
Differential Metabolites and Metabolic Pathways Involved in Aerobic Exercise Improvement of Chronic Fatigue Symptoms in Adolescents Based on Gas Chromatography–Mass Spectrometry



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Exercise Intervention Program
- (1)
- Warm-up phase: Active movement of the six major joints and jogging for 5 min with a heart rate no higher than 55% HRmax (HRmax = [(220-age) × 55%]).
- (2)
- Aerobic running phase: Under the guidance of the physical education teacher, the participants gradually increased their speed so that they reached the prescribed exercise intensity of 55~65% HRmax (HRmax = [(220-age) × 55~75%]) within 10 min, and all subjects maintained this exercise intensity for 20 min. If the subjects could not complete 20 min continuously, they were given rest time until they reached 20 min cumulatively (except in the case of discomfort or injury).
- (3)
- Relaxation phase: Subjects performed 10 min of slow walking or stretching activities.
2.3. Fatigue Level Measurement
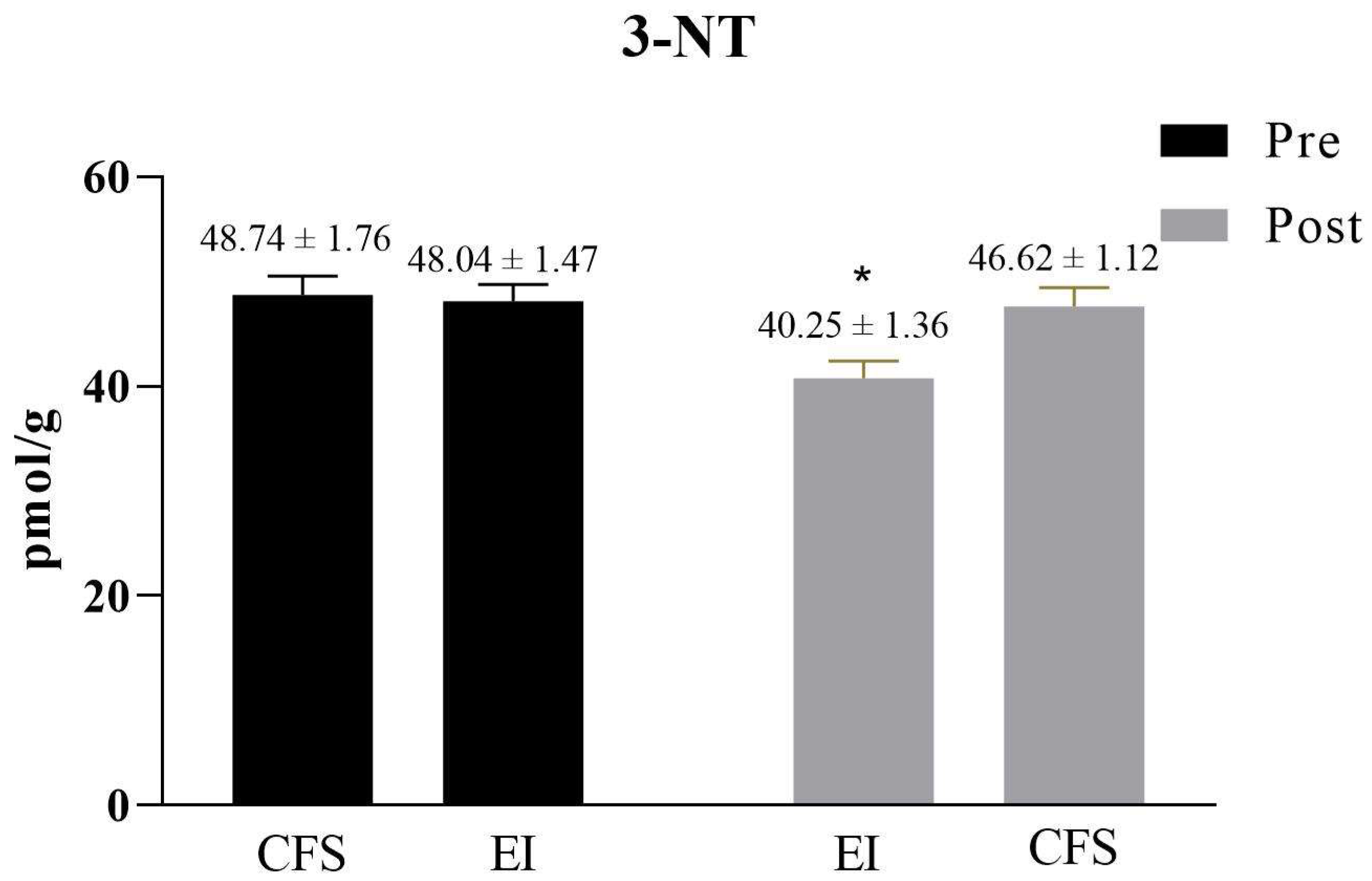
2.4. Oxidation Level Detection
2.4.1. Sample Handling
2.4.2. Protein Standard Curve and Total Protein Assay
2.4.3. Separation of Proteins
2.5. Metabonomics Analysis
2.5.1. Urine Sample Collection and Extraction of Metabolites
2.5.2. GC-TOF-MS Analysis
2.5.3. Metabolomics Data Pre-Processing
2.5.4. Multivariate Pattern Recognition Analysis
2.6. Statistical Analysis
3. Results
3.1. Comparison of General Information
3.2. The Efficacy of Exercise Intervention
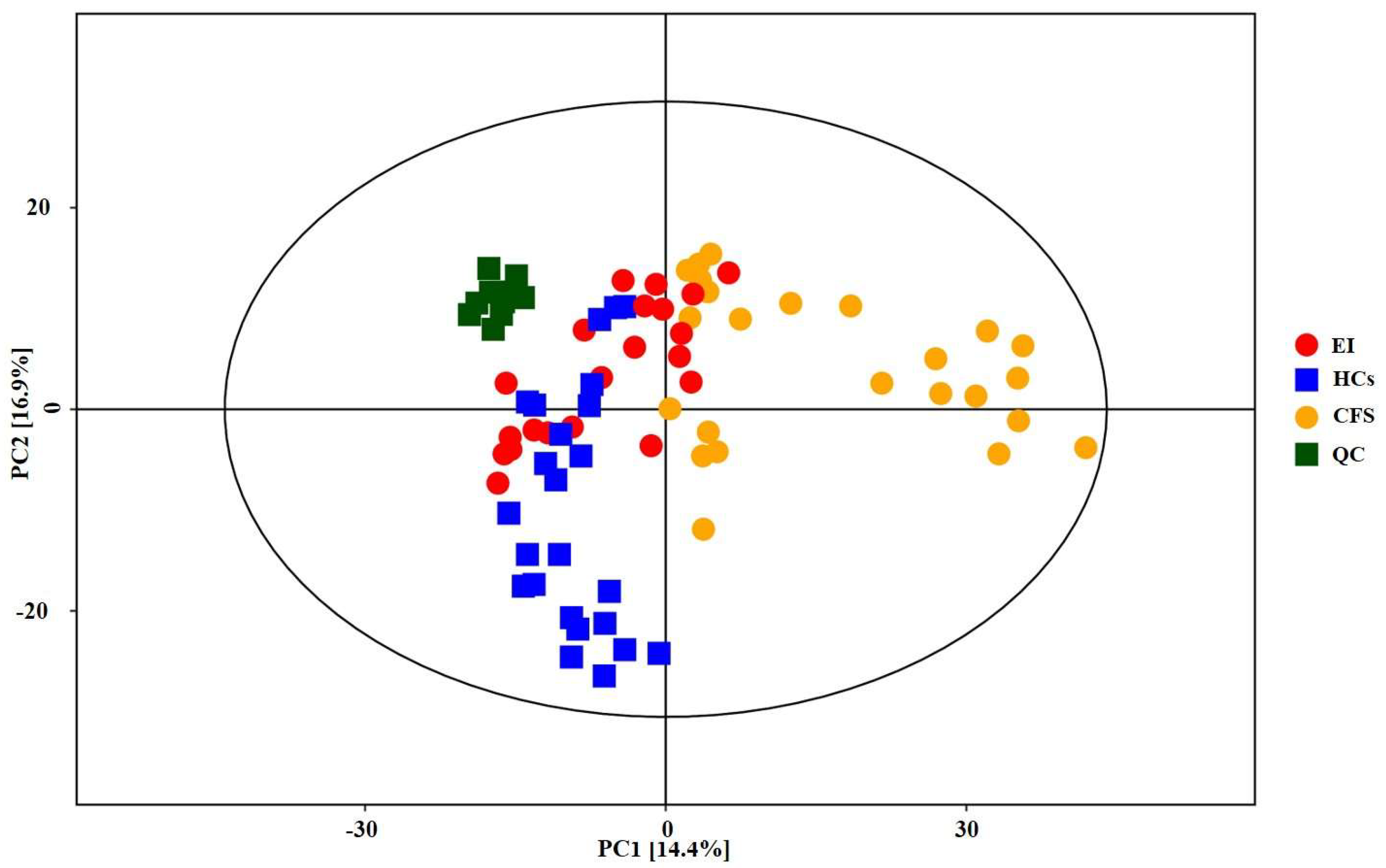
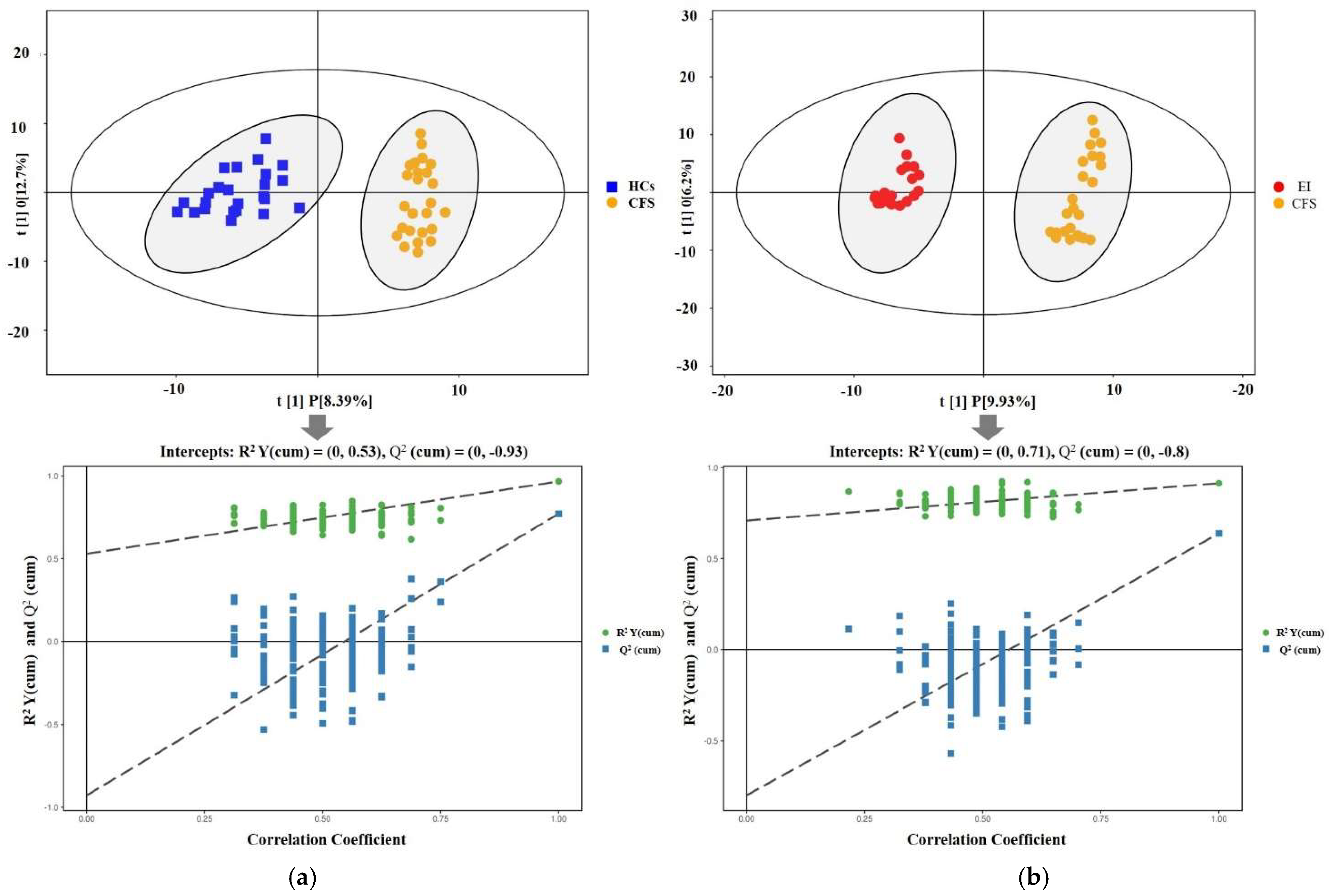
3.3. Multivariate Data Analysis Results
3.4. Differential Metabolite Results
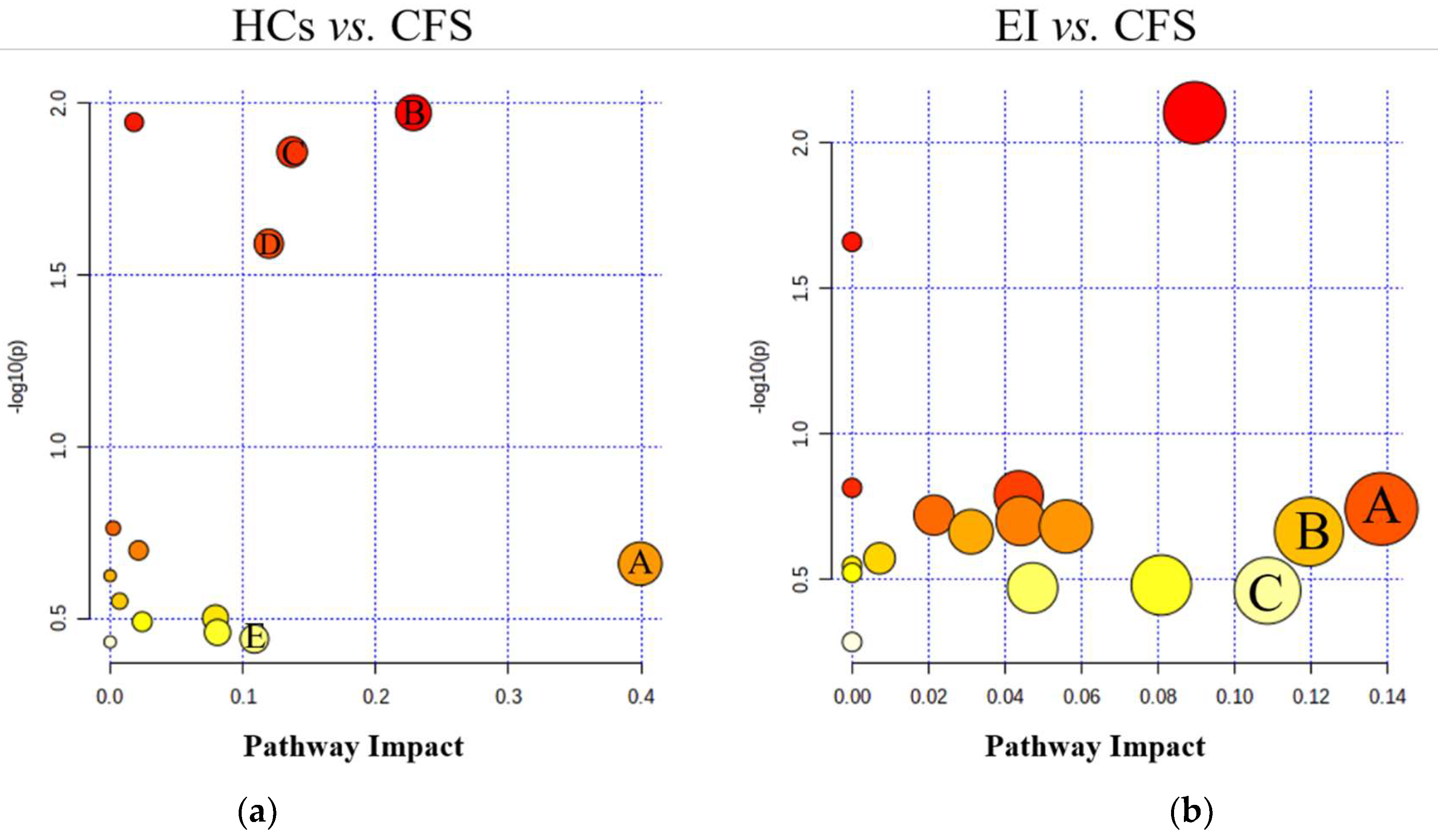
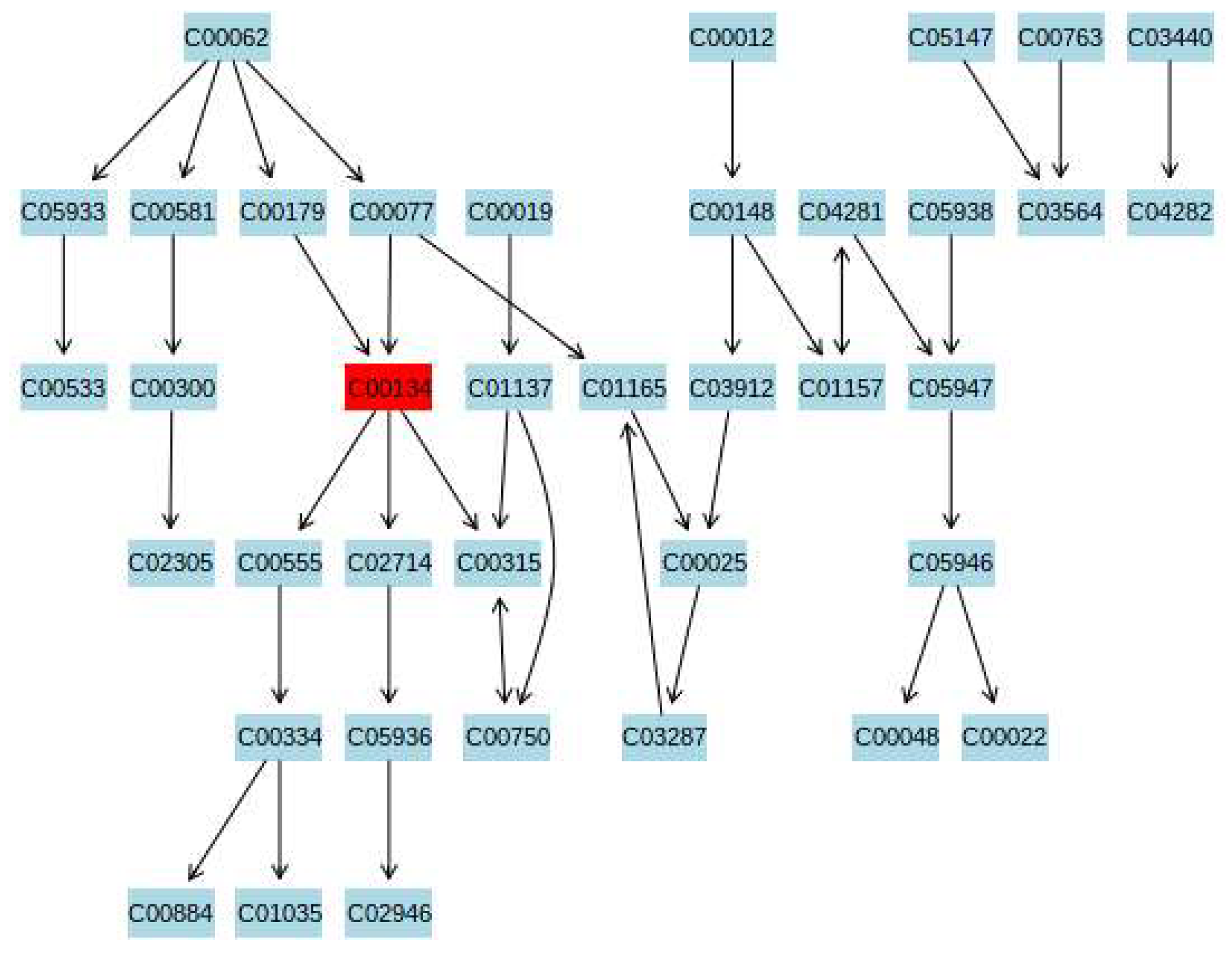
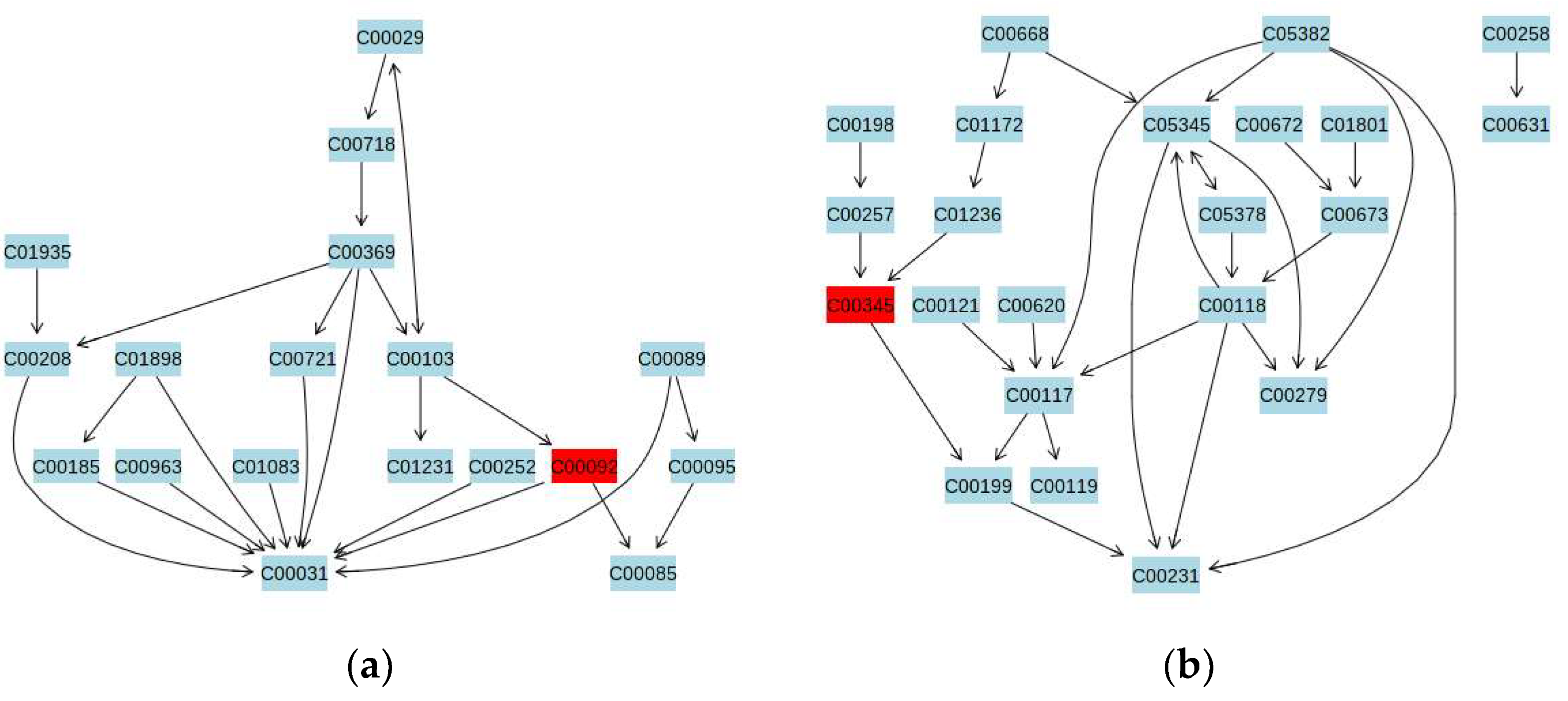
3.5. Metabolic Pathway Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnston, S.; Brenu, E.W.; Staines, D.; Marshall-Gradisnik, S. The prevalence of chronic fatigue syndrome/myalgic encephalomyelitis: A meta-analysis. Clin. Epidemiol. 2013, 5, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. American ME and CFS Society. How Many People Have ME/CFS? U.S. American ME and CFS Society: Whately, MA, USA, 2019. [Google Scholar]
- Chalder, T.; Goodman, R.; Wessely, S.; Hotopf, M.; Meltzer, H. Epidemiology of chronic fatigue syndrome and self reported myalgic encephalomyelitis in 5–15 year olds: Cross sectional study. BMJ 2003, 327, 654–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bell, D.S.; Jordan, K.; Robinson, M. Thirteen-year follow-up of children and adolescents with chronic fatigue syndrome. Pediatrics 2001, 107, 994–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van de Putte, E.M.; Uiterwaal, C.S.; Bots, M.L.; Kuis, W.; Kimpen, J.L.; Engelbert, R.H. Is chronic fatigue syndrome a connective tissue disorder? A cross-sectional study in adolescents. Pediatrics 2005, 115, e415–e422. [Google Scholar] [CrossRef] [Green Version]
- Lloyd, S.; Chalder, T.; Sallis, H.M.; Rimes, K.A. Telephone-based guided self-help for adolescents with chronic fatigue syndrome: A non-randomised cohort study. Behav. Res. Ther. 2012, 50, 304–312. [Google Scholar] [CrossRef]
- Rimes, K.A.; Goodman, R.; Hotopf, M.; Wessely, S.; Meltzer, H.; Chalder, T. Incidence, prognosis, and risk factors for fatigue and chronic fatigue syndrome in adolescents: A prospective community study. Pediatrics 2007, 119, e603–e609. [Google Scholar] [CrossRef] [Green Version]
- Kawatani, J.; Mizuno, K.; Shiraishi, S.; Takao, M.; Joudoi, T.; Fukuda, S.; Watanabe, Y.; Tomoda, A. Cognitive dysfunction and mental fatigue in childhood chronic fatigue syndrome-A 6-month follow-up study. Brain Dev. 2011, 33, 832–841. [Google Scholar] [CrossRef]
