
A Global Survey of Ethnic Indian Women Living with Polycystic Ovary Syndrome: Co-Morbidities, Concerns, Diagnosis Experiences, Quality of Life, and Use of Treatment Methods
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Ethical Approval and Consent
2.2. Study Design and Research Instrument
2.3. Setting and Recruitment
2.4. Eligibility
3. Data Analysis
4. Results
4.1. Sample Characteristics
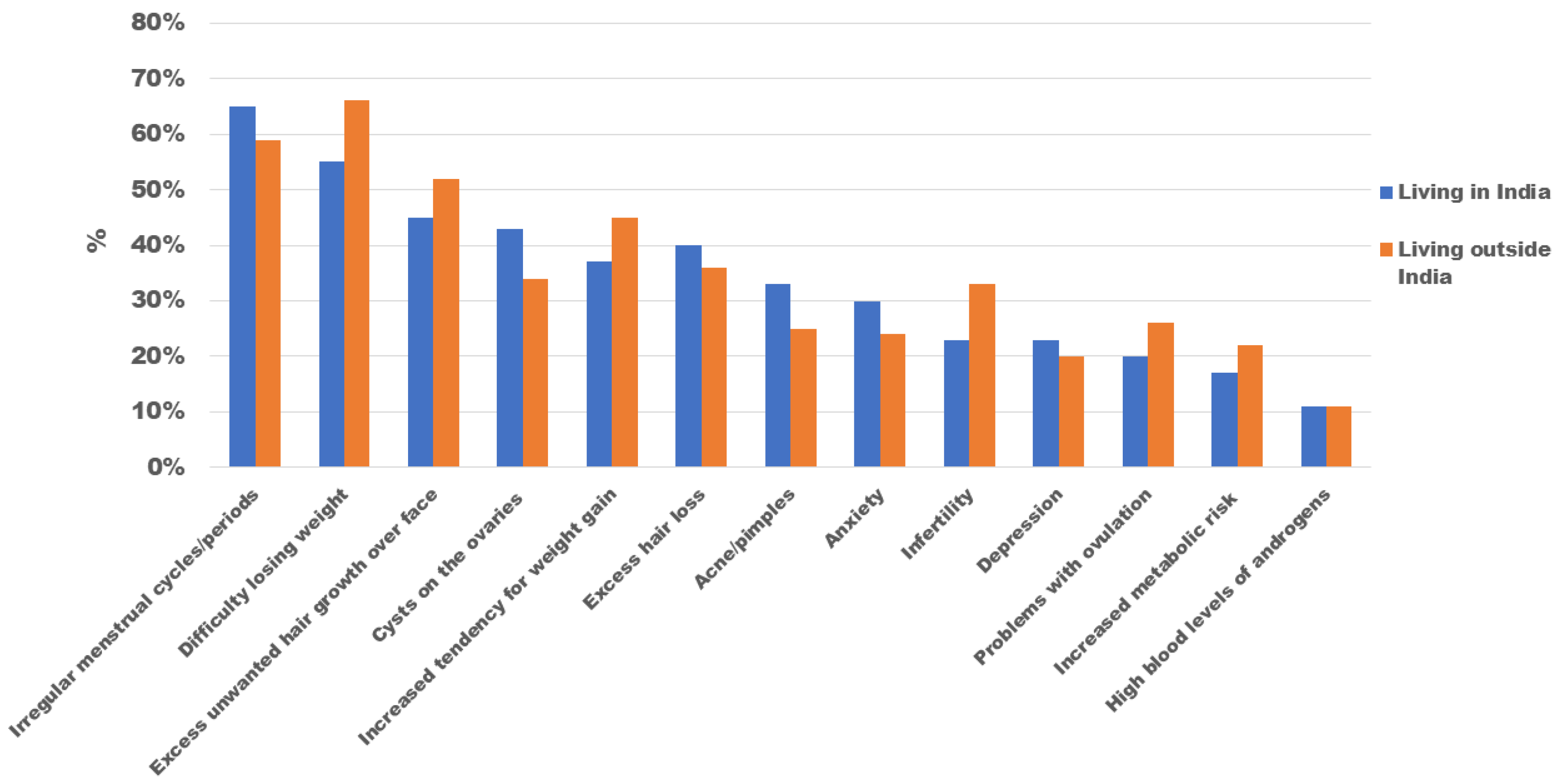
4.2. Co-Morbidities Associated with PCOS
4.3. Key Concerns of PCOS
4.4. Experience with the Onset of PCOS Symptoms and Diagnosis
4.5. Provision of Information and Satisfaction with the Information Provided at the Time of Diagnosis
4.5.1. Provision of Information and Level of Satisfaction with the Country of Residence
4.5.2. Provision of Information and Level of Satisfaction with Delay in Seeking Help
4.5.3. Provision of Information and Level of Satisfaction with Delay in Diagnosis
4.6. Health Professionals and Treatment Methods
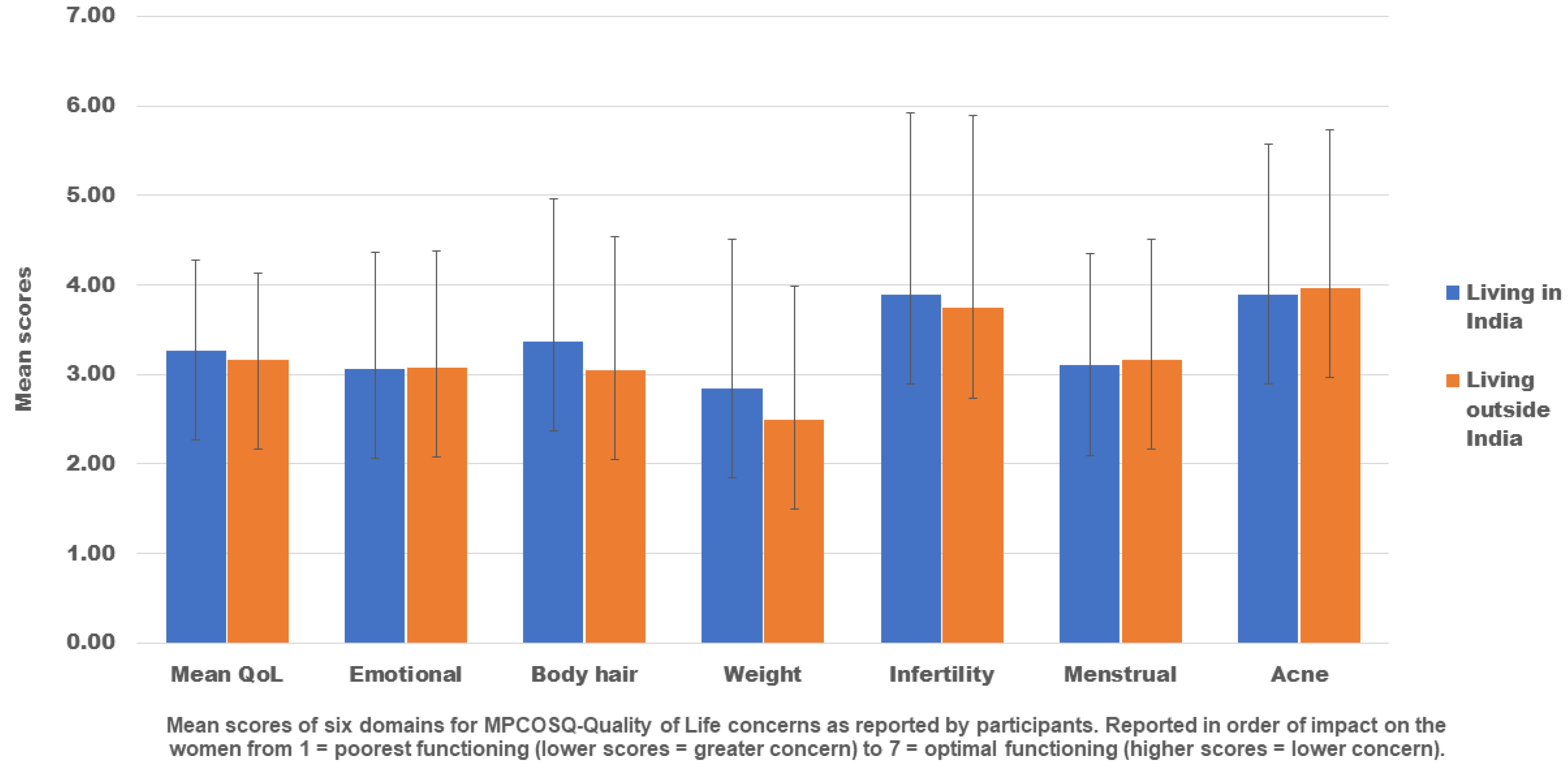
4.7. Health-Related Quality of Life Using MPCOSQ
5. Discussion
6. Strengths and Limitations
7. Conclusions
8. Future Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- ESHRE, T.R.; Group, A.-S.P.C.W. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil. Steril. 2004, 81, 19–25. [Google Scholar]
- Balen, A.H.; Laven, J.S.; Tan, S.L.; Dewailly, D. Ultrasound assessment of the polycystic ovary: International consensus definitions. Hum. Reprod. Update 2003, 9, 505–514. [Google Scholar] [CrossRef]
- Kakoly, N.; Khomami, M.; Joham, A.; Cooray, S.; Misso, M.; Norman, R.; Harrison, C.; Ranasinha, S.; Teede, H.; Moran, L. Ethnicity, obesity and the prevalence of impaired glucose tolerance and type 2 diabetes in PCOS: A systematic review and meta-regression. Hum. Reprod. Update 2018, 24, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Wekker, V.; Van Dammen, L.; Koning, A.; Heida, K.; Painter, R.; Limpens, J.; Laven, J.; Roeters van Lennep, J.; Roseboom, T.; Hoek, A. Long-term cardiometabolic disease risk in women with PCOS: A systematic review and meta-analysis. Hum. Reprod. Update 2020, 26, 942–960. [Google Scholar] [CrossRef] [PubMed]
- Bahri Khomami, M.; Moran, L.J.; Kenny, L.; Grieger, J.A.; Myers, J.; Poston, L.; McCowan, L.; Walker, J.; Dekker, G.; Norman, R. Lifestyle and pregnancy complications in polycystic ovary syndrome: The SCOPE cohort study. Clin. Endocrinol. 2019, 90, 814–821. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef] [PubMed]
- Barry, J.A. Exploration of Biological Causes of Psychological Problems in Polycystic Ovary Syndrome (PCOS); City University London: London, UK, 2011. [Google Scholar]
- Pirotta, S.; Barillaro, M.; Brennan, L.; Grassi, A.; Jeanes, Y.M.; Joham, A.E.; Kulkarni, J.; Couch, L.M.; Lim, S.S.; Moran, L.J. Disordered eating behaviours and eating disorders in women in Australia with and without polycystic ovary syndrome: A cross-sectional study. J. Clin. Med. 2019, 8, 1682. [Google Scholar] [CrossRef] [PubMed]
- Ding, T.; Hardiman, P.J.; Petersen, I.; Wang, F.-F.; Qu, F.; Baio, G.J.O. The prevalence of polycystic ovary syndrome in reproductive-aged women of different ethnicity: A systematic review and meta-analysis. Oncotarget 2017, 8, 96351. [Google Scholar] [CrossRef]
- Louwers, Y.; Lao, O.; Kayser, M. Inferred genetic ancestry versus reported ethnicity in polycystic ovary syndrome (PCOS). In Human Reproduction; Oxford University Press: Oxford, England, 2013. [Google Scholar]
- Azziz, R.; Ezeh, U.; Pall, M.; Dumesic, D.; Goodarzi, M. Effect of race on the metabolic dysfunction of Polycystic Ovary Syndrome (PCOS): Comparing African-American (AA) and Non-Hispanic White (NHW) patients. In Endocrine Reviews; Endocrine Society: Washington, DC, USA, 2010. [Google Scholar]
