
Disparities in Excess, All-Cause Mortality among Black, Hispanic, and White Veterans at the U.S. Department of Veterans Affairs during the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bilinski, A.; Emanuel, E.J. COVID-19 and excess all-cause mortality in the US and 18 comparison countries. JAMA 2020, 324, 2100–2102. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Chen, J.T.; Waterman, P.D. Excess mortality in men and women in Massachusetts during the COVID-19 pandemic. Lancet 2020, 395, 1829. [Google Scholar] [CrossRef]
- Woolf, S.H.; Chapman, D.A.; Sabo, R.T.; Zimmerman, E.B. Excess deaths from COVID-19 and other causes in the US, March 1, 2020, to January 2, 2021. JAMA 2021, 325, 1786–1789. [Google Scholar] [CrossRef]
- Achilleos, S.; Quattrocchi, A.; Gabel, J.; Heraclides, A.; Kolokotroni, O.; Constantinou, C.; Ugarte, M.P.; Nicolaou, N.; Rodriguez-Llanes, J.M.; Bennett, C.M.; et al. Excess all-cause mortality and COVID-19-related mortality: A temporal analysis in 22 countries, from January until August 2020. Int. J. Epidemiol. 2021. [Google Scholar] [CrossRef]
- Ahmad, F.B.; Anderson, R.N. The Leading Causes of Death in the US for 2020. JAMA 2021, 325, 1829–1830. [Google Scholar] [CrossRef] [PubMed]
- Rossen, L.M.; Branum, A.M.; Ahmad, F.B.; Sutton, P.; Anderson, R.N. Excess deaths associated with COVID-19, by age and race and ethnicity—United States, January 26–October 3, 2020. MMWR 2020, 69, 1522. [Google Scholar] [CrossRef]
- Agha, Z.; Lofgren, R.P.; Van Ruiswyk, J.V.; Layde, P.M. Are patients at Veterans Affairs medical centers sicker?: A comparative analysis of health status and medical resource use. Arch. Intern. Med. 2000, 160, 3252–3257. [Google Scholar] [CrossRef]