- Crawley, E.; Sterne, J.A. Association between school absence and physical function in paediatric chronic fatigue syndrome/myalgic encephalopathy. Arch. Dis. Child. 2009, 94, 752–756. [Google Scholar] [CrossRef]
- Nijhof, S.L.; Maijer, K.; Bleijenberg, G.; Uiterwaal, C.S.; Kimpen, J.L.; van de Putte, E.M. Adolescent chronic fatigue syndrome: Prevalence, incidence, and morbidity. Pediatrics 2011, 127, e1169–e1175. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.A.; Patel, D.R.; Darmawan, D. Participation in sports in relation to adolescent growth and development. Transl. Pediatr. 2017, 6, 150–159. [Google Scholar] [CrossRef] [Green Version]
- Larun, L.; Brurberg, K.G.; Odgaard-Jensen, J.; Price, J.R. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst. Rev. 2017, 4, Cd003200. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, M.; Kesten, O. An empirical evaluation of Chinese college admissions reforms through a natural experiment. Proc. Natl. Acad. Sci. USA 2020, 117, 31696–31705. [Google Scholar] [CrossRef] [PubMed]
- Bhurosy, T.; Thiagarajah, K. Are Eating Habits Associated with Adequate Sleep among High School Students? J. Sch. Health 2020, 90, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Shen, J.; Xie, J.; Zhi, J.; Xu, Y. Chronic fatigue syndrome in Chinese middle-school students. Medicine (Baltimore) 2018, 97, e9716. [Google Scholar] [CrossRef] [PubMed]
- Loew, S.J.; Marsh, N.V.; Watson, K. Symptoms of Meares-Irlen/Visual Stress Syndrome in subjects diagnosed with Chronic Fatigue Syndrome. Int. J. Clin. Health Psychol. 2014, 14, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Kindlon, T. Educational programs for chronic fatigue syndrome need to take cognizance of the condition’s abnormal response to exercise. Arch. Phys. Med. Rehabil. 2011, 92, 1015–1016. [Google Scholar] [CrossRef]
- Joyce, J.; Hotopf, M.; Wessely, S. The prognosis of chronic fatigue and chronic fatigue syndrome: A systematic review. QJM 1997, 90, 223–233. [Google Scholar] [CrossRef] [Green Version]
- Deale, A.; Husain, K.; Chalder, T.; Wessely, S. Long-term outcome of cognitive behavior therapy versus relaxation therapy for chronic fatigue syndrome: A 5-year follow-up study. Am. J. Psychiatry 2001, 158, 2038–2042. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Xu, C.; Pan, K.; Xiong, H. Acupuncture and moxibustion for chronic fatigue syndrome in traditional Chinese medicine: A systematic review and meta-analysis. BMC Complement. Altern. Med. 2017, 17, 163. [Google Scholar] [CrossRef] [Green Version]
- Larun, L.; Brurberg, K.G.; Odgaard-Jensen, J.; Price, J.R. Exercise therapy for chronic fatigue syndrome. Cochrane Database Syst. Rev. 2019, 10, Cd003200. [Google Scholar] [CrossRef]
- White, P.D.; Goldsmith, K.A.; Johnson, A.L.; Potts, L.; Walwyn, R.; DeCesare, J.C.; Baber, H.L.; Burgess, M.; Clark, L.V.; Cox, D.L.; et al. Comparison of adaptive pacing therapy, cognitive behaviour therapy, graded exercise therapy, and specialist medical care for chronic fatigue syndrome (PACE): A randomised trial. Lancet 2011, 377, 823–836. [Google Scholar] [CrossRef] [Green Version]
- Van Cauwenbergh, D.; De Kooning, M.; Ickmans, K.; Nijs, J. How to exercise people with chronic fatigue syndrome: Evidence-based practice guidelines. Eur. J. Clin. Investig. 2012, 42, 1136–1144. [Google Scholar] [CrossRef] [PubMed]
- Busch, A.J.; Webber, S.C.; Brachaniec, M.; Bidonde, J.; Bello-Haas, V.D.; Danyliw, A.D.; Overend, T.J.; Richards, R.S.; Sawant, A.; Schachter, C.L. Exercise therapy for fibromyalgia. Curr. Pain Headache Rep. 2011, 15, 358–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wallman, K.E.; Morton, A.R.; Goodman, C.; Grove, R. Exercise prescription for individuals with chronic fatigue syndrome. Med. J. Aust. 2005, 183, 142–143. [Google Scholar] [CrossRef]
