Prostate Cancer Lesions by Zone and Race: Does Multiparametric MRI Demonstrate Racial Difference in Prostate Cancer Lesions for African American Men?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iremashvili, V.; Soloway, M.S.; Rosenberg, D.L.; Manoharan, M. Clinical and demographic characteristics associated with prostate cancer progression in patients on active surveillance. Urology 2012, 187, 1594–1599. [Google Scholar] [CrossRef]
- Moreira, D.M.; Presti, J.C.; Aronson, W.J.; Terris, M.K.; Kane, C.J.; Amling, C.L.; Sun, L.L.; Moul, J.W.; Freedland, S.J. The effect of race on the discriminatory accuracy of models to predict biochemical recurrence after radical prostatectomy: Results from the Shared Equal Access Regional Cancer Hospital and Duke Prostate Center databases. Prostate Cancer Prostatic Dis. 2010, 13, 87–93. [Google Scholar] [CrossRef]
- Tooker, G.M.; Truong, H.; Pinto, P.A.; Siddiqui, M. National Survey of Patterns Employing Targeted MRI/US Guided Prostate Biopsy in the Diagnosis and Staging of Prostate Cancer. Curr. Urol. 2018, 12, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.; Müller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef]
- McNeal, J.E.; Redwine, E.A.; Freiha, F.S.; Stamey, T.A. Zonal distribution of prostatic adenocarcinoma. Correlation with histologic pattern and direction of spread. Am. J. Surg. Pathol. 1988, 12, 897–906. [Google Scholar] [CrossRef] [PubMed]
- Kato, D.; Ozawa, K.; Takeuchi, S.; Kawase, M.; Kawase, K.; Nakai, C.; Takai, M.; Iinuma, K.; Nakane, K.; Kato, H.; et al. The Utility of Combined Target and Systematic Prostate Biopsies in the Diagnosis of Clinically Significant Prostate Cancer Using Prostate Imaging Reporting and Data System Version 2 Based on Biparametric Magnetic Resonance Imaging. Curr. Oncol. 