
Are There Differences between the Stress Responses of Philippine Men and Women to the COVID-19 Pandemic?
 , ,
, ,
Abstract
:1. Introduction
2. Data and Methods
2.1. Data Collection
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Adjusted Model
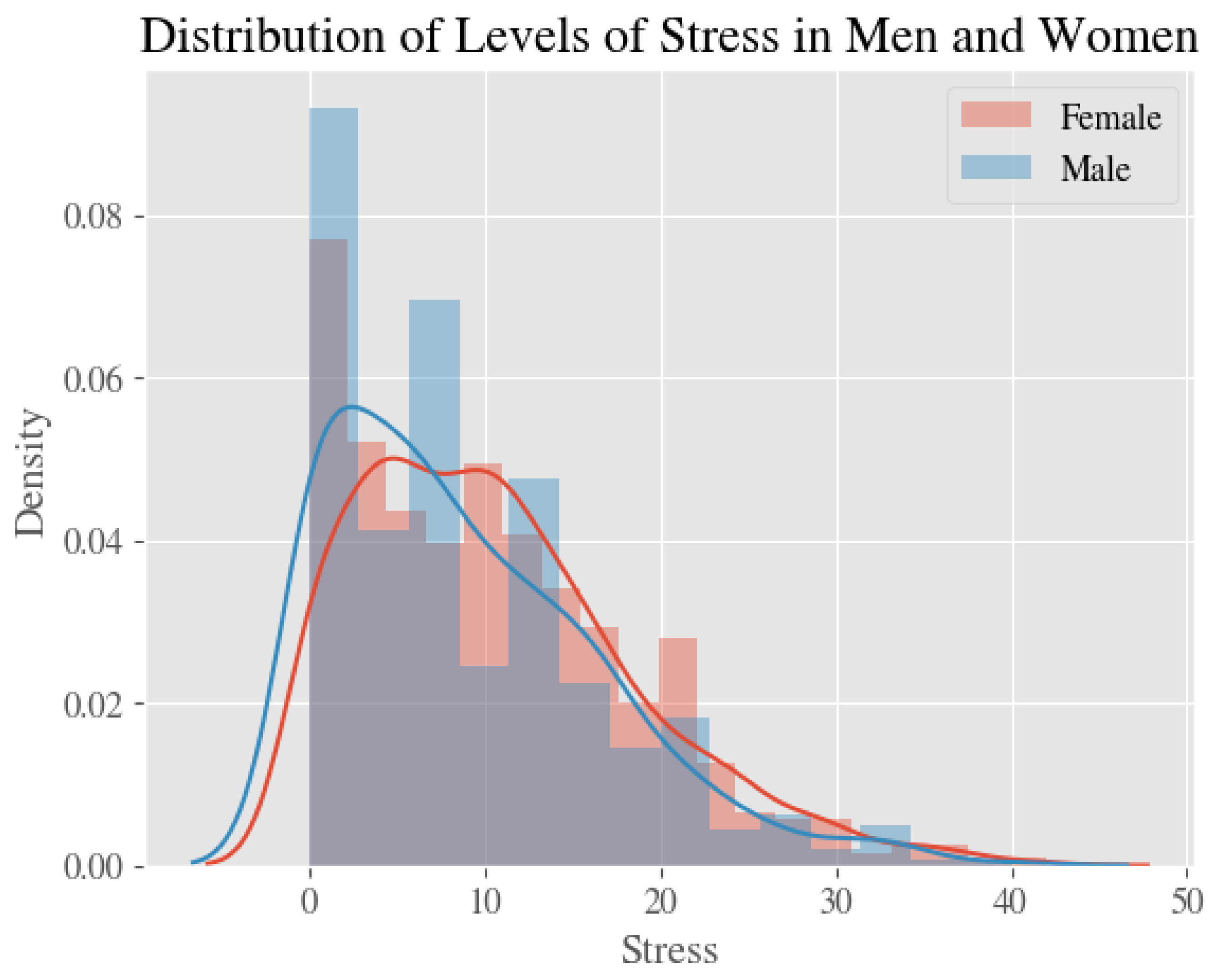
3.2. Stress
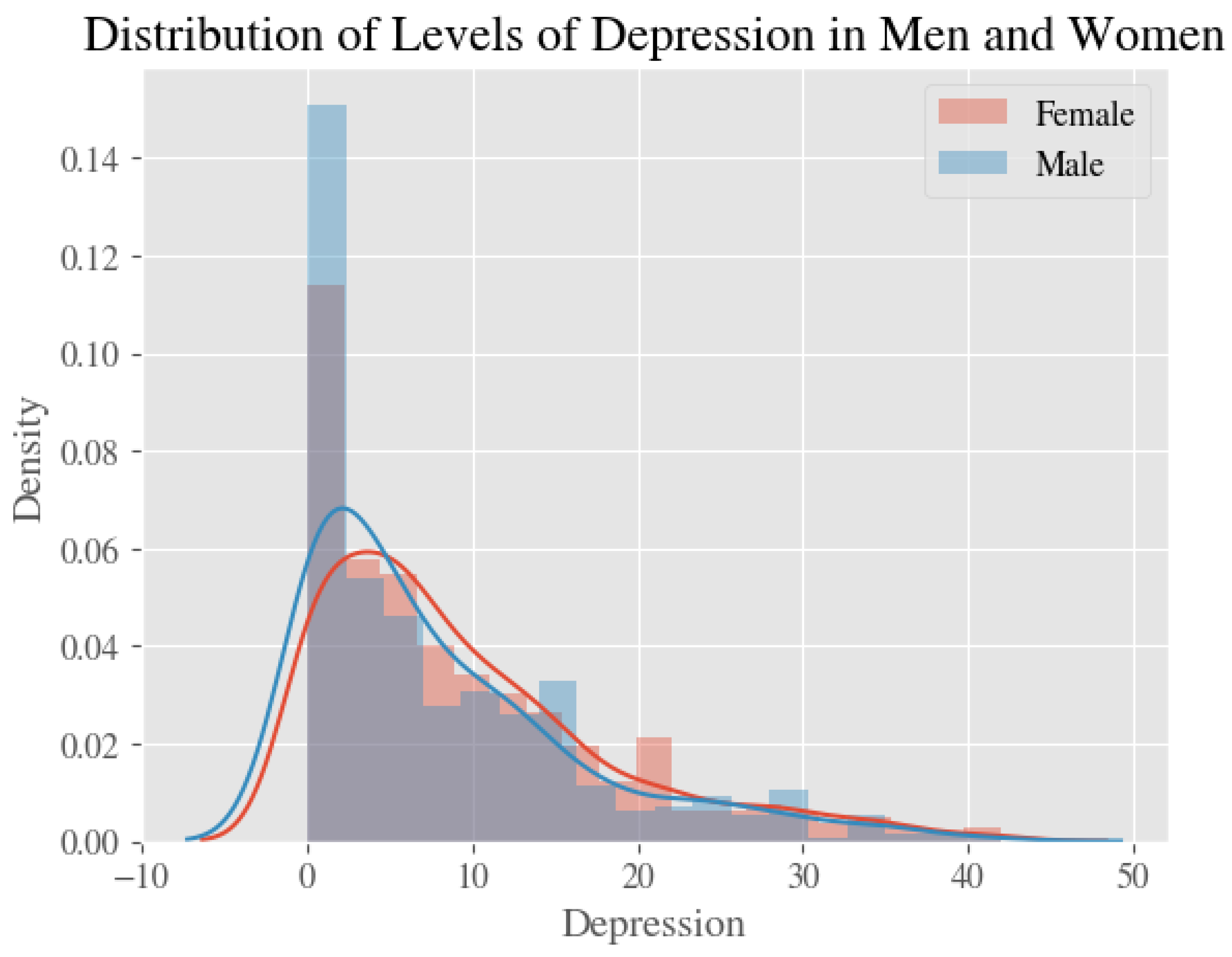
3.3. Depression