- NCVAS. Department of Veterans Affairs Statistics at a Glance, Statistics; United States Department of Veterans Affairs: Washington, DC, USA, 2016; pp. 1–6.
- Feyman, Y.; Auty, S.G.; Tenso, K.; Strombotne, K.L.; Legler, A.; Griffith, K.N. County-Level Impact of the COVID-19 Pandemic on Excess Mortality Among US Veterans: A Population-Based Study. Lancet Reg. Health-Am. 2021, 5, 100093. [Google Scholar]
- Rentsch, C.T.; Kidwai-Khan, F.; Tate, J.P.; Park, L.S.; King, J.T., Jr.; Skanderson, M.; Hauser, R.G.; Schultze, A.; Jarvis, C.I.; Holodniy, M.; et al. Patterns of COVID-19 testing and mortality by race and ethnicity among United States veterans: A nationwide cohort study. PLoS Med. 2020, 17, e1003379. [Google Scholar] [CrossRef]
- Cardemil, C.V.; Dahl, R.; Prill, M.M.; Cates, J.; Brown, S.; Perea, A.; Marconi, V.; Bell, L.; Rodriguez-Barradas, M.C.; Rivera-Dominguez, G.; et al. COVID-19–Related Hospitalization Rates and Severe Outcomes Among Veterans From 5 Veterans Affairs Medical Centers: Hospital-Based Surveillance Study. JMIR Public Health Surveill. 2021, 7, e24502. [Google Scholar] [CrossRef]
- SShiels, M.S.; Haque, M.A.T.; Haozous, E.A.; Albert, P.S.; Almeida, J.S.; García-Closas, M.; Nápoles, A.M.; Pérez-Stable, E.J.; Freedman, N.D.; de González, A.B. Racial and ethnic disparities in excess deaths during the COVID-19 pandemic, March to December 2020. Ann. Intern. Med. 2021, 174, 1693–1699. [Google Scholar] [CrossRef] [PubMed]