- Deale, A.; Chalder, T.; Marks, I.; Wessely, S. Cognitive behavior therapy for chronic fatigue syndrome: A randomized controlled trial. Am. J. Psychiatry 1997, 154, 408–414. [Google Scholar] [CrossRef] [Green Version]
- Wallman, K.E.; Morton, A.R.; Goodman, C.; Grove, R.; Guilfoyle, A.M. Randomised controlled trial of graded exercise in chronic fatigue syndrome. Med. J. Aust. 2004, 180, 444–448. [Google Scholar] [CrossRef]
- Wearden, A.J.; Dowrick, C.; Chew-Graham, C.; Bentall, R.P.; Morriss, R.K.; Peters, S.; Riste, L.; Richardson, G.; Lovell, K.; Dunn, G. Nurse led, home based self help treatment for patients in primary care with chronic fatigue syndrome: Randomised controlled trial. BMJ 2010, 340, c1777. [Google Scholar] [CrossRef] [Green Version]
- Moss-Morris, R.; Sharon, C.; Tobin, R.; Baldi, J.C. A randomized controlled graded exercise trial for chronic fatigue syndrome: Outcomes and mechanisms of change. J. Health Psychol. 2005, 10, 245–259. [Google Scholar] [CrossRef]
- Jason, L.A.; Torres-Harding, S.; Friedberg, F.; Corradi, K.; Njoku, M.G.; Donalek, J.; Reynolds, N.; Brown, M.; Weitner, B.B.; Rademaker, A.; et al. Non-pharmacologic Interventions for CFS: A Randomized Trial. J. Clin. Psychol. Med. Settings 2007, 14, 275–296. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef]
- Bested, A.C.; Marshall, L.M. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: An evidence-based approach to diagnosis and management by clinicians. Rev. Environ. Health 2015, 30, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Holmes, G.P.; Kaplan, J.E.; Gantz, N.M.; Komaroff, A.L.; Schonberger, L.B.; Straus, S.E.; Jones, J.F.; Dubois, R.E.; Cunningham-Rundles, C.; Pahwa, S.; et al. Chronic fatigue syndrome: A working case definition. Ann. Intern. Med. 1988, 108, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Montoya, J.G.; Holmes, T.H.; Anderson, J.N.; Maecker, H.T.; Rosenberg-Hasson, Y.; Valencia, I.J.; Chu, L.; Younger, J.W.; Tato, C.M.; Davis, M.M. Cytokine signature associated with disease severity in chronic fatigue syndrome patients. Proc. Natl. Acad. Sci. USA 2017, 114, E7150–E7158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giloteaux, L.; Goodrich, J.K.; Walters, W.A.; Levine, S.M.; Ley, R.E.; Hanson, M.R. Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome 2016, 4, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esfandyarpour, R.; Kashi, A.; Nemat-Gorgani, M.; Wilhelmy, J.; Davis, R.W. A nanoelectronics-blood-based diagnostic biomarker for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Proc. Natl. Acad. Sci. USA 2019, 116, 10250–10257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, A.; Kang, C.; Zhang, Y.; Tang, L.; Guo, H.; Li, H.; Zhang, K. Immunomodulating and antioxidant effects of polysaccharide conjugates from the fruits of Ziziphus Jujube on Chronic Fatigue Syndrome rats. Carbohydr. Polym. 2015, 122, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Lakshmi Priya, M.D.; Geetha, A. A biochemical study on the level of proteins and their percentage of nitration in the hair and nail of autistic children. Clin. Chim. Acta 2011, 412, 1036–1042. [Google Scholar] [CrossRef]
- Bandookwala, M.; Sengupta, P. 3-Nitrotyrosine: A versatile oxidative stress biomarker for major neurodegenerative diseases. Int. J. Neurosci. 2020, 130, 1047–1062. [Google Scholar] [CrossRef]
- Maes, M.; Kubera, M.; Uytterhoeven, M.; Vrydags, N.; Bosmans, E. Increased plasma peroxides as a marker of oxidative stress in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Med. Sci. Monit. 2011, 17, Sc11–Sc15. [Google Scholar] [CrossRef] [Green Version]
