
Factors Associated with Regular Dental Checkups’ Discontinuation during the COVID-19 Pandemic: A Nationwide Cross-Sectional Web-Based Survey in Japan



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Survey Items
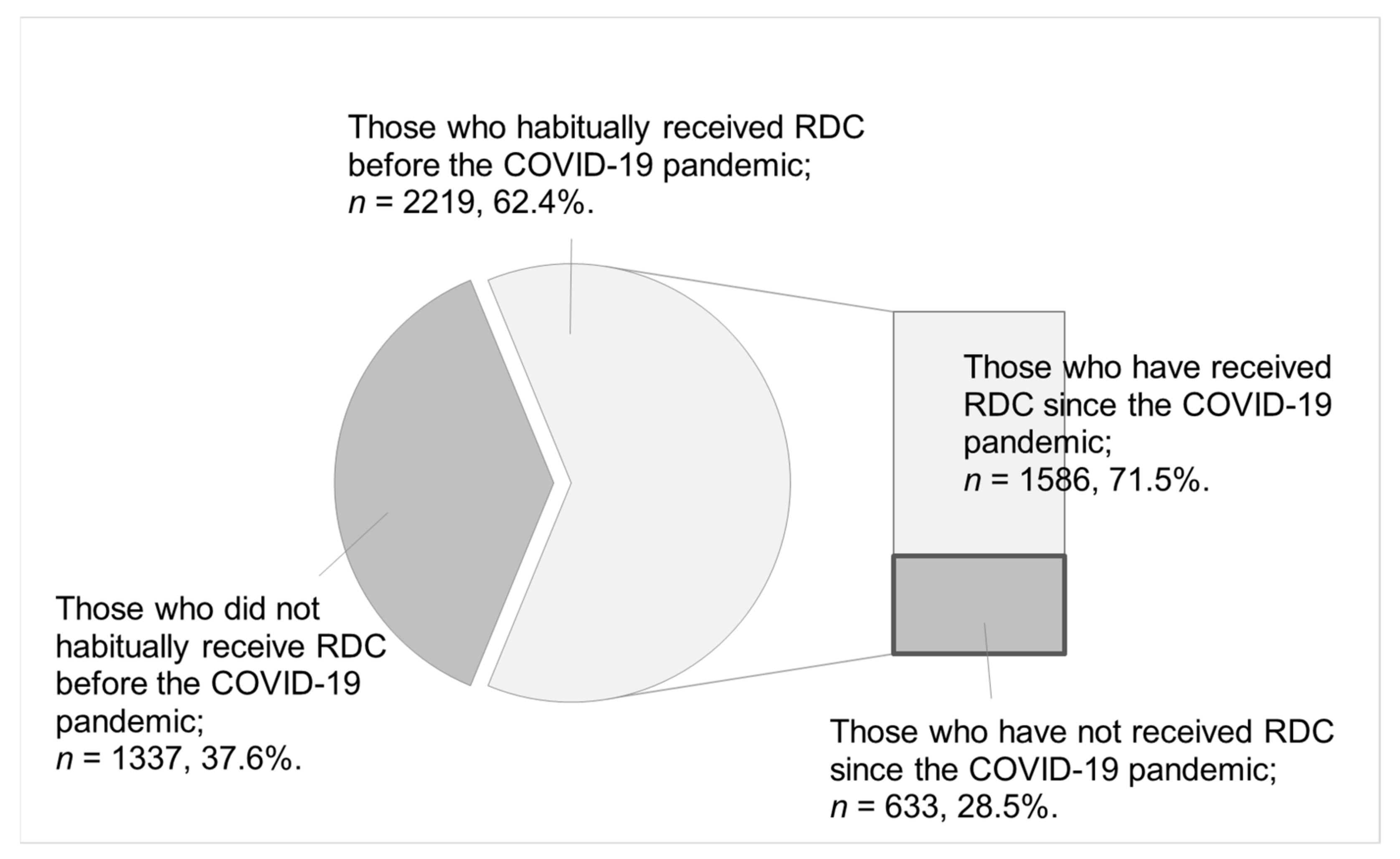
- We asked participants to select from the following four choices about changes in their receipt of RDCs before and after the COVID-19 pandemic: “I habitually received regular dental checkups before the COVID-19 pandemic, and I have received regular dental checkups since the pandemic”; “I habitually received regular dental checkups before the COVID-19 pandemic, but I have not received regular dental checkups since the pandemic”; “I did not habitually receive regular dental checkups before the COVID-19 pandemic, but I have received regular dental checkups since the pandemic”; “I did not habitually receive regular dental checkups before the COVID-19 pandemic, and I have not received regular dental checkups since the pandemic.” In this study, RDC was defined as “receiving at least one dental checkup during a year” [24].