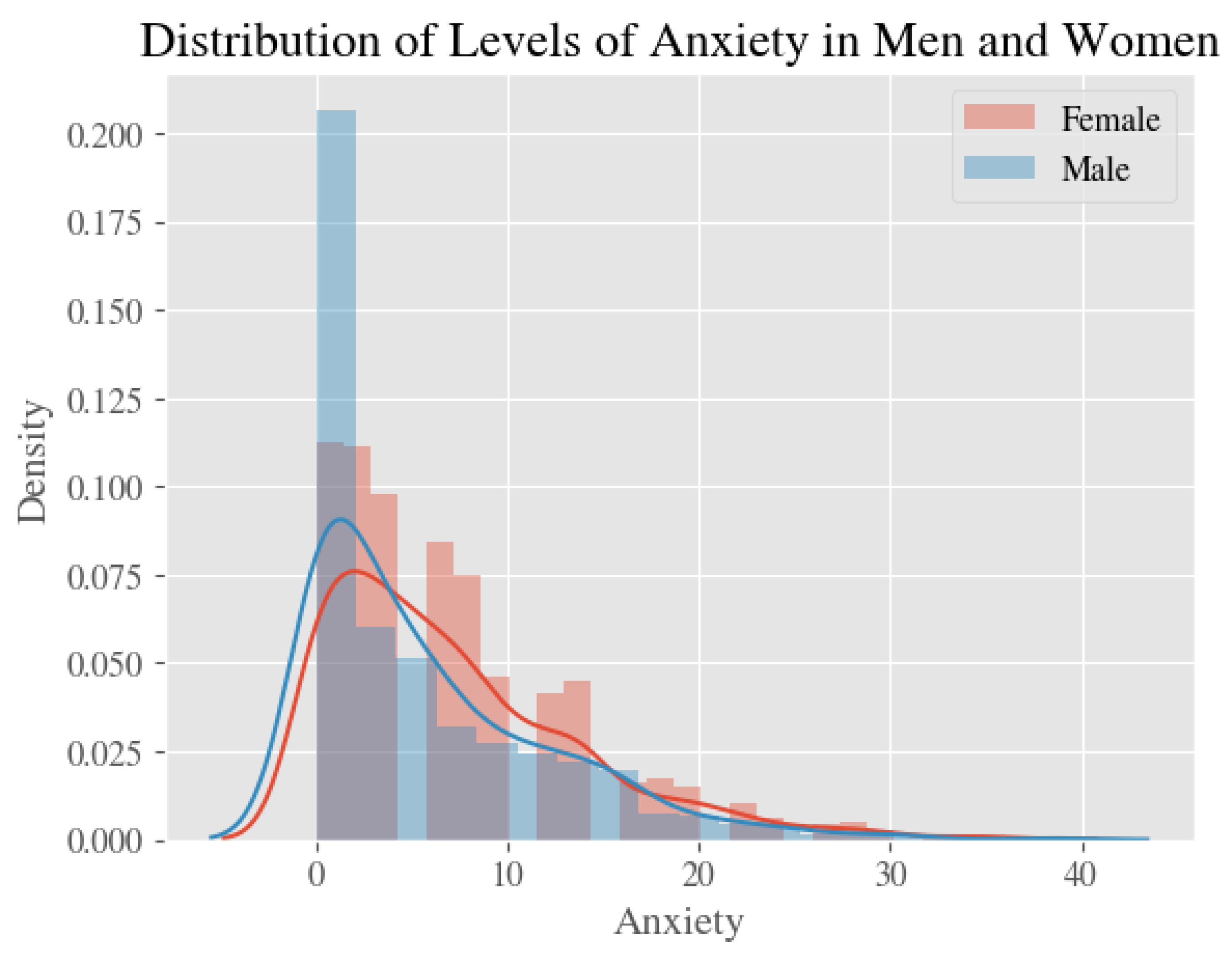
3.4. Anxiety
3.5. Impacts of COVID-19
4. Discussion
Public Health Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 17 November 2022).