- Morris, G.; Maes, M. Oxidative and Nitrosative Stress and Immune-Inflammatory Pathways in Patients with Myalgic Encephalomyelitis (ME)/Chronic Fatigue Syndrome (CFS). Curr. Neuropharmacol. 2014, 12, 168–185. [Google Scholar] [CrossRef] [Green Version]
- Godlewska, B.R.; Williams, S.; Emir, U.E.; Chen, C.; Sharpley, A.L.; Goncalves, A.J.; Andersson, M.I.; Clarke, W.; Angus, B.; Cowen, P.J. Neurochemical abnormalities in chronic fatigue syndrome: A pilot magnetic resonance spectroscopy study at 7 Tesla. Psychopharmacology 2022, 239, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Lowder, T.; Padgett, D.A.; Woods, J.A. Moderate exercise protects mice from death due to influenza virus. Brain Behav. Immun. 2005, 19, 377–380. [Google Scholar] [CrossRef] [PubMed]
- Vidali, S.; Aminzadeh, S.; Lambert, B.; Rutherford, T.; Sperl, W.; Kofler, B.; Feichtinger, R.G. Mitochondria: The ketogenic diet--A metabolism-based therapy. Int. J. Biochem. Cell Biol. 2015, 63, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Czerska, M.; Mikołajewska, K.; Zieliński, M.; Gromadzińska, J.; Wąsowicz, W. Today’s oxidative stress markers. Med. Pr. 2015, 66, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Wu, Y.; Liu, T.; Li, R.; Xie, M. Serotonin regulation in a rat model of exercise-induced chronic fatigue. Neuroscience 2017, 349, 27–34. [Google Scholar] [CrossRef]
- Shao, C.; Ren, Y.; Wang, Z.; Kang, C.; Jiang, H.; Chi, A. Detection of Urine Metabolites in a Rat Model of Chronic Fatigue Syndrome before and after Exercise. BioMed Res. Int. 2017, 2017, 8182020. [Google Scholar] [CrossRef]
- Leal, D.V.; Taylor, L.; Hough, J. Exercise-Induced Salivary Hormone Responses to High-Intensity, Self-Paced Running. Int. J. Sports Physiol. Perform. 2021, 16, 1319–1327. [Google Scholar] [CrossRef]
- Lindon, J.C.; Holmes, E.; Bollard, M.E.; Stanley, E.G.; Nicholson, J.K. Metabonomics technologies and their applications in physiological monitoring, drug safety assessment and disease diagnosis. Biomarkers 2004, 9, 1–31. [Google Scholar] [CrossRef]
- Oresta, B.; Braga, D.; Lazzeri, M.; Frego, N.; Saita, A.; Faccani, C.; Fasulo, V.; Colombo, P.; Guazzoni, G.; Hurle, R.; et al. The Microbiome of Catheter Collected Urine in Males with Bladder Cancer According to Disease Stage. J. Urol. 2021, 205, 86–93. [Google Scholar] [CrossRef]
- Wu, Z.; Zhao, P.; Long, Z.; Li, J.; Yang, G.; Zhang, Q.; Duan, G.; Li, H. Biomarker screening for antenatal depression in women who underwent caesarean section: A matched observational study with plasma Lipidomics. BMC Psychiatry 2019, 19, 259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, J.; Song, S.L.; Castro-Perez, J.; Plumb, R.S.; Xu, G.W. Metabonomics and its applications. Sheng Wu Gong Cheng Xue Bao 2005, 21, 1–5. [Google Scholar] [PubMed]
- Markley, J.L.; Brüschweiler, R.; Edison, A.S.; Eghbalnia, H.R.; Powers, R.; Raftery, D.; Wishart, D.S. The future of NMR-based metabolomics. Curr. Opin. Biotechnol. 2017, 43, 34–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadimitropoulos, M.P.; Vasilopoulou, C.G.; Maga-Nteve, C.; Klapa, M.I. Untargeted GC-MS Metabolomics. Methods Mol. Biol. 2018, 1738, 133–147. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, K.; Straus, S.E.; Hickie, I.; Sharpe, M.C.; Dobbins, J.G.; Komaroff, A. The chronic fatigue syndrome: A comprehensive approach to its definition and study. International Chronic Fatigue Syndrome Study Group. Ann. Intern. Med. 1994, 121, 953–959. [Google Scholar] [CrossRef]
- Chalder, T.; Berelowitz, G.; Pawlikowska, T.; Watts, L.; Wessely, S.; Wright, D.; Wallace, E.P. Development of a fatigue scale. J. Psychosom. Res. 1993, 37, 147–153. [Google Scholar] [CrossRef] [Green Version]
