
Utilization of Palliative Care Screening Tool to Early Identify Patients with COVID-19 Needing Palliative Care: A Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Background Information and Data Source
2.2. Study Participants
2.3. Advance Care Planning and Advance Directives
2.4. Outcome and Main Predictor Variables
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Participant Selection
3.2. Baseline Characteristics of Patients with Palliative Care Screening
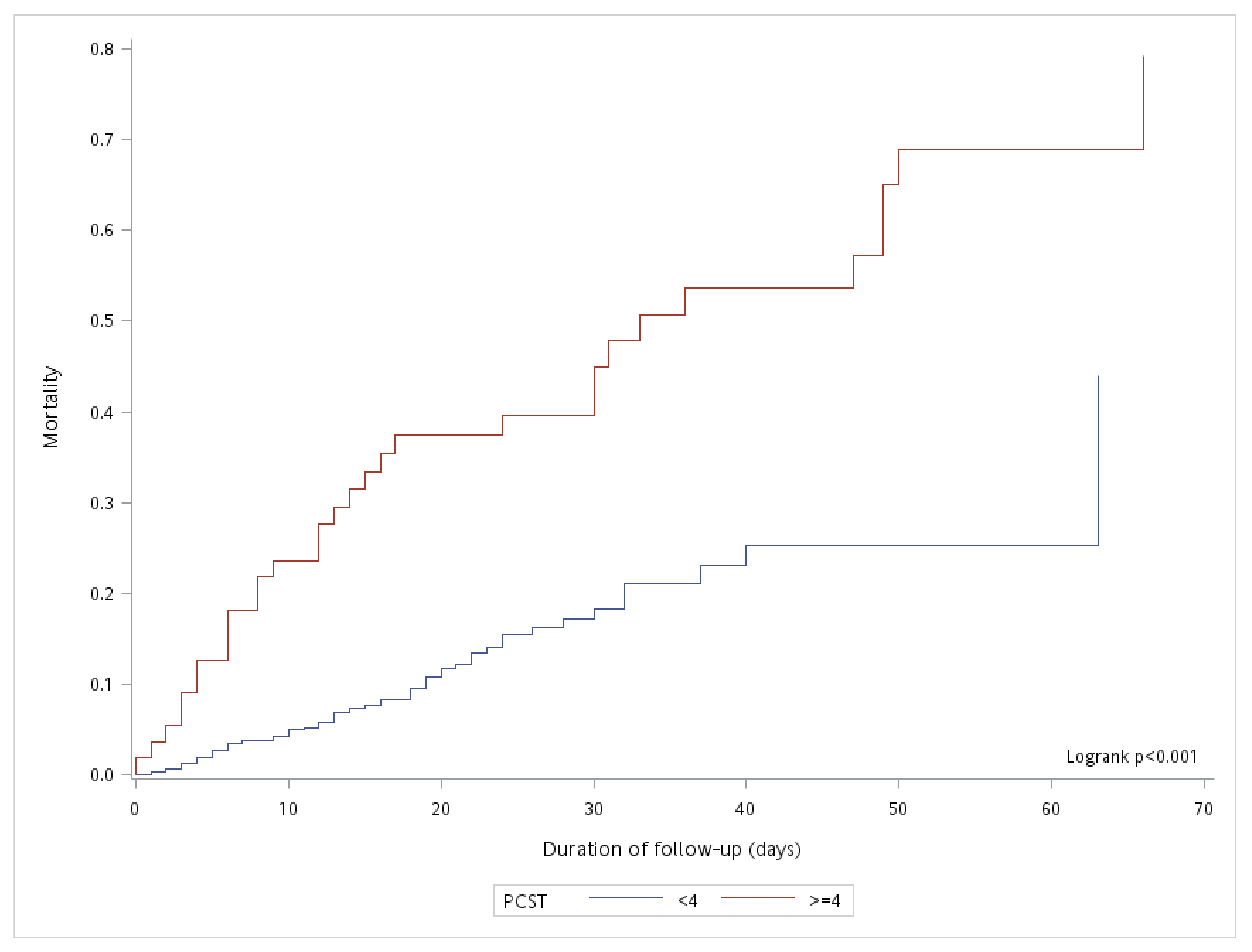
3.3. Factors Associated with Mortality in Patients with COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PCST | palliative care screening tool |
| COVID-19 | coronavirus disease 2019 |
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/ (accessed on 5 November 2021).