- Individual socioeconomic factors included gender, age, household income, employment status, marital status, and residential municipality. Participants’ ages were categorized into six groups: 20s, 30s, 40s, 50s, 60s, and 70 and above. The household income of the participants was categorized into six groups: <2000 K JPY, 2000 K–< 4000 K JPY, 4000 K–< 6000 K JPY, 6000 K–< 8000 K JPY, ≥8000 K JPY, and unknown. (As of 2018, the average annual household income in Japan was 5523 K JPY, and the median value was 4370 K JPY. 1 K JPY = USD 9.1, September 2021 [25].) The participants’ employment status was categorized into five groups: regular employees, self-employed, homemakers, nonregular employees, and not working. Participants’ marital status was categorized as married or single. The municipalities where the participants lived were categorized into four, based on the Japanese municipal system: metropolis (ordinance-designated cities with a population of 500,000 or more, and 23 special wards of Tokyo), core cities (ordinance-designated cities with a population of 200,000 or more, excluding metropolises), cities (cities with a population of 50,000 or more, excluding metropolises and core cities), and towns and villages (small municipalities that do not meet city requirements).
- With regard to oral health status, we used data on the number of teeth and oral cleaning. The number of teeth was categorized into four groups: 0–9 teeth, 10–19 teeth, 20–27 teeth, and 28 or more teeth. Data on the number of teeth were obtained by questioning the participants. There are two ways to determine the number of teeth: a dentist’s examination or using a questionnaire, but there is no significant difference between the two methods [26,27]. Oral cleaning entails the number of times teeth are brushed per day and the habit of interdental cleaning.
2.3. Statistical Analysis
2.4. Ethical Consideration
3. Results
3.1. Status of Participants Receiving RDCs Owing to the COVID-19 Pandemic
3.2. Relationship between Receiving RDCs Owing to the COVID-19 Pandemic and the Study Participants’ Characteristics
3.3. Characteristics of Those Who Have Stopped Receiving RDCs since the COVID-19 Pandemic
4. Discussion
4.1. Main Findings
4.2. Influence on Receiving RDCs Due to the COVID-19 Pandemic and Implications of This Study
4.3. Relationship between Those Who Have Stopped Receiving RDCs since the COVID-19 Pandemic and Socioeconomic Factors
4.4. Relationship between Receiving RDCs and Oral Health Status
4.5. Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Thomson, W.M.; Williams, S.M.; Broadbent, J.; Poulton, R.; Locker, D. Long-term Dental Visiting Patterns and Adult Oral Health. J. Dent. Res. 2010, 89, 307–311. [Google Scholar] [CrossRef]
- Åstrøm, A.N.; Ekback, G.; Ordell, S.; Nasir, E. Long-term routine dental attendance: Influence on tooth loss and oral health-related quality of life in Swedish older adults. Community Dent. Oral Epidemiol. 2014, 42, 460–469. [Google Scholar] [CrossRef]
- Eguchi, T.; Tada, M.; Shiratori, T.; Imai, M.; Onose, Y.; Suzuki, S.; Satou, R.; Ishizuka, Y.; Sugihara, N. Factors Associated with Undergoing Regular Dental Check-ups in Healthy Elderly Individuals. Bull. Tokyo Dent. Coll. 2018, 59, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Gerritsen, A.E.; Allen, P.F.; Witter, D.J.; Bronkhorst, E.M.; Creugers, N.H.J. Tooth loss and oral health-related quality of life: A systematic review and meta-analysis. Health Qual. Life Outcomes 2010, 8, 126. [Google Scholar] [CrossRef] [Green Version]
- Tan, H.; Peres, K.; Peres, M. Retention of Teeth and Oral Health–Related Quality of Life. J. Dent. Res. 2016, 95, 1350–1357. [Google Scholar] [CrossRef]
- Lauritano, D.; Moreo, G.; Della Vella, F.; Di Stasio, D.; Carinci, F.; Lucchese, A.; Petruzzi, M. Oral Health Status and Need for Oral Care in an Aging Population: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 4558. [Google Scholar] [CrossRef] [Green Version]
- Healthy People 2030. Preventive Care. Available online: https://health.gov/healthypeople/objectives-and-data/browse-objectives/preventive-care (accessed on 16 November 2021).
