
Relationships between Volunteering, Neighbourhood Deprivation and Mental Wellbeing across Four British Birth Cohorts: Evidence from 10 Years of the UK Household Longitudinal Study


Abstract
:1. Introduction
1.1. Age and Birth Cohort
1.2. Neighbourhoods
2. Data and Methods
2.1. Measures
2.2. Analysis
3. Results
3.1. Descriptive
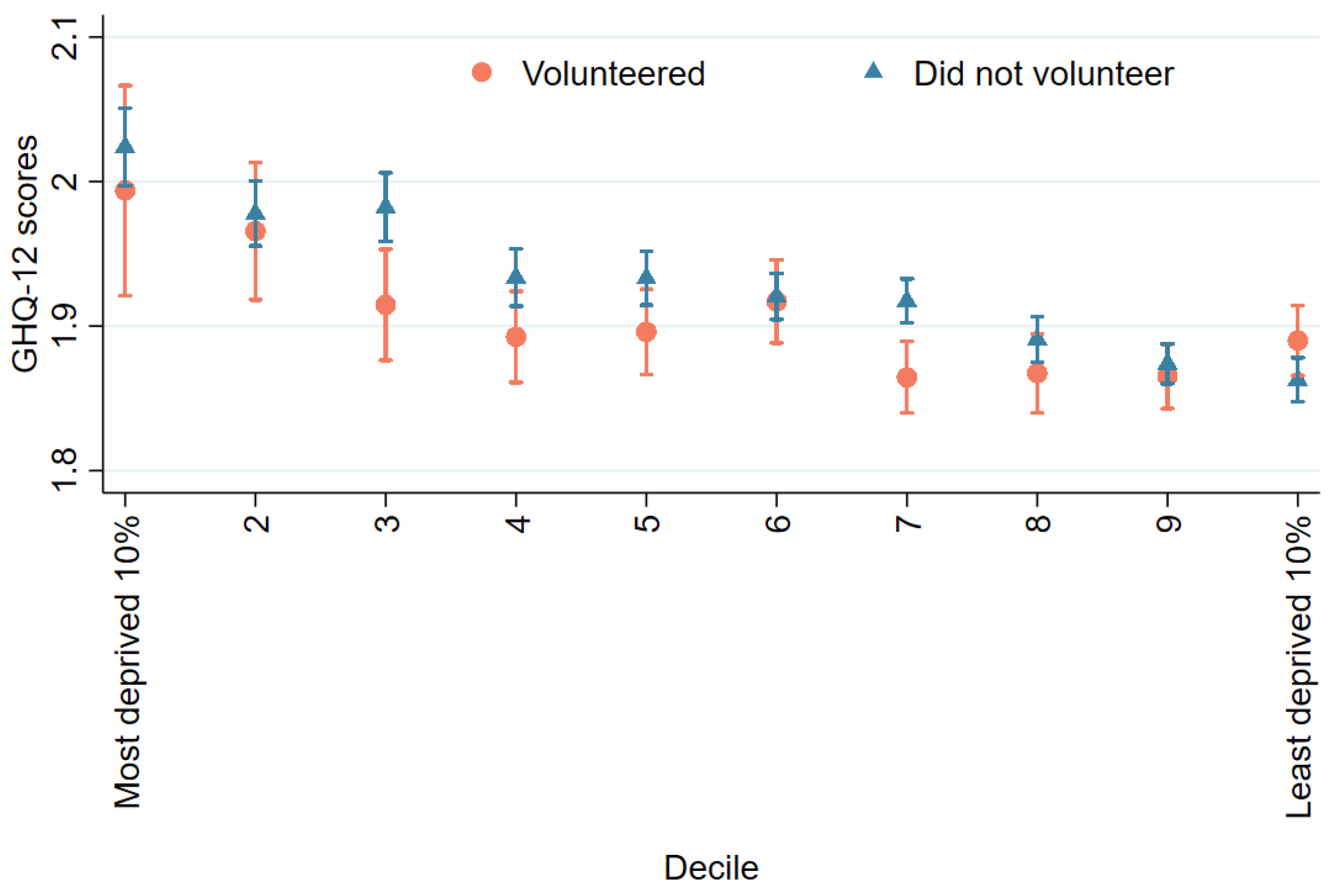
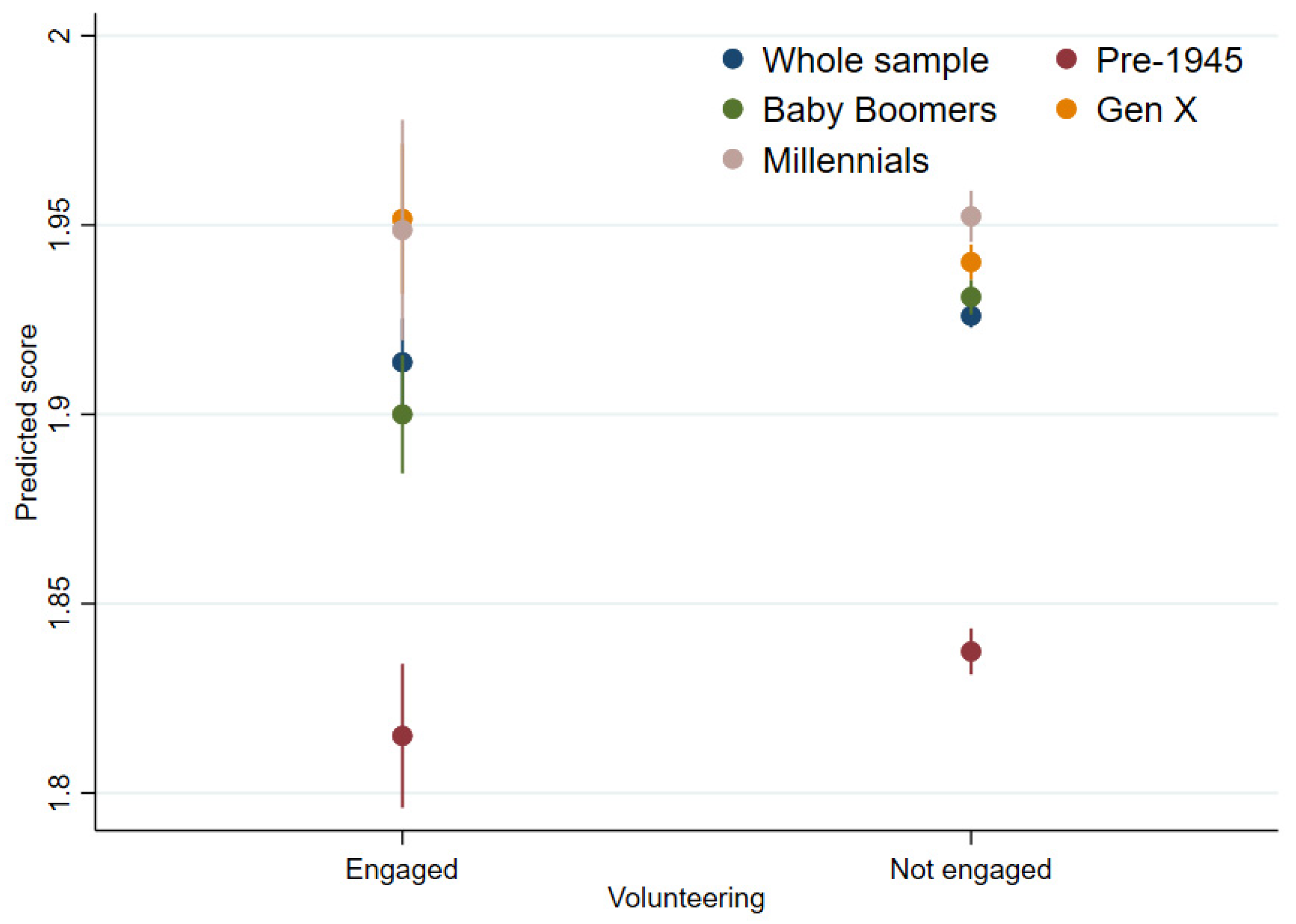