- Belenkaia, L.V.; Lazareva, L.M.; Walker, W.; Lizneva, D.V.; Suturina, L.V. Criteria, phenotypes and prevalence of polycystic ovary syndrome. Minerva Ginecol 2019, 71, 211–223. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Qiao, J. Ethnic differences in the phenotypic expression of polycystic ovary syndrome. Steroids 2013, 78, 755–760. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Choi, Y.M. Phenotype and genotype of polycystic ovary syndrome in Asia: Ethnic differences. J. Obstet. Gynaecol. Res. 2019, 45, 2330–2337. [Google Scholar] [CrossRef] [PubMed]
- Sendur, S.N.; Yildiz, B.O. Influence of ethnicity on different aspects of polycystic ovary syndrome: A systematic review. Reprod. BioMedicine Online 2021, 42, 799–818. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.L.; Kar, S.; Vanky, E.; Morin-Papunen, L.; Piltonen, T.; Puurunen, J.; Tapanainen, J.S.; Maciel, G.A.R.; Hayashida, S.A.Y.; Soares, J.M., Jr. Racial and ethnic differences in the prevalence of metabolic syndrome and its components of metabolic syndrome in women with polycystic ovary syndrome: A regional cross-sectional study. Am. J. Obstet. Gynecol. 2017, 217, 189.e181–189.e188. [Google Scholar] [CrossRef]
- Dadachanji, R.; Sawant, D.; Patil, A.; Mukherjee, S. Replication study of THADA rs13429458 variant with PCOS susceptibility and its related traits in Indian women. Gynecol. Endocrinol. 2021, 37, 716–720. [Google Scholar] [CrossRef] [PubMed]
- Allahbadia, G.N.; Merchant, R. Polycystic ovary syndrome in the Indian Subcontinent. Semin. Reprod. Med. 2008, 26, 22–34. [Google Scholar] [CrossRef] [PubMed]
- Tillin, T.; Hughes, A.D.; Godsland, I.F.; Whincup, P.; Forouhi, N.G.; Welsh, P.; Sattar, N.; McKeigue, P.M.; Chaturvedi, N. Insulin resistance and truncal obesity as important determinants of the greater incidence of diabetes in Indian Asians and African Caribbeans compared with Europeans: The Southall And Brent REvisited (SABRE) cohort. Diabetes Care 2013, 36, 383–393. [Google Scholar] [CrossRef] [PubMed]
- Nations, U. World Migration Report 2020; International Organization for Migration: Geneva, Switzerland, 2019; p. 3. [Google Scholar]
- Gibson-Helm, M.E.; Lucas, I.M.; Boyle, J.A.; Teede, H.J. Women’s experiences of polycystic ovary syndrome diagnosis. Fam. Pract. 2014, 31, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Gibson-Helm, M.; Teede, H.; Dunaif, A.; Dokras, A. Delayed diagnosis and a lack of information associated with dissatisfaction in women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2017, 102, 604–612. [Google Scholar] [CrossRef]
- Kaur, I.; Suri, V.; Rana, S.V.; Singh, A. Treatment pathways traversed by polycystic ovary syndrome (PCOS) patients: A mixed-method study. PLoS ONE 2021, 16, e0255830. [Google Scholar] [CrossRef] [PubMed]
- Pathak, G.S. “Supportive” Masculinities and Polycystic Ovary Syndrome: Changing Gender Relations in Contemporary Urban India. In Reconceiving Muslim Men; Berghahn Books: New York, NY, USA, 2018. [Google Scholar]
- Sharma, S.; Mishra, A.J. Tabooed disease in alienated bodies: A study of women suffering from Polycystic Ovary Syndrome (PCOS). Clin. Epidemiol. Glob. Health 2018, 6, 130–136. [Google Scholar] [CrossRef]
- Widge, A. Seeking conception: Experiences of urban Indian women with in vitro fertilisation. Patient Educ. Couns. 2005, 59, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Gill, H.; Tiwari, P.; Dabadghao, P. Prevalence of polycystic ovary syndrome in young women from North India: A Community-based study. Indian J. Endocrinol. Metab. 2012, 16, 389–392. [Google Scholar] [CrossRef]