- Wong, M.S.; Hoggatt, K.J.; Steers, W.N.; Frayne, S.M.; Huynh, A.K.; Yano, E.M.; Saechao, F.S.; Ziaeian, B.; Washington, D.L. Racial/ethnic disparities in mortality across the Veterans Health Administration. Health Equity 2019, 3, 99–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, M.; Haderlein, T.; Yuan, A.; Moy, E.; Jones, K.; Washington, D. Time Trends in Racial/Ethnic Differences in COVID-19 Infection and Mortality. Int. J. Environ. Res. Public Health 2021, 18, 4848. [Google Scholar] [CrossRef] [PubMed]
- Ramasamy, R.; Milne, K.M.; Bell, D.; Stoneham, S.M.; Chevassut, T.J. Molecular mechanisms for thrombosis risk in Black people: A role in excess mortality from COVID-19. Br.J. Haematol. 2020, 190, e78–e80. [Google Scholar] [CrossRef] [PubMed]
- Baum, A.; Schwartz, M.D. Admissions to veterans affairs hospitals for emergency conditions during the COVID-19 pandemic. JAMA 2020, 324, 96–99. [Google Scholar] [CrossRef] [PubMed]
- Simon, P.; Ho, A.; Shah, M.D.; Shetgiri, R. Trends in Mortality from COVID-19 and other Leading Causes of Death among Latino vs White Individuals in Los Angeles County, 2011–2020. JAMA 2021, 326, 973–974. [Google Scholar] [CrossRef]
- Ahmed, N.; Conway, C.A. Medical and mental health comorbidities among minority racial/ethnic groups in the United States. JSBHS 2020, 14, 11. [Google Scholar] [CrossRef]
- Williams, D.R.; Rucker, T.D. Understanding and addressing racial disparities in health care. HCFR 2000, 21, 75. [Google Scholar]
- Ward, R.; Nguyen, X.-M.; Li, Y.; Lord, E.; Lecky, V.; Song, R.; Casas, J.; Cho, K.; Gaziano, J.; Harrington, K.; et al. Racial and Ethnic Disparities in US Veteran Health Characteristics. Int. J. Environ. Res. Public Health 2021, 18, 2411. [Google Scholar] [CrossRef]
