
Use of Irrigation Device for Duct Dilatation during Sialendoscopy
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Discussion
4. Conclusions
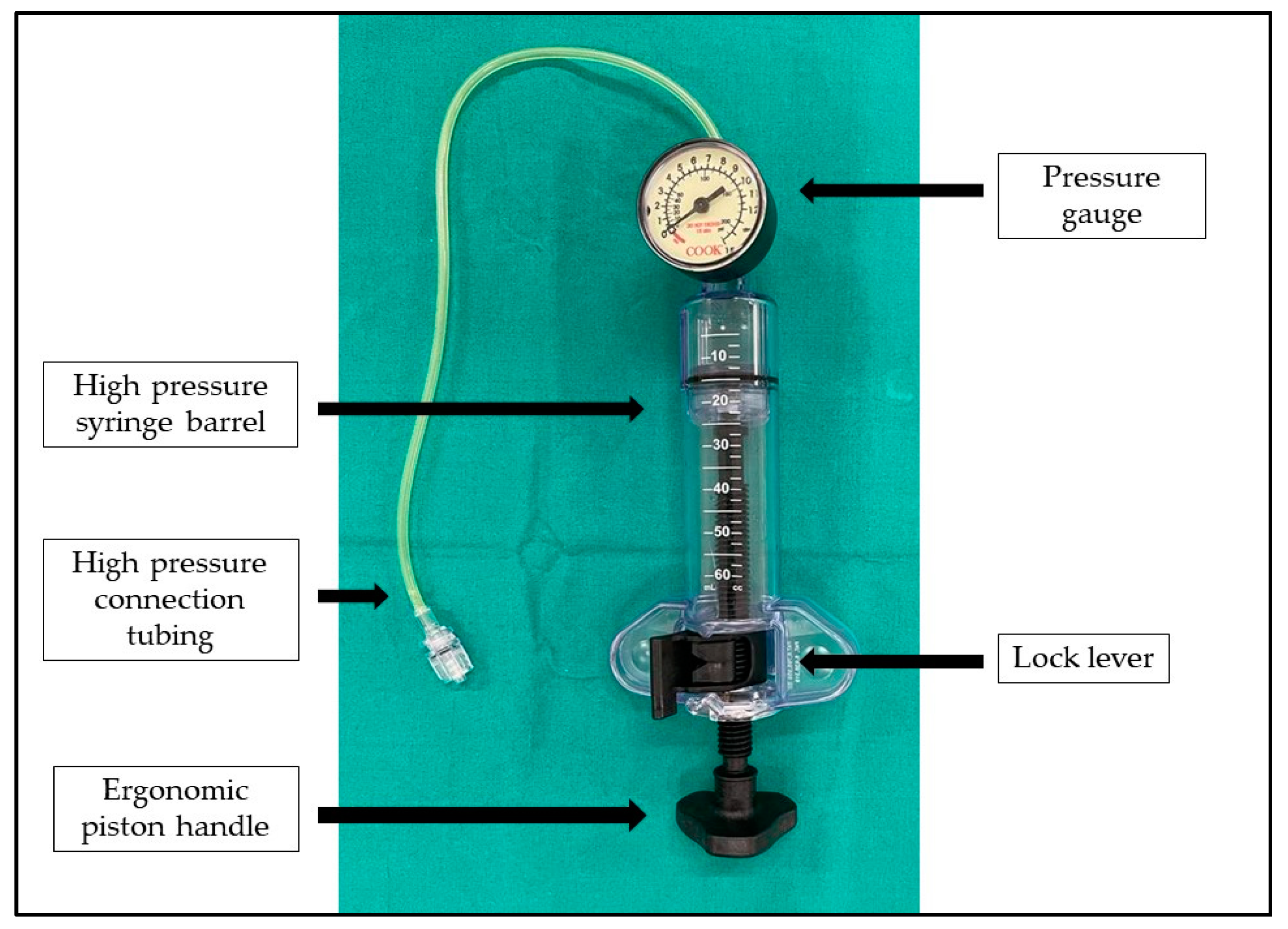
- During sialendoscopy, a continuous rinsing of the duct is necessary to achieve dilatation of the duct and an adequate visualization of the lumen.
- Manual irrigation with medical syringe is sometimes tiring and unwarranted.
- The adapted balloon inflation device permits a non-laborious duct irrigation and dilation under pression control in any patient who undergoes sialendoscopy.