- Joshi, B.; Mukherjee, S.; Patil, A.; Purandare, A.; Chauhan, S.; Vaidya, R. A cross-sectional study of polycystic ovarian syndrome among adolescent and young girls in Mumbai, India. Indian J. Endocrinol. Metab. 2014, 18, 317–324. [Google Scholar] [CrossRef]
- Choudhary, A.; Jain, S.; Chaudhari, P. Prevalence and symptomatology of polycystic ovarian syndrome in Indian women: Is there a rising incidence? Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 4971–4976. [Google Scholar] [CrossRef]
- Cronin, L.; Guyatt, G.; Griffith, L.; Wong, E.; Azziz, R.; Futterweit, W.; Cook, D.; Dunaif, A. Development of a health-related quality-of-life questionnaire (PCOSQ) for women with polycystic ovary syndrome (PCOS). J. Clin. Endocrinol. Metab. 1998, 83, 1976–1987. [Google Scholar] [PubMed]
- Barnard, L.; Ferriday, D.; Guenther, N.; Strauss, B.; Balen, A.; Dye, L. Quality of life and psychological well being in polycystic ovary syndrome. Hum. Reprod. 2007, 22, 2279–2286. [Google Scholar] [CrossRef] [PubMed]
- Misra, A.; Chowbey, P.; Makkar, B.; Vikram, N.; Wasir, J.; Chadha, D.; Joshi, S.R.; Sadikot, S.; Gupta, R.; Gulati, S. Consensus statement for diagnosis of obesity, abdominal obesity and the metabolic syndrome for Asian Indians and recommendations for physical activity, medical and surgical management. Japi 2009, 57, 163–170. [Google Scholar] [PubMed]
- Jadhav, A.; Pramod, D.; Ramanathan, K. Comparison of performance of data imputation methods for numeric dataset. Appl. Artif. Intell. 2019, 33, 913–933. [Google Scholar] [CrossRef]
- IBM Corp, N. IBM SPSS Statistics for Windows; IBM Corp.: Armonk, NY, USA, 2021. [Google Scholar]
- Mani, H.; Davies, M.J.; Bodicoat, D.H.; Levy, M.J.; Gray, L.J.; Howlett, T.A.; Khunti, K. Clinical characteristics of polycystic ovary syndrome: Investigating differences in White and South Asian women. Clin. Endocrinol. 2015, 83, 542–549. [Google Scholar] [CrossRef]
- Wijeyaratne, C.N.; Balen, A.H.; Barth, J.H.; Belchetz, P.E. Clinical manifestations and insulin resistance (IR) in polycystic ovary syndrome (PCOS) among South Asians and Caucasians: Is there a difference? Clin. Endocrinol. 2002, 57, 343–350. [Google Scholar] [CrossRef]
- Conway, G.; Dewailly, D.; Diamanti-Kandarakis, E.; Escobar-Morreale, H.F.; Franks, S.; Gambineri, A.; Kelestimur, F.; Macut, D.; Micic, D.; Pasquali, R. European survey of diagnosis and management of the polycystic ovary syndrome: Results of the ESE PCOS Special Interest Group’s Questionnaire. Eur. J. Endocrinol. 2014, 171, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Bronstein, J.; Tawdekar, S.; Liu, Y.; Pawelczak, M.; David, R.; Shah, B. Age of onset of polycystic ovarian syndrome in girls may be earlier than previously thought. J. Pediatric Adolesc. Gynecol. 2011, 24, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Trent, M.E.; Rich, M.; Austin, S.B.; Gordon, C.M. Quality of life in adolescent girls with polycystic ovary syndrome. Arch. Pediatrics Adolesc. Med. 2002, 156, 556–560. [Google Scholar] [CrossRef] [PubMed]
- Nair, M.; Pappachan, P.; Balakrishnan, S.; Leena, M.; George, B.; Russell, P.S. Menstrual irregularity and poly cystic ovarian syndrome among adolescent girls—a 2 year follow-up study. Indian J. Pediatrics 2012, 79, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Capozzi, A.; Scambia, G.; Lello, S. Polycystic ovary syndrome (PCOS) and adolescence: How can we manage it? Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 250, 235–240. [Google Scholar] [CrossRef]
- Pharmaceuticals, E. Indian Women’s Health Report 2021. Available online: https://unconditionyourself.com/wp-content/uploads/2021/12/UY-Indian-Womens-Health-Report-2021-Final.pdf (accessed on 21 July 2022).