3.2. Mental Distress (GHQ-12)
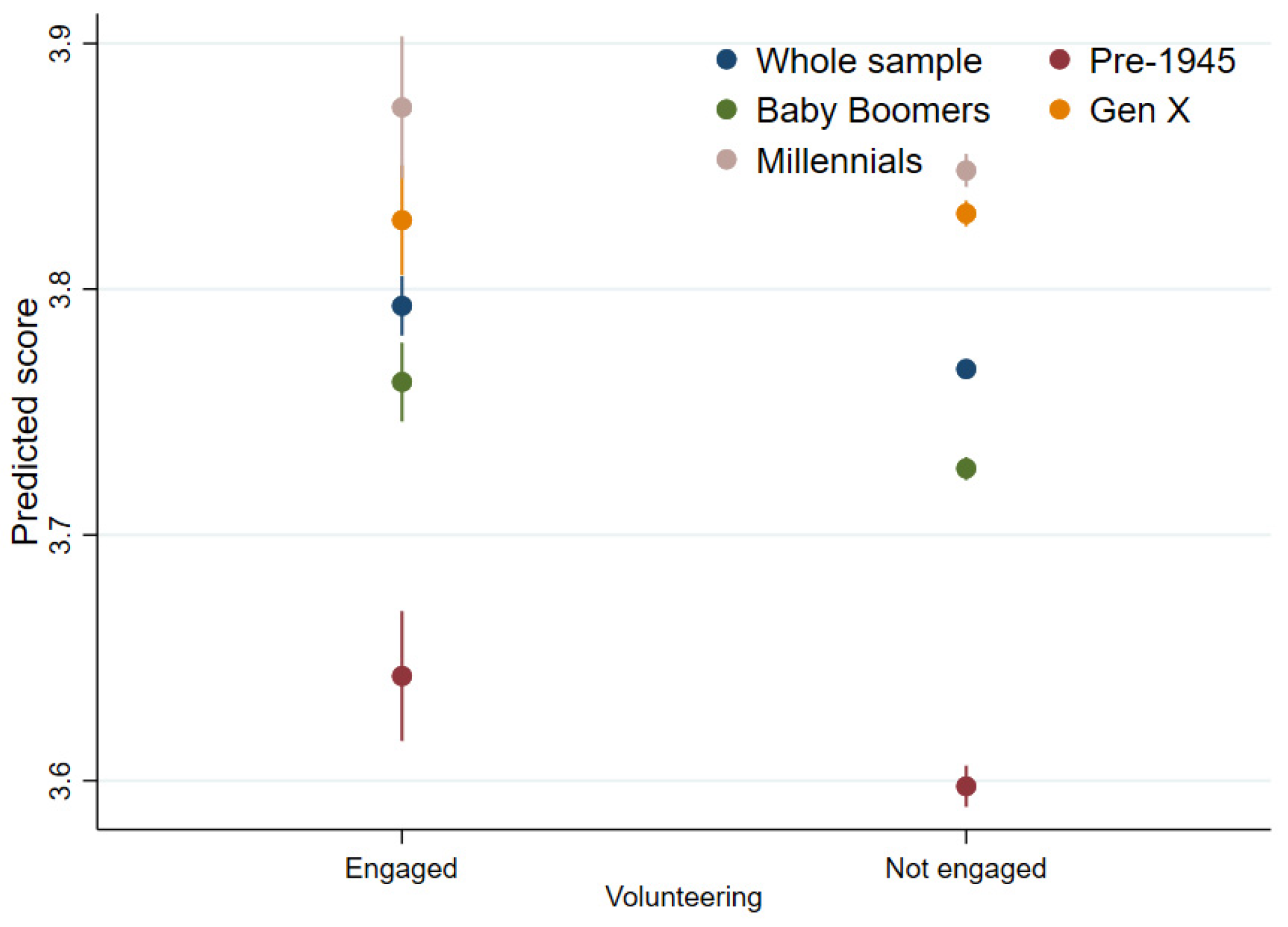
3.3. Health-Related Quality of Life (SF-12)
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volunteering. National Council for Voluntary Organisations. Available online: https://www.ncvo.org.uk/policy-and-research/volunteering-policy (accessed on 22 November 2021).
- The Power of Volunteerism. UN Volunteers. Available online: https://www.unv.org/power-volunteerism (accessed on 26 October 2021).
- Mcgarvey, A.; Jochum, V.; Davies, J.; Dobbs, J.; Hornung, L. Time Well Spent: A National Survey on the Volunteer Experience; NCVO: London, UK, 2019. [Google Scholar]
- Covid-19 Mutual Aid, UK. Find Your Local Group–Covid-19 Mutual Aid 2020. Available online: https://covidmutualaid.org/local-groups/ (accessed on 26 May 2020).
