
Native and Indigenous Populations and Gastric Cancer: A Worldwide Review

 ,
, {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
Incidence and Prevalence of Gastric Cancer: A Worldwide Perspective
2. Methods
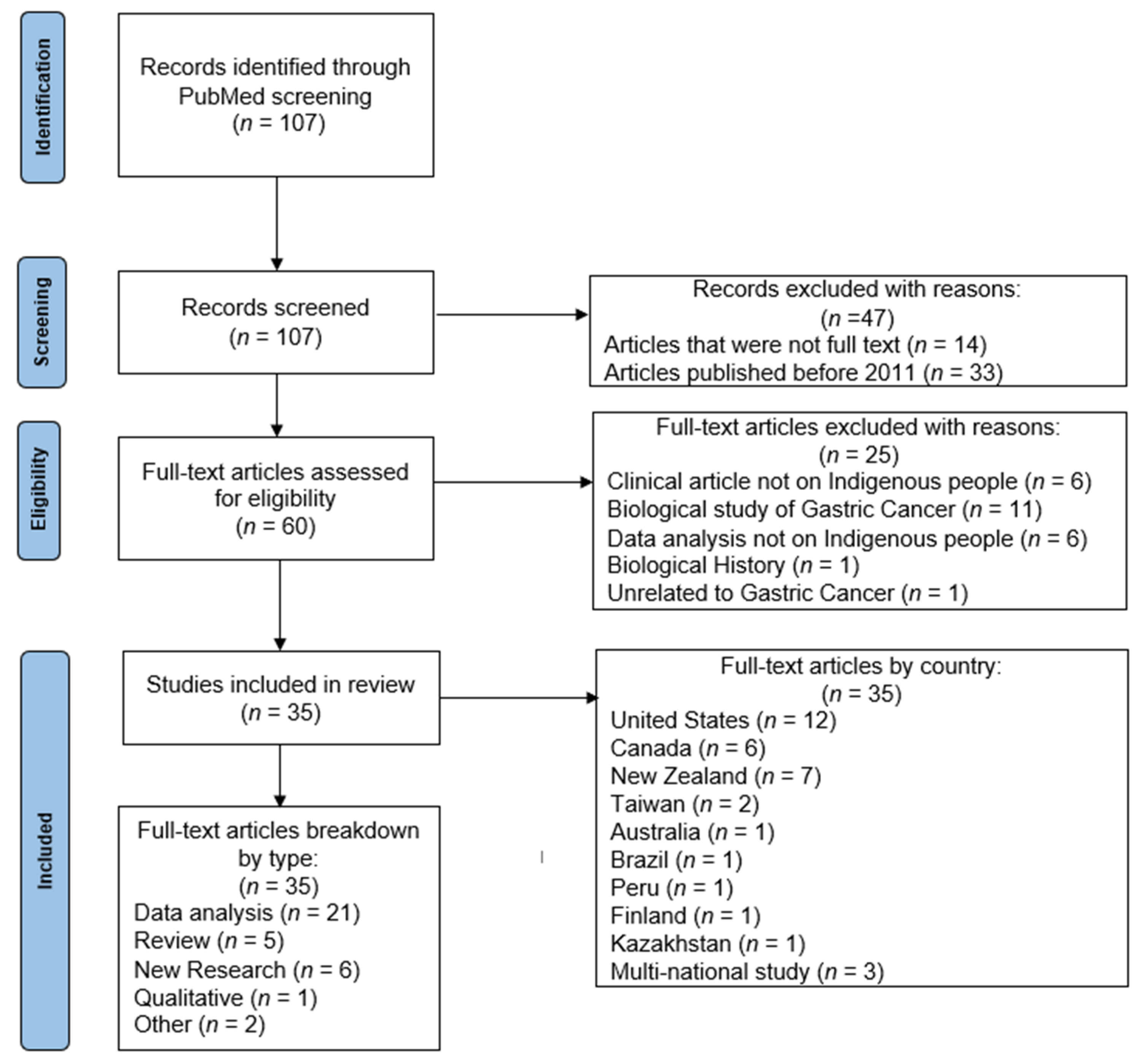
2.1. Systematic Literature Review
2.2. Sources beyond the Systematic Review
3. Results of Review and Outside Sources Supplementary Findings
3.1. Systematic Literature Review
3.2. Sources beyond the Systematic Review
4. Literature Review Qualitative Findings
5. Food and Gastric Cancer
5.1. Access
5.2. Choices
6. Environmental Factors
6.1. Uranium Exposure
6.2. The Built Environment and Water
6.3. H. pylori
7. The Health Care System
7.1. Access to Cancer Prevention and Control for All Cancer Types among Indigenous Populations: Challenges of Time, Geography and Communication
7.2. Indigenous Gastric Cancer Patients: Challenges of Access to Cancer Prevention and Control
8. Education and Awareness
8.1. Examples of Successful Indigenous Gastric Cancer Programming
8.2. Inceasing Education: A Potential Tool for Explaining Gastric Biology/Cancer through a Cultural Lens
9. Discussion
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cancer Fact Sheet. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 10 November 2021).
- National Cancer Institute Surveillance. Epidemiology, and End Results Program. Cancer Stat Facts: Stomach Cancer. Available online: https://seer.cancer.gov/statfacts/html/stomach.html (accessed on 11 November 2021).
- Melkonian, S.C.; Pete, D.; Jim, M.A.; Haverkamp, D.; Wiggins, C.L.; Bruce, M.G.; White, M.C. Gastric cancer among American Indian and Alaska native populations in the United States, 2005–2016. Am. J. Gastroenterol. 2020, 115, 1989–1997. [Google Scholar] [CrossRef] [PubMed]
- Bair, M.J.; Chuang, S.L.; Lei, W.Y.; Chen, C.L.; Tian, H.W.; Chiang, T.H.; Su, W.W.; Lin, C.C.; Chung Lo, Y.T.; Jou, Y.Y.; et al. Planning mass eradication of Helicobacter pylori infection for indigenous Taiwanese peoples to reduce gastric cancer. J. Gastroenterol. Hepatol. 2020, 35, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Signal, V.; Sarfati, D.; Cunningham, R.; Gurney, J.; Koea, J.; Ellison-Loschmann, L. Indigenous inequities in the presentation and management of stomach cancer in New Zealand: A country with universal health care coverage. Gastric Cancer 2015, 18, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.P.; Forman, D.; Piñeros, M.; Fernández, S.M.; de Oliveira Santos, M.; Bray, F. Cancer in indigenous people in Latin America and the Caribbean: A review. Cancer Med. 2014, 3, 70–80. [Google Scholar] [CrossRef] [Green Version]
- Nolen, L.D.; Vindigni, S.M.; Parsonnet, J. Combating gastric cancer in Alaska native people: An expert and community symposium. Gastroenterology 2020, 158, 1197–1201. [Google Scholar] [CrossRef]