- Health Japan 21 (The Second Term). Analysis and Assessments Project. Available online: https://www.nibiohn.go.jp/eiken/kenkounippon21/en/kenkounippon21/mokuhyou.html (accessed on 16 November 2021).
- World Health Organization. COVID-19—China. Available online: https://www.who.int/emergencies/disease-outbreak-news/item/2020-DON229 (accessed on 16 November 2021).
- Ministry of Health, Labour and Welfare. Visualizing the Data: Information on COVID-19 Infections. Available online: https://covid19.mhlw.go.jp/ (accessed on 16 February 2022).
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 12 November 2021).
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Ammar, A.; Chtourou, H.; Boukhris, O.; Trabelsi, K.; Masmoudi, L.; Brach, M.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. COVID-19 Home Confinement Negatively Impacts Social Participation and Life Satisfaction: A Worldwide Multicenter Study. Int. J. Environ. Res. Public Health 2020, 17, 6237. [Google Scholar] [CrossRef]
- Kranz, A.; Gahlon, G.; Dick, A.; Stein, B. Characteristics of US Adults Delaying Dental Care Due to the COVID-19 Pandemic. JDR Clin. Transl. Res. 2021, 6, 8–14. [Google Scholar] [CrossRef]
- Hajek, A.; De Bock, F.; Huebl, L.; Kretzler, B.; König, H.-H. Postponed Dental Visits during the COVID-19 Pandemic and their Correlates. Evidence from the Nationally Representative COVID-19 Snapshot Monitoring in Germany (COSMO). Healthcare 2021, 9, 50. [Google Scholar] [CrossRef]
- Iwasaki, M.; Usui, M.; Ariyoshi, W.; Nakashima, K.; Nagai-Yoshioka, Y.; Inoue, M.; Kobayashi, K.; Nishihara, T. Interruption of regular dental visits during the COVID-19 pandemic due to concerns regarding dental visits was associated with periodontitis in Japanese office workers. J. Periodontal Res. 2021, 56, 1091–1098. [Google Scholar] [CrossRef]
- Sekundo, C.; Langowski, E.; Frese, C. Influence of COVID-19 Restrictions on Patients’ Self-reported Oral Health Care Needs. Oral Health Prev. Dent. 2021, 19, 339–343. [Google Scholar] [CrossRef]
- Meisha, D.E.; Alsolami, A.M.; Alharbi, G.M. Social determinants of seeking emergency and routine dental care in Saudi Arabia during the COVID-19 pandemic. BMC Oral Health 2021, 21, 212. [Google Scholar] [CrossRef]
- Walter, E.; von Bronk, L.; Hickel, R.; Huth, K. Impact of COVID-19 on Dental Care during a National Lockdown: A Retrospective Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 7963. [Google Scholar] [CrossRef]
- Cabinet Secretariat. COVID-19 Information and Resources. Available online: https://corona.go.jp/emergency/ (accessed on 13 November 2021).
