
Mechanical Comparison of a Novel Hybrid and Commercial Dorsal Double Plating for Distal Radius Fracture: In Vitro Fatigue Four-Point Bending and Biomechanical Testing


Abstract
:1. Introduction
2. Materials and Methods
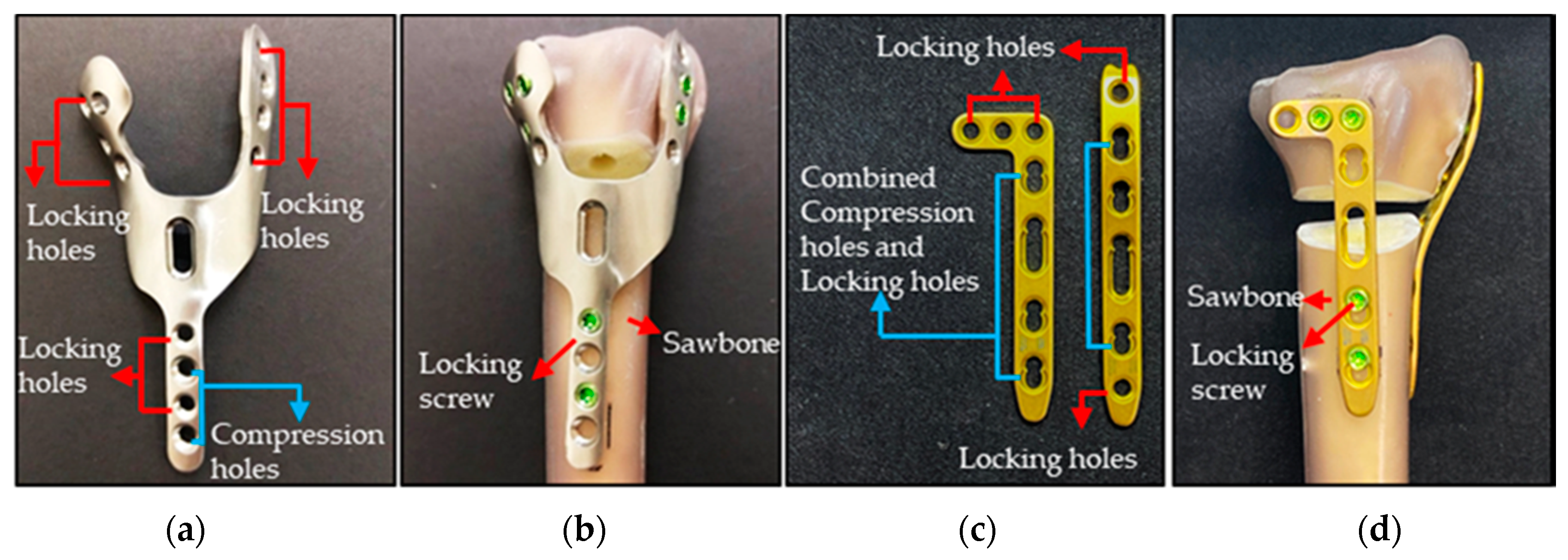
2.1. HDDP Design and Manufacture
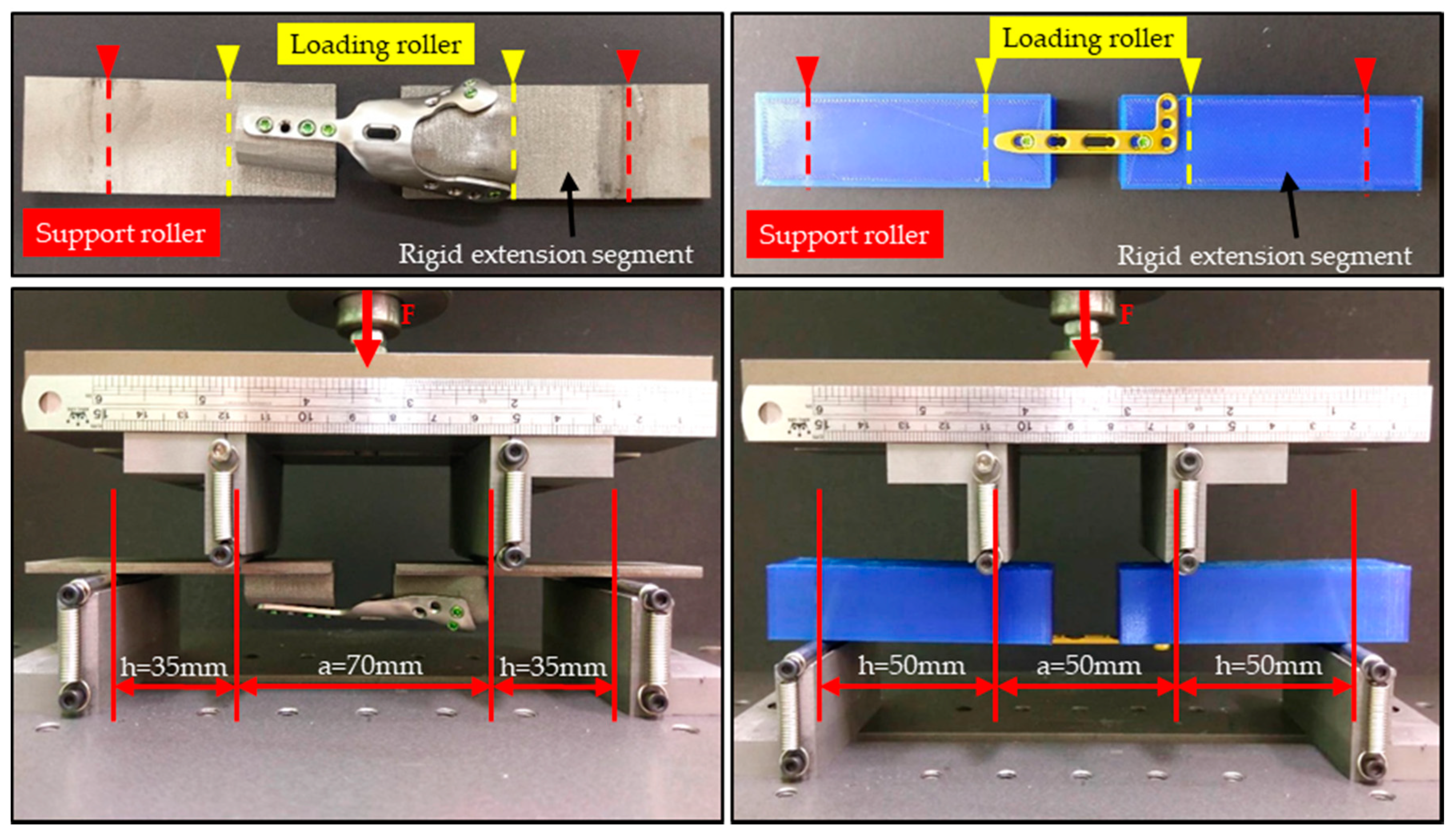
2.2. Four-Point Bending Mechanical Testing
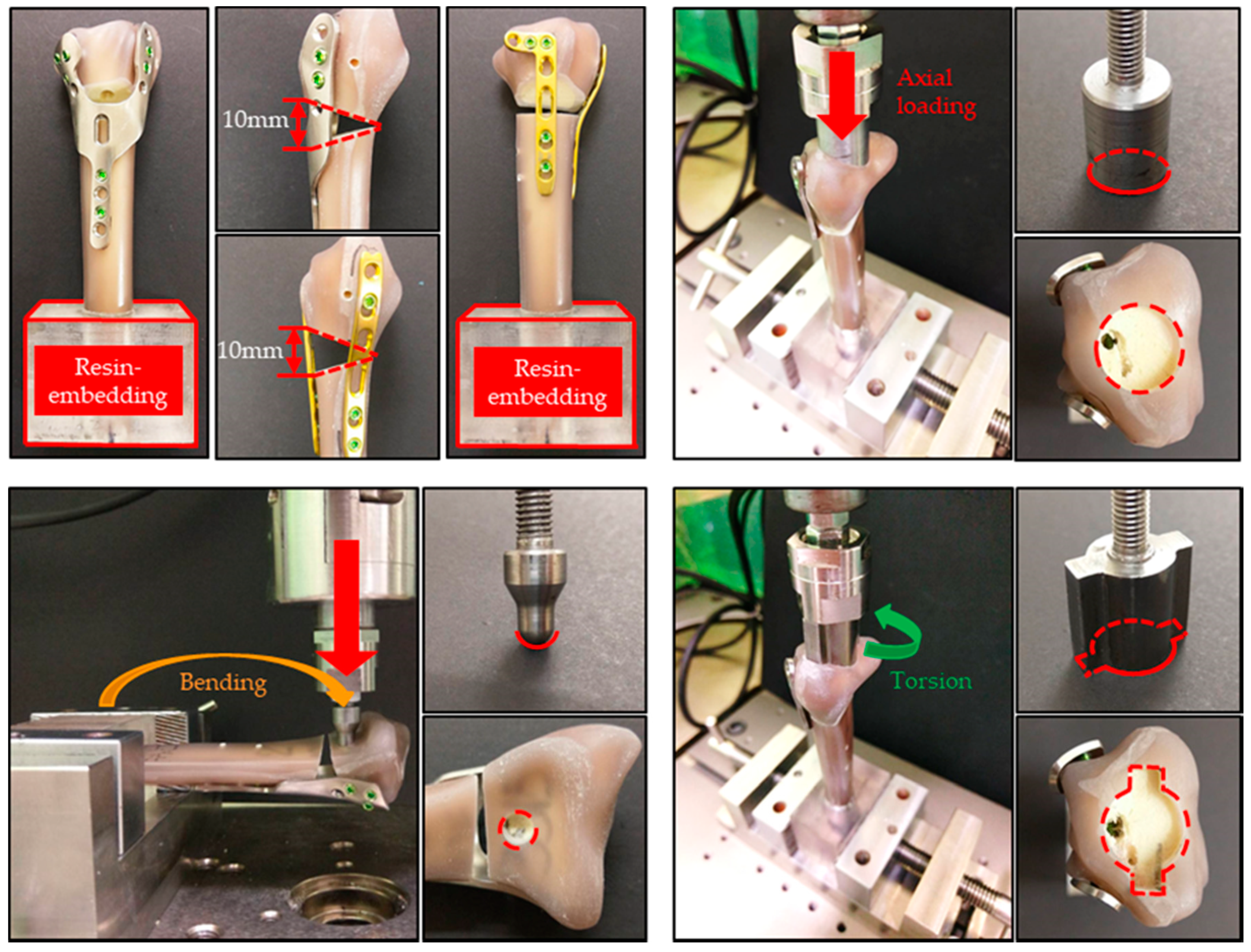
2.3. Biomechanical Fatigue Test