- Harris, R.B.; Begay, R.; Sanderson, P.R.; Chief, C.; Monroy, F.; Brown, H.E.; Oren, E. Helicobacter Pylori Infections in Navajo Communities of Northern Arizona. In Cancer Epidemiology Biomarkers & Prevention; American Association for Cancer Research: Philadelphia, PA, USA, 2020. [Google Scholar]
- Ulanja, M.B.; Beutler, B.D.; Rishi, M.; Konam, K.G.; Zell, S.C.; Patterson, D.R.; Ambika, S.; Gullapalli, N. Influence of race and geographic setting on the management of gastric adenocarcinoma. J. Surg. Oncol. 2019, 120, 270–279. [Google Scholar] [CrossRef]
- Arnold, M.; Moore, S.P.; Hassler, S.; Ellison-Loschmann, L.; Forman, D.; Bray, F. The burden of stomach cancer in indigenous populations: A systematic review and global assessment. Gut 2014, 63, 64–71. [Google Scholar] [CrossRef] [Green Version]
- Yusefi, A.R.; Bagheri Lankarani, K.; Bastani, P.; Radinmanesh, M.; Kavosi, Z. Risk factors for gastric cancer: A systematic review. Asian Pac. J. Cancer Prev. 2018, 19, 591–603. [Google Scholar]
- Reading, C. Structural Determinants of Aboriginal Peoples’ Health. In Determinants of Indigenous Peoples’ Health: Beyond the Social; Canadian Scholars’ Press Inc.: Toronto, ON, Canada, 2018; Volume 1. [Google Scholar]
- Sumner, J.; Tarhan, M.; McMurtry, J. Eating in place: Mapping alternative food procurement in Canadian indigenous communities. J. Agric. Food Syst. Community Dev. 2019, 9, 239–250. [Google Scholar] [CrossRef]
- Batal, M.; Decelles, S. A scoping review of obesity among indigenous peoples in Canada. J. Obes. 2019, 2019, 9741090. [Google Scholar] [CrossRef]
- Jernigan, V.B.B.; Huyser, K.R.; Valdes, J.; Simonds, V.W. Food insecurity among American Indians and Alaska natives: A national profile using the current population survey-food security supplement. J. Hunger Environ. Nutr. 2017, 12, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenny, T.-A.; Little, M.; Lemieux, T.; Griffin, P.J.; Wesche, S.D.; Ota, Y.; Batal, M.; Chan, H.M.; Lemire, M. The retail food sector and indigenous peoples in high-income countries: A systematic scoping review. Int. J. Environ. Res. Public Health 2020, 17, 8818. [Google Scholar] [CrossRef] [PubMed]
- Simkin, J.; Nash, S.H.; Barchuk, A.; O’Brien, D.K.; Erickson, A.C.; Hanley, B.; Hannah, H.; Corriveau, A.; Larsen, I.K.; Skovlund, C.W.; et al. Stomach cancer incidence and mortality trends among circumpolar nations. Cancer Epidemiol. Biomark. Prev. 2021, 30, 845–856. [Google Scholar] [CrossRef] [PubMed]
- Thurber, K.A.; Long, J.; Salmon, M.; Cuevas, A.G.; Lovett, R. Sugar-sweetened beverage consumption among Indigenous Australian children aged 0–3 years and association with sociodemographic, life circumstances and health factors. Public Health Nutr. 2020, 23, 295–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richmond, C.; Kerr, R.B.; Neufeld, H.; Steckley, M.; Wilson, K.; Dokis, B. Supporting food security for Indigenous families through the restoration of Indigenous foodways. Can. Geogr. 2021, 65, 97–109. [Google Scholar] [CrossRef]