- Jain, T.; Negris, O.; Brown, D.; Galic, I.; Salimgaraev, R.; Zhaunova, L. Characterization of polycystic ovary syndrome among Flo app users around the world. Reprod. Biol. Endocrinol. 2021, 19, 36. [Google Scholar] [CrossRef]
- Solomon, C.G.; Hu, F.B.; Dunaif, A.; Rich-Edwards, J.; Willett, W.C.; Hunter, D.J.; Colditz, G.A.; Speizer, F.E.; Manson, J.E. Long or highly irregular menstrual cycles as a marker for risk of type 2 diabetes mellitus. JAMA 2001, 286, 2421–2426. [Google Scholar] [CrossRef] [PubMed]
- Petermann, T.; Angel, B.; Maliqueo, M.; Carvajal, F.; Santos, J.; Pérez-Bravo, F. Prevalence of Type II diabetes mellitus and insulin resistance in parents of women with polycystic ovary syndrome. Diabetologia 2002, 45, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, B.O.; Yarali, H.; Oguz, H.; Bayraktar, M. Glucose intolerance, insulin resistance, and hyperandrogenemia in first degree relatives of women with polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2003, 88, 2031–2036. [Google Scholar] [CrossRef] [PubMed]
- Kahsar-Miller, M.D.; Nixon, C.; Boots, L.R.; Go, R.C.; Azziz, R.J.F. Prevalence of polycystic ovary syndrome (PCOS) in first-degree relatives of patients with PCOS. Fertil. Steril. 2001, 75, 53–58. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Boyle, J.A.; Garad, R.M.; McAllister, V.; Downes, L.; Gibson-Helm, M.; Hart, R.J.; Rombauts, L.; Moran, L. Translation and implementation of the Australian-led PCOS guideline: Clinical summary and translation resources from the International Evidence-based Guideline for the Assessment and management of polycystic ovary syndrome. Med. J. Aust. 2018, 209, S3–S8. [Google Scholar] [CrossRef] [PubMed]
- Ching, H.; Burke, V.; Stuckey, B. Quality of life and psychological morbidity in women with polycystic ovary syndrome: Body mass index, age and the provision of patient information are significant modifiers. Clin. Endocrinol. 2007, 66, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Colwell, K.; Lujan, M.E.; Lawson, K.L.; Pierson, R.A.; Chizen, D.R. Women’s perceptions of polycystic ovary syndrome following participation in a clinical research study: Implications for knowledge, feelings, and daily health practices. J. Obstet. Gynaecol. Can. 2010, 32, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Chiu, W.-L.; Kuczynska-Burggraf, M.; Gibson-Helm, M.; Teede, H.J.; Vincent, A.; Boyle, J.A. What can you find about polycystic ovary syndrome (PCOS) online? Assessing online information on PCOS: Quality, content, and user-friendliness. In Seminars in Reproductive Medicine; Thieme Medical Publishers: New York, NY, USA, 2018. [Google Scholar]
- Htet, T.T.; Cassar, S.; Kuczynska-Burggraf, M.; Boyle, J.; Gibson-Helm, M.; Stepto, N.; Moran, L. The accuracy of information for lifestyle management on websites for the management of PCOS. Clin. Endocrinol. 2017, 86, 47. [Google Scholar]
- Shrivastava, S.R.; Shrivastava, P.S.; Ramasamy, J. Mainstreaming of Ayurveda, Yoga, Naturopathy, Unani, Siddha, and Homeopathy with the health care delivery system in India. J. Tradit. Complementary Med. 2015, 5, 116–118. [Google Scholar] [CrossRef] [PubMed]
- Schmid, J.; Kirchengast, S.; Vytiska-Binstorfer, E.; Huber, J. Infertility caused by PCOS--health-related quality of life among Austrian and Moslem immigrant women in Austria. Hum. Reprod. 2004, 19, 2251–2257. [Google Scholar] [CrossRef]
- Jones, G.L.; Palep-Singh, M.; Ledger, W.L.; Balen, A.H.; Jenkinson, C.; Campbell, M.J.; Lashen, H. Do South Asian women with PCOS have poorer health-related quality of life than Caucasian women with PCOS? A comparative cross-sectional study. Health Qual. Life Outcomes 2010, 8, 18. [Google Scholar] [CrossRef]