- Nochaiwong, S.; Ruengorn, C.; Thavorn, K.; Hutton, B.; Awiphan, R.; Phosuya, C.; Ruanta, Y.; Wongpakaran, N.; Wongpakaran, T. Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 10173. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Pandemic Triggers 25% Increase in Prevalence of Anxiety and Depression Worldwide. Available online: https://www.who.int/news/item/02-03-2022-covid-19-pandemic-triggers-25-increase-in-prevalence-of-anxiety-and-depression-worldwide (accessed on 17 November 2022).
- COVID-19 and Women’s Mental Health: The Impact on Wellbeing, Disparities, and Future Implications. Community Connection Magazine Baylor University. Available online: https://www.baylor.edu/communityconnection/news.php?action=story&story=222809 (accessed on 1 April 2021).
- Amatori, G.; Cappelli, A.; Carmassi, C.; Rodgers, R.F.; Bui, E. Impact of the COVID-19 pandemic on mental health among women: An editorial. Int. J. Ment. Health 2022, 51, 98–101. [Google Scholar] [CrossRef]
- Health, T.L.G. Mental health matters. Lancet Glob. Health 2020, 8, e1352. [Google Scholar] [CrossRef] [PubMed]
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stata Statistical Software, Release 16; StataCorp LLC: College Station, TX, USA, 2019.
- COVID-19 and Its Economic Toll on Women: The Story Behind the Numbers. UN Women—Headquarters. Retrieved. 2022. Available online: https://www.unwomen.org/en/news/stories/2020/9/feature-covid-19-economic-impacts-on-women (accessed on 17 November 2022).
- Madgavkar, A.; White, O.; Krishnan, M.; Mahajan, D.; Azcue, X. COVID-19 and Gender Equality: Countering the Regressive Effects. McKinsey Global Institute. 2020. Available online: https://www.mckinsey.com/featured-insights/future-of-work/covid-19-and-gender-equality-countering-the-regressive-effects (accessed on 17 November 2022).
- Mental Health—Household Pulse Survey—COVID-19. Available online: https://www.cdc.gov/nchs/covid19/pulse/mental-health.htm (accessed on 17 November 2022).
- Philippine Statistics Authority Republic of the Philippines. Available online: https://psa.gov.ph/vital-statistics (accessed on 17 November 2022).
- Yahoo! News Covid-19 Vaccination Survey (Yahoo! News Covid-19 Vaccination Survey). Yahoo News. 2021. Available online: https://docs.cdn.yougov.com/b7tjs9k8au/20210222_yahoo_vaccine_tabs.pdf (accessed on 17 November 2022).
- Beutel, M.E.; Klein, E.M.; Brähler, E.; Reiner, I.; Jünger, C.; Michal, M.; Wiltink, J.; Wild, P.S.; Münzel, T.; Lackner, K.J.; et al. Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry 2017, 17, 97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hwang, T.-J.; Rabheru, K.; Peisah, C.; Reichman, W.; Ikeda, M. Loneliness and social isolation during the COVID-19 pandemic. Int. Psychogeriatr. 2020, 32, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Clair, R.; Gordon, M.; Kroon, M.; Reilly, C. The effects of social isolation on well-being and life satisfaction during pandemic. Humanit. Soc. Sci. Commun. 2021, 8, 1. [Google Scholar] [CrossRef]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Study Finds Sex Differences in Mental Illness. Available online: https://www.apa.org/news/press/releases/2011/08/mental-illness (accessed on 12 January 2023).