2021, 28, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.P.; Lebastchi, A.H.; Horuz, R.; Lebastchi, A.H.; Horuz, R.; Rastinehad, A.R.; Siddiqui, M.M.; Grummet, J.; Kastner, C.; Ahmed, H.U.; et al. Role of multiparametric prostate MRI in the management of prostate cancer. World J. Urol. 2021, 39, 651–659. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, J.W.; Leinwand, G.; Feibus, A.H.; Haney, N.M.; Krane, L.S.; Thomas, R.; Sartor, O.; Silberstein, J.L. Prospective Observational Study of a Racially Diverse Group of Men on Active Surveillance for Prostate Cancer. Urology 2021, 148, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Cai, G.-H.; Yang, Q.-H.; Chen, W.-B.; Liu, Q.-Y.; Zeng, Y.-R.; Zeng, Y.-J. Diagnostic Performance of PI-RADS v2, Proposed Adjusted PI-RADS v2 and Biparametric Magnetic Resonance Imaging for Prostate Cancer Detection: A Preliminary Study. Curr. Oncol. 2021, 28, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- De Santis, C.E.; Siegel, R.L.; Sauer, A.; Miller, K.D.; Fedewa, S.; Alcaraz, K.I.; Jemal, A. Cancer statistics for African Americans, 2016: Progress and opportunities in reducing racial disparities. CA Cancer J. Clin. 2016, 66, 290–308. [Google Scholar] [CrossRef]
- Lagacé, F.; Ghazawi, F.M.; Le, M.; Savin, E.; Zubarev, A.; Powell, M.; Moreau, L.; Sasseville, D.; Popa, I.; Litvinov, I.V. Incidence and Mortality of Prostate Cancer in Canada during 1992–2010. Curr. Oncol. 2021, 28, 978–990. [Google Scholar] [CrossRef] [PubMed]
