
Acute Effects of Ischemic Intra-Conditioning on 30 m Sprint Performance
 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
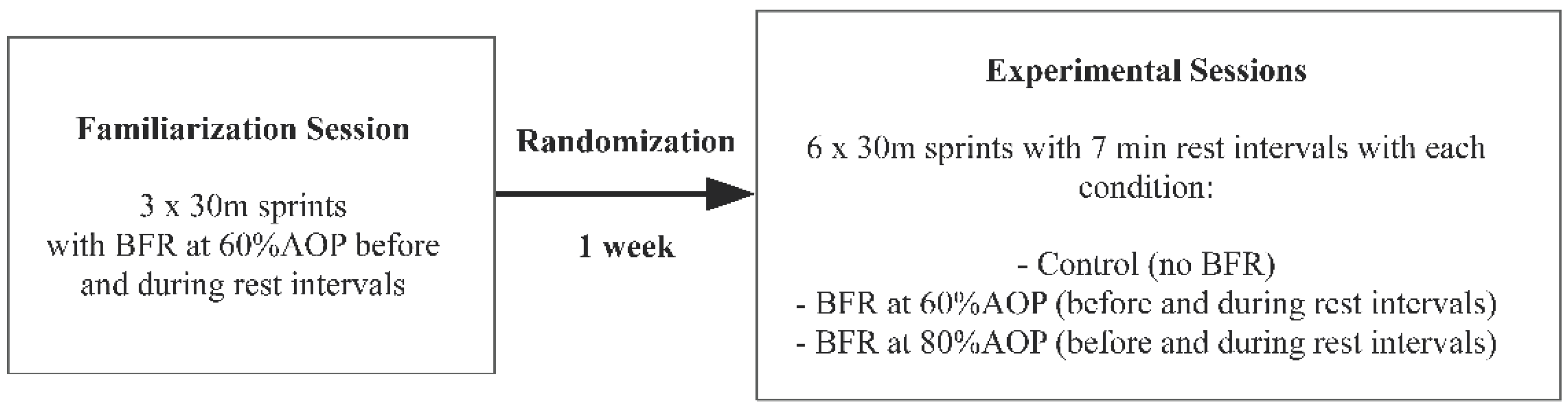
2.1. Experimental Approach to the Problem
2.2. Subjects
2.3. Procedures
2.3.1. Familiarization Session
2.3.2. Experimental Sessions
2.3.3. Ischemic Intra-Conditioning Procedure
2.3.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wilk, M.; Krzysztofik, M.; Jarosz, J.; Krol, P.; Leznicka, K.; Zajac, A.; Stastny, P.; Bogdanis, G.C. Impact of Ischemic Intra-Conditioning on Power Output and Bar Velocity of the Upper Limbs. Front. Physiol. 2021, 12, 626915. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Kawamoto, K.; Yasuda, T.; Kearns, C.F.; Midorikawa, T.; Sato, Y. Eight days KAATSU-resistance training improved sprint but not jump performance in collegiate male track and field athletes. Int. J. KAATSU Train. Res. 2005, 1, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Cook, C.J.; Kilduff, L.P.; Beaven, C.M. Improving Strength and Power in Trained Athletes with 3 Weeks of Occlusion Training. Int. J. Sport. Physiol. Perform. 2014, 9, 166–172. [Google Scholar] [CrossRef]
- Kaijser, L.; Sundberg, C.J.; Eiken, O.; Nygren, A.; Esbjornsson, M.; Sylven, C.; Jansson, E. Muscle oxidative capacity and work performance after training under local leg ischemia. J. Appl. Physiol. 1990, 69, 785–787. [Google Scholar] [CrossRef] [PubMed]
- Scott, B.R.; Loenneke, J.P.; Slattery, K.M.; Dascombe, B.J. Blood flow restricted exercise for athletes: A review of available evidence. J. Sci. Med. Sport 2016, 19, 360–367. [Google Scholar] [CrossRef] [PubMed]
- Burgomaster, K.A.; Moore, D.R.; Schofield, L.M.; Phillips, S.M.; Sale, D.G.; Gibala, M.J. Resistance Training with Vascular Occlusion: Metabolic Adaptations in Human Muscle. Med. Sci. Sport. Exerc. 2003, 35, 1203–1208. [Google Scholar] [CrossRef]
- Sundberg, C.J. Exercise and training during graded leg ischaemia in healthy man with special reference to effects on skeletal muscle. Acta Physiol. Scandinavica. Suppl. 1994, 615, 1–50. [Google Scholar]
- Esbjörnsson, M.; Jansson, E.; Sundberg, C.J.; Sylvén, C.; Eiken, O.; Nygren, A.; Kaijser, L. Muscle fibre types and enzyme activities after training with local leg ischaemia in man. Acta Physiol. Scand. 1993, 148, 233–241. [Google Scholar] [CrossRef]
- Mitchell, E.A.; Martin, N.R.W.; Turner, M.C.; Taylor, C.W.; Ferguson, R.A. The combined effect of sprint interval training and blood flow restriction on critical power, capillary growth and mitochondrial proteins in trained cyclists. J. Appl. Physiol. 2019, 126, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.T.; Hsieh, Y.Y.; Ho, J.Y.; Lin, J.C. Effects of Running Exercise Combined with Blood Flow Restriction on Strength and Sprint Performance. J. Strength Cond. Res. 2021, 35, 3090–3096. [Google Scholar] [CrossRef]
- Trybulski, R.; Jarosz, J.; Krzysztofik, M.; Lachowicz, M.; Trybek, G.; Zajac, A.; Wilk, M. Ischemia during rest intervals between sets prevents decreases in fatigue during the explosive squat exercise—a randomized, crossover study. Sci. Rep. 2022, 12, 5922. [Google Scholar] [CrossRef]
- Gepfert, M.; Jarosz, J.; Wojdala, G.; Krzysztofik, M.; Campos, Y.; Filip-Stachnik, A.; Kostrzewa, M.; Gawel, D.; Szkudlarek, A.; Godlewski, P.; et al. Acute impact of blood flow restriction on strength-endurance performance during the bench press exercise. Biol. Sport 2021, 38, 653–658. [Google Scholar] [CrossRef]