- Smith, D.T.; Mouzon, D.M.; Elliott, M. Reviewing the Assumptions About Men’s Mental Health: An Exploration of the Gender Binary. Am. J. Men’s Health 2018, 12, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Women Bear Disproportionate Share of Covid-19 Burden, U.N. Official Warns. (n.d.). NBC News. Available online: https://www.nbcnews.com/news/world/covid-19-women-girls-bear-unequal-share-pandemic-burden-u-n1240681 (accessed on 17 November 2022).
- Philippine Commission on Women. Available online: https://pcw.gov.ph/ (accessed on 17 November 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total N = 1879 (100%) | Men N = 583 (31%) | Women N = 1296 (69%) |
|---|---|---|---|
| Age | |||
| ≤19 | 11.50% | 11.70% | 11.40% |
| 20–24 | 20.50% | 17.30% | 22.00% |
| 25–29 | 10.60% | 11.00% | 10.50% |
| 30–34 | 11.70% | 12.50% | 11.30% |
| ≥35 | 45.60% | 47.50% | 44.80% |
| Marital Status | |||
| Never Married | 63.70% | 65.20% | 63.00% |
| Ever Married | 36.40% | 34.80% | 37.00% |
| Healthcare Professional | |||
| No | 33.40% | 34.20% | 33.00% |
| Yes | 66.60% | 65.80% | 67.00% |
| Household Size | |||
| 1 person | 5.70% | 5.80% | 5.60% |
| 2–5 people | 63.60% | 66.70% | 62.20% |
| ≥6 people | 30.70% | 27.40% | 32.20% |
| Parental Status | |||
| No | 65.80% | 67.90% | 64.80% |
| Yes | 34.20% | 32.10% | 35.20% |
| Employment Status | |||
| Unemployed | 38.40% | 36.70% | 39.20% |
| Employed | 61.60% | 63.30% | 60.80% |
| Education Status | |||
| <College | 7.08% | 7.03% | 7.10% |
| ≥College | 92.90% | 93.00% | 92.90% |
| Traveled | |||
| No | 1.70% | 1.50% | 1.70% |
| Yes | 98.40% | 98.50% | 98.30% |
| Measures | Total (Mean, 95% CI) | Among Men (Mean, 95% CI) | Among Women (Mean, 95% CI) |
|---|---|---|---|
| Stress [0–42] | 10.1 (9.75–10.47) | 8.9 (8.29–9.55) | 10.6 (10.21–11.08) |
| Anxiety [0–32] | 6.8 (6.50–7.09) | 6.0 (5.45–6.49) | 7.2 (6.80–7.52) |
| Depression [0–42] | 9.0 (8.64–9.43) | 8.1 (7.44–8.85) | 9.4 (8.96–9.91) |
| IESR [0–81] | 19.6 (19.0–20.2) | 17.7 (16.66–18.75) | 20.4 (19.69–21.12) |
| a: Bivariate analysis of socio-demographic factors and psychosocial well-being among men. | ||||
| Socio-Demographic Factors | % Not Stressed | % Not Depressed | % Not Anxious | % Not Impacted by COVID (IESR Scale) |
| Age | ||||
| ≤19 | 11.60% | 11.30% | 11.50% | 10.80% |
| 20–24 | 13.10% | 14.30% | 13.50% | 15.70% |
| 25–29 | 10.50% | 10.80% | 10.40% | 10.00% |
| 30–34 | 13.10% | 11.30% | 11.20% | 11.50% |
| ≥35 | 51.70% | 52.30% | 53.40% | 52.10% |
| (p = 0.019) | (p = 0.000) | (p = 0.001) | (p = 0.009) | |
| Marital Status | ||||
| Never Married | 59.80% | 60.40% | 58.50% | 60.80% |