- Zhan, Y.X.; Zhao, S.Y.; Yuan, J.; Liu, H.; Liu, Y.F.; Gui, L.L.; Zheng, H.; Zhou, Y.M.; Qiu, L.H.; Chen, J.H.; et al. Prevalence and Influencing Factors on Fatigue of First-line Nurses Combating with COVID-19 in China: A Descriptive Cross-Sectional Study. Curr. Med. Sci. 2020, 40, 625–635. [Google Scholar] [CrossRef]
- Walsh, M.C.; Brennan, L.; Malthouse, J.P.; Roche, H.M.; Gibney, M.J. Effect of acute dietary standardization on the urinary, plasma, and salivary metabolomic profiles of healthy humans. Am. J. Clin. Nutr. 2006, 84, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Dunn, W.B.; Broadhurst, D.; Begley, P.; Zelena, E.; Francis-McIntyre, S.; Anderson, N.; Brown, M.; Knowles, J.D.; Halsall, A.; Haselden, J.N.; et al. Procedures for large-scale metabolic profiling of serum and plasma using gas chromatography and liquid chromatography coupled to mass spectrometry. Nat. Protoc. 2011, 6, 1060–1083. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. 3), 1–72. [Google Scholar] [CrossRef] [Green Version]
- Marzetti, E.; Calvani, R.; Tosato, M.; Cesari, M.; Di Bari, M.; Cherubini, A.; Broccatelli, M.; Savera, G.; D’Elia, M.; Pahor, M.; et al. Physical activity and exercise as countermeasures to physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 35–42. [Google Scholar] [CrossRef]
- Capodaglio, E.M. Physical activity, tool for the prevention and management of chronic diseases (Attività fisica, strumento di prevenzione e gestione delle malattie croniche). G. Ital. Med. Lav. Ergon. 2018, 40, 106–119. [Google Scholar] [PubMed]
- Cheshire, A.; Ridge, D.; Clark, L.; White, P. Guided graded Exercise Self-help for chronic fatigue syndrome: Patient experiences and perceptions. Disabil. Rehabil. 2020, 42, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Clark, L.V.; McCrone, P.; Ridge, D.; Cheshire, A.; Vergara-Williamson, M.; Pesola, F.; White, P.D. Graded Exercise Therapy Guided Self-Help Trial for Patients with Chronic Fatigue Syndrome (GETSET): Protocol for a Randomized Controlled Trial and Interview Study. JMIR Res. Protoc. 2016, 5, e70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fulcher, K.Y.; White, P.D. Randomised controlled trial of graded exercise in patients with the chronic fatigue syndrome. BMJ 1997, 314, 1647–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salmon, P. Effects of physical exercise on anxiety, depression, and sensitivity to stress: A unifying theory. Clin. Psychol. Rev. 2001, 21, 33–61. [Google Scholar] [CrossRef]
- Yancey, J.R.; Thomas, S.M. Chronic fatigue syndrome: Diagnosis and treatment. Am. Fam. Physician 2012, 86, 741–746. [Google Scholar]
- Lim, S.; Choi, S.H.; Jeong, I.K.; Kim, J.H.; Moon, M.K.; Park, K.S.; Lee, H.K.; Kim, Y.B.; Jang, H.C. Insulin-sensitizing effects of exercise on adiponectin and retinol-binding protein-4 concentrations in young and middle-aged women. J. Clin. Endocrinol. Metab. 2008, 93, 2263–2268. [Google Scholar] [CrossRef] [Green Version]
- Brkić, S.; Tomić, S.; Ruzić, M.; Marić, D. Chronic fatigue syndrome. Srp. Arh. Celok. Lek. 2011, 139, 256–261. [Google Scholar] [CrossRef]
- Chand, S.P.; Kuckel, D.P.; Huecker, M.R. Cognitive Behavior Therapy. In StatPearls; StatPearls Publishing Copyright© 2021; StatPearls Publishing LLC: St. Petersburg, FL, USA, 2021. [Google Scholar]
- Eulenburg, V.; Armsen, W.; Betz, H.; Gomeza, J. Glycine transporters: Essential regulators of neurotransmission. Trends Biochem. Sci. 2005, 30, 325–333. [Google Scholar] [CrossRef]
- Kopple, J.D. Phenylalanine and tyrosine metabolism in chronic kidney failure. J. Nutr. 2007, 137 (Suppl. 1), 1586S–1590S; Discussion 1597S–1598S. [Google Scholar] [CrossRef]