- Behringer, M.; Behlau, D.; Montag, J.C.K.; McCourt, M.L.; Mester, J. Low-Intensity Sprint Training with Blood Flow Restriction Improves 100-m Dash. J. Strength Cond. Res. 2017, 31, 2462–2472. [Google Scholar] [CrossRef]
- Ellefsen, S.; Hammarström, D.; Strand, T.A.; Zacharo, E.; Whist, J.E.; Rauk, I.; Nygaard, H.; Vegge, G.; Hanestadhaugen, M.; Wernbom, M.; et al. Blood flow-restricted strength training displays high functional and biological ecacy in women: A within-subject comparison with high-load strength training. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2015, 309, R767–R779. [Google Scholar] [CrossRef] [Green Version]
- Kacin, A.; Strazar, K. Frequent low-load ischemic resistance exercise to failure enhances muscle oxygen delivery and endurance capacity. Scand. J. Med. Sci. Sport. 2011, 21, e231–e241. [Google Scholar] [CrossRef] [PubMed]
- Schwiete, C.; Franz, A.; Roth, C.; Behringer, M. Effects of Resting vs. Continuous Blood-Flow Restriction-Training on Strength, Fatigue Resistance, Muscle Thickness, and Perceived Discomfort. Front. Physiol. 2021, 12, 663665. [Google Scholar] [CrossRef] [PubMed]
- Gepfert, M.; Krzysztofik, M.; Kostrzewa, M.; Jarosz, J.; Trybulski, R.; Zajac, A.; Wilk, M. The Acute Impact of External Compression on Back Squat Performance in Competitive Athletes. Int. J. Environ. Res. Public Health 2020, 17, 4674. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Sherk, V.D.; Thiebaud, R.S.; Abe, T.; Bemben, D.A.; Bemben, M.G. Effects of cuff width on arterial occlusion: Implications for blood flow restricted exercise. Eur. J. Appl. Physiol. 2012, 112, 2903–2912. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Abe, T.; Wilson, J.M.; Ugrinowitsch, C.; Bemben, M.G. Blood Flow Restriction: How Does It Work? Front. Physiol. 2012, 3, 392. [Google Scholar] [CrossRef] [Green Version]
- Karabulut, M.; Mccarron, J.; Abe, T.; Sato, Y.; Bemben, M. The effects of different initial restrictive pressures used to reduce blood flow and thigh composition on tissue oxygenation of the quadriceps. J. Sport. Sci. 2011, 29, 951–958. [Google Scholar] [CrossRef]
- Kocman, E.A.; Ozatik, O.; Sahin, A.; Guney, T.; Kose, A.A.; Dag, I.; Alatas, O.; Cetin, C. Effects of ischemic preconditioning protocols on skeletal muscle ischemia–reperfusion injury. J. Surg. Res. 2015, 193, 942–952. [Google Scholar] [CrossRef]
- Barbosa, T.C.; Machado, A.C.; Braz, I.D.; Fernandes, I.A.; Vianna, L.C.; Nobrega, A.C.L.; Silva, B.M. Remote ischemic preconditioning delays fatigue development during handgrip exercise. Scand. J. Med. Sci. Sport. 2014, 25, 356–364. [Google Scholar] [CrossRef] [PubMed]
- de Groot, P.C.; Thijssen, D.H.; Sanchez, M.; Ellenkamp, R.; Hopman, M.T. Ischemic preconditioning improves maximal performance in humans. Eur. J. Appl. Physiol. 2010, 108, 141–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, M.; Ueda, K.; Goto, C.; Jitsuiki, D.; Nishioka, K.; Umemura, T.; Noma, K.; Yoshizumi, M.; Chayama, K.; Higashi, Y. Repetition of ischemic preconditioning augments endothelium-dependent vasodilation in humans: Role of endothelium-derived nitric oxide and endothelial progenitor cells. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 1403–1410. [Google Scholar] [CrossRef] [PubMed]