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or Moderate COVID-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Finelli, L.; Gupta, V.; Petigara, T.; Yu, K.; Bauer, K.A.; Puzniak, L.A. Mortality Among US Patients Hospitalized with SARS-CoV-2 Infection in 2020. JAMA Netw. Open 2021, 4, e216556. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Fadul, N.; Elsayem, A.F.; Bruera, E. Integration of palliative care into COVID-19 pandemic planning. BMJ Support. Palliat. Care 2021, 11, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Hurst, E.; Yessayan, L.; Mendez, M.; Hammad, A.; Jennings, J. Preliminary Analysis of a Modified Screening Tool to Increase the Frequency of Palliative Care Consults. Am. J. Hosp. Palliat. Care 2018, 35, 417–422. [Google Scholar] [CrossRef] [PubMed]
- DiLello, L.C.; Mulvihill, K.; Carpini, J.D.; Shah, R.; Hermanowski, J.; Chaubey, D. Content Validation of Advanced Illness Criteria of a Palliative Care Screening Tool. J. Palliat. Med. 2018, 21, 1604–1608. [Google Scholar] [CrossRef] [PubMed]
- Yen, Y.F.; Lee, Y.L.; Hu, H.Y.; Lai, Y.J.; Sun, W.J.; Ko, M.C.; Chen, C.C.; Curtis, J.R.; Huang, S.J.; Chu, D. An Interventional Study for the Early Identification of Patients with Palliative Care Needs and the Promotion of Advance Care Planning and Advance Directives. J. Pain Symptom. Manag. 2020, 59, 974–982.e3. [Google Scholar] [CrossRef] [PubMed]
- Curtis, J.R.; Kross, E.K.; Stapleton, R.D. The Importance of Addressing Advance Care Planning and Decisions About Do-Not-Resuscitate Orders During Novel Coronavirus 2019 (COVID-19). JAMA 2020, 323, 1771–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallo, M.B.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, e2146. [Google Scholar]
- Wang, S.S.; Huang, C.M.; Feng, R.C.; Wu, Y.L.; Huang, S.J. Validation of a concise screening tool for the identification of palliative care needs among inpatients: A prospective study in hospital setting. J. Formos. Med. Assoc. 2019, 118, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Gray, W.K.; Navaratnam, A.V.; Day, J.; Wendon, J.; Briggs, T.W.R. Changes in COVID-19 in-hospital mortality in hospitalised adults in England over the first seven months of the pandemic: An observational study using administrative data. Lancet Reg. Health Eur. 2021, 5, 100104. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Greco, M.; Zanella, A.; Albano, G.; Antonelli, M.; Bellani, G.; Bonanomi, E.; Cabrini, L.; Carlesso, E.; Castelli, G.; et al. Risk Factors Associated with Mortality Among Patients With COVID-19 in Intensive Care Units in Lombardy, Italy. JAMA Intern. Med. 2020, 180, 1345–1355. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.I.; Yoon, S.; Lee, H.J. Impact of comorbidity burden on mortality in patients with COVID-19 using the Korean health insurance database. Sci. Rep. 2021, 11, 6375. [Google Scholar] [CrossRef] [PubMed]