- Love, C.V.; Taniguchi, T.E.; Williams, M.B.; Noonan, C.J.; Wetherill, M.S.; Salvatore, A.L.; Jacob, T.; Cannady, T.K.; Standridge, J.; Spiegel, J.; et al. Diabetes and obesity associated with poor food environments in american indian communities: The tribal health and resilience in vulnerable environments (THRIVE) study. Curr. Dev. Nutr. 2019, 3 (Suppl. 2), 63–68. [Google Scholar] [PubMed] [Green Version]
- Redvers, N.; Chischilly, A.M.; Warne, D.; Pino, M.; Lyon-Colbert, A. Uranium exposure in American Indian communities: Health, policy, and the way forward. Environ. Health Perspect. 2021, 129, 35002. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Wu, X.; Li, S.; Li, C.; Guo, Z. Impact of environmental factors on gastric cancer: A review of the scientific evidence, human prevention and adaptation. J. Environ. Sci. 2020, 89, 65–79. [Google Scholar] [CrossRef]
- Schultz, R. Investigating the health impacts of the ranger uranium mine on Aboriginal people. Med. J. Aust. 2021, 215, 157–159. [Google Scholar] [CrossRef]
- Kreuzer, M.; Straif, K.; Marsh, J.W.; Dufey, F.; Grosche, B.; Nosske, D.; Sogl, M. Occupational dust and radiation exposure and mortality from stomach cancer among German uranium miners, 1946–2003. Occup. Environ. Med. 2012, 69, 217–223. [Google Scholar] [CrossRef]
- Wagner, S.E.; Burch, J.B.; Bottai, M.; Puett, R.; Porter, D.; Bolick-Aldrich, S.; Temples, T.; Wilkerson, R.C.; Vena, J.E.; Hébert, J.R. Groundwater uranium and cancer incidence in South Carolina. Cancer Causes Control 2011, 22, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.C.; Jones, L.; Credo, J.; Rock, T. Uranium and arsenic unregulated water issues on Navajo lands. J. Vac. Sci. Technol. A 2020, 38, 031003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, A.; Wilton, D.H.C.; Fitzgerald, E.; Sharma, A.; Sharma, A.; Sathya, A.J. Environmental impact assessment of uranium exploration and development on indigenous land in Labrador (Canada): A community-driven initiative. Environ. Geochem. Health 2019, 41, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Chief, C.; Sanderson, P.R.; Willeto, A.A.A.; Yazzie, A.; McKinley, A.; Monroy, F.P.; Harris, R.B.; Oren, E. “Nobody Is Talking About It”: Diné (Navajo) communities speak about stomach cancer and helicobacter pylori infections. J. Cancer Educ. 2020, 37, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Sitarz, R.; Skierucha, M.; Mielko, J.; Offerhaus, G.J.A.; Maciejewski, R.; Polkowski, W.P. Gastric cancer: Epidemiology, prevention, classification, and treatment. Cancer Manag. Res. 2018, 10, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Mayer, B.; Joshweseoma, L.; Sehongva, G. Environmental risk perceptions and community health: Arsenic, air pollution, and threats to traditional values of the Hopi Tribe. J. Community Health 2019, 44, 896–902. [Google Scholar] [CrossRef]