| Ever Married | 40.20% | 39.60% | 41.50% | 39.20% |
| (p = 0.000) | (p = 0.000) | (p = 0.000) | (p = 0.002) | |
| Healthcare Professional | ||||
| No | 35.60% | 35.00% | 36.70% | 38.10% |
| Yes | 64.40% | 65.00% | 63.30% | 61.90% |
| (p = 0.115) | (p = 0.048) | (p = 0.001) | (p = 0.004) | |
| Household Size | ||||
| 1 person | 6.00% | 4.38% | 4.30% | 5.10% |
| 2–5 people | 66.40% | 68.00% | 67.20% | 67.80% |
| ≥6 people | 27.60% | 27.70% | 28.50% | 27.10% |
| (p = 0.001) | (p = 0.001) | (p = 0.012) | (p = 0.777) | |
| Parental Status | ||||
| No | 63.50% | 64.30% | 62.60% | 65.20% |
| Yes | 36.50% | 35.70% | 37.40% | 34.80% |
| (p = 0.004) | (p = 0.002) | (p = 0.000) | (p = 0.034) | |
| Employment Status | ||||
| Unemployed | 34.10% | 35.00% | 34.90% | 34.10% |
| Employed | 65.90% | 65.00% | 65.10% | 65.90% |
| (p = 0.032) | (p = 0.103) | (p = 0.160) | (p = 0.011) | |
| Education Status | ||||
| <College | 6.80% | 7.40% | 7.10% | 6.80% |
| ≥College | 93.20% | 92.60% | 92.90% | 93.20% |
| (p = 0.764) | (p = 0.508) | (p = 0.304) | (p = 0.009) | |
| Traveled | ||||
| No | 1.80% | 1.60% | 1.30% | 1.60% |
| Yes | 98.20% | 98.40% | 98.70% | 98.40% |
| (p = 0.182) | (p = 0.353) | (p = 0.326) | (p = 0.919) | |
| b: Bivariate analysis of socio-demographic factors and psychosocial well-being among women. | ||||
| Socio-demographic factors | % Not Stressed | % Not Depressed | % Not Anxious | % Not Impacted by COVID (IESR Scale) |
| Age | ||||
| ≤19 | 11.10% | 9.70% | 9.80% | 10.00% |
| 20–24 | 17.90% | 20.10% | 19.60% | 19.40% |
| 25–29 | 11.10% | 10.00% | 9.70% | 9.00% |
| 30–34 | 10.80% | 11.30% | 11.10% | 11.00% |
| ≥35 | 49.20% | 48.90% | 49.70% | 50.50% |
| (p = 0.000) | (p = 0.000) | (p = 0.000) | (p = 0.000) | |
| Marital Status | ||||
| Never Married | 59.50% | 59.50% | 59.00% | 59.60% |
| Ever Married | 40.50% | 40.50% | 41.00% | 40.40% |
| (p = 0.000) | (p = 0.001) | (p = 0.001) | (p = 0.001) | |
| Healthcare Professional | ||||
| No | ||||
| Yes | 33.70% | 34.40% | 35.70% | 35.80% |
| 66.30% | 65.60% | 64.30% | 64.30% | |
| (p = 0.458) | (p = 0.233) | (p = 0.201) | (p = 0.015) | |
| Household Size | ||||
| 1 person | 5.70% | 5.60% | 5.80% | 5.40% |
| 2–5 people | 63.70% | 62.00% | 62.20% | 62.30% |
| ≥6 people | 30.50% | 32.40% | 32.10% | 32.30% |
| (p = 0.619) | (p = 0.790) | (p = 0.975) | (p = 0.686) | |
| Parental Status | ||||
| No | 61.70% | 61.60% | 61.10% | 61.70% |
| Yes | 38.30% | 38.40% | 38.90% | 38.30% |
| (p = 0.000) | (p = 0.004) | (p = 0.002) | (p = 0.002) | |
| Employment Status | ||||
| Unemployed | 38.30% | 37.80% | 38.20% | 37.10% |