- Parimi, S.; Bondy, S.; Aparicio, M.; Sunderland, K.; Cho, J.; Bachand, F.; Chi, K.N.; Pickles, T.; Tyldesley, S. Presenting Stage and Risk Group in Men Dying of Prostate Cancer. Curr. Oncol. 2020, 27, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Dess, R.T.; Hartman, H.E.; Mahal, B.A.; Soni, P.D.; Jackson, W.C.; Cooperberg, M.R.; Amling, C.L.; Aronson, W.J.; Kane, C.J.; Terris, M.K.; et al. Association of Black Race with Prostate Cancer–Specific and Other-Cause Mortality. JAMA Oncol. 2019, 5, 975–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundi, D.; Ross, A.E.; Humphreys, E.B.; Han, M.; Partin, A.W.; Carter, H.B.; Schaeffer, E.M. African American en with very low-risk prostate cancer exhibit adverse oncologic outcomes after radical prostatectomy: Should active surveillance still be an option for them? J. Clin. Oncol. 2013, 31, 2991–2997. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schouten, M.G.; van der Leest, M.; Pokorny, M. Why and Where do We Miss Significant Prostate Cancer with Multi-parametric Magnetic Resonance Imaging followed by Magnetic Resonance-guided and Transrectal Ultrasound-guided Biopsy in Biopsy-naïve Men? Eur. Urol. 2017, 71, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Leinwand, G.Z.; Krane, L.S.; Silberstein, J.L. Rethinking active surveillance for prostate cancer in African American men. Transl. Androl. Urol. 2018, 7, S397–S410. [Google Scholar] [CrossRef] [PubMed]
- Odedina, F.T.; Akinremi, T.O.; Chinegwundoh, F.; Roberts, R.; Yu, D.-H.; Reams, R.R.; Freedman, M.L.; Rivers, B.; Green, B.L.; Kumar, N. Prostate cancer disparities in Black men of African descent: A comparative literature review of prostate cancer burden among Black men in the United States, Caribbean, United Kingdom, and West Africa. Infect. Agent Cancer 2009, 4 (Suppl. 1). [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ingersoll, T.N. The Slave Trade and the Ethnic Diversity of Louisiana’s Slave Community. In The African American Experience in Louisiana: Part A; Vincent, C., Ed.; University of Southwestern: Lafayette, LA, USA, 1999; Volume 37, pp. 133–161. [Google Scholar]