- Bhatraju, P.K.; Ghassemieh, B.J.; Nichols, M.; Kim, R.; Jerome, K.R.; Nalla, A.K.; Greninger, A.L.; Pipavath, S.; Wurfel, M.M.; Evans, L.; et al. COVID-19 in Critically Ill Patients in the Seattle Region—Case Series. N. Engl. J. Med. 2020, 382, 2012–2022. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Crooms, R.C.; Gelfman, L.P. Palliative Care and End-of-Life Considerations for the Frail Patient. Anesth. Analg. 2020, 130, 1504–1515. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | No. (%) of Subjects * | p Value | ||
|---|---|---|---|---|
| Total, n = 897 | Palliative Care Screening Score (<4 Points), n = 842 | Palliative Care Screening Score (≥4 Points), n = 55 | ||
| Age, years | ||||
| Mean ± SD | 58.1 ± 16.7 | 57.1 ± 16.3 | 74.2 ± 13.6 | <0.001 |
| 18–64 | 551 (61.43) | 541 (64.25) | 10 (18.18) | <0.001 |
| ≥65 | 346 (38.57) | 301 (35.75) | 45 (81.82) | |
| Sex | ||||
| Female | 456 (50.84) | 433 (51.43) | 23 (41.82) | 0.167 |
| Male | 441 (49.16) | 409 (48.57) | 32 (58.18) | |
| Hospital units | ||||
| General ward | 871 (97.10) | 829 (98.46) | 42 (76.36) | <0.001 |
| Intensive care unit | 26 (2.90) | 13 (1.54) | 13 (23.64) | |
| Comorbidities | ||||
| Cancer | 13 (1.45) | 10 (1.19) | 3 (5.45) | 0.01 |
| Heart failure | 11 (1.23) | 10 (1.19) | 1 (1.82) | 0.681 |
| COPD | 10 (1.11) | 8 (0.95) | 2 (3.64) | 0.066 |
| Cerebrovascular disease | 17 (1.90) | 9 (1.07) | 8 (14.55) | <0.001 |
| Diabetes | 174 (19.40) | 159 (18.88) | 15 (27.27) | 0.127 |
| Hypertension | 230 (25.64) | 215 (25.53) | 15 (27.27) | 0.775 |
| Hemodialysis | ||||
| No | 875 (97.55) | 822 (97.62) | 53 (96.36) | 0.558 |
| Yes | 22 (2.45) | 20 (2.38) | 2 (3.64) | |
| Intubation | ||||
| No | 829 (92.42) | 787 (93.47) | 42 (76.36) | <0.001 |
| Yes | 68 (7.58) | 55 (6.53) | 13 (23.64) | |
| Advance care planning discussion | ||||
| No | 842 (93.87) | 801 (95.13) | 41 (74.55) | <0.001 |
| Yes | 55 (6.13) | 41 (4.87) | 14 (25.45) | |
| Advance directive completion | ||||
| No | 882 (98.33) | 836 (99.29) | 46 (83.64) | <0.001 |
| Yes | 15 (1.67) | 6 (0.71) | 9 (16.36) | |
| Outcome | ||||
| Death | 106 (11.82) | 75 (8.91) | 31 (56.36) | <0.001 |
| Follow-up days, mean (SD) | 16.1 ± 11.6 | 15.4 ± 10.4 | 27.1 ± 21.1 | <0.001 |
| Total follow-up duration (person-days) | 14473 | 12984 | 1489 | <0.001 |
| Variables | Number of Patients | Number of Deaths | Follow-Up Days | Incident Mortality a (95% CI) | Unadjusted HR (95% CI) | Adjusted HR (95% CI) |
|---|---|---|---|---|---|---|
| Palliative Care Screening Score | ||||||
| <4 points | 842 | 75 | 12,984 | 0.58 (0.45–0.72) | 1 | 1 |