| Employed | 61.70% | 62.20% | 61.80% | 62.90% |
| (p = 0.053) | (p = 0.491) | (p = 0.244) | (p = 0.084) | |
| Education Status | ||||
| <College | 7.50% | 6.30% | 6.70% | 7.30% |
| ≥College | 92.50% | 93.70% | 93.30% | 92.70% |
| (p = 0.603) | (p = 0.531) | (p = 0.252) | (p = 0.263) | |
| Traveled | ||||
| No | 1.70% | 1.60% | 1.40% | 1.20% |
| Yes | 98.30% | 98.50% | 98.60% | 98.80% |
| (p = 0.166) | (p = 0.710) | (p = 0.214) | (p = 0.224) | |
| Stress OR, CI, p-Value * | Depression OR, CI, p-Value * | Anxiety OR, CI, p-Value * | IESR OR, CI, p-Value * | |
|---|---|---|---|---|
| Women (ref) | 1 | 1 | 1 | 1 |
| Men | 0.51 (0.38, 0.68) *** | 0.70(0.54, 0.90) ** | 0.56(0.44, 0.71) *** | 0.46 (0.25, 0.86) * |
| Men Odds Ratio, CI, p-Value * | Women Odds Ratio, CI, p-Value * | |
|---|---|---|
| (a) Stress | ||
| Age | ||
| ≤19 | ||
| 20–24 | 1.77 (0.95, 3.36) | 1.33 (0.89, 2.00) |
| 25–29 | 0.98 (0.41, 2.32) | 0.63 (0.36, 1.08) |
| 30–34 | 0.87 (0.36, 2.11) | 0.80 (0.46, 1.39) |
| ≥35 | 0.89 (0.39, 2.06) | 0.58 (0.34, 0.98) * |
| Marital Status | ||
| Never Married | ||
| Ever Married | 0.61 (0.30, 1.25) | 0.94 (0.62, 1.41) |
| Healthcare Professional | ||
| No | ||
| Yes | 0.95 (0.62, 1.44) | |
| Household Size | ||
| 1 person | ||
| 2–5 people | 1.22 (0.54, 2.76) | |
| ≥6 people | 1.10 (0.46, 2.62) | |
| Parental Status | ||
| No | ||
| Yes | 0.90 (0.45, 1.81) | 1.02 (0.69, 1.51) |
| Employment Status | ||
| Unemployed | ||
| Employed | 1.21 (0.70, 2.10) | 1.37 (1.00, 1.88) |
| Education Status | ||
| <College | ||
| ≥College | ||
| Traveled | ||
| No | ||
| Yes | 1.79 (0.35, 9.04) | 0.90 (0.38, 2.15) |
| (b) Depression: | ||
| Men Odds Ratio, CI, p-Value * | Women Odds Ratio, CI, p-Value * | |
| Age | ||
| ≤19 | ||
| 20–24 | 1.38 (0.70, 2.72) | 0.83 (0.55, 1.25) |
| 25–29 | 0.62 (0.24, 1.62) | 0.76 (0.47, 1.23) |
| 30–34 | 0.91(0.35, 2.34) | 0.68 (0.42, 1.11) |
| ≥35 | 0.50 (0.20, 1.25) | 0.52 (0.32, 0.82) * |
| Marital Status | ||
| Never Married | ||
| Ever Married | 0.46 (0.20, 1.04) | 0.91 (0.58, 1.42) |
| Healthcare Professional | ||
| No | ||
| Yes | 0.86 (0.54, 1.37) | |
| Household Size | ||
| 1 person | ||
| 2–5 people | 0.42 (0.19, 0.94) * | |
| ≥6 people | 0.39 (0.16, 0.92) * | |
| Parental Status | ||
| No | ||
| Yes | 1.39 (0.63, 3.06) | 0.93 (0.60, 1.42) |
| Employment Status | ||
| Unemployed | ||
| Employed | ||
| 1.47 (0.79, 2.71) | ||
| Education Status | ||
| <College | ||
| ≥College | ||
| Traveled | ||
| No | ||
| Yes | ||
| (c) Anxiety | ||
| Men Odds Ratio, CI, p-Value * | Women Odds Ratio, CI, p-Value * | |
| Age | ||
| ≤19 | ||
| 20–24 | 1.58 (0.83, 3.03) | 0.92 (0.62, 1.38) |