- NHS. Volunteer Responders: 250,000 Target Smashed with Three Quarters of a Million Committing to Volunteer. Available online: https://www.england.nhs.uk/2020/03/250000-nhs-volunteers/ (accessed on 13 May 2020).
- Milbourn, B.; Saraswati, J.; Buchanan, A. The relationship between time spent in volunteering activities and quality of life in adults over the age of 50 years: A systematic review. Br. J. Occup. Ther. 2018, 81, 613–623. [Google Scholar] [CrossRef]
- Isham, J.; Kolodinsky, J.; Kimberly, G. The effects of volunteering for nonprofit organizations on social capital formation: Evidence from a statewide survey. Nonprofit Volunt. Sect. Q. 2006, 35, 367–383. [Google Scholar] [CrossRef] [Green Version]
- Jongenelis, M.I.; Jackson, B.; Newton, R.U.; Pettigrew, S. Longitudinal associations between formal volunteering and well-being among retired older people: Follow-up results from a randomized controlled trial. Aging Ment. Health 2022, 26, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.I.; Morrow-Howell, N. Health outcomes of experience corps: A high-commitment volunteer program. Soc. Sci. Med. 2010, 71, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Han, S.H.; Kim, K.; Burr, J.A. Stress-buffering effects of volunteering on salivary cortisol: Results from a daily diary study. Soc. Sci. Med. 2018, 201, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Schreier, H.M.C.; Schonert-Reichl, K.A.; Chen, E. Effect of volunteering on risk factors for cardiovascular disease in adolescents: A randomized controlled trial. JAMA Pediatr. 2013, 167, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkinson, E.C.; Dickens, A.P.; Jones, K.; Thompson-Coon, J.; Taylor, R.S.; Rogers, M.; Bambra, C.L.; Lang, I.; Richards, S.H. Is volunteering a public health intervention? A systematic review and meta-analysis of the health and survival of volunteers. BMC Public Health 2013, 13, 773. [Google Scholar] [CrossRef] [Green Version]
- Pilkington, P.D.; Windsor, T.D.; Crisp, D.A. Volunteering and subjective well-being in midlife and older adults: The role of supportive social networks. J. Gerontol. Ser. B. 2012, 67, 249–260. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, L.; Burls, A.; Townsend, M.; Ebden, M. Volunteering in nature as a way of enabling people to reintegrate into society. Perspect. Public Health 2011, 131, 71–81. [Google Scholar] [CrossRef]
- Stuart, J.; Kamerāde, D.; Connolly, S.; Ellis, A.P.; Nichols, G.; Grotz, J. The Impacts of Volunteering on the Subjective Wellbeing of Volunteers: A Rapid Evidence Assessment; What Works Centre for Wellbeing: London, UK, 2020. [Google Scholar]
- Jang, H.; Tang, F.; Gonzales, E.; Lee, Y.S.; Morrow-Howell, N. Formal volunteering as a protector of health in the context of social 476 losses. J. Gerontol. Soc. Work 2018, 61, 834–848. [Google Scholar] [CrossRef]
- Zaninotto, P.; Breeze, E.; Mcmunn, A.; Nazroo, J. Socially productive activities, reciprocity and well-being in early old age: Gender-specific results from the English Longitudinal Study of Ageing (ELSA). Popul. Ageing 2013, 6, 47–57. [Google Scholar] [CrossRef]
- Yang, J.; Matz, C. A latent deprivation perspective: Mechanisms linking volunteering to mental health in later life. Int. J. Aging Hum. Dev. 2020. [Google Scholar] [CrossRef]
- Russell, A.R.; Nyame-Mensah, A.; de Wit, A.; Handy, F. Volunteering and wellbeing among ageing adults: A longitudinal analysis. Volunt. Int. J. Volunt. Nonprofit Organ. 2019, 30, 115–128. [Google Scholar] [CrossRef]
- Moore, C.W.; Allen, J.P. The effects of volunteering on the young volunteer. J. Prim. Prev. 1996, 17, 231–258. [Google Scholar] [CrossRef] [PubMed]