- Japan Dental Association. About the COVID-19. Available online: https://www.jda.or.jp/corona/ (accessed on 15 November 2021).
- Macromill, Inc. Available online: https://www.macromill.com/ (accessed on 20 November 2021).
- Ministry of Internal Affairs and Communications. Population Census. Available online: https://www.stat.go.jp/english/data/kokusei/index.html (accessed on 15 November 2021).
- Ministry of Health, Labour and Welfare. National Health and Nutrition Survey. Available online: https://www.mhlw.go.jp/toukei/itiran/gaiyo/k-eisei.html (accessed on 16 February 2022).
- Ministry of Health, Labour and Welfare. Comprehensive Survey of Living Conditions. Available online: https://www.mhlw.go.jp/english/database/db-hss/cslc-tables.html (accessed on 17 November 2021).
- Ueno, M.; Zaitsu, T.; Shinada, K.; Ohara, S.; Kawaguchi, Y. Validity of the self-reported number of natural teeth in Japanese adults. J. Investig. Clin. Dent. 2010, 1, 79–84. [Google Scholar] [CrossRef]
- Matsui, D.; Yamamoto, T.; Nishigaki, M.; Miyatani, F.; Watanabe, I.; Koyama, T.; Ozaki, E.; Kuriyama, N.; Kanamura, N.; Watanabe, Y. Validity of self-reported number of teeth and oral health variables. BMC Oral Health 2016, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Aquilanti, L.; Gallegati, S.; Temperini, V.; Ferrante, L.; Skrami, E.; Procaccini, M.; Rappelli, G. Italian Response to Coronavirus Pandemic in Dental Care Access: The DeCADE Study. Int. J. Environ. Res. Public Health 2020, 17, 6977. [Google Scholar] [CrossRef]
- Moffat, R.; Yentes, C.; Crookston, B.; West, J. Patient Perceptions about Professional Dental Services during the COVID-19 Pandemic. JDR Clin. Transl. Res. 2021, 6, 15–23. [Google Scholar] [CrossRef]
- Peloso, R.M.; Pini, N.I.P.; Sundfeld Neto, D.; Mori, A.A.; de Oliveira, R.C.G.; Valarelli, F.P.; Freitas, K.M.S. How Does the Quarantine Resulting from COVID-19 Impact Dental Appointments and Patient Anxiety Levels? Braz. Oral Res. 2020, 34, e84. [Google Scholar] [CrossRef]
- Ibrahim, M.S.; Alibrahim, H.; Al Madani, A.; Alamri, A.; Bamashmous, M.; Tounsi, A. Fear Factor in Seeking Dental Care among Saudis during COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 10589. [Google Scholar] [CrossRef]
- Anikeeva, O.; Brennan, D.S.; Teusner, D.N. Household income modifies the association of insurance and dental visiting. BMC Health Serv. Res. 2013, 13, 432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, T.; Haroon, H.; Baig, M.; Hui, J. Coronavirus Disease 2019 (COVID-19) Pandemic and Economic Impact. Pak. J. Med. Sci. 2020, 36, S73–S78. [Google Scholar] [CrossRef] [PubMed]
- Takashima, R.; Onishi, R.; Saeki, K.; Hirano, M. Perception of COVID-19 Restrictions on Daily Life among Japanese Older Adults: A Qualitative Focus Group Study. Healthcare 2020, 8, 450. [Google Scholar] [CrossRef] [PubMed]
- Ghanbarzadegan, A.; Bastani, P.; Luzzi, L.; Brennan, D. Inequalities in utilization and provision of dental services: A scoping review. Syst. Rev. 2021, 10, 222. [Google Scholar] [CrossRef]
- Matsuyama, Y.; Aida, J.; Takeuchi, K.; Koyama, S.; Tabuchi, T. Dental Pain and Worsened Socioeconomic Conditions Due to the COVID-19 Pandemic. J. Dent. Res. 2021, 100, 591–598. [Google Scholar] [CrossRef]
- Ministry of Internal Affairs and Communications. Internet Usage. Available online: https://www.soumu.go.jp/johotsusintokei/whitepaper/ja/r03/html/nd242120.html (accessed on 22 November 2021).