| 25–29 | 0.80 (0.33, 1.96) | 0.87 (0.54, 1.38) |
| 30–34 | 1.14 (0.47, 2.76) | 0.77 (0.48, 1.24) |
| ≥35 | 0.68 (0.29, 1.60) | 0.58 (0.37, 0.91) * |
| Marital Status | ||
| Never Married | ||
| Ever Married | 0.46 (0.22, 0.97) | 0.95 (0.63, 1.43) |
| Healthcare Professional | ||
| No | ||
| Yes | 1.12 (0.73, 1.73) | |
| Household Size | ||
| 1 person | ||
| 2–5 people | 0.50 (0.23, 1.11) | |
| ≥6 people | 0.43 (0.18, 1.00) | |
| Parental Status | ||
| No | ||
| Yes | 1.16 (0.56, 2.41) | 0.94 (0.64, 1.39) |
| Employment Status | ||
| Unemployed | ||
| Employed | 1.44 (0.82, 2.56) | |
| Education Status | ||
| <College | ||
| ≥College | ||
| Traveled | ||
| No | ||
| Yes | ||
| (d) IESR | ||
| Men Odds Ratio, CI, p-Value * | Women Odds ratio, CI, p-Value * | |
| Age | ||
| ≤19 | ||
| 20–24 | 1.11 (0.56, 2.23) | 0.98 (0.65, 1.48) |
| 25–29 | 1.43(0.55, 3.76) | 0.95 (0.55, 1.65) |
| 30–34 | 1.79 (0.69, 4.66) | 0.66 (0.37, 1.18) |
| ≥35 | 1.05 (0.41, 2.64) | 0.36 (0.21, 0.64) *** |
| Marital Status | ||
| Never Married | ||
| Ever Married | 0.37 (0.16, 0.82) * | 1.22 (0.78, 1.91) |
| Healthcare Professional | ||
| No | ||
| Yes | 1.78 (1.10, 2.86) * | 1.22 (0.92, 1.60) |
| Household Size | ||
| 1 person | ||
| 2–5 people | ||
| ≥6 people | ||
| Parental Status | ||
| No | ||
| Yes | 1.68 (0.77, 3.63) | 1.08 (0.71, 1.65) |
| Employment Status | ||
| Unemployed | ||
| Employed | 0.95 (0.53, 1.70) | 1.17 (0.84, 1.63) |
| Education Status | ||
| <College | ||
| ≥College | 0.95 (0.62, 1.42) | |
| Traveled | ||
| No | ||
| Yes | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Periyakoil, D.; Periyakoil, P.; Tee, C.A.; Spanos, C.J.; Diener-West, M.; Tee, M.; Prata, N. Are There Differences between the Stress Responses of Philippine Men and Women to the COVID-19 Pandemic? Int. J. Environ. Res. Public Health 2023, 20, 2326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032326
Periyakoil D, Periyakoil P, Tee CA, Spanos CJ, Diener-West M, Tee M, Prata N. Are There Differences between the Stress Responses of Philippine Men and Women to the COVID-19 Pandemic? International Journal of Environmental Research and Public Health. 2023; 20(3):2326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032326
Chicago/Turabian StylePeriyakoil, Divya, Preethi Periyakoil, Cherica A. Tee, Costas J. Spanos, Marie Diener-West, Michael Tee, and Ndola Prata. 2023. "Are There Differences between the Stress Responses of Philippine Men and Women to the COVID-19 Pandemic?" International Journal of Environmental Research and Public Health 20, no. 3: 2326. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph20032326