- Cossrow, N.; Falkner, B. Race/ethnic issues in obesity and obesity-related comorbidities. J. Clin. Endocrinol. Metab. 2004, 89, 2590–2594. [Google Scholar] [CrossRef] [Green Version]
- Do, D.P.; Frank, R. Using race-and age-specific COVID-19 case data to investigate the determinants of the excess COVID-19 mortality burden among Hispanic Americans. Demog. Res. 2021, 44, 699–718. [Google Scholar] [CrossRef]
- Polyakova, M.; Udalova, V.; Kocks, G.; Genadek, K.; Finlay, K.; Finkelstein, A.N. Racial Disparities In Excess All-Cause Mortality During The Early COVID-19 Pandemic Varied Substantially Across States: Study examines the geographic variation in excess all-cause mortality by race to better understand the impact of the COVID-19 pandemic. Health Aff. 2021, 40, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Raifman, M.A.; Raifman, J.R. Disparities in the population at risk of severe illness from COVID-19 by race/ethnicity and income. Am. J. Prev. Med. 2020, 59, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Do, D.P.; Frank, R. Unequal burdens: Assessing the determinants of elevated COVID-19 case and death rates in New York City’s racial/ethnic minority neighbourhoods. J. Epidemiol. Community Health 2021, 75, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Stoto, M.A.; Rothwell, C.; Lichtveld, M.; Wynia, M.K. A national framework to improve mortality, morbidity, and disparities data for COVID-19 and other large-scale disasters. AJPH 2021, 111, S93–S100. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| White | Black | Hispanic | Total | White | Black | Hispanic | Total | |