- Bahri, S.; Zerrouk, N.; Aussel, C.; Moinard, C.; Crenn, P.; Curis, E.; Chaumeil, J.C.; Cynober, L.; Sfar, S. Citrulline: From metabolism to therapeutic use. Nutrition 2013, 29, 479–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rashid, J.; Kumar, S.S.; Job, K.M.; Liu, X.; Fike, C.D.; Sherwin, C.M.T. Therapeutic Potential of Citrulline as an Arginine Supplement: A Clinical Pharmacology Review. Paediatr. Drugs 2020, 22, 279–293. [Google Scholar] [CrossRef]
- Janssen-Heininger, Y.M.; Persinger, R.L.; Korn, S.H.; Pantano, C.; McElhinney, B.; Reynaert, N.L.; Langen, R.C.; Ckless, K.; Shrivastava, P.; Poynter, M.E. Reactive nitrogen species and cell signaling: Implications for death or survival of lung epithelium. Am. J. Respir. Crit. Care Med. 2002, 166 Pt 2, S9–S16. [Google Scholar] [CrossRef] [PubMed]
- Trinity, J.D.; Broxterman, R.M.; Richardson, R.S. Regulation of exercise blood flow: Role of free radicals. Free Radic. Biol. Med. 2016, 98, 90–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, J.; Druhan, L.J.; Zweier, J.L. Reactive oxygen and nitrogen species regulate inducible nitric oxide synthase function shifting the balance of nitric oxide and superoxide production. Arch. Biochem. Biophys. 2010, 494, 130–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fukuda, S.; Nojima, J.; Motoki, Y.; Yamaguti, K.; Nakatomi, Y.; Okawa, N.; Fujiwara, K.; Watanabe, Y.; Kuratsune, H. A potential biomarker for fatigue: Oxidative stress and anti-oxidative activity. Biol. Psychol. 2016, 118, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Wawrzyniak, N.R.; Joseph, A.M.; Levin, D.G.; Gundermann, D.M.; Leeuwenburgh, C.; Sandesara, B.; Manini, T.M.; Adhihetty, P.J. Idiopathic chronic fatigue in older adults is linked to impaired mitochondrial content and biogenesis signaling in skeletal muscle. Oncotarget 2016, 7, 52695–52709. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, G.; Spence, V.A.; McLaren, M.; Hill, A.; Underwood, C.; Belch, J.J. Oxidative stress levels are raised in chronic fatigue syndrome and are associated with clinical symptoms. Free Radic. Biol. Med. 2005, 39, 584–589. [Google Scholar] [CrossRef]
- Garatachea, N.; Pareja-Galeano, H.; Sanchis-Gomar, F.; Santos-Lozano, A.; Fiuza-Luces, C.; Morán, M.; Emanuele, E.; Joyner, M.J.; Lucia, A. Exercise attenuates the major hallmarks of aging. Rejuvenation Res. 2015, 18, 57–89. [Google Scholar] [CrossRef] [Green Version]
- Korsager Larsen, M.; Matchkov, V.V. Hypertension and physical exercise: The role of oxidative stress. Medicina (Kaunas) 2016, 52, 19–27. [Google Scholar] [CrossRef]
- Viña, J.; Gomez-Cabrera, M.C.; Lloret, A.; Marquez, R.; Miñana, J.B.; Pallardó, F.V.; Sastre, J. Free radicals in exhaustive physical exercise: Mechanism of production, and protection by antioxidants. IUBMB Life 2000, 50, 271–277. [Google Scholar] [CrossRef] [PubMed]
- Yol, Y.; Turgay, F.; Yigittürk, O.; Aşıkovalı, S.; Durmaz, B. The effects of regular aerobic exercise training on blood nitric oxide levels and oxidized LDL and the role of eNOS intron 4a/b polymorphism. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165913. [Google Scholar] [CrossRef]
- Yao, W.; Li, H.; Liu, Q.; Gao, Y.; Dai, J.; Bao, B.; Zhang, L.; Ding, A. Cellular Metabolomics Revealed the Cytoprotection of Amentoflavone, a Natural Compound, in Lipopolysaccharide-Induced Injury of Human Umbilical Vein Endothelial Cells. Int. J. Mol. Sci. 2016, 17, 1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.; Jin, Y.; Yang, Y.; Wu, Z.; Wu, G. Epithelial Dysfunction in Lung Diseases: Effects of Amino Acids and Potential Mechanisms. Adv. Exp. Med. Biol. 2020, 1265, 57–70. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhang, H. Reprogramming of glucose, fatty acid and amino acid metabolism for cancer progression. Cell Mol. Life Sci. 2016, 73, 377–392. [Google Scholar] [CrossRef] [PubMed]