- Tabassum, F.; Mohan, J.; Smith, P. Association of volunteering with mental well-being: A lifecourse analysis of a national population-based longitudinal study in the U.K. BMJ Open 2016, 6, e011327. [Google Scholar] [CrossRef] [Green Version]
- Elias, J.K.; Sudhir, P.; Mehrotra, S. Long-term engagement in formal volunteering and well-being: An exploratory Indian study. Behav. Sci. 2016, 6, 20. [Google Scholar] [CrossRef] [Green Version]
- Musick, M.; Wilson, J. Volunteers: A Social Profile; Indiana University Press: Bloomington, IN, USA, 2008. [Google Scholar]
- Brewis, G. A Short History of Student Volunteering: Celebrating Ten Years of Student Volunteering Week; The British Library: London, UK, 2011. [Google Scholar]
- Brewis, G. Towards a New Understanding of Volunteering in England before 1960? Institute for Volunteering Research: London, UK, 2011. [Google Scholar]
- Gaskin, K. Young People, Volunteering and Civic Service: A Review of the Literature; Institute for Volunteering Research: London, UK; The British Library: London, UK, 2004. [Google Scholar]
- Smith, J.D. Volunteers: Making a Difference? In Voluntary Organisations and Social Policy in Britain; Harris, M., Rochester, C., Eds.; Palgrave: London, UK, 2001; pp. 185–198. [Google Scholar] [CrossRef]
- Lindsey, R.; Mohan, J.; Bulloch, S.; Metcalfe, E. Continuity and Change in Voluntary Action; Bristol University Press: Bristol, UK; Policy Press: Bristol, UK, 2018. [Google Scholar]
- Layard, R. Can We Be Happier? Evidence and Ethics; Penguin Random House: London, UK, 2021. [Google Scholar]
- Buck, D.; Fwbank, L. What Is Social Prescribing? King’s Fund: London, UK, 2020. [Google Scholar]
- Duncan, D.T.; Kawachi, I. Neighborhoods and Health, 2nd ed.; Oxford University Press: New York, NY, USA, 2018. [Google Scholar]
- Grinshteyn, E.G.; Sugar, J.A. Perceived neighbourhood safety and volunteerism among older adults. Ageing Soc. 2020, 41, 2914–2932. [Google Scholar] [CrossRef]
- Okun, M.A.; Michel, J. Sense of community and being a volunteer among the young-old. J. Appl. Gerontol. 2006, 25, 173–188. [Google Scholar] [CrossRef]
- Dury, S.; Willems, J.; De Witte, N.; De Donder, L.; Buffel, T.; Verté, D. Municipality and neighborhood influences on volunteering in later life. J. Appl. Gerontol. 2016, 35, 601–626. [Google Scholar] [CrossRef]
- Torgerson, M.; Edwards, M.E. Demographic determinants of perceived barriers to community involvement: Examining rural/urban differences. Nonprofit Volunt. Sect. Q. 2012, 42, 371–390. [Google Scholar] [CrossRef] [Green Version]
- Mcculloch, A.; Mohan, J.; Smith, P. Patterns of social capital, voluntary activity, and area deprivation in England. Environ. Plan. A 2012, 44, 1130–1147. [Google Scholar] [CrossRef] [Green Version]
- Clifford, D. Voluntary sector organisations working at the neighbourhood level in England: Patterns by local area deprivation. Environ. Plan A 2012, 44, 1148–1164. [Google Scholar] [CrossRef] [Green Version]
- Buck, N.; Mcfall, S. Understanding Society: Design overview. Longit. Life Course Stud. 2012, 3, 5–17. [Google Scholar]
- Census Geography. Office for National Statistics. Available online: https://www.ons.gov.uk/methodology/geography/ukgeographies/censusgeography#super-output-area-soa (accessed on 1 July 2020).
- Office for National Statistics. Changes to Output Areas and Super Output Areas in England and Wales, 2001 to 2011; Office for National Statistics: London, UK, 2012.
- Department for Communities and Local Government. The English Indices of Deprivation 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/465791/English_Indices_of_Deprivation_2015_-_Statistical_Release.pdf (accessed on 1 November 2021).
