4.1. Literature Analysis
This research identified important findings in understanding how paternal attitudes, perceptions over couple satisfaction, intimacy problems, and stress levels correlate when there is a child with cystic fibrosis who is born inside the family. Among the significant findings in these respondents, it was observed that they engaged less frequently in sexual activity. It was also observed that the cases group had a significantly higher proportion of smokers. Although smoking parents are more likely to have an unhealthy child, and smoking was proven to cause CFTR dysfunction that is involved in cystic fibrosis, no direct causality was linked between paternal smoking and cystic fibrosis in children [
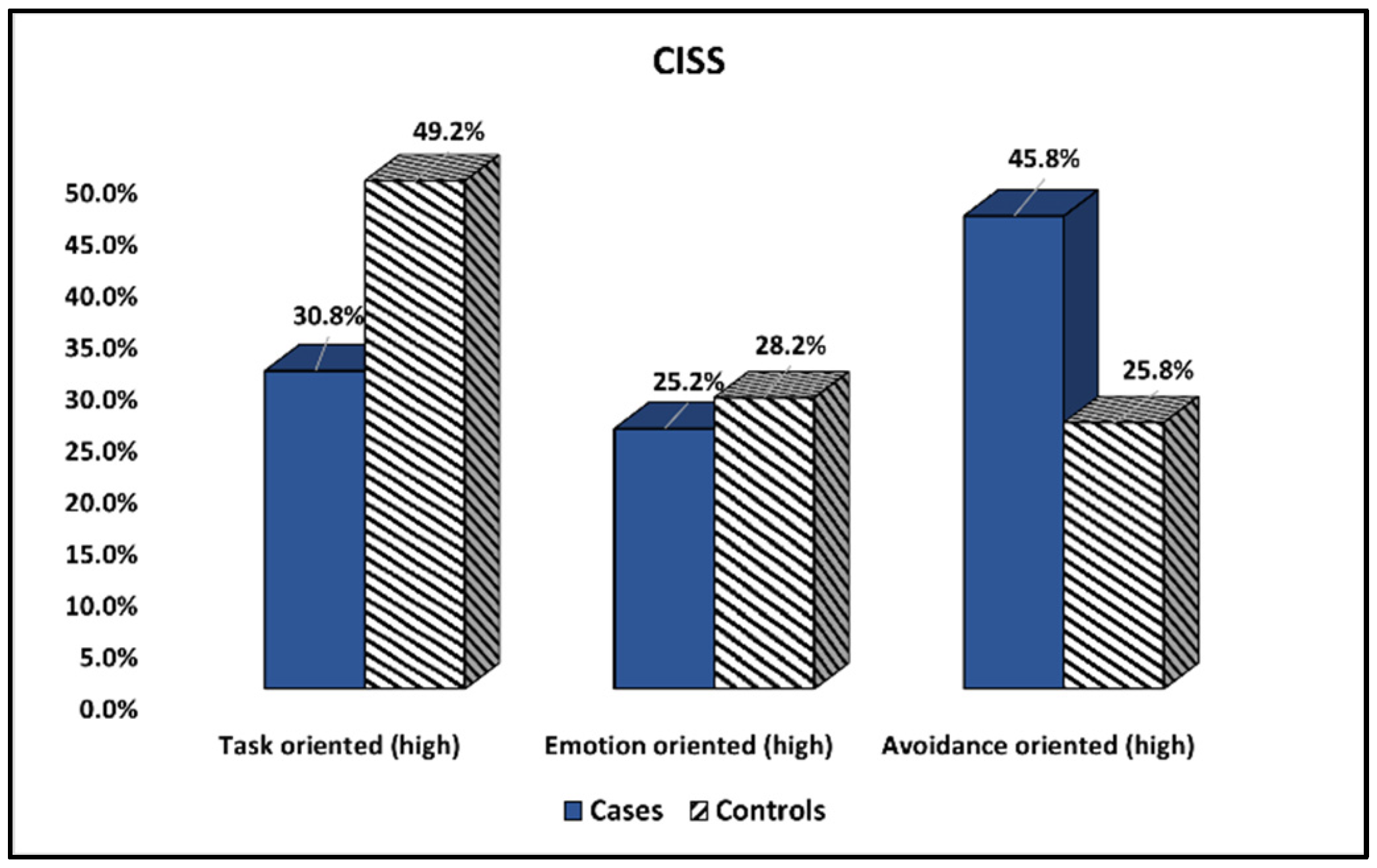
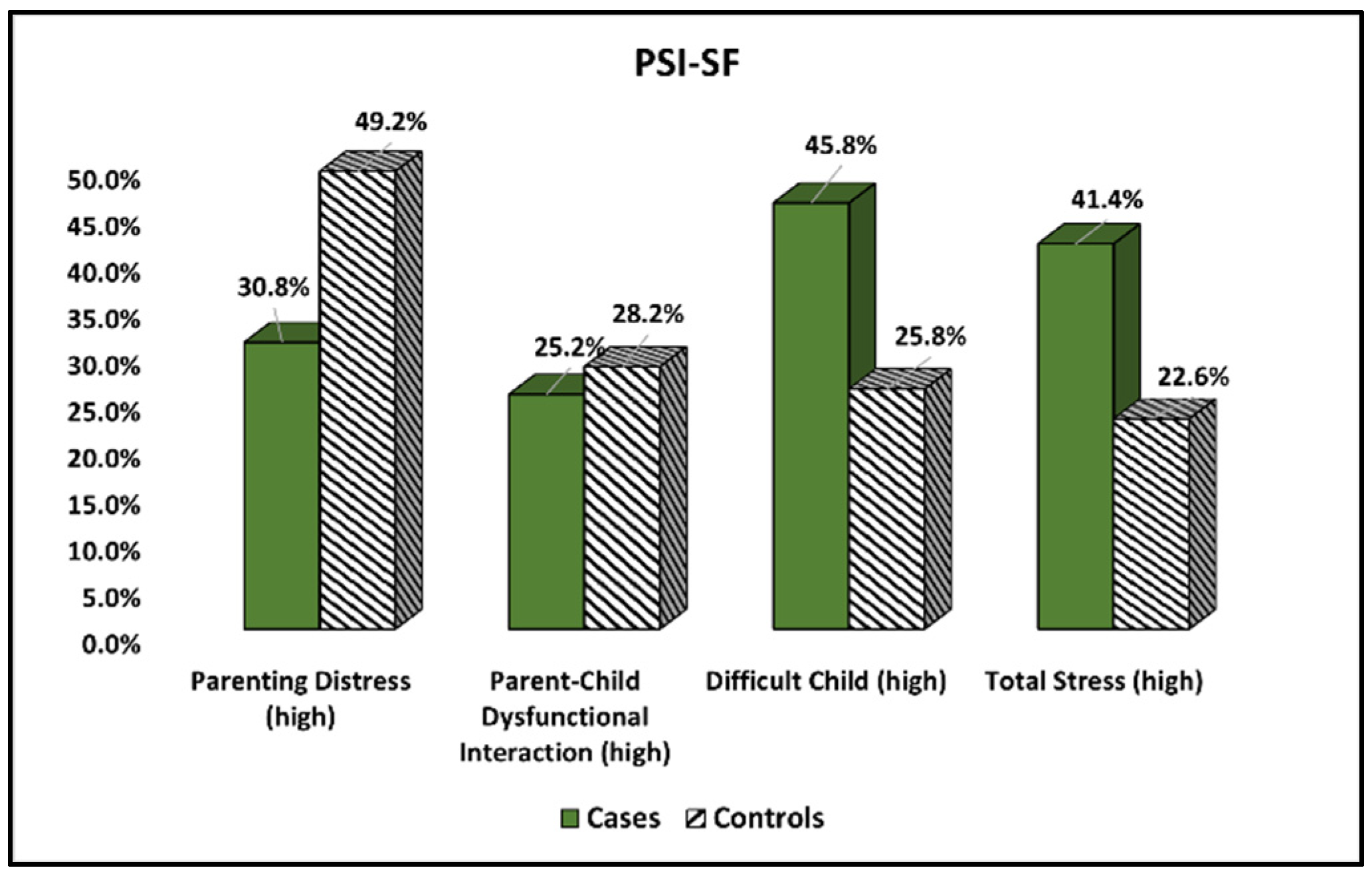
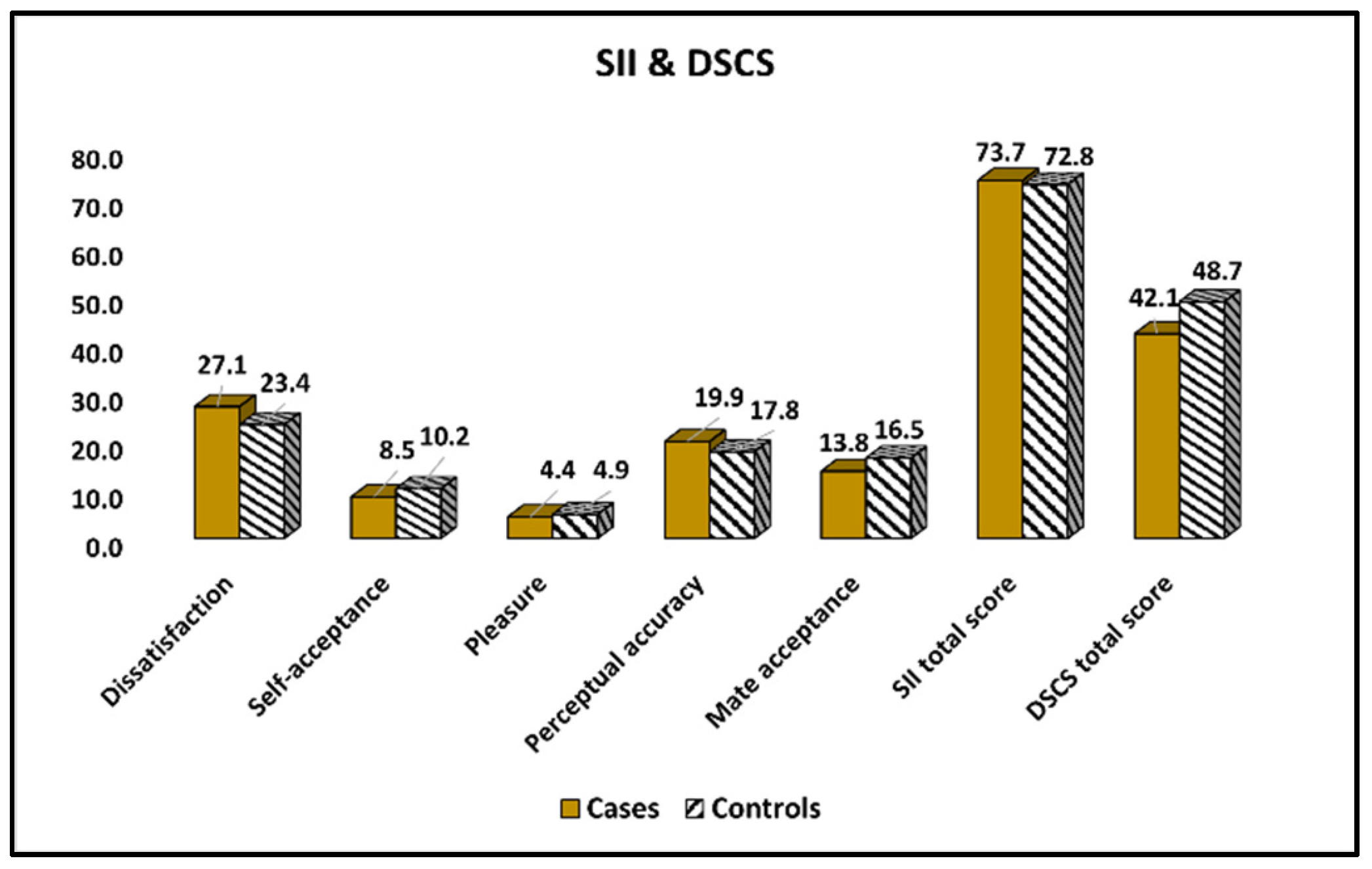
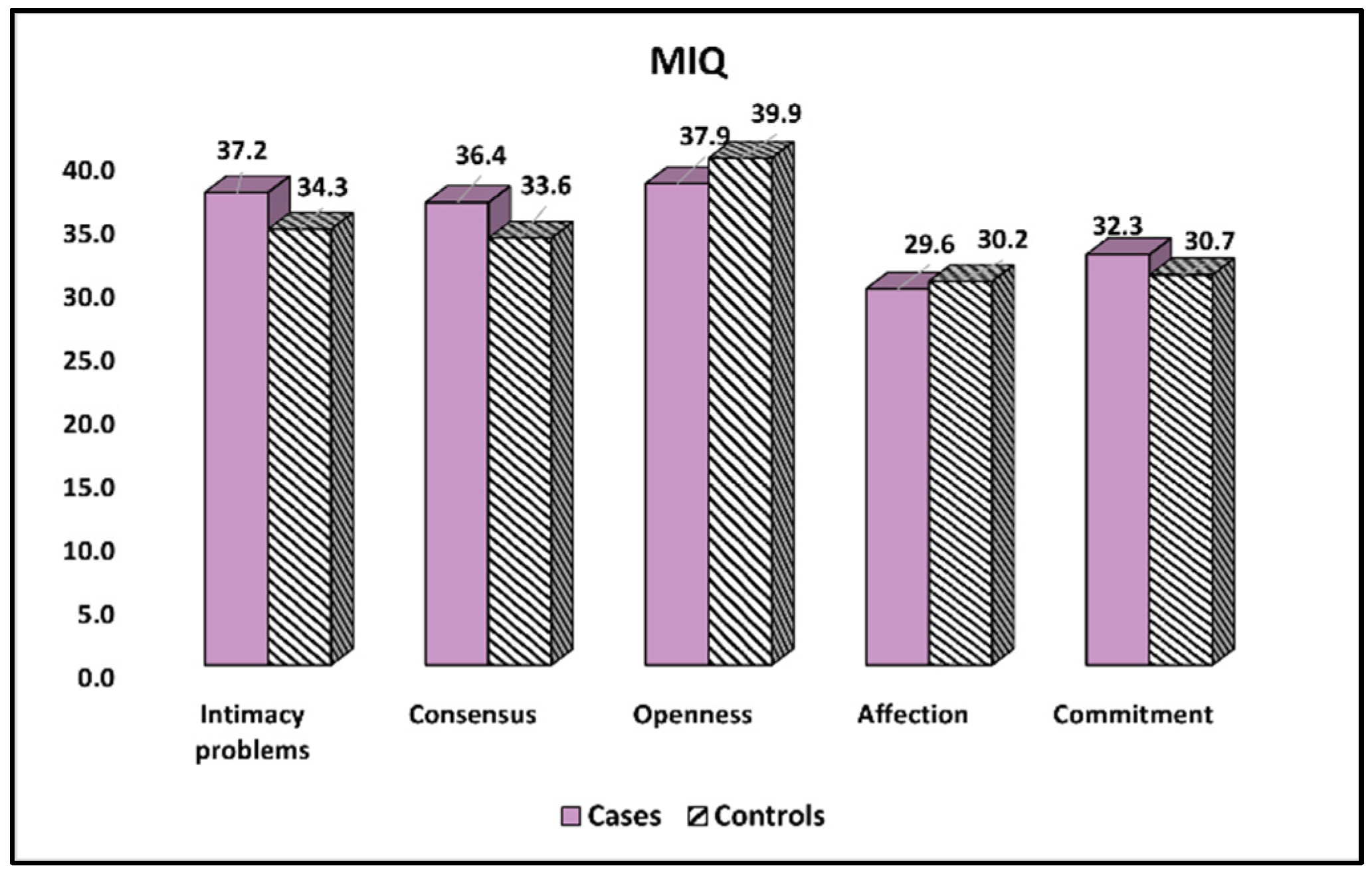
22]. Additionally, a higher proportion of them reported marital distress and inhibited sexual desire, all in association with a higher number of men taking psychiatric medication. More than 40% of all respondents declared high levels of general stress and parenting distress, while the most frequently used coping mechanism for stress was avoidance-oriented. Other important findings were the high levels of dissatisfaction and lower levels of marital quality on the SII scale, equivalent to the intimacy problems on the MIQ scale.
Parenting is inextricably linked to the presence of stress resulting from a variety of normal and abnormal life situations. Parenting a child with a disability may bring particular obstacles to the family’s ability to function, despite the fact that the majority of children cause mothers and fathers to experience stress [
23]. It is estimated that 17% of children under the age of 18 in the United States have developmental impairments [
24]. The authors describe fathers of children with disabilities as reporting considerably higher levels of parental stress than parents of healthy children [
25]. Families with children who have educational challenges generally feel elevated levels of stress, particularly in regard to parental obligations. In a matched sample comparing parents of normally developing children with parents of children with Down syndrome, it was observed that parents of children with Down syndrome reported greater levels of parent-related stress, challenges in perceived parenting competence, health concerns, and parental depression [
26].