|---|---|---|---|---|---|---|---|---|
| Number of deaths | Age, gender Standardized mortality rates per 100,000 | |||||||
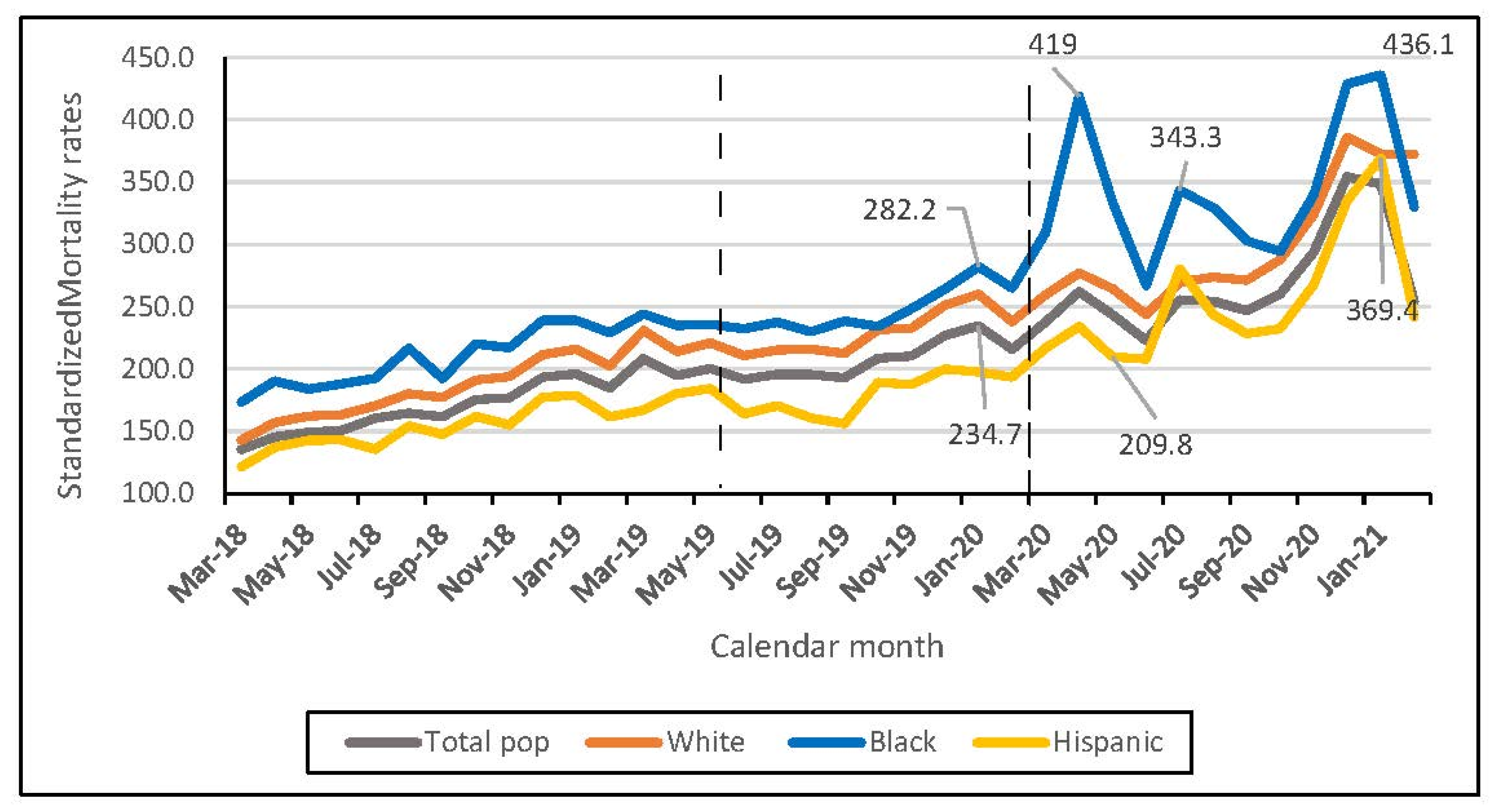
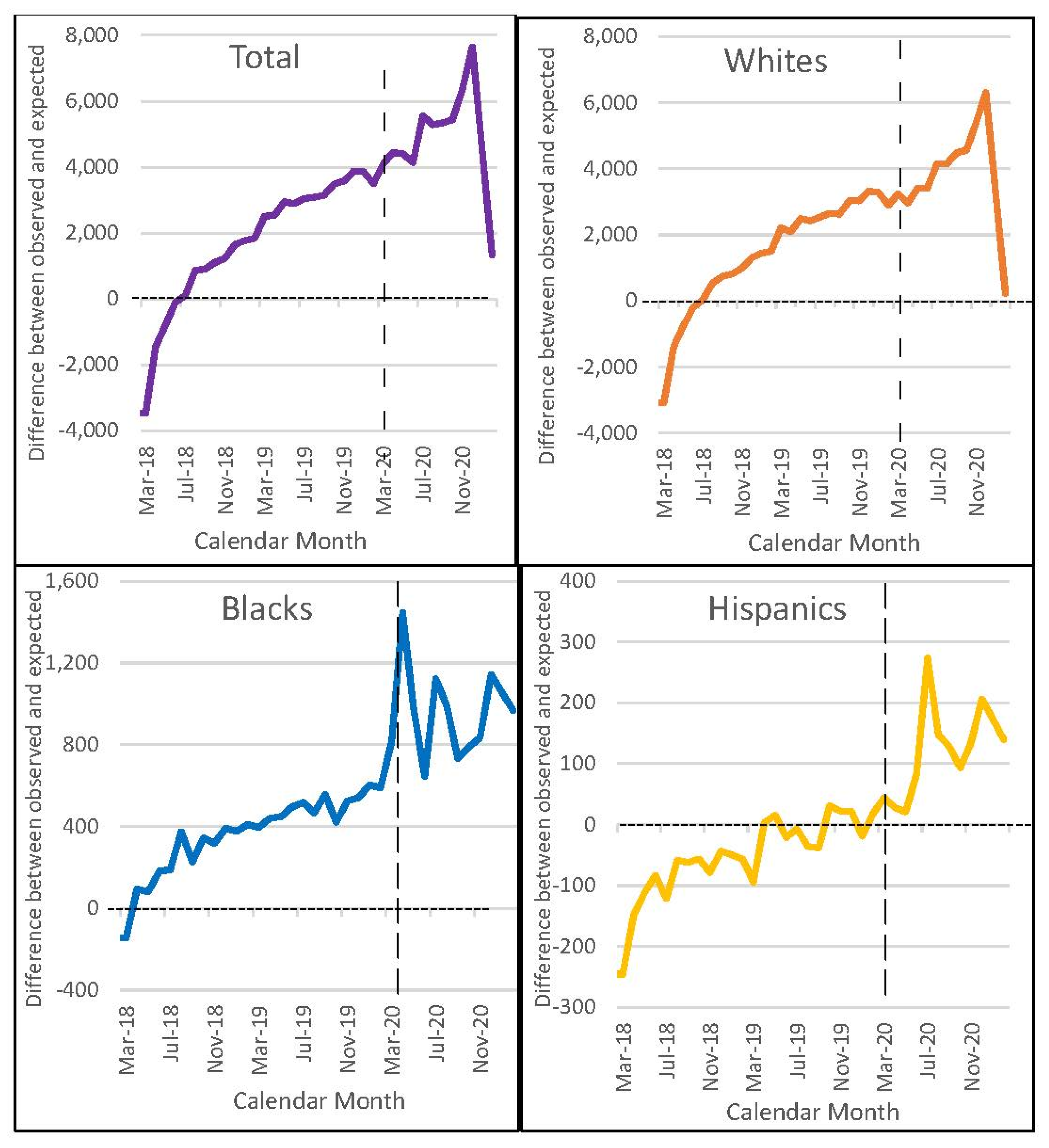
| Period 1 * | 136,228 | 20,436 | 6351 | 163,015 | 181 | 207 | 151 | 166 |
| Period 2 * | 161,566 | 23,117 | 7182 | 191,865 | 228 | 245 | 179 | 206 |
| Period 3 * | 190,551 | 30,455 | 9657 | 230,663 | 300 | 345 | 256 | 270 |
| Percent change | Percent change | |||||||
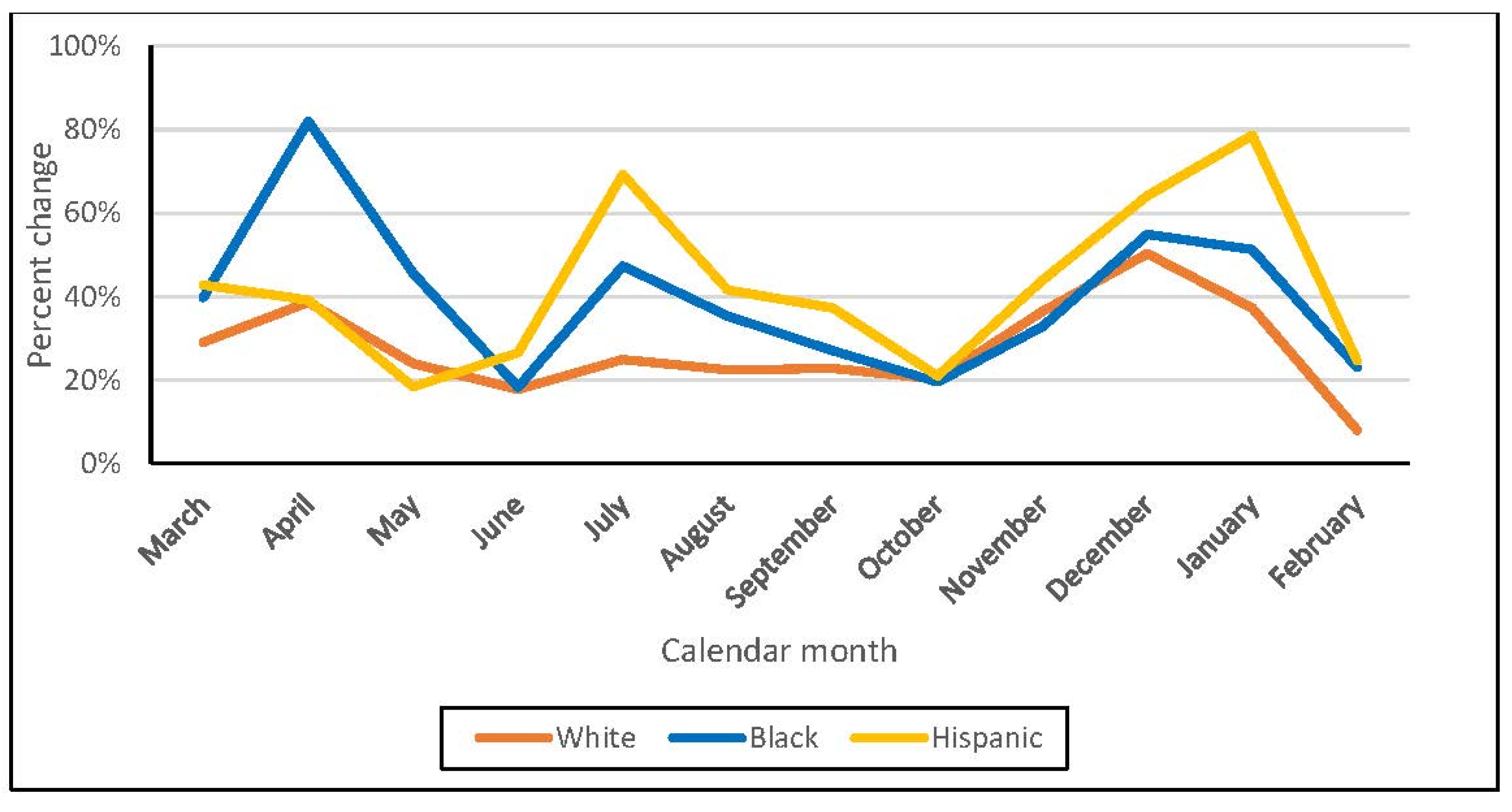
| Periods 1, 2 | 19% | 13% | 13% | 18% | 26% | 19% | 18% | 24% |
| Periods 2, 3 | 18% | 32% | 34% | 20% | 32% | 40% | 43% | 31% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lukowsky, L.R.; Der-Martirosian, C.; Dobalian, A. Disparities in Excess, All-Cause Mortality among Black, Hispanic, and White Veterans at the U.S. Department of Veterans Affairs during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 2368. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042368
Lukowsky LR, Der-Martirosian C, Dobalian A. Disparities in Excess, All-Cause Mortality among Black, Hispanic, and White Veterans at the U.S. Department of Veterans Affairs during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(4):2368. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042368
Chicago/Turabian StyleLukowsky, Lilia R., Claudia Der-Martirosian, and Aram Dobalian. 2022. "Disparities in Excess, All-Cause Mortality among Black, Hispanic, and White Veterans at the U.S. Department of Veterans Affairs during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 4: 2368. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042368