{kind=link}
| Total Number | Those Who Habitually Received RDC before the COVID-19 Pandemic (n = 2219) | Those Who Did Not Habitually Receive RDC before the COVID-19 Pandemic (n = 1337) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Those Who Have Received RDC since the Pandemic | Those Who Have Not Received RDC since the Pandemic | p Value * | Those Who Have Received RDC since the Pandemic | Those Who Have Not Received RDC since the Pandemic | p Value * | |||||
| Total, n (%) | 3556 | 1586 | (71.5) | 633 | (28.5) | 103 | (7.7) | 1234 | (92.3) | ||
| Gender, n (%) | |||||||||||
| Male | 1708 | 721 | (75.9) | 229 | (24.1) | <0.001 | 48 | (6.3) | 710 | (93.7) | 0.031 |
| Female | 1848 | 865 | (68.2) | 404 | (31.8) | 55 | (9.5) | 524 | (90.5) | ||
| Age, n (%) | |||||||||||
| 20–29 years | 430 | 123 | (63.4) | 71 | (36.6) | 0.010 | 28 | (11.9) | 208 | (88.1) | 0.032 |
| 30–39 years | 535 | 201 | (71.8) | 79 | (28.2) | 21 | (8.2) | 234 | (91.8) | ||
| 40–49 years | 629 | 266 | (72.5) | 101 | (27.5) | 11 | (4.2) | 251 | (95.8) | ||
| 50–59 years | 529 | 215 | (66.6) | 108 | (33.4) | 14 | (6.8) | 192 | (93.2) | ||
| 60–69 years | 618 | 324 | (76.1) | 102 | (23.9) | 18 | (9.4) | 174 | (90.6) | ||
| ≥70 years | 815 | 457 | (72.7) | 172 | (27.3) | 11 | (5.9) | 175 | (94.1) | ||
| Household income, n (%) | |||||||||||
| <2000 K JPY | 299 | 119 | (69.6) | 52 | (30.4) | 0.049 | 9 | (7.0) | 119 | (93.0) | 0.412 |
| 2000 K–< 4000 K JPY | 850 | 381 | (70.7) | 158 | (29.3) | 25 | (8.0) | 286 | (92.0) | ||
| 4000 K–< 6000 K JPY | 703 | 331 | (77.0) | 99 | (23.0) | 14 | (5.1) | 259 | (94.9) | ||
| 6000 K–< 8000 K JPY | 455 | 221 | (72.2) | 85 | (27.8) | 9 | (6.0) | 140 | (94.0) | ||
| ≥8000 K JPY | 478 | 243 | (71.7) | 96 | (28.3) | 14 | (10.1) | 125 | (89.9) | ||
| Unknown | 771 | 291 | (67.1) | 143 | (32.9) | 32 | (9.5) | 305 | (90.5) | ||
| Employment status, n (%) | |||||||||||
| Regular employee | 1351 | 557 | (71.9) | 218 | (28.1) | 0.189 | 45 | (7.8) | 531 | (92.2) | 0.913 |
| Non-regular employee | 454 | 214 | (73.5) | 77 | (26.5) | 12 | (7.4) | 151 | (92.6) | ||
| Homemaker | 756 | 381 | (69.5) | 167 | (30.5) | 19 | (9.1) | 189 | (90.9) | ||
| Self-employed and others | 339 | 136 | (66.3) | 69 | (33.7) | 9 | (6.7) | 125 | (93.3) | ||
| Not working | 656 | 298 | (74.5) | 102 | (25.5) | 18 | (7.0) | 238 | (93.0) | ||
| Marital status, n (%) | |||||||||||
| Married | 2296 | 1106 | (72.3) | 423 | (27.7) | 0.181 | 60 | (7.8) | 707 | (92.2) | 0.850 |
| Single | 1260 | 480 | (69.6) | 210 | (30.4) | 43 | (7.5) | 527 | (92.5) | ||