- Curtis, S. Space, Place and Mental Health; Routledge: London, UK, 2010. [Google Scholar] [CrossRef]
- Pevalin, D.J. Multiple applications of the GHQ-12 in a general population sample: An investigation of long-term retest effects. Soc. Psychiatry 2000, 35, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, D.P.; Williams, P. A User’s Guide to the General Health Questionnaire; NFER-Nelson: Windsor, UK, 1988. [Google Scholar]
- Ware, J.; Kosinksi, M.; Keller, S. A 12-Item short-form health survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allison, P.D. Fixed Effects Regression Models; SAGE Publishing: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Heo, J.; Chun, S.; Lee, S.; Kim, J. Life satisfaction and psychological well-being of older adults with cancer experience: The role of optimism and volunteering. Int. J. Aging Hum. Dev. 2016, 83, 274–289. [Google Scholar] [CrossRef] [PubMed]
- Chan, W.; Chui, C.H.K.; Cheung, J.C.S.; Lum, T.Y.S.; Lu, S. Associations between Volunteering and Mental Health during COVID-19 among Chinese Older Adults. J. Gerontol. Soc. Work 2021, 64, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Bradley, D.B. A reason to rise each morning: The meaning of volunteering in the lives of older adults. Generations 2000, 23, 45–50. Available online: https://lemosandcrane.co.uk/resources/Generations%20-%20A%20Reason%20to%20Rise%20Each%20Morning%20-%20The%20Meaning%20of%20Volunteering%20in%20the%20Lives%20of%20Older%20Adults.pdf (accessed on 27 November 2021).
- Rochester, C. Trends in Volunteering. Volunteer Now. 2018; Building Change Trust: Belfast, UK, 2018; Available online: https://volunteernow.aw-stage.co.uk/app/uploads/2018/10/Trends-in-Volunteering-Final-Report.pdf (accessed on 27 November 2021).
- Collishaw, S.; Maughan, B.; Goodman, R.; Pickles, A. Time trends in adolescent mental health. J. Child Psychol. Psychiatry Allied Discip. 2004, 45, 1350–1362. [Google Scholar] [CrossRef]
- Vizard, T.; Sadler, K.; Ford, T.; Newlove-Delgado, T.; McManus, S.; Marcheselli, F.; Davis, J.; Williams, T.; Leach, C.; Mandalia, D.; et al. The Mental Health of Children and Young People in England 2020; NHS Digital: Leeds, UK, 2020; Available online: https://files.digital.nhs.uk/AF/AECD6B/mhcyp_2020_rep_v2.pdf (accessed on 27 November 2021).
- Keyes, C.L.M. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [Green Version]
- McDonnell, D.; Mohan, J.; Norman, P. Charity density and social need: A longitudinal perspective. Nonprofit Volunt. Sect. Q. 2020, 49, 1082–1104. [Google Scholar] [CrossRef]
- Clifford, D. Disparities by deprivation: The geographical impact of unprecedented changes in local authority financing on the voluntary sector in England. EPA Econ. Sp. 2021, 53, 2050–2067. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Descriptive Statistics of Volunteering Frequency and Mental Health/Wellbeing | |||||
|---|---|---|---|---|---|
| Variables of Interest | Whole Sample | Pre-1945 (Born before 1945) | Baby Boomers (Born in 1945–1964) | Gen X (Born in 1965–1979) | Millennials (Born in 1980 or After) |
| Volunteering | |||||
| Overall mean | 0.21 | 0.24 | 0.23 | 0.19 | 0.19 |
| Between-participant SD (σu) | 0.33 | 0.37 | 0.34 | 0.29 | 0.31 |
| Within-participant SD (σe) | 0.30 | 0.28 | 0.29 | 0.31 | 0.33 |
| Intraclass correlation (ρ) | 0.54 | 0.63 | 0.58 | 0.47 | 0.47 |