- Gray, L.R.; Tompkins, S.C.; Taylor, E.B. Regulation of pyruvate metabolism and human disease. Cell Mol. Life Sci. 2014, 71, 2577–2604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCommis, K.S.; Finck, B.N. Mitochondrial pyruvate transport: A historical perspective and future research directions. Biochem. J. 2015, 466, 443–454. [Google Scholar] [CrossRef] [Green Version]
- Baklund, I.H.; Dammen, T.; Moum, T.; Kristiansen, W.; Duarte, D.S.; Castro-Marrero, J.; Helland, I.B.; Strand, E.B. Evaluating Routine Blood Tests According to Clinical Symptoms and Diagnostic Criteria in Individuals with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Clin. Med. 2021, 10, 3105. [Google Scholar] [CrossRef]
- Whiteside, T.L.; Friberg, D. Natural killer cells and natural killer cell activity in chronic fatigue syndrome. Am. J. Med. 1998, 105, 27s–34s. [Google Scholar] [CrossRef]
- Glaser, R.; Kiecolt-Glaser, J.K. Stress-associated immune modulation: Relevance to viral infections and chronic fatigue syndrome. Am. J. Med. 1998, 105, 35s–42s. [Google Scholar] [CrossRef]
- Petersen, K.F.; Dufour, S.; Cline, G.W.; Shulman, G.I. Regulation of hepatic mitochondrial oxidation by glucose-alanine cycling during starvation in humans. J. Clin. Investig. 2019, 129, 4671–4675. [Google Scholar] [CrossRef]
- Sandler, C.X.; Lloyd, A.R. Chronic fatigue syndrome: Progress and possibilities. Med. J. Aust. 2020, 212, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Bjørklund, G.; Dadar, M.; Pen, J.J.; Chirumbolo, S.; Aaseth, J. Chronic fatigue syndrome (CFS): Suggestions for a nutritional treatment in the therapeutic approach. Biomed. Pharmacother. 2019, 109, 1000–1007. [Google Scholar] [CrossRef] [PubMed]
- Fernie, A.R.; Carrari, F.; Sweetlove, L.J. Respiratory metabolism: Glycolysis, the TCA cycle and mitochondrial electron transport. Curr. Opin. Plant Biol. 2004, 7, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Stincone, A.; Prigione, A.; Cramer, T.; Wamelink, M.M.; Campbell, K.; Cheung, E.; Olin-Sandoval, V.; Grüning, N.M.; Krüger, A.; Tauqeer Alam, M.; et al. The return of metabolism: Biochemistry and physiology of the pentose phosphate pathway. Biol. Rev. Camb. Philos. Soc. 2015, 90, 927–963. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | CFS (n = 23) | EI (n = 23) | HCs (n = 24) |
|---|---|---|---|
| Age, years | 16.72 ± 0.41 | 16.57 ± 0.28 | 16.42 ± 0.74 |
| Height, cm | 176.30 ± 1.37 | 174.50 ± 1.24 | 176.50 ± 1.47 |
| Weight, kg | 71.46 ± 1.73 | 69.24 ± 2.41 | 68.65 ± 3.58 |
| BMI, kg/m2 | 22.25 ± 1.12 | 22.46 ± 1.31 | 22.92 ± 0.60 |
| Baseline | 12 Weeks | |||
|---|---|---|---|---|
| EI | CFS | CFS | EI | |
| Total fatigue score | 10.72 ± 0.14 | 10.14 ± 0.14 | 8.46 ±0.16 | 4.36 ± 0.16 ***### |
| Physical fatigue score | 5.18 ± 0.12 | 5.05 ± 0.18 | 4.41 ± 0.22 | 2.13 ± 0.15 ***### |
| Mental fatigue score | 5.22 ± 0.18 | 5.09 ± 0.12 | 4.05 ± 0.15 | 2.22 ± 0.22 ***### |
| Metabolite | HMDB ID | RT (min) | m/z | VIP | p-Value | FC |
|---|---|---|---|---|---|---|
| Uric acid | HMDB0000289 | 20.02 | 55 | 3.17 | 0.00001 | 3.35 |
| D-Glyceric acid | HMDB0000139 | 11.34 | 71 | 1.36 | 0.01121 | 2.00 |
| Lactose | HMDB0041627 | 24.98 | 64 | 2.56 | 0.00001 | 2.68 |
| 4-hydroxyphenylacetic acid | HMDB0000020 | 15.31 | 179 | 2.3 | 0.00009 | 0.45 |
| N-Acetyl-L-glutamic acid | HMDB0001138 | 15.74 | 117 | 2.87 | 0.00000 | 8.47 |
| 3,4-Dihydroxyphenylacetic acid | HMDB0001336 | 17.36 | 179 | 2.68 | 0.00003 | 3.29 |