- Eibner, C.; Krull, H.; Brown, K.M.; Cefalu, M.; Mulcahy, A.W.; Pollard, M.S.; Shetty, K.; Adamson, D.A.; Amaral, E.F.L.; Armour, P.; et al. Current and Projected Characteristics and Unique Health Care Needs of the Patient Population Served by the Department of Veterans Affairs. RAND Health Q. 2016, 5, 13. [Google Scholar] [CrossRef]
- Schult, T.M.; Schmunk, S.K.; Marzolf, J.R.; Mohr, D.C. The Health Status of Veteran Employees Compared to Civilian Employees in Veterans Health Administration. Mil. Med. 2019, 184, e218–e224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brenner, L.A.; Hoisington, A.J.; Stearns-Yoder, K.A.; Stamper, C.E.; Heinze, J.D.; Postolache, T.T.; Hadidi, D.A.; Hoffmire, C.A.; Stanislawski, M.A.; Lowry, C.A. Military-Related Exposures, Social Determinants of Health, and Dysbiosis: The United States-Veteran Microbiome Project (US-VMP). Front. Cell. Infect. Microbiol. 2018, 8, 400. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographics (IQR) | Total | AA | Non-AA | p-Value |
|---|---|---|---|---|
| Number (%) | 246 (100%) | 166 (67.5%) | 80 (32.5%) | --- |
| Median age | 68.05 (7.8) | 68.0 (7.08) | 68.2 (8.96) | 0.87 |
| Median BMI | 28.9 (6.59) | 29.1 (6.71) | 28.4 (6.48) | 0.53 |
| Median Bx PSA (ng/ml) | 6.37 (4.69) | 6.34 (4.29) | 6.38 (5.10) | 0.74 |
| Median PSA density | 0.13 (0.12) | 0.13 (0.14) | 0.14 (0.10) | 0.89 |
| Median testosterone | 3.12 (1.16) | 3.19 (1.33) | 2.89 (1.13) | 0.15 |
| Median prostate volume TRUS | 46.8 (±29.4) | 48.3 (33.0) | 44.0 (23.8) | 0.58 |
| Median prostate volume MRI | 53.8 (40.1) | 56.0 (±40.6) | 50.3 (±33.3) | 0.16 |