- McCook, J.G.; Reame, N.E.; Thatcher, S.S. Health-related quality of life issues in women with polycystic ovary syndrome. J. Obstet. Gynecol. Neonatal Nurs. 2005, 34, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Alur-Gupta, S.; Lee, I.; Chemerinski, A.; Liu, C.; Lipson, J.; Allison, K.; Gallop, R.; Dokras, A. Racial differences in anxiety, depression, and quality of life in women with polycystic ovary syndrome. FS Rep. 2021, 2, 230–237. [Google Scholar] [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J.J.H.R. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum. Reprod. 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total Responses, N (%) | Living in India, n (%) | Living Outside India, n (%) | |
|---|---|---|---|
| Age (years) | 4409 | 2046 (74) | 734 (26) |
| 18–24 | 1631 (37) | 950 (46) | 114 (16) |
| 25–34 | 2367 (53) | 963 (47) | 489 (67) |
| ≥35 | 411 (9.3) | 133 (7) | 131 (17) |
| BMI (kg/m2) | 4409 | - | - |
| <18.0 | 110 (3) | 57 (3) | 10 (2) |
| 18.0–22.9 | 930 (21) | 515 (25) | 109 (15) |
| 23.0–24.9 | 674 (15) | 293 (14) | 99 (13) |
| ≥25.0 | 2695 (61) | 1181 (58) | 516 (70) |
| Country of birth | 2780 | ||
| India | 2577 (93) | 1996 (98) | 581 (79) |
| Other countries | 203 (7) | 50 (2) | 153 (21) |
| Missing | 1629 (37) | - | - |
| Education | 2780 | ||
| Postgraduate degree | 1213 (44) | 767 (37) | 375 (51) |
| Undergraduate degree | 1375 (49) | 1077 (53) | 298 (41) |
| Below undergraduate degree | 192 (7) | 202 (10) | 61 (8) |
| Missing | 1629 (37) | - | - |
| Occupation | 2806 | ||
| Employed | 1521 (54) | 1003 (49) | 483 (66) |
| Studying | 860 (31) | 671 (33) | 89 (12) |
| Unemployed | 365 (13) | 190 (9) | 66 (9) |
| Home Duties | 330 (12) | 159 (8) | 90 (12) |
| Other a | 110 (4) | 21 (1) | 5 (1) |
| Missing | 1603 (36) | - | - |
| Relationship status | 2780 | ||
| Married and living with a partner/In a relationship | 1623 (58) | 1058 (52) | 565 (77) |
| Single | 1113 (40) | 960 (47) | 153 (21) |
| Other b | 596 (21) | 28 (1) | 16 (2) |
| Missing | 16,291 (37) | - | - |
| History of pregnancy | 2780 | ||
| No | 2185 (79) | 1740 (85) | 445 (61) |
| Yes | 595 (21) | 306 (15) | 289 (39) |
| Missing | 1629 (37) | - | - |
| If yes, ever needed treatment to fall pregnant | 589 | ||
| • NO | 307 (52) | 151 (50) | 156 (55) |
| • Yes | 282 (48) | 154 (50) | 128 (45) |
| • Missing | 6 (0.01) | - | - |
| If yes, the number of biological children | 526 | ||
| • One | 228 (43) | 110 (41) | 118 (45) |
| • Currently pregnant | 160 (30) | 73 (27) | 87 (33) |
| • Two or more | 73 (14) | 30 (11) | 43 (16) |
| • None | 70 (13) | 54 (20) | 16 (6) |
| • Missing | 69 (12) | - | - |
| Family history of PCOS | 3993 | ||
| No | 3274 (82) | 1677 (82) | 575 (79) |
| Yes | 719 (18) | 365 (18) | 154 (21) |
| • Sister | 513 (66) | 249 (68) | 116 (75) |
| • Mother | 250 (32) | 135 (37) | 50 (32) |
| • Daughter | 14 (2) | 7 (2) | 4 (3) |
| Missing | 416 (9) | - | - |
| Family history of type 2 diabetes | 3963 | ||
| No | 2251 (57) | 1161 (57) | 386 (53) |
| Yes | 1712 (43) | 862 (43) | 434 (47) |
| • Father | 1290 (75) | 632 (73) | 231 (53) |
| • Mother | 828 (48) | 392 (45) | 177 (41) |
| • Sister | 40 (2) | 11 (1) | 14 (3) |
| • Brother | 35 (2) | 16 (2) | 10 (2) |
| • Daughter or Son | 5 (0.1) | 3 (0) | 2 (1) |
| Missing | 446 (10) | - | - |
| Overall Responses, Mean (SD) | Living in India, Mean (SD) | Living Outside India, Mean (SD) | |
|---|---|---|---|
| Age when symptoms first appeared | 19.0 (5.0) | 18.5 (4.7) | 19.6 (5.4) |
| Age when first visited a health professional | 20.0 (5.0) | 19.6 (4.6) | 20.8 (5.2) |