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katz, P. Endoscopie des glandes salivaires [Endoscopy of the salivary glands]. Ann. Radiol. 1991, 34, 110–113. (In French) [Google Scholar] [PubMed]
- Gillespie, M.B.; Intaphan, J.; Nguyen, S.A. Endoscopic-assisted management of chronic sialadenitis. Head Neck. 2011, 33, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Benazzo, M.; Capaccio, P.; De Campora, L.; De Vincentiis, M.; Fusconi, M.; Martellucci, S.; Paludetti, G.; Pasquini, E.; Puxeddu, R.; et al. Sialoendoscopy: State of the art, challenges and further perspectives. Round Table, 101(st) SIO National Congress, Catania 2014. Acta Otorhinolaryngol. Ital. 2015, 35, 217–233. [Google Scholar] [PubMed]
- Koch, M.; Zenk, J.; Bozzato, A.; Bumm, K.; Iro, H. Sialoscopy in cases of unclear swelling of the major salivary glands. Otolaryngol. Head Neck Surg. 2005, 133, 863–868. [Google Scholar] [CrossRef] [PubMed]
- Colella, G.; Lo Giudice, G.; De Luca, R.; Troiano, A.; Lo Faro, C.; Santillo, V.; Tartaro, G. Interventional sialendoscopy in parotidomegaly related to eating disorders. J. Eat. Disord. 2021, 9, 25. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, G.; Marra, P.M.; Colella, C.; Itro, A.; Tartaro, G.; Colella, G. Salivary Gland Disorders in Pediatric Patients: A 20 Years’ Experience. Appl. Sci. 2022, 12, 1999. [Google Scholar] [CrossRef]
- Fusconi, M.; Meliante, P.G.; Pagliuca, G.; Greco, A.; de Vincentiis, M.; Polimeni, A.; Musy, I.; Candelori, F.; Gallo, A. Interpretation of the mucous plug through sialendoscopy. Oral Dis. 2022, 28, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Marchal, F.; Dulguerov, P.; Becker, M.; Barki, G.; Disant, F.; Lehmann, W. Submandibular diagnostic and interventional sialendoscopy: New procedure for ductal disorders. Ann. Otol. Rhinol. Laryngol. 2002, 111, 27–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahlieli, O.; Baruchin, A.M. Long-term experience with endoscopic diagnosis and treatment of salivary gland inflammatory diseases. Laryngoscope 2000, 110, 988–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, A.; Capaccio, P.; Benazzo, M.; De Campora, L.; De Vincentiis, M.; Farneti, P.; Fusconi, M.; Gaffuri, M.; Lo Russo, F.; Martellucci, S.; et al. Outcomes of interventional sialendoscopy for obstructive salivary gland disorders: An Italian multicentre study. Acta Otorhinolaryngol. Ital. 2016, 36, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Martellucci, S.; Fusconi, M.; Pagliuca, G.; Greco, A.; De Virgilio, A.; De Vincentiis, M. Sialendoscopic management of autoimmune sialadenitis: A review of literature. Acta Otorhinolaryngol. Ital. 2017, 37, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Nahlieli, O.; Nazarian, Y. Sialadenitis following radioiodine therapy—A new diagnostic and treatment modality. Oral Dis. 2006, 12, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Gallo, A.; Clemenzi, V.; Stolfa, A.; Pagliuca, G.; Benedetti, F.M.N.; Caporale, C.; del Giudice, A.M.; Maino, T.; de Robertis, V.; Cariti, F.; et al. The secretory senescence of the oro-pharyngo-laryngeal tract. J. Gerontol. Geriatr. 2020, 68, 69–76. [Google Scholar] [CrossRef]
- Shacham, R.; Droma, E.B.; London, D.; Bar, T.; Nahlieli, O. Long-term experience with endoscopic diagnosis and treatment of juvenile recurrent parotitis. J. Oral Maxillofac. Surg. 2009, 67, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Ardekian, L.; Shamir, D.; Trabelsi, M.; Peled, M. Chronic obstructive parotitis due to strictures of Stenson’s duct--our treatment experience with sialoendoscopy. J. Oral Maxillofac. Surg. 2010, 68, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Luers, J.C.; Ortmann, M.; Beutner, D.; Hüttenbrink, K.B. Intraductal pressure during sialendoscopy. J. Laryngol. Otol. 2014, 128, 897–901. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagliuca, G.; Clemenzi, V.; Stolfa, A.; Martellucci, S.; Greco, A.; de Vincentiis, M.; Gallo, A. Use of Irrigation Device for Duct Dilatation during Sialendoscopy. Int. J. Environ. Res. Public Health 2022, 19, 14830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214830
Pagliuca G, Clemenzi V, Stolfa A, Martellucci S, Greco A, de Vincentiis M, Gallo A. Use of Irrigation Device for Duct Dilatation during Sialendoscopy. International Journal of Environmental Research and Public Health. 2022; 19(22):14830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214830
Chicago/Turabian StylePagliuca, Giulio, Veronica Clemenzi, Andrea Stolfa, Salvatore Martellucci, Antonio Greco, Marco de Vincentiis, and Andrea Gallo. 2022. "Use of Irrigation Device for Duct Dilatation during Sialendoscopy" International Journal of Environmental Research and Public Health 19, no. 22: 14830. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192214830