| Municipalities, n (%) | |||||||||||
| Metropolis (pop 500,000+) | 1242 | 583 | (70.8) | 240 | (29.2) | 0.239 | 37 | (8.8) | 382 | (91.2) | 0.101 |
| Core cities (pop 200,000+) | 685 | 310 | (73.3) | 113 | (26.7) | 11 | (4.2) | 251 | (95.8) | ||
| Cities (pop 50,000+) | 1417 | 616 | (72.2) | 237 | (27.8) | 49 | (8.7) | 515 | (91.3) | ||
| Towns and villages | 212 | 77 | (64.2) | 43 | (35.8) | 6 | (6.5) | 86 | (93.5) | ||
| Number of teeth, n (%) | |||||||||||
| 0–9 | 183 | 50 | (61.7) | 31 | (38.3) | 0.115 # | 5 | (4.9) | 97 | (95.1) | 0.645 # |
| 10–19 | 369 | 179 | (69.6) | 78 | (30.4) | 9 | (8.0) | 103 | (92.0) | ||
| 20–27 | 1392 | 656 | (72.2) | 253 | (27.8) | 41 | (8.5) | 442 | (91.5) | ||
| ≥28 | 1612 | 701 | (72.1) | 271 | (27.9) | 48 | (7.5) | 592 | (92.5) | ||
| Frequency of brushing teeth, n (%) | |||||||||||
| ≥three times daily | 928 | 503 | (73.3) | 183 | (26.7) | 0.431 # | 24 | (9.9) | 218 | (90.1) | 0.008 # |
| Twice daily | 1894 | 826 | (70.2) | 350 | (29.8) | 61 | (8.5) | 657 | (91.5) | ||
| Once daily | 674 | 249 | (72.2) | 96 | (27.8) | 17 | (5.2) | 312 | (94.8) | ||
| Sometimes/No brushing | 60 | 8 | (66.7) | 4 | (33.3) | 1 | (2.1) | 47 | (97.9) | ||
| Interdental cleaning, n (%) | |||||||||||
| Yes | 2040 | 1199 | (75.4) | 392 | (24.6) | <0.001 | 58 | (12.9) | 391 | (87.1) | <0.001 |
| No | 1516 | 387 | (61.6) | 241 | (38.4) | 45 | (5.1) | 843 | (94.9) | ||
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95%CI | p Value | OR | 95%CI | p Value |
| Gender | ||||||
| Male | 0.65 | (0.51–0.82) | <0.001 | 0.58 | (0.45–0.74) | <0.001 |
| Female | 1.00 | Reference | 1.00 | Reference | ||
| Age | ||||||
| 20–29 years | 1.55 | (1.06–2.28) | 0.025 | 1.45 | (0.98–2.14) | 0.064 |
| 30–39 years | 1.04 | (0.73–1.48) | 0.810 | 1.04 | (0.73–1.48) | 0.838 |
| 40–49 years | 1.00 | Reference | 1.00 | |||
| 50–59 years | 1.33 | (0.96–1.85) | 0.091 | 1.34 | (0.96–1.87) | 0.088 |
| 60–69 years | 0.83 | (0.59–1.15) | 0.266 | 0.85 | (0.60–1.19) | 0.332 |
| ≥70 years | 0.95 | (0.69–1.32) | 0.757 | 0.94 | (0.67–1.32) | 0.710 |
| Household income | ||||||
| <2000 K JPY | 1.54 | (1.01–2.35) | 0.045 | 1.45 | (0.94–2.23) | 0.089 |
| 2000 K–< 4000 K JPY | 1.45 | (1.08–1.96) | 0.014 | 1.46 | (1.08–1.98) | 0.014 |
| 4000 K–< 6000 K JPY | 1.00 | Reference | 1.00 | Reference | ||
| 6000 K–< 8000 K JPY | 1.29 | (0.91–1.81) | 0.147 | 1.28 | (0.91–1.82) | 0.157 |
| ≥8000 K JPY | 1.31 | (0.94–1.83) | 0.116 | 1.32 | (0.94–1.86) | 0.106 |
| Unknown | 1.53 | (1.12–2.09) | 0.007 | 1.53 | (1.12–2.09) | 0.008 |