| Age when diagnosed with PCOS | 20.8 (4.8) | 20.0 (4.4) | 22.0 (5.4) |
| Sign/symptoms at onset, n (%) | 3824 | ||
| Irregular menstrual cycles/periods | 3156 (83) | 1724 (85) | 613 (84) |
| Cysts on the ovaries (in an ultrasound) | 2263 (59) | 1274 (63) | 418 (57) |
| Excess unwanted hair growth on the face | 1836 (48) | 967 (47) | 406 (55) |
| Increased tendency for weight gain | 1820 (48) | 986 (48) | 376 (51) |
| Difficulty losing weight | 1763 (46) | 930 (46) | 371 (51) |
| Acne/Pimples | 1637 (43) | 928 (46) | 276 (38) |
| Excess hair loss | 1443 (38) | 821 (40) | 233 (32) |
| Anxiety | 757 (20) | 421 (21) | 136 (19) |
| Problems with ovulation | 662 (17) | 329 (16) | 153 (21) |
| Depression | 578 (15) | 333 (16) | 94 (12) |
| High blood levels of androgens/male hormones (e.g., testosterone) | 511 (13) | 279 (14) | 121 (17) |
| Not able to fall pregnant (Infertility) | 375 (10) | 170 (8) | 111 (15) |
| Other than above | 189 (5) | 117 (6) | 34 (5) |
| Increased metabolic risk (e.g., fear of developing type 2 diabetes) | 23 (1) | 128 (6) | 56 (8) |
| I do not remember | 19 (0.1) | 6 (0.3) | 5 (0.7) |
| Missing | 585 (13) | - | - |
| Diagnosed with PCOS by, n (%) | 3839 | ||
| Gynecologists/obstetrician | 3149 (82) | 1746 (85) | 543 (74) |
| General practitioner/family physician/family doctor | 376 (9.8) | 121 (6) | 122 (17) |
| Endocrinologist | 150 (3.9) | 78 (4) | 43 (6) |
| Dermatologist | 82 (2.1) | 47 (2) | 8 (1) |
| Infertility specialist | 77 (2.0) | 42 (2) | 17 (2) |
| Cardiologist | 3 (0.001) | - | - |
| Psychiatrist | 2 (0.001) | 2 (0.1) | 0 (0) |
| Missing | 577 (13) | - | - |
| Overall Responses, (N = 3595) | Country of Residence (n = 2780) | p-Value * | ||
|---|---|---|---|---|
| n (%) | Living in India, n (%) | Living Outside India, n (%) | ||
| Information provision about | ||||
| PCOS | 0.039 | |||
| Information was not given | 482 (13) | 309 (15) | 88 (12) | |
| Information was given | 3113 (87) | 1737 (85) | 646 (88) | |
| Long-term complications | 0.042 | |||
| Information was not given | 1240 (35) | 749 (37) | 238 (32) | |
| Information was given | 2355 (65) | 1297 (63) | 496 (68) | |
| Treatment options | 0.594 | |||
| Information was not given | 516 (14) | 298 (15) | 101 (14) | |
| Information was given | 3079 (86) | 1748 (85) | 633 (86) | |
| Diet | 0.655 | |||
| Information was not given | 871 (24) | 507 (25) | 188 (26) | |
| Information was given | 2724 (76) | 1539 (75) | 456 (74) | |
| Exercise | 0.004 | |||
| Information was not given | 737 (21) | 409 (20) | 184 (25) | |
| Information was given | 2858 (79) | 1637 (80) | 550 (75) | |
| Behavioural advice to support diet and exercise | 0.068 | |||
| Information was not given | 1071 (30) | 625 (31) | 251 (34) | |
| Information was given | 2524 (70) | 1421 (70) | 483 (66) | |
| Emotional support after diagnosis | 0.927 | |||
| Information was not given | 1232 (34) | 737 (36) | 263 (36) | |
| Information was given | 2363 (66) | 1309 (64) | 471 (64) | |
| Overall satisfaction with the manner of diagnosis | ||||
| Dissatisfied | 1067 (30) | 618 (30) | 229 (31) | 0.314 |
| Neutral | 1304 (36) | 763 (37) | 251 (34) | |
| Satisfied | 1224 (34) | 665 (33) | 254 (35) | |
| Satisfaction with the information given about | 3113 | 2383 | ||
| PCOS | 0.278 | |||
| Dissatisfied | 1038 (33) | 591(34) | 229 (36) | |
| Neutral | 910 (29) | 515 (30) | 170 (26) | |
| Satisfied | 1165 (38) | 631 (36) | 247 (38) | |
| Long-term complications | 2355 | 1793 | 0.502 | |
| Dissatisfied | 959 (41) | 532 (41) | 198 (40) | |
| Neutral | 594 (25) | 326 (25) | 138 (28) | |
| Satisfied | 802 (34) | 439 (34) | 160 (32) | |
| Treatment options | 3079 | 2381 | 0.424 | |