- Lawson, C.; Downey, J. Preconditioning: State of the art myocardial protection. Cardiovasc. Res. 1993, 27, 542–550. [Google Scholar] [CrossRef] [PubMed]
- Li, X.D.; Cheng, Y.T.; Yang, Y.J.; Meng, X.M.; Zhao, J.L.; Zhang, H.T.; You, S.J.; Wu, Y.L. PKA-mediated eNOS phosphorylation in the protection of ischemic preconditioning against no-reflow. Microvasc. Res. 2012, 84, 44–54. [Google Scholar] [CrossRef]
- Paganelli, W.; Pendergast, D.R.; Koness, J.; Cerretelli, P. The effect of decreased muscle energy stores on the VO2 kinetics at the onset of exercise. Eur. J. Appl. Physiol. Occup. Physiol. 1989, 59, 321–326. [Google Scholar] [CrossRef]
- Pang, C.Y.; Yang, R.Z.; Zhong, A.; Xu, N.; Boyd, B.; Forrest, C.R. Acute ischaemic preconditioning protects against skeletal muscle infarction in the pig. Cardiovasc. Res. 1995, 29, 782–788. [Google Scholar] [CrossRef]
- Paradis-Deschênes, P.; Joanisse, D.R.; Billaut, F. Ischemic preconditioning increases muscle perfusion, oxygen uptake, and forcein strength-trained athletes. Appl. Physiol. Nutr. Metab. 2016, 41, 938–944. [Google Scholar] [CrossRef] [Green Version]
- Torma, F.; Gombos, Z.; Fridvalszki, M.; Langmar, G.; Tarcza, Z.; Merkely, B.; Naito, H.; Ichinoseki-Sekine, N.; Takeda, M.; Murlasitsf, Z.; et al. Blood flow restriction in human skeletal muscle during rest periods after high-load resistance training down-regulates miR 206 and induces Pax7. J. Sport Health Sci. 2021, 10, 470–477. [Google Scholar] [CrossRef]
- Winbanks, C.E.; Beyer, C.; Hagg, A.; Qian, H.; Sepulveda, P.V.; Gregorevic, P. miR-206 Represses Hypertrophy of Myogenic Cells but Not Muscle Fibers via Inhibition of HDAC4. PLoS ONE 2013, 8, e73589. [Google Scholar] [CrossRef] [PubMed]
- Taylor, C.W.; Ingham, S.A.; Ferguson, R.A. Acute and chronic effect of sprint interval training combined with postexercise blood-flow restriction in trained individuals. Exp. Physiol. 2016, 101, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rolnick, N.; Kimbrell, K.; Cerqueira, M.S.; Weatherford, B.; Brandner, C. Perceived Barriers to Blood Flow Restriction Training. Front. Rehabil. Sci. 2021. [Google Scholar] [CrossRef]
- Brandner, C.R.; Warmington, S.A. Delayed Onset Muscle Soreness and Perceived Exertion after Blood Flow Restriction Exercise. J. Strength Cond. Res. 2017, 31, 3101–3108. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.B.; Brown, K.A.; DeRuisseau, K.; Kanaley, J.A.; Ploutz-Snyder, L.L. Skeletal muscle adaptations following blood flow-restricted training during 30 days of muscular unloading. J. Appl. Physiol. 2010, 109, 341–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, B.C.; Manini, T.M. Can KAATSU exercise cause rhabdomyolysis? Clin. J. Sport Med. 2017, 27, e1–e2. [Google Scholar] [CrossRef] [PubMed]
- Wernbom, M.; Paulsen, G.; Bjørnsen, T.; Cumming, K.; Raastad, T. Risk of Muscle Damage with Blood Flow–Restricted Exercise Should Not Be Overlooked. Clin. J. Sport Med. 2021, 31, 223–224. [Google Scholar] [CrossRef]
- Neto, G.R.; Novaes, J.S.; Salerno, V.P.; Gonçalves, M.M.; Batista, G.R.; Cirilo-Sousa, M.S. Does a resistance exercise session with continuous or intermittent blood flow restriction promote muscle damage and increase oxidative stress? J. Sport. Sci. 2017, 36, 104–110. [Google Scholar] [CrossRef]