| Previous Bx (%) | --- | --- | --- | --- |
| 199 (80.9%) | 136 (82%) | 63 (79%) | --- |
| 47 (19.1%) | 30 (18%) | 17 (21%) | 0.61 |
| Median total ROI count (%) | --- | --- | --- | --- |
| 246 (100%) | 166 (100%) | 80 (100%) | --- |
| 180 (73.2%) | 121 (72.9%) | 59 (73.8) | --- |
| 87 (35.3%) | 58 (34.9%) | 29 (36.3%) | --- |
| 24 (9.76%) | 15 (9.04%) | 9 (11.3%) | --- |
| 1 (0.41%) | 0 (0%) | 1 (1.25%) | --- |
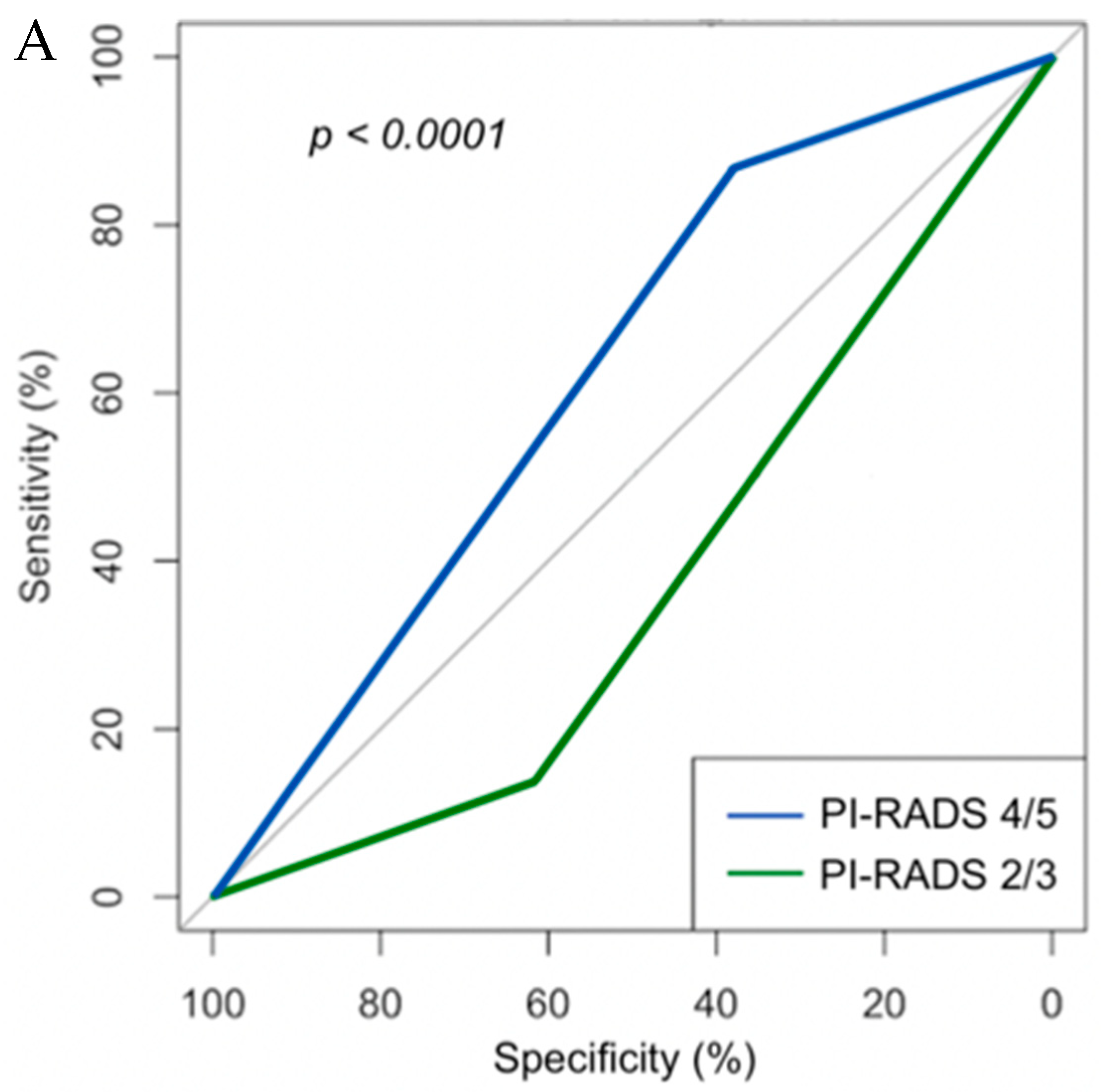
| Variable | OR (95% CI) | p-Value |
|---|---|---|
| Age | 1.03 (0.98–1.08) | 0.22 |
| BMI | 0.98 (0.93–1.03) | 0.38 |
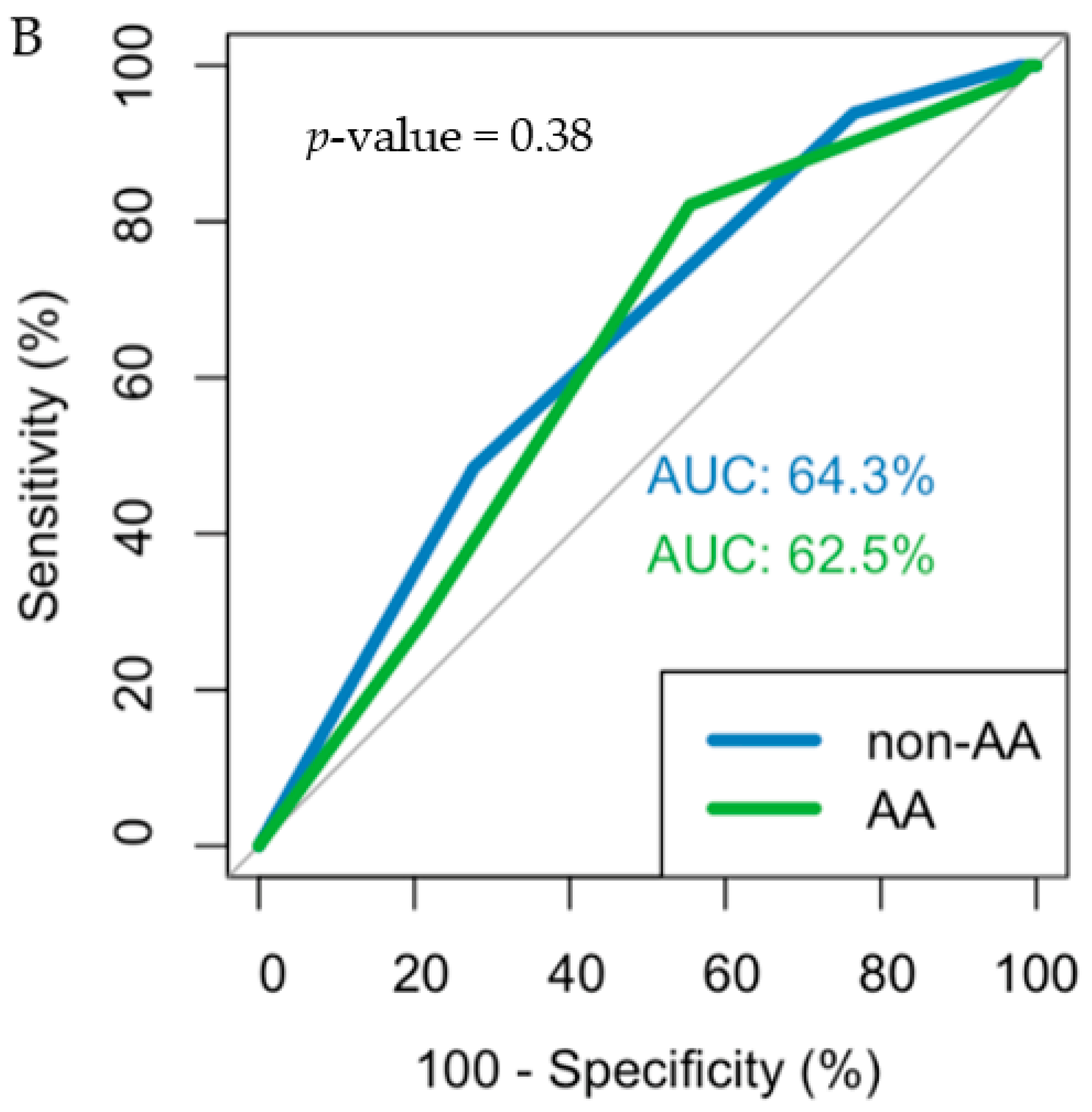
| Race | 1.05 (0.58–1.95) | 0.16 |
| PSA | 1.03 (0.99–1.12) | 0.35 |
| MRI volume | 0.97 (0.96–0.99) | <0.001 |
| PSAD | 0.60 (0.01–1.47) | 0.26 |
| PI-RADS score | 1.94 (1.34–2.87) | <0.001 |
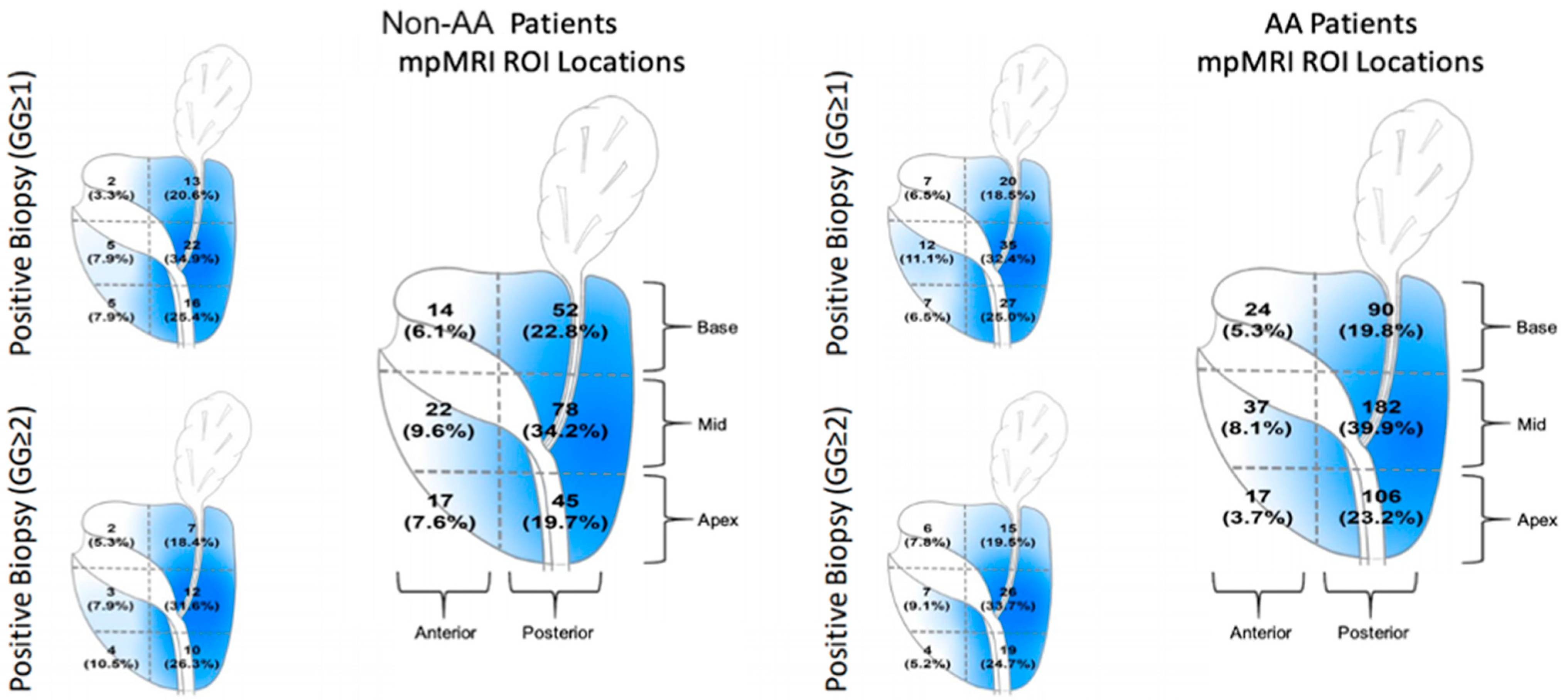
| ROI Location | AA | Non-AA | p-Value | ||
|---|---|---|---|---|---|
| n Positive | n Negative | n Positive | n Negative | ||
| GG ≥ 1 | |||||
| Overall (%) | 76 (23%) | 260 (77%) | 45 (26%) | 126 (74%) | 0.38 |
| Anterior lesion (%) | --- | --- | --- | --- | 0.83 |
| 5 (6%) | 26 (10%) | 2 (5%) | 7 (6%) | 0.64 |
| 5 (6%) | 9 (3.5%) | 4 (9%) | 22 (17%) | 0.23 |
| 9 (12%) | 9 (3.5%) | 6 (13%) | 4 (3%) | 0.71 |
| Transitional zone (%) | --- | --- | --- | --- | 0.99 |
| 4 (5%) | 18 (7%) | 1 (2%) | 6 (5%) | 0.99 |
| 4 (5%) | 14 (5%) | 0 (0%) | 6 (5%) | 0.54 |
| 0 (0%) | 6 (2%) | 2 (4%) | 5 (4%) | 0.46 |
| Peripheral zone (%) | --- | --- | --- | --- | 0.21 |
| 18 (24%) | 106 (41%) | 3 (7%) | 31 (25%) | 0.57 |
| 25 (33%) | 56 (22%) | 19 (42%) | 33 (26%) | 0.57 |
| 6 (8%) | 16 (6%) | 8 (18%) | 12 (9%) | 0.52 |
| GG ≥ 2 | |||||
| Overall (%) | 53 (16%) | 283 (84%) | 27 (16%) | 144 (84%) | 0.99 |