Similarly, in the present research, the percentage of fathers with children suffering from cystic fibrosis who self-reported marital difficulty was considerably greater (15.0% vs. 6.5%), with an odds ratio (OR) of 2.54, suggesting a 2.54-fold increased chance of marital distress in this group. Additionally, 5.9% more fathers in the cases group reported using psychiatric medication. The estimated odds ratio was 4.92, showing a 4.92 times greater risk for males in this group to be on psychiatric medication, which may be related to a higher frequency of depression among parents of children with chronic conditions. Lastly, it was observed that the same respondents in the cases group had a 10.6% higher inhibition of sexual desire than fathers in the control group, with a 2.02 times higher odds ratio (OR = 2.02), although this may be partially attributable to the use of psychiatric medications such as selective serotonin reuptake inhibitors. Despite the fact that having a child born with a handicap is difficult for everyone concerned, little is known about the culture and experiences of men who have a child with a disability, since much prior study has concentrated on the mothers’ perspectives [
27]. While studies often see dads as peripheral or external system members, the notion that the duties of fathers of children with disabilities are restricted to assisting the mother is being contested. Although not all fathers saw parenting a child with impairments as difficult, those who did assessed their children as less adaptive and acceptable, as well as more demanding, irritable, and distracted. In addition to greater melancholy and lower connection to their children, fathers with high stress perceived less competence as a parent, experienced social isolation, and had poor health outcomes [
28].
Family stress theory-based research examining the experiences of parents parenting a child with a developmental handicap revealed that the child’s traits predicted just 8% of the stress experienced by fathers. The factors connected to family resources contributed to 33% of paternal stress, whereas the characterization and interpretation, of the issue, accounted for 37% [
29]. The most significant predictor of parental stress was a negative situational description. Particularly for dads, this negative connotation was related to the child’s social acceptability. Thus, the observed views of other individuals affected the father’s assessment of an unhealthy child as a burden or disaster. To some authors, it seems that men were more affected than mothers by the unfavorable opinions of others and depended more on their spouse’s support and their own ability to cope [
30].
Thus, parents of children with a chronic disease who are confronted with challenging parenting circumstances are less likely to seek emotional assistance from others, as described in the literature. They also seek moral support, friendship, compassion, and understanding less often than parents of healthy developing children [
31]. This pattern would also result in a decrease in the intensity of avoidance methods since the primary emphasis is on childcare. These results are significant because they may explain the correlation between depression and social disengagement among parents of children with disabilities. Indeed, social support is a protective factor against emotional issues and poor self-perceived life satisfaction, and it might be a crucial aspect in the development of successful support programs for this population of parents. Fascinatingly, parents did not exhibit the major tactics associated with obtaining emotional support from religion, which are more prevalent among parents of normal children. In this regard, parents may see religious coping techniques as maladaptive. Other investigations, however, show that religious support is favorable. In this regard, the findings of prior research involving children with various types of disabilities are inconsistent [
32].
Regarding coping techniques, our study identified the avoidance-oriented mechanism as the most prevalent among the affected fathers. This is in accordance with one research that found substantial differences between parents of children with developmental disabilities and parents of children without developmental disabilities for one of three coping strategies [
33]. Less often did parents of children with developmental impairments use the avoidance-oriented and emotional support styles. The task-oriented attitude and tactics were prevalent across both parent groups. In stressful circumstances associated with childrearing, parents of children with developmental impairments do not rely on emotional support and religion as often as parents of healthy children.
4.2. Strengths and Limitations
Even though the present research complied with the very minimal standards for sample size requirements, there are some weak points of the study that need to be pointed out. First, the cases and control samples were not matched, therefore it was not possible to control for confounding factors. Thus, a matched sample could provide more accurate results. Second, the cross-sectional design might be considered a limiting feature since it does not provide a compelling evaluation and assessment in time of the stress levels and intimacy problems experienced by the men involved. This prevents the levels of stress and couple satisfaction from being determined in an accurate manner since the surveys measure only the participants’ answers at one point in time. As a third limitation, the use of questionnaires may result in a high subjectivity index from all of the participants who consented to fill them out, which can lead to several biases in the data collected. Another possible limitation of the study is the lack of a main outcome; therefore, causality cannot be determined from the studied survey scores as predictors. Further limitations comprise the lack of comparison with the maternal side, the bias of reporting intimacy and intimate questionnaire responses, as well as there being no experimental setting or controlled matching to interpret findings in a clearer manner. In conclusion, the findings of the present research can only be generalized to the population that was investigated because of the possibility that some unique aspects of the population, such as religion and culture, would have a particular effect on the findings.

 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}