| Employment status | ||||||
| Regular employee | 1.00 | Reference | 1.00 | Reference | ||
| Non-regular employee | 0.76 | (0.55–1.06) | 0.111 | 0.76 | (0.54–1.07) | 0.112 |
| Homemaker | 0.96 | (0.70–1.32) | 0.785 | 0.96 | (0.70–1.33) | 0.820 |
| Self-employed and others | 1.34 | (0.94–1.90) | 0.102 | 1.33 | (0.93–1.89) | 0.119 |
| Not working | 0.92 | (0.66–1.28) | 0.625 | 0.96 | (0.68–1.34) | 0.804 |
| Marital status | ||||||
| Married | 1.00 | (0.80–1.26) | 0.982 | 1.03 | (0.82–1.30) | 0.773 |
| Single | 1.00 | Reference | 1.00 | Reference | ||
| Municipalities | ||||||
| Metropolis (pop. 500,000+) | 1.06 | (0.85–1.31) | 0.613 | 1.13 | (0.91–1.41) | 0.265 |
| Core cities (pop. 200,000+) | 0.96 | (0.73–1.25) | 0.755 | 0.99 | (0.76–1.30) | 0.939 |
| Cities (pop. 50,000+) | 1.00 | Reference | 1.00 | Reference | ||
| Towns and villages | 1.46 | (0.97–2.19) | 0.070 | 1.49 | (0.98–2.26) | 0.059 |
| Number of teeth | ||||||
| 0–9 | 1.00 | Reference | ||||
| 10–19 | 0.74 | (0.43–1.27) | 0.269 | |||
| 20–27 | 0.63 | (0.39–1.03) | 0.066 | |||
| ≥28 | 0.60 | (0.36–0.98) | 0.040 | |||
| Frequency of brushing teeth | ||||||
| ≥three times daily | 0.97 | (0.71–1.32) | 0.838 | |||
| Twice daily | 1.13 | (0.86–1.50) | 0.387 | |||
| Once daily | 1.00 | Reference | ||||
| Sometimes/No brushing | 1.54 | (0.43–5.55) | 0.513 | |||
| Interdental cleaning | ||||||
| Yes | 0.51 | (0.41–0.63) | <0.001 | |||
| No | 1.00 | Reference | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oshima, K.; Miura, H.; Tano, R.; Fukuda, H. Factors Associated with Regular Dental Checkups’ Discontinuation during the COVID-19 Pandemic: A Nationwide Cross-Sectional Web-Based Survey in Japan. Int. J. Environ. Res. Public Health 2022, 19, 2917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052917
Oshima K, Miura H, Tano R, Fukuda H. Factors Associated with Regular Dental Checkups’ Discontinuation during the COVID-19 Pandemic: A Nationwide Cross-Sectional Web-Based Survey in Japan. International Journal of Environmental Research and Public Health. 2022; 19(5):2917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052917
Chicago/Turabian StyleOshima, Katsuo, Hiroko Miura, Rumi Tano, and Hideki Fukuda. 2022. "Factors Associated with Regular Dental Checkups’ Discontinuation during the COVID-19 Pandemic: A Nationwide Cross-Sectional Web-Based Survey in Japan" International Journal of Environmental Research and Public Health 19, no. 5: 2917. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19052917