| Anterior lesion (%) | --- | --- | --- | --- | 0.99 |
| 2 (4%) | 29 (11%) | 0 (0%) | 9 (6%) | 0.99 |
| 3 (6%) | 11 (4%) | 2 (7.5%) | 24 (17%) | 0.32 |
| 7 (13%) | 11 (4%) | 6 (22%) | 4 (3%) | 0.43 |
| Transitional zone (%) | --- | --- | --- | --- | 0.26 |
| 4 (7.5%) | 18 (6%) | 1 (4%) | 6 (4%) | 0.99 |
| 4 (7.5%) | 14 (5%) | 0 (0%) | 6 (4%) | 0.54 |
| 0 (0%) | 6 (2%) | 0 (0%) | 7 (5%) | 0.99 |
| Peripheral zone (%) | --- | --- | --- | --- | 0.63 |
| 10 (19%) | 114 (40%) | 2 (7.5%) | 32 (22%) | 0.99 |
| 18 (34%) | 63 (22%) | 10 (37%) | 42 (29%) | 0.83 |
| 5 (9%) | 17 (6%) | 6 (22%) | 14 (10%) | 0.73 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koller, C.R.; Greenberg, J.W.; Shelton, T.M.; Hughes, W.M.; Sanekommu, G.; Silberstein, J.; Krane, L.S. Prostate Cancer Lesions by Zone and Race: Does Multiparametric MRI Demonstrate Racial Difference in Prostate Cancer Lesions for African American Men? Curr. Oncol. 2021, 28, 2308-2316. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040212
Koller CR, Greenberg JW, Shelton TM, Hughes WM, Sanekommu G, Silberstein J, Krane LS. Prostate Cancer Lesions by Zone and Race: Does Multiparametric MRI Demonstrate Racial Difference in Prostate Cancer Lesions for African American Men? Current Oncology. 2021; 28(4):2308-2316. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040212
Chicago/Turabian StyleKoller, Christopher R., Jacob W. Greenberg, Thomas M. Shelton, William M. Hughes, Ganesh Sanekommu, Jonathan Silberstein, and Louis S. Krane. 2021. "Prostate Cancer Lesions by Zone and Race: Does Multiparametric MRI Demonstrate Racial Difference in Prostate Cancer Lesions for African American Men?" Current Oncology 28, no. 4: 2308-2316. https://0-doi-org.brum.beds.ac.uk/10.3390/curroncol28040212