- Martin, C.; Simonds, V.W.; Young, S.L.; Doyle, J.; Lefthand, M.; Eggers, M.J. Our relationship to water and experience of water insecurity among Apsáalooke (Crow Indian) people, Montana. Int. J. Environ. Res. Public Health 2021, 18, 582. [Google Scholar] [CrossRef]
- Balazs, C.L.; Ray, I. The drinking water disparities framework: On the origins and persistence of inequities in exposure. Am. J. Public Health 2014, 104, 603–611. [Google Scholar] [CrossRef]
- Doyle, J.T.; Kindness, L.; Realbird, J.; Eggers, M.J.; Camper, A.K. Challenges and opportunities for tribal waters: Addressing disparities in safe public drinking water on the crow reservation in Montana, USA. Int. J. Environ. Res. Public Health 2018, 15, 567. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.; Gonzales, M.; Burnette, C.; Benally, M.; Seanez, P.; Shuey, C.; Nez, H.; Nez, C.; Nez, S. Environmental exposures to metals in Native communities and implications for child development: Basis for the Navajo birth cohort study. J. Soc. Work Disabil. Rehabil. 2015, 14, 245–269. [Google Scholar] [CrossRef]
- VanDerslice, J. Drinking water infrastructure and environmental disparities: Evidence and methodological considerations. Am. J. Public Health 2011, 101 (Suppl. 1), S109–S114. [Google Scholar] [CrossRef] [PubMed]
- Mosites, E.; Seeman, S.; Fenaughty, A.; Fink, K.; Eichelberger, L.; Holck, P.; Thomas, T.K.; Bruce, M.G.; Hennessy, T.W. Lack of in-home piped water and reported consumption of sugar-sweetened beverages among adults in rural Alaska. Public Health Nutr. 2020, 23, 861–868. [Google Scholar] [CrossRef] [PubMed]
- Mosites, E.; Lefferts, B.; Seeman, S.; January, G.; Dobson, J.; Fuente, D.; Bruce, M.; Thomas, T.; Hennessy, T. Community water service and incidence of respiratory, skin, and gastrointestinal infections in rural Alaska, 2013–2015. Int. J. Hyg. Environ. Health 2020, 225, 113475. [Google Scholar] [CrossRef] [PubMed]
- Blair, V.; Kahokehr, A.; Sammour, T. Cancer in Māori: Lessons from prostate, colorectal and gastric cancer and progress in hereditary stomach cancer in New Zealand. ANZ J. Surg. 2013, 83, 42–48. [Google Scholar] [CrossRef]
- Cheung, J.; Goodman, K.J.; Girgis, S.; Bailey, R.; Morse, J.; Fedorak, R.N.; Geary, J.; Fagan-Garcia, K.; van Zanten, S.V. Disease manifestations of Helicobacter pylori infection in Arctic Canada: Using epidemiology to address community concerns. BMJ Open 2014, 4, e003689. [Google Scholar] [CrossRef] [Green Version]