| ≥4 points | 55 | 31 | 1489 | 2.08 (1.42–2.94) | 3.57 (2.28–5.57) *** | 2.08 (1.22–3.54) ** |
| Age, years | ||||||
| 18–64 | 551 | 25 | 7840 | 0.32 (0.21–0.47) | 1 | 1 |
| ≥65 | 346 | 81 | 6633 | 1.22 (0.97–1.52) | 3.73 (2.36–5.90) *** | 2.45 (1.50–3.98) *** |
| Sex | ||||||
| Female | 456 | 38 | 6988 | 0.54 (0.39–0.75) | 1 | 1 |
| Male | 441 | 68 | 7485 | 0.91 (0.71–1.15) | 1.63 (1.10–2.43) | 1.30 (0.86–1.96) |
| Hospital units | ||||||
| General ward | 871 | 83 | 13,946 | 0.60 (0.47–0.74) | 1 | 1 |
| Intensive care unit | 26 | 23 | 527 | 4.36 (2.79–6.48) | 6.72 (4.19–10.77) *** | 1.69 (0.92–3.08) |
| Comorbidities | ||||||
| Cancer | ||||||
| No | 884 | 101 | 14,162 | 0.71 (0.58–0.87) | 1 | 1 |
| Yes | 13 | 5 | 311 | 1.61 (0.52–3.71) | 2.11 (0.85–5.21) | 2.41 (0.94–6.16) |
| Heart failure | ||||||
| No | 886 | 99 | 14,271 | 0.69 (0.56–0.84) | 1 | 1 |
| Yes | 11 | 7 | 202 | 3.47 (1.40–7.01) | 4.67 (2.16–10.08) *** | 4.04 (1.67–9.78) ** |
| COPD | ||||||
| No | 887 | 103 | 14,221 | 0.72 (0.59–0.88) | 1 | 1 |
| Yes | 10 | 3 | 252 | 1.19 (0.25–3.44) | 1.51 (0.48–4.79) | 0.83 (0.21–3.32) |
| Cerebrovascular disease | ||||||
| No | 880 | 103 | 13,998 | 0.74 (0.60–0.89) | 1 | 1 |
| Yes | 17 | 3 | 475 | 0.63 (0.13–1.83) | 0.77 (0.24–2.45) | 0.59 (0.18–1.94) |
| Diabetes | ||||||
| No | 723 | 78 | 11,214 | 0.70 (0.55–0.87) | 1 | 1 |
| Yes | 174 | 28 | 3259 | 0.86 (0.57–1.24) | 1.19 (0.77–1.84) | 0.89 (0.55–1.42) |
| Hypertension | ||||||
| No | 667 | 75 | 10,604 | 0.71 (0.56–0.89) | 1 | 1 |
| Yes | 230 | 31 | 3869 | 0.80 (0.54–1.14) | 1.13 (0.74–1.71) | 1.08 (0.68–1.70) |
| Hemodialysis | ||||||
| No | 875 | 92 | 14,007 | 0.66 (0.53–0.80) | 1 | 1 |
| Yes | 22 | 14 | 466 | 3.00 (1.65–4.99) | 4.45 (2.52–7.85) *** | 2.55 (1.36–4.77) ** |
| Intubation | ||||||
| No | 829 | 62 | 12,834 | 0.48 (0.37–0.62) | 1 | 1 |
| Yes | 68 | 44 | 1639 | 2.68 (1.96–3.59) | 5.51 (3.69–8.21) *** | 3.05 (1.90–4.90) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, Y.-F.; Hu, H.-Y.; Chou, Y.-C.; Chen, C.-C.; Ho, C.-Y. Utilization of Palliative Care Screening Tool to Early Identify Patients with COVID-19 Needing Palliative Care: A Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031054
Yen Y-F, Hu H-Y, Chou Y-C, Chen C-C, Ho C-Y. Utilization of Palliative Care Screening Tool to Early Identify Patients with COVID-19 Needing Palliative Care: A Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031054
Chicago/Turabian StyleYen, Yung-Feng, Hsiao-Yun Hu, Yi-Chang Chou, Chu-Chieh Chen, and Chin-Yu Ho. 2022. "Utilization of Palliative Care Screening Tool to Early Identify Patients with COVID-19 Needing Palliative Care: A Cohort Study" International Journal of Environmental Research and Public Health 19, no. 3: 1054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031054