| Mental distress (GHQ 12) | |||||
| Overall mean | 1.92 | 1.83 | 1.92 | 1.94 | 1.95 |
| Between-participant SD (σu) | 0.34 | 0.27 | 0.34 | 0.33 | 0.38 |
| Within-participant SD (σe) | 0.33 | 0.26 | 0.31 | 0.34 | 0.39 |
| Intraclass correlation (ρ) | 0.51 | 0.52 | 0.55 | 0.48 | 0.49 |
| Health-related quality of life (SF-12) | |||||
| Overall mean | 3.77 | 3.61 | 3.74 | 3.83 | 3.85 |
| Between-participant SD (σu) | 0.55 | 0.56 | 0.60 | 0.51 | 0.47 |
| Within-participant SD (σe) | 0.37 | 0.40 | 0.36 | 0.37 | 0.39 |
| Intraclass correlation (ρ) | 0.68 | 0.66 | 0.74 | 0.65 | 0.59 |
| Number of obs | 51,206 | 7351 | 21,809 | 13,256 | 8790 |
| Number of groups | 10,989 | 1491 | 4431 | 2702 | 2365 |
| Fixed-Effects Analysis Predicting the Associations between Volunteering and Mental Distress (GHQ-12) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample | Model 1 Volunteering | Model 2 = Model 1 + Demography and SEP | Model 3 = Model 2 + IMD | Number of Obs | Number of Groups | ||||||
| Coef | 95%CI | p-Value | Coef | 95%CI | p-Value | Coef | 95%CI | p-Value | |||
| Whole sample | −0.01 | −0.03, 0.00 | 0.121 | −0.01 | −0.03, 0.00 | 0.099 | −0.01 | −0.03, 0.00 | 0.101 | 51,206 | 10,989 |
| Pre-1945 (born before 1945) | −0.03 | −0.05, −0.00 | 0.026 | −0.02 | −0.05, 0.00 | 0.082 | −0.02 | −0.05, 0.00 | 0.082 | 7351 | 1491 |
| Baby Boomers (born in 1945–1964) | −0.03 | −0.05, −0.01 | 0.007 | −0.03 | −0.05, −0.01 | 0.003 | −0.03 | −0.05, −0.01 | 0.003 | 21,809 | 4431 |
| Gen X (born in 1965–1979) | 0.02 | −0.01, 0.04 | 0.213 | 0.01 | −0.01, 0.04 | 0.359 | 0.01 | −0.01, 0.04 | 0.360 | 13,256 | 2702 |
| Millennials (born in 1980 or after) | −0.01 | −0.05, 0.03 | 0.592 | −0.00 | −0.04, 0.03 | 0.833 | −0.00 | −0.04, 0.03 | 0.844 | 8790 | 2365 |
| Fixed-Effects Models Interacting with Index of Multiple Deprivation (IMD) 20% Most Deprived Areas | |||||
|---|---|---|---|---|---|
| Sample | Mental Distress (GHQ-12) | Number of Obs | Number of Groups | ||
| Coef | 95%CI | p-Value | |||
| Whole sample | 51,206 | 10,989 | |||
| Volunteering | −0.01 | −0.03, 0.00 | 0.133 | ||
| IMD 20% most deprived | −0.03 | −0.07, 0.02 | 0.281 | ||
| Volunteering * IMD 20% most deprived | −0.01 | −0.06, 0.04 | 0.788 | ||
| Pre-1945 (born before 1945) | 7351 | 1491 | |||
| Volunteering | −0.02 | −0.05, 0.00 | 0.100 | ||
| IMD 20% most deprived | −0.12 | −0.30, 0.07 | 0.213 | ||
| Volunteering * IMD 20% most deprived | −0.00 | −0.08, 0.08 | 0.999 | ||
| Baby Boomers (born in 1945–1964) | 21,809 | 4431 | |||
| Volunteering | –0.03 | –0.05, –0.01 | 0.001 | ||
| IMD 20% most deprived | −0.02 | −0.11, 0.08 | 0.732 | ||
| Volunteering * IMD 20% most deprived | 0.02 | −0.07, 0.11 | 0.736 | ||
| Gen X (born in 1965–1979) | 13,256 | 2702 | |||
| Volunteering | 0.01 | −0.02, 0.03 | 0.529 | ||
| IMD 20% most deprived | 0.01 | −0.06, 0.08 | 0.807 | ||
| Volunteering * IMD 20% most deprived | 0.02 | −0.06, 0.10 | 0.591 | ||
| Millennials (born in 1980 or after) | 8790 | 2365 | |||
| Volunteering | 0.01 | −0.03, 0.05 | 0.732 | ||
| IMD 20% most deprived | −0.02 | −0.08, 0.05 | 0.674 | ||
| Volunteering * IMD 20% most deprived | −0.05 | −0.14, 0.05 | 0.326 | ||
| Fixed-Effects Analysis Predicting the Associations between Volunteering and Health-Related Quality of Life (SF-12) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sample | Model 1 Volunteering | Model 2 = Model 1 + Demography and SEP | Model 3 = Model 2 + IMD | Number of Obs | Number of Groups | ||||||