- Robinson, L.G.; Black, F.L.; Lee, F.K.; Sousa, A.O.; Owens, M.; Danielsson, D.; Nahmias, A.J.; Gold, B.D. Helicobacter pylori prevalence among indigenous peoples of South America. J. Infect. Dis. 2002, 186, 1131–1137. [Google Scholar] [CrossRef] [Green Version]
- Melius, E.J.; Davis, S.I.; Redd, J.T.; Lewin, M.; Herlihy, R.; Henderson, A.; Sobel, J.; Gold, B.; Cheek, J.E. Estimating the prevalence of active Helicobacter pylori infection in a rural community with global positioning system technology-assisted sampling. Epidemiol. Infect. 2013, 141, 472–480. [Google Scholar] [CrossRef]
- Stancioiu, F.A.S.; Buschor, R. Helicobacter pylori: Findings in a Native American population. IHS Prim. Care Provid. 2005, 30, 59–74. [Google Scholar]
- Yang, L.; Kartsonaki, C.; Yao, P.; de Martel, C.; Plummer, M.; Chapman, D.; Guo, Y.; Clark, S.; Walters, R.G.; Chen, Y.; et al. The relative and attributable risks of cardia and non-cardia gastric cancer associated with Helicobacter pylori infection in China: A case-cohort study. Lancet Public Health 2021, 6, e888–e896. [Google Scholar] [CrossRef]
- Nolen, L.D.; Bressler, S.; Vindigni, S.M.; Miller, K.; Nash, S. Gastric cancer in Alaska Native and American Indian people living in Alaska, 1990–2017. Clin. Transl. Gastroenterol. 2021, 12, e00374. [Google Scholar] [CrossRef]
- Batai, K.; Gachupin, F.C.; Estrada, A.L.; Garcia, D.O.; Gomez, J.; Kittles, R.A. Patterns of cancer related health disparities in Arizona. Cancer Health Disparities 2019, 3, e1–e20. [Google Scholar] [PubMed]
- Adams, S.V.; Bansal, A.; Burnett-Hartman, A.N.; Cohen, S.A.; Karnopp, A.; Warren-Mears, V.; Ramsey, S.D. Cancer treatment delays in American Indians and Alaska Natives enrolled in medicare. J. Health Care Poor Underserved 2017, 28, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Liddell, J.L.; Burnette, C.E.; Roh, S.; Lee, Y.S. Healthcare barriers and supports for American Indian women with cancer. Soc. Work Health Care 2018, 57, 656–673. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Xu, M.; Gao, T.; Xu, L.; Zeng, P.; Bo, H.; Li, F.; Zhang, W.; Wang, Z. Surgical compliance and outcomes in gastric cancer: A population-based cohort study. J. Cancer 2019, 10, 779–788. [Google Scholar] [CrossRef]
- Onega, T.; Duell, E.J.; Shi, X.; Wang, D.; Demidenko, E.; Goodman, D. Geographic access to cancer care in the U.S. Cancer 2008, 112, 909–918. [Google Scholar] [CrossRef]
- Manitowabi, S. Historical and Contemporary Realities: Movement Towards Reconciliation; Open Library Pressbook: Toronto, ON, Canada, 2018. [Google Scholar]
- O’Connor, A.; O’Moráin, C. Digestive function of the stomach. Dig. Dis. 2014, 32, 186–191. [Google Scholar] [CrossRef]
- Al Asqah, M.; Al Hamoudi, N.; Anil, S.; Al Jebreen, A.; Al-Hamoudi, W.K. Is the presence of Helicobacter pylori in dental plaque of patients with chronic periodontitis a risk factor for gastric infection? Can. J. Gastroenterol. 2009, 23, 177–179. [Google Scholar] [CrossRef] [Green Version]