| Dissatisfied | 1533 (50) | 875 (50) | 334 (51) | |
| Neutral | 691 (22) | 400 (23) | 131 (21) | |
| Satisfied | 855 (28) | 473 (73) | 168 (26) | |
| Diet | 2724 | 2085 | 0.012 | |
| Dissatisfied | 1065 (24) | 600 (39) | 242 (44) | |
| Neutral | 666 (15) | 363 (24) | 138 (25) | |
| Satisfied | 993 (22) | 576 (37) | 546 (31) | |
| Exercise | 2858 | 2187 | 0.009 | |
| Dissatisfied | 939 (33) | 518 (32) | 202 (37) | |
| Neutral | 725 (25) | 416 (25) | 152 (28) | |
| Satisfied | 1194 (42) | 703 (43) | 196 (35) | |
| Behavioural advice to support diet and exercise | 2524 | 1904 | 0.158 | |
| Dissatisfied | 962 (38) | 551 (39) | 209 (43) | |
| Neutral | 701 (28) | 388 (27) | 130 (27) | |
| Satisfied | 861 (34) | 482 (34) | 144 (30) | |
| Emotional support after diagnosis | 2363 | 1780 | 0.834 | |
| Dissatisfied | 1239 (53) | 716 (55) | 256 (54) | |
| Neutral | 530 (22) | 273 (21) | 104 (22) | |
| Satisfied | 594 (22) | 320 (24) | 111 (24) | |
| Delay in seeking help after symptoms onset | 3276 | 2325 | 0.263 | |
| Less than 1 year | 1707 (52) | 897 (52) | 292 (49) | |
| 1 year and above | 1569 (48) | 834 (48) | 302 (51) | |
| Delay in diagnosis | 3195 | 2320 | 0.296 | |
| Less than 1 year | 2340 (73) | 1249 (74) | 443 (71) | |
| 1 year and above | 855 (27) | 450 (26) | 178 (29) | |
| Country of Residency: India a/Outside India | Delay in Diagnosis: Less Than 1 Year a/1 Year or More | Delay in Seeking Help: Less Than 1 Year a/1 Year or More | |
|---|---|---|---|
| OR (95% CI), p-Value | OR (95% CI), p-Value | OR (95% CI), p-Value | |
| Overall satisfaction with the manner of diagnosis | 1.01 (1.0 to 1.2), 0.722 | 0.69 (0.5 to 0.8), <0.001 * | 0.91 (0.7 to 1.0), 0.270 |
| Information provided about b | |||
| PCOS | 1.40 (1.0 to 1.8), 0.014 * | 0.62 (0.4 to 0.8), <0.001 * | 0.97 (0.7 to 1.2), 0.836 |
| Long-term complications | 1.23 (1.0 to 1.4), 0.030 * | 0.81 (0.6 to 0.9), 0.031 * | 1.0 (0.8 to 1.1), 0.938 |
| Treatment options | 1.18 (0.9 to 1.5), 0.197 | 0.79 (0.6 to 1.0), 0.082 | 0.95 (0.7 to 1.2), 0.693 |
| Diet | 1.04 (0.8 to 1.2), 0.711 | 0.91 (0.7 to 1.1), 0.399 | 0.96 (0.7 to 1.4), 0.670 |
| Exercise | 0.83 (0.6 to 1.0), 0.106 | 0.90 (0.7 to 1.1), 0.390 | 0.77 (0.6 to 0.9), 0.011 * |
| Behavioural advice to improve diet and exercise | 0.91 (0.9 to 1.1), 0.368 | 1.00 (0.8 to 1.2), 0.986 | 0.88 (0.7 to 1.0), 0.183 |
| Emotional support after diagnosis | 1.02 (0.8 to 1.2), 0.775 | 1.04 (0.8 to 0.2), 0.682 | 0.83 (0.7 to 0.9), 0.037 * |
| Level of satisfaction with the information provided about c | |||
| PCOS | 0.97 (0.8 to 1.1), 0.722 | 0.68 (0.5 to 0.8), <0.001 * | 0.86 (0.7 to 1.0), 0.069 |
| Long-term complications | 0.96 (0.7 to 1.1), 0.726 | 0.70 (0.5 to 0.8), <0.001 * | 0.94 (0.7 to 1.1), 0.577 |
| Treatment options | 0.84 (0.6 to 1.0), 0.065 | 0.73 (0.6 to 0.8), 0.002 * | 0.71 (0.6 to 0.8), <0.001 * |
| Diet | 0.74 (0.6 to 0.8), 0.002 * | 0.74 (0.6 to 0.9), 0.004 * | 0.80 (0.6 to 0.9), 0.013 * |
| Exercise | 0.74 (0.6 to 0.9), 0.002 * | 0.68 (0.5 to 0.8), <0.001 * | 0.86 (0.7 to 1.0), 0.101 |
| Behavioural advice to improve diet and exercise | 0.74 (0.6 to 0.9), 0.004 * | 0.72 (0.5 to 0.8), 0.002 * | 0.69 (0.5 to 0.8), <0.001 * |
| Emotional support after diagnosis | 0.87 (0.7 to 1.0), 0.212 | 0.78 (0.6 to 0.9), 0.034 * | 0.62 (0.5 to 0.7), <0.001 * |
| Total Responses, n (%) | Living in India | Living Outside India | |
|---|---|---|---|
| The number of health professionals consulted | 3117 | ||
| One | 1444 (46) | 958 (48) | 287 (40) |
| Two | 1368 (44) | 877 (44) | 338 (47) |
| Three or more | 305 (10) | 180 (9) | 92 (13) |
| List of health professionals consulted | 3117 | ||