| N-Acetylglutamic acid | HMDB0001138 | 16.89 | 84 | 2.89 | 0.00000 | 2.91 |
| D-(glycerol 1-phosphate) | HMDB0000126 | 16.60 | 292 | 2.98 | 0.00000 | 5.61 |
| Inosine | HMDB0000195 | 23.99 | 230 | 1.26 | 0.00826 | 0.38 |
| Purine riboside | HMDB0029956 | 22.35 | 103 | 3.02 | 0.00000 | 5.36 |
| Beta-Alanine | HMDB0000056 | 12.57 | 174 | 2.06 | 0.00192 | 2.73 |
| 6-phosphogluconic acid | HMDB0001316 | 22.70 | 217 | 2.50 | 0.00014 | 5.47 |
| N-Carbamylglutamate | HMDB0015673 | 19.46 | 174 | 1.44 | 0.01197 | 0.36 |
| 4-Androsten-11beta-ol-3,17-dione | HMDB0006773 | 26.82 | 361 | 1.29 | 0.01217 | 0.32 |
| Adrenaline | HMDB0000068 | 17.57 | 267 | 2.84 | 0.00262 | 2.35 |
| L-Dithiothreitol | HMDB0013593 | 15.00 | 195 | 2.05 | 0.00057 | 0.03 |
| Citrulline | HMDB0000904 | 16.52 | 71 | 1.45 | 0.01879 | 1.52 |
| Putrescine | HMDB0001414 | 16.59 | 72 | 2.87 | 0.00000 | 2.50 |
| Elaidic acid | HMDB0000573 | 21.29 | 131 | 1.45 | 0.01773 | 1.52 |
| 2,2-Dimethylsuccinic Acid | HMDB0002074 | 11.27 | 71 | 2.70 | 0.00000 | 2.81 |
| Metabolite | HMDB ID | RT (min) | m/z | VIP | p-Value | FC |
|---|---|---|---|---|---|---|
| Oxalic acid | HMDB0002329 | 8.58 | 79 | 1.68 | 0.001044 | 0.76 |
| Cellobiose | HMDB0000055 | 24.96 | 79 | 1.00 | 0.014957 | 1.48 |
| Uric acid | HMDB0000289 | 20.02 | 55 | 1.90 | 0.000031 | 3.65 |
| Quinolinic acid | HMDB0000232 | 16.29 | 79 | 2.15 | 0.000772 | 0.63 |
| N-Acetylmannosamine | HMDB0001129 | 19.78 | 79 | 2.27 | 0.000533 | 0.64 |
| Lactose | HMDB0041627 | 24.98 | 38 | 2.38 | 0.000020 | 16.9 |
| Orotic acid | HMDB0000226 | 16.44 | 79 | 1.50 | 0.014485 | 0.74 |
| Glycerol 1-phosphate | HMDB0000126 | 16.60 | 46 | 2.23 | 0.009390 | 2.99 |
| L-Malic acid | HMDB0000156 | 13.42 | 76 | 1.05 | 0.035540 | 1.58 |
| Malonic acid | HMDB0000691 | 9.51 | 79 | 1.31 | 0.021348 | 1.36 |
| 3-Methylglutaric Acid | HMDB0000752 | 12.66 | 67 | 1.65 | 0.010768 | 0.62 |
| Purine riboside | HMDB0029956 | 22.35 | 48 | 2.97 | 0.000000 | 19.9 |
| Uridine | HMDB0000296 | 23.06 | 79 | 2.21 | 0.000191 | 0.72 |
| 6-phosphogluconic acid | HMDB0001316 | 22.70 | 32 | 1.97 | 0.002571 | 4.19 |
| 3-Hydroxypyridine acid | HMDB0013188 | 8.74 | 71 | 1.18 | 0.021134 | 1.62 |
| Citraconic acid | HMDB0000634 | 12.84 | 76 | 1.05 | 0.002329 | 0.65 |
| 5,6-dihydrouracil | HMDB0000076 | 15.10 | 41 | 1.08 | 0.028759 | 0.35 |
| Putrescine | HMDB0001414 | 21.95 | 57 | 2.11 | 0.000006 | 0.22 |
| Glucose-6-phosphate | HMDB0001401 | 23.43 | 39 | 1.74 | 0.018920 | 0.22 |
| 2,2-Dimethylsuccinic Acid | HMDB0002074 | 11.27 | 31 | 2.18 | 0.001279 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, S.; Chi, A.; Wan, B.; Liang, J. Differential Metabolites and Metabolic Pathways Involved in Aerobic Exercise Improvement of Chronic Fatigue Symptoms in Adolescents Based on Gas Chromatography–Mass Spectrometry. Int. J. Environ. Res. Public Health 2022, 19, 2377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042377
Zhao S, Chi A, Wan B, Liang J. Differential Metabolites and Metabolic Pathways Involved in Aerobic Exercise Improvement of Chronic Fatigue Symptoms in Adolescents Based on Gas Chromatography–Mass Spectrometry. International Journal of Environmental Research and Public Health. 2022; 19(4):2377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042377
Chicago/Turabian StyleZhao, Shanguang, Aiping Chi, Bingjun Wan, and Jian Liang. 2022. "Differential Metabolites and Metabolic Pathways Involved in Aerobic Exercise Improvement of Chronic Fatigue Symptoms in Adolescents Based on Gas Chromatography–Mass Spectrometry" International Journal of Environmental Research and Public Health 19, no. 4: 2377. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19042377