- Traditional Foods Resource Guide. Available online: http://keepitsacred.itcmi.org/traditional-foods-resource-guide/ (accessed on 11 November 2021).
- Bitsóí, A. 11,000-Year-Old Solution to Modern Problem: Ancient Potato Could Thrive in Changing Climate. Available online: https://www.sltrib.com/artsliving/food/2021/09/28/year-old-solution-modern/ (accessed on 13 November 2021).
- Recipes for Resistance: Indigikitchen Teaches Diet Decolonization. Available online: https://www.cbc.ca/radio/unreserved/using-food-to-strengthen-indigenous-culture-and-resist-colonization-1.5126272/recipes-for-resistance-indigikitchen-teaches-diet-decolonization-1.5126279 (accessed on 13 November 2021).
- Eddie, R.S.; Welle, D.L. TAKING ACTION: Policy Advocacy for American Indian/Alaska Native Children: School Nutrition and Indigenous Food Sovereignty. In Policy & Politics in Nursing and Health Care-E-Book; Elsevier: Amsterdam, The Netherlands, 2020; pp. 194–198. [Google Scholar]
- Crowe, R.; Stanley, R.; Probst, Y.; McMahon, A. Culture and healthy lifestyles: A qualitative exploration of the role of food and physical activity in three urban Australian Indigenous communities. Aust. N. Z. J. Public Health 2017, 41, 411–416. [Google Scholar] [CrossRef]
- Burnette, C.E.; Clark, C.B.; Rodning, C.B. “Living off the Land”: How subsistence promotes well-being and resilience among Indigenous peoples of the Southeastern United States. Soc. Serv. Rev. 2018, 92, 369–400. [Google Scholar] [CrossRef]
- American Indian Cancer Foundation for Cancer Screening Test & Awareness. Available online: https://americanindiancancer.org/ (accessed on 13 November 2021).
- Grimes, C.; Dankovchik, J.; Cahn, M.; Warren-Mears, V. American Indian and Alaska Native cancer patients’ perceptions of a culturally specific patient navigator program. J. Prim. Prev. 2017, 38, 121–135. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordova-Marks, F.M.; Carson, W.O.; Monetathchi, A.; Little, A.; Erdrich, J. Native and Indigenous Populations and Gastric Cancer: A Worldwide Review. Int. J. Environ. Res. Public Health 2022, 19, 5437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095437
Cordova-Marks FM, Carson WO, Monetathchi A, Little A, Erdrich J. Native and Indigenous Populations and Gastric Cancer: A Worldwide Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095437
Chicago/Turabian StyleCordova-Marks, Felina M., William O. Carson, Angela Monetathchi, Alyssa Little, and Jennifer Erdrich. 2022. "Native and Indigenous Populations and Gastric Cancer: A Worldwide Review" International Journal of Environmental Research and Public Health 19, no. 9: 5437. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19095437