| Gynecologist/obstetrician | 2809 (90) | 1855 (91) | 611 (83) |
| General practitioner/family physician/family doctor | 825 (26) | 421 (21) | 313 (43) |
| Allied health professional (e.g., dietician, exercise physiologist) | 621 (20) | 399 (20) | 148 (20) |
| Endocrinologist | 518 (17) | 306 (15) | 157 (21) |
| Dermatologist | 505 (16) | 356 (17) | 89 (12) |
| Infertility specialist | 350 (11) | 201 (10) | 118 (16) |
| Psychiatrist | 122 (4) | 78 (4) | 32 (4) |
| Cardiologist | 14 (0.1) | 7 (0.3) | 4 (0.5) |
| Other than above | 225 (7) | 168 (8) | 37 (5) |
| Never seen a medical doctor or allied health practitioner for PCOS treatment | 58 (2) | 31 (2) | 17 (2) |
| Missing | 1292 (29) | - | - |
| List of conventional treatments used | 2547 | ||
| Combined oral contraceptive pills (estrogen + progestin) | 1613 (63) | 1052 (64) | 389 (63) |
| Metformin (insulin-sensitizing medicines) | 1048 (41) | 593 (36) | 332 (54) |
| Anti-androgen drugs (to correct male-hormone levels) | 637 (25) | 436 (27) | 131 (21) |
| Ovulation induction to fall pregnant (e.g., Letrozole, Clomid, gonadotropins) | 359 (14) | 193 (12) | 133 (22) |
| Anti-obesity drugs | 174 (7) | 115 (7) | 41 (7) |
| Intrauterine insemination (IUI) | 131 (5) | 83 (5) | 34 (6) |
| Laparoscopic surgery (ovarian drilling) | 123 (5) | 63 (4) | 52 (8) |
| In-vitro fertilization (IVF) or intracytoplasmic sperm injection (ICSI) | 99 (4) | 41 (3) | 48 (8) |
| Intrauterine device (IUD) (e.g., Mirena or Depo Provera) | 39 (2) | 11 (1) | 24 (4) |
| Bariatric surgery | 15 (1) | 2 (0.1) | 8 (1.3) |
| Other than above | 463 (18) | 337 (21) | 71 (12) |
| Missing | 1862 (42) | - | - |
| Diets used to manage PCOS in the past five years | 2921 | ||
| Yes | 1978 (68) | 1328 (65) | 558 (76) |
| No | 943 (32) | 718 (35) | 176 (24) |
| Missing | 1448 (33) | - | - |
| Use of exercise | 2921 | ||
| Yes | 2241 (77) | 1572 (77) | 540 (74) |
| None of the given forms | 680 (23) | 474 (23) | 194 (26) |
| Missing | 1488 (34) | - | - |
| Use of ingestible TCIM | 3098 | ||
| Yes | 1942 (63) | 1345 (66) | 399 (54) |
| No | 1156 (37) | 701 (34) | 335 (46) |
| Missing | 1279 (29) | - | - |
| Use of yoga | 3027 | ||
| Yes | 1775 (59) | 1238 (61) | 367 (50) |
| No | 1252 (41) | 808 (39) | 367 (50) |
| Missing | 1382 (31) | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rao, V.S.; Cowan, S.; Armour, M.; Smith, C.A.; Cheema, B.S.; Moran, L.; Lim, S.; Gupta, S.; Manincor, M.D.; Sreedhar, V.; et al. A Global Survey of Ethnic Indian Women Living with Polycystic Ovary Syndrome: Co-Morbidities, Concerns, Diagnosis Experiences, Quality of Life, and Use of Treatment Methods. Int. J. Environ. Res. Public Health 2022, 19, 15850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315850
Rao VS, Cowan S, Armour M, Smith CA, Cheema BS, Moran L, Lim S, Gupta S, Manincor MD, Sreedhar V, et al. A Global Survey of Ethnic Indian Women Living with Polycystic Ovary Syndrome: Co-Morbidities, Concerns, Diagnosis Experiences, Quality of Life, and Use of Treatment Methods. International Journal of Environmental Research and Public Health. 2022; 19(23):15850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315850
Chicago/Turabian StyleRao, Vibhuti Samarth, Stephanie Cowan, Mike Armour, Caroline A. Smith, Birinder S. Cheema, Lisa Moran, Siew Lim, Sabrina Gupta, Michael De Manincor, Vikram Sreedhar, and et al. 2022. "A Global Survey of Ethnic Indian Women Living with Polycystic Ovary Syndrome: Co-Morbidities, Concerns, Diagnosis Experiences, Quality of Life, and Use of Treatment Methods" International Journal of Environmental Research and Public Health 19, no. 23: 15850. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph192315850