- Pearson, S.J.; Hussain, S.R. A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sport. Med. 2014, 45, 187–200. [Google Scholar] [CrossRef]


{kind=link}
| CONTROL [s] (95% CI) | BFR 60% AOP [s] (95% CI) | BFR 80% AOP [s] (95% CI) | Interaction Condition × Sprint Trial | Main effect of BFR Condition | |
|---|---|---|---|---|---|
| Sprint no. 1 | 4.46 ± 0.33 (4.34 to 4.57) | 4.48 ± 0.30 (4.37 to 4.58) | 4.45 ± 0.30 (4.34 to 4.56) | 0.052 | 0.190 |
| Sprint no. 2 | 4.44 ± 0.35 (4.32 to 4.56) | 4.47 ± 0.32 (4.36 to 4.58) | 4.44 ± 0.32 (4.33 to 4.55) | ||
| Sprint no. 3 | 4.48 ± 0.34 (4.36 to 4.59) | 4.46 ± 0.35 (4.34 to 4.58) | 4.44 ± 0.33 (4.33 to 4.56) | ||
| Sprint no. 4 | 4.44 ± 0.32 (4.33 to 4.55) | 4.46 ± 0.34 (4.34 to 4.58) | 4.47 ± 0.32 (4.35 to 4.58) | ||
| Sprint no. 5 | 4.47 ± 0.32 (4.36 to 4.58) | 4.51 ± 0.33 (4.39 to 4.62) | 4.48 ± 0.32 (4.37 to 4.59) | ||
| Sprint no. 6 | 4.44 ± 0.34 (4.32 to 4.56) | 4.46 ± 0.36 (4.33 to 4.58) | 4.48 ± 0.30 (4.37 to 4.58) |
| CONTROL vs. BFR 60% AOP | CONTROL vs. BFR 80% AOP | BFR 60% AOP vs. BFR 80% AOP | |
|---|---|---|---|
| Sprint no. 1 | 0.06 | 0.03 | 0.10 |
| Sprint no. 2 | 0.09 | 0.00 | 0.09 |
| Sprint no. 3 | 0.06 | 0.12 | 0.06 |
| Sprint no. 4 | 0.06 | 0.09 | 0.03 |
| Sprint no. 5 | 0.12 | 0.03 | 0.09 |
| Sprint no. 6 | 0.06 | 0.13 | 0.06 |
| CONTROL [s] (95% CI) | BFR 60% AOP [s] (95% CI) | BFR 80% AOP [s] (95% CI) | Interaction Condition × Delta Sprint | Main Effect of Delta BFR Condition | |
|---|---|---|---|---|---|
| Sprint no. 2—Sprint no. 1 | −0.020± 0.097 (−0.054 to 0.014) | 0.016 ± 0.111 (−0.022 to 0.055) | −0.019 ± 0.116 (−0.060 to 0.021) | 0.016 * | 0.59 |
| Sprint no. 3—Sprint no. 1 | 0.010 ± 0.136 (−0.037 to 0.057) | −0.016 ± 0.122 (−0.058 to 0.027) | −0.009 ± 0.093 (−0.042to 0.023) | ||
| Sprint no. 4—Sprint no. 1 | −0.019 ± 0.133 (−0.065 to 0.028) | −0.017 ± 0.110 (−0.056 to 0.021) | 0.026 ± 0.153 (−0.027 to 0.079) | ||
| Sprint no. 5—Sprint no. 1 | −0.022 ± 0.116 (−0.062 to 0.019) | −0.008 ± 0.096 (−0.041to 0.026) | −0.008 ± 0.101 (−0.043to 0.027) | ||
| Sprint no. 6—Sprint no. 1 | 0.015 ± 0.088 (−0.016 to 0.046) | 0.030 ± 0.119 (−0.012 to 0.071) | 0.026 ±0.080 (−0.002 to 0.054) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fostiak, K.; Bichowska, M.; Trybulski, R.; Trabka, B.; Krzysztofik, M.; Rolnick, N.; Filip-Stachnik, A.; Wilk, M. Acute Effects of Ischemic Intra-Conditioning on 30 m Sprint Performance. Int. J. Environ. Res. Public Health 2022, 19, 12633. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912633
Fostiak K, Bichowska M, Trybulski R, Trabka B, Krzysztofik M, Rolnick N, Filip-Stachnik A, Wilk M. Acute Effects of Ischemic Intra-Conditioning on 30 m Sprint Performance. International Journal of Environmental Research and Public Health. 2022; 19(19):12633. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912633
Chicago/Turabian StyleFostiak, Krzysztof, Marta Bichowska, Robert Trybulski, Bartosz Trabka, Michal Krzysztofik, Nicholas Rolnick, Aleksandra Filip-Stachnik, and Michal Wilk. 2022. "Acute Effects of Ischemic Intra-Conditioning on 30 m Sprint Performance" International Journal of Environmental Research and Public Health 19, no. 19: 12633. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph191912633