| Coef | 95%CI | p-Value | Coef | 95%CI | p-Value | Coef | 95%CI | p-Value | |||
| Whole sample | 0.03 | 0.02, 0.05 | 0.000 | 0.03 | 0.01, 0.04 | 0.001 | 0.03 | 0.01, 0.04 | 0.001 | 51,206 | 10,989 |
| Pre-1945 (born before 1945) | 0.09 | 0.05, 0.13 | 0.000 | 0.04 | 0.01, 0.08 | 0.012 | 0.04 | 0.01, 0.08 | 0.012 | 7351 | 1491 |
| Baby Boomers (born in 1945–1964) | 0.03 | 0.01, 0.05 | 0.003 | 0.04 | 0.01, 0.06 | 0.001 | 0.04 | 0.01, 0.06 | 0.001 | 21,809 | 4431 |
| Gen X (born in 1965–1979) | −0.01 | −0.04, 0.02 | 0.611 | −0.00 | −0.03, 0.02 | 0.852 | −0.00 | −0.03, 0.02 | 0.846 | 13,256 | 2702 |
| Millennials (born in 1980 or after) | 0.04 | 0.00, 0.08 | 0.041 | 0.03 | −0.01, 0.06 | 0.157 | 0.03 | −0.01, 0.06 | 0.159 | 8790 | 2365 |
| Fixed-Effects Models Interacting with Index of Multiple Deprivation (IMD) 20% Most Deprived Areas | |||||
|---|---|---|---|---|---|
| Sample | Health-Related Quality of Life (SF-12) | Number of Obs | Number of Groups | ||
| Coef | 95%CI | p-Value | |||
| Whole sample | 51,206 | 10,989 | |||
| Volunteering | 0.02 | 0.01, 0.04 | 0.004 | ||
| IMD 20% most deprived | −0.00 | −0.05, 0.05 | 0.973 | ||
| Volunteering * IMD 20% most deprived | 0.02 | −0.03, 0.08 | 0.375 | ||
| Pre-1945 (born before 1945) | 7351 | 1491 | |||
| Volunteering | 0.04 | 0.00, 0.07 | 0.035 | ||
| IMD 20% most deprived | −0.07 | −0.30, 0.16 | 0.547 | ||
| Volunteering * IMD 20% most deprived | 0.08 | −0.08, 0.23 | 0.335 | ||
| Baby Boomers (born in 1945–1964) | 21,809 | 4431 | |||
| Volunteering | 0.04 | 0.02, 0.06 | 0.000 | ||
| IMD 20% most deprived | −0.08 | −0.19, 0.03 | 0.142 | ||
| Volunteering * IMD 20% most deprived | −0.02 | −0.11, 0.07 | 0.614 | ||
| Gen X (born in 1965–1979) | 13,256 | 2702 | |||
| Volunteering | 0.00 | −0.03, 0.03 | 0.908 | ||
| IMD 20% most deprived | 0.05 | −0.03, 0.13 | 0.193 | ||
| Volunteering * IMD 20% most deprived | −0.03 | −0.11, 0.04 | 0.380 | ||
| Millennials (born in 1980 or after) | 8790 | 2365 | |||
| Volunteering | 0.01 | −0.03, 0.04 | 0.725 | ||
| IMD 20% most deprived | −0.01 | −0.08, 0.07 | 0.888 | ||
| Volunteering * IMD 20% most deprived | 0.09 | −0.01, 0.19 | 0.091 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mak, H.W.; Coulter, R.; Fancourt, D. Relationships between Volunteering, Neighbourhood Deprivation and Mental Wellbeing across Four British Birth Cohorts: Evidence from 10 Years of the UK Household Longitudinal Study. Int. J. Environ. Res. Public Health 2022, 19, 1531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031531
Mak HW, Coulter R, Fancourt D. Relationships between Volunteering, Neighbourhood Deprivation and Mental Wellbeing across Four British Birth Cohorts: Evidence from 10 Years of the UK Household Longitudinal Study. International Journal of Environmental Research and Public Health. 2022; 19(3):1531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031531
Chicago/Turabian StyleMak, Hei Wan, Rory Coulter, and Daisy Fancourt. 2022. "Relationships between Volunteering, Neighbourhood Deprivation and Mental Wellbeing across Four British Birth Cohorts: Evidence from 10 Years of the UK Household Longitudinal Study" International Journal of Environmental Research and Public Health 19, no. 3: 1531. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19031531