccine, (%) | ||||
| CoronaVac | 12 (70.6) | 9 (60.0) | 0.450 | 21 (65.6) |
| AstraZeneca/Oxford | 4 (23.5) | 6 (40.0) | 10 (31.3) | |
| Pfizer | 1 (5.9) | 0 (0.0) | 1 (3.1) | |
| Partially vaccinated, (%) | 6 (35.3) | 5 (33.3) | 1.000 | 11 (34.4) |
| Fully vaccinated, (%) | 11 (64.7) | 10 (66.7) | 21 (65.6) | |
| Household size, (%) | ||||
| 1–2 persons | 11 (64.7) | 10 (66.7) | 1.000 | 21 (65.6) |
| 3+ persons | 6 (35.3) | 5 (33.3) | 11 (34.4) | |
| Housing surface area, m2 | 284 ± 103 | 115 ± 69 | <0.001 | 205 ± 123 |
| Housing surface area, (%) | ||||
| ≤105 m2 | 1 (5.9) | 10 (66.7) | <0.001 | 11 (34.4) |
| 106–249 m2 | 7 (41.2) | 5 (33.3) | 12 (37.5) | |
| ≥250 m2 | 9 (52.9) | 0 (0.0) | 9 (28.1) |
| Detached House | Apartment/Row House | |||||||
|---|---|---|---|---|---|---|---|---|
| June 2020 | July 2021 | June 2020 | July 2021 | |||||
| EMM (95% CI) | EMM (95% CI) | β (95% CI) a | p | EMM (95% CI) | EMM (95% CI) | β (95% CI) a | p | |
| SEDENTARY BEHAVIOR | ||||||||
| Weekdays | ||||||||
| Sedentary, wear time % | 69.5 (65.5, 73.5) | 69.5 (66.6, 72.3) | −0.1 (−3.5, 3.4) | 0.970 | 73.9 (70.1, 77.6) | 70.1 (66.3, 74) | −3.7 (−6.5, −1) | 0.008 |
| Sedentary, min/day | 687 (648, 727) | 688 (660, 716) | 1 (−36, 38) | 0.963 | 728 (693, 764) | 698 (659, 737) | −31 (−62, 0) | 0.052 |
| Weekend | ||||||||
| Sedentary, wear time % | 70.2 (65.5, 74.8) | 69.8 (65.4, 74.3) | −0.3 (−4.7, 4.1) | 0.890 | 74.9 (69.5, 80.3) | 68.3 (64.9, 71.7) | −6.6 (−11.3, −1.9) | 0.007 |
| Sedentary, min/day | 660 (618, 702) | 660 (616, 704) | −1 (−44, 43) | 0.976 | 706 (657, 755) | 645 (614, 676) | −61 (−104, −17) | 0.007 |
| PHYSICAL ACTIVITY | ||||||||
| Weekdays | ||||||||
| Light PA, wear time % | 28.8 (25.5, 32.1) | 28.6 (25.6, 31.5) | −0.2 (−3.6, 3.2) | 0.903 | 25.1 (21.3, 28.9) | 28.6 (25, 32.1) | 3.5 (0.9, 6) | 0.009 |
| Light PA, min/day | 286 (254, 319) | 283 (254, 313) | −3 (−38, 32) | 0.869 | 251 (214, 288) | 281 (245, 316) | 29 (0, 59) | 0.053 |
| MVPA, wear time % | 1.7 (0.7, 2.6) | 2 (1.3, 2.6) | 0.3 (−0.6, 1.2) | 0.538 | 1 (0.1, 1.9) | 1.3 (0.4, 2.2) | 0.3 (−0.2, 0.8) | 0.268 |
| MVPA, min/day | 17.3 (7.7, 26.9) | 18.7 (12.9, 24.5) | 1.4 (−7.5, 10.4) | 0.753 | 11.1 (1.9, 20.4) | 11.9 (2.9, 21) | 0.8 (−5.1, 6.7) | 0.788 |
| Steps/day | 5556 (4103, 7008) | 5787 (4773, 6800) | 231 (−876, 1339) | 0.678 | 4222 (3152, 5292) | 5038 (3686, 6389) | 816 (−173, 1804) | 0.104 |
| Weekend | ||||||||
| Light PA, wear time % | 28.9 (24.7, 33) | 28.9 (24.5, 33.2) | 0 (−4.1, 4.2) | 0.995 | 24.5 (19, 29.9) | 31 (27.7, 34.3) | 6.5 (1.7, 11.3) | 0.008 |
| Light PA, min/day | 277 (240, 314) | 275 (232, 318) | −2 (−44, 40) | 0.931 | 235 (185, 284) | 295 (265, 325) | 61 (16, 106) | 0.009 |
| MVPA, wear time % | 1 (0.4, 1.7) | 1.3 (0.5, 2) | 0.3 (−0.5, 1) | 0.462 | 0.6 (0, 1.3) | 0.7 (0.3, 1.1) | 0 (−0.3, 0.4) | 0.815 |
| MVPA, min/day | 9.9 (3.7, 16) | 11.9 (4.8, 19) | 1.3 (−3.3, 6) | 0.520 | 6.7 (−0.3, 13.7) | 6.5 (2.4, 10.6) | −0.2 (−4.4, 3.9) | 0.911 |
| Steps/day | 4451 (3519, 5383) | 4976 (3775, 6178) | 525 (−430, 1480) | 0.275 | 3484 (2404, 4564) | 4460 (3551, 5369) | 976 (−109, 2061) | 0.077 |
| Detached House | Apartment/Row House | |||||||
|---|---|---|---|---|---|---|---|---|
| June 2020 | July 2021 | June 2020 | July 2021 | |||||
| EMM (95% CI) | EMM (95% CI) | β (95% CI) a | p | EMM (95% CI) | EMM (95% CI) | β (95% CI) a | p | |
| SEDENTARY BEHAVIOR | ||||||||
| Weekdays | ||||||||
| Sedentary bouts ≥ 10 min, bouts/day | 20.1 (18.1, 22.1) | 19.7 (18.4, 20.9) | −0.4 (−2.6, 1.7) | 0.692 | 21.3 (19.8, 22.7) | 20.1 (18.6, 21.7) | −1.1 (−2.7, 0.4) | 0.158 |
| Sedentary bouts ≥ 30 min, bouts/day | 3.9 (3.4, 4.5) | 4.3 (3.5, 5.1) | 0.4 (−0.5, 1.3) | 0.435 | 5.1 (4.2, 6) | 4.7 (4, 5.3) | −0.4 (−1.2, 0.3) | 0.260 |
| Sedentary bouts ≥ 10 min, min/day | 441 (394, 489) | 450 (408, 493) | 9 (−41, 59) | 0.721 | 502 (448, 556) | 466 (417, 514) | −37 (−82, 9) | 0.113 |
| Sedentary bouts ≥ 30 min, min/day | 184 (158, 210) | 205 (165, 245) | 21 (−19, 62) | 0.299 | 241 (192, 290) | 215 (180, 250) | −26 (−63, 11) | 0.162 |
| Length of sedentary bouts, min/day | 6.8 (6.2, 7.5) | 6.8 (6, 7.6) | 0 (−0.8, 0.7) | 0.940 | 7.8 (6.8, 8.7) | 6.9 (6.3, 7.6) | −0.9 (−1.6, −0.1) | 0.020 |
| Breaks ≥ 1 min, breaks/day | 102 (96, 109) | 104 (95, 112) | 1.1 (−6.5, 8.8) | 0.770 | 98 (89, 106) | 102 (96, 108) | 4.4 (−1.4, 10.2) | 0.133 |
| Breaks ≥ 5 min, breaks/day | 16.6 (13.2, 20) | 17.1 (14.2, 19.9) | 0.5 (−2.1, 3) | 0.713 | 12.9 (9.7, 16.1) | 16.3 (13.2, 19.4) | 3.5 (0.7, 6.2) | 0.015 |
| Break rate ≥ 1 min, breaks/h | 6.2 (5.8, 6.6) | 6.3 (5.8, 6.8) | 0.1 (−0.4, 0.6) | 0.675 | 5.9 (5.4, 6.4) | 6.2 (5.8, 6.5) | 0.3 (−0.1, 0.6) | 0.119 |
| Break rate ≥ 5 min, breaks/h | 1 (0.8, 1.2) | 1 (0.9, 1.2) | 0 (−0.1, 0.2) | 0.602 | 0.8 (0.6, 1) | 1 (0.8, 1.2) | 0.2 (0.1, 0.4) | 0.009 |
| Weekend | ||||||||
| Sedentary bouts ≥ 10 min, bouts/day | 20.3 (18.2, 22.4) | 18.7 (16.6, 20.7) | −1.6 (−3.7, 0.4) | 0.120 | 20.3 (18.2, 22.5) | 18.1 (16.2, 19.9) | −2.2 (−4.3, −0.1) | 0.036 |
| Sedentary bouts ≥ 30 min, bouts/day | 4.2 (3.1, 5.2) | 4.9 (3.7, 6.1) | 0.7 (−0.6, 2.1) | 0.287 | 4.9 (3.6, 6.1) | 3.4 (2.7, 4.1) | −1.4 (−2.6, −0.3) | 0.012 |
| Sedentary bouts ≥ 10 min, min/day | 448 (398, 499) | 439 (376, 502) | −9 (−60, 42) | 0.725 | 486 (422, 551) | 392 (346, 438) | −94 (−155, −33) | 0.003 |
| Sedentary bouts ≥ 30 min, min/day | 189 (139, 239) | 216 (161, 271) | 27 (−24, 78) | 0.294 | 235 (171, 300) | 157 (123, 190) | −79 (−137, −21) | 0.008 |
| Length of sedentary bouts, min/day | 7.3 (6.4, 8.2) | 7.3 (6.2, 8.3) | 0 (−0.8, 0.7) | 0.942 | 7.9 (6.7, 9.1) | 6.3 (5.6, 7) | −1.6 (−2.9, −0.3) | 0.014 |
| Breaks ≥ 1 min, breaks/day | 93.8 (87.2, 100.3) | 95.2 (88, 102.5) | 1.5 (5.8, 8.5) | 0.680 | 93.4 (84, 102.9) | 106.7 (97.7, 115.7) | 13.3 (3.1, 23.4) | 0.011 |
| Breaks ≥ 5 min, breaks/day | 15.3 (12.4, 18.2) | 15.8 (12.1, 19.6) | 0.5 (−2.6, 3.7) | 0.729 | 10.9 (7.6, 14.3) | 17.4 (14.8, 20.1) | 6.5 (3.1, 9.8) | <0.001 |
| Break rate ≥ 1 min, breaks/h | 5.9 (5.5, 6.4) | 6 (5.6, 6.5) | 0.1 (−0.4, 0.5) | 0.767 | 5.9 (5.3, 6.5) | 6.7 (6.2, 7.2) | 0.8 (0.2, 1.4) | 0.015 |
| Break rate ≥ 5 min, breaks/h | 1 (0.8, 1.1) | 1 (0.8, 1.2) | 0 (−0.2, 0.2) | 0.694 | 0.7 (0.5, 0.9) | 1.1 (0.9, 1.3) | 0.4 (0.2, 0.6) | <0.001 |
| PHYSICAL ACTIVITY | ||||||||
| Weekdays | ||||||||
| Light PA in bouts ≥ 10 min, bouts/day | 3.7 (2.8, 4.6) | 3.1 (2.1, 4.2) | −0.6 (−1.5, 0.4) | 0.240 | 3 (1.8, 4.2) | 3.4 (1.9, 4.9) | 0.4 (−0.8, 1.6) | 0.514 |
| Light PA in bouts ≥ 10 min, min/day | 54.6 (40.6, 68.5) | 46.2 (27.6, 64.8) | −8.4 (−26.1, 9.4) | 0.350 | 41.8 (24.3, 59.4) | 47.1 (24, 70.3) | 5.3 (−12.4, 22.9) | 0.552 |
| MVPA in bouts ≥ 10 min, bouts/day | 0.2 (0.1, 0.4) | 0.2 (0.1, 0.4) | 0.0 (−0.3, 0.2) | 0.819 | 0.2 (0.0, 0.5) | 0.2 (0.0, 0.4) | 0.0 (−0.2, 0.2) | 0.851 |
| MVPA in bouts ≥ 10 min, min/day | 4.5 (1.3, 7.7) | 4.5 (0.6, 8.4) | 0 (−5.1, 5) | 0.990 | 7.4 (−1.3, 16.1) | 3.7 (−1.4, 8.8) | −3.7 (−9.1, 1.8) | 0.185 |
| Weekend | ||||||||
| Light PA in bouts ≥ 10 min, bouts/day | 4.5 (3, 6) | 3.8 (2.5, 5.1) | 0.7 (−2, 0.6) | 0.300 | 2.9 (1, 4.7) | 3.2 (2, 4.4) | 0.3 (−1.2, 1.9) | 0.667 |
| Light PA in bouts ≥ 10 min, min/day | 67.2 (43.2, 91.2) | 59.2 (37.1, 81.3) | −8 (−29.6, 13.6) | 0.462 | 44.4 (9.7, 79.2) | 44.1 (27.4, 60.9) | −0.3 (−28.8, 28.2) | 0.983 |
| MVPA in bouts ≥ 10 min, bouts/day | 0.1 (−0.1, 0.4) | 0.2 (−0.1, 0.5) | 0.1 (−0.2, 0.3) | 0.447 | 0.1 (0, 0.3) | 0 (0, 0.1) | −0.1 (−0.3, 0) | 0.120 |
| MVPA in bouts ≥ 10 min, min/day | 1.4 (−1.2, 4) | 4.3 (−2.1, 10.7) | 2.9 (−3.4, 9.1) | 0.359 | 5 (−1.9, 11.8) | 1.3 (−1.5, 4) | −3.7 (−10.4, 3) | 0.274 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Browne, R.A.V.; Cabral, L.L.P.; Oliveira, G.T.A.; Macêdo, G.A.D.; Sócrates, J.; Silva, R.d.M.; Araújo, M.B.F.; Freire, Y.A.; Costa, E.C. Life-Space Mobility and Objectively Measured Movement Behavior in Older Adults with Hypertension after Receiving COVID-19 Vaccination. Int. J. Environ. Res. Public Health 2022, 19, 12532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912532
Browne RAV, Cabral LLP, Oliveira GTA, Macêdo GAD, Sócrates J, Silva RdM, Araújo MBF, Freire YA, Costa EC. Life-Space Mobility and Objectively Measured Movement Behavior in Older Adults with Hypertension after Receiving COVID-19 Vaccination. International Journal of Environmental Research and Public Health. 2022; 19(19):12532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912532
Chicago/Turabian StyleBrowne, Rodrigo A. V., Ludmila L. P. Cabral, Gledson T. A. Oliveira, Geovani A. D. Macêdo, Júlio Sócrates, Raíssa de M. Silva, Maria B. F. Araújo, Yuri A. Freire, and Eduardo C. Costa. 2022. "Life-Space Mobility and Objectively Measured Movement Behavior in Older Adults with Hypertension after Receiving COVID-19 Vaccination" International Journal of Environmental Research and Public Health 19, no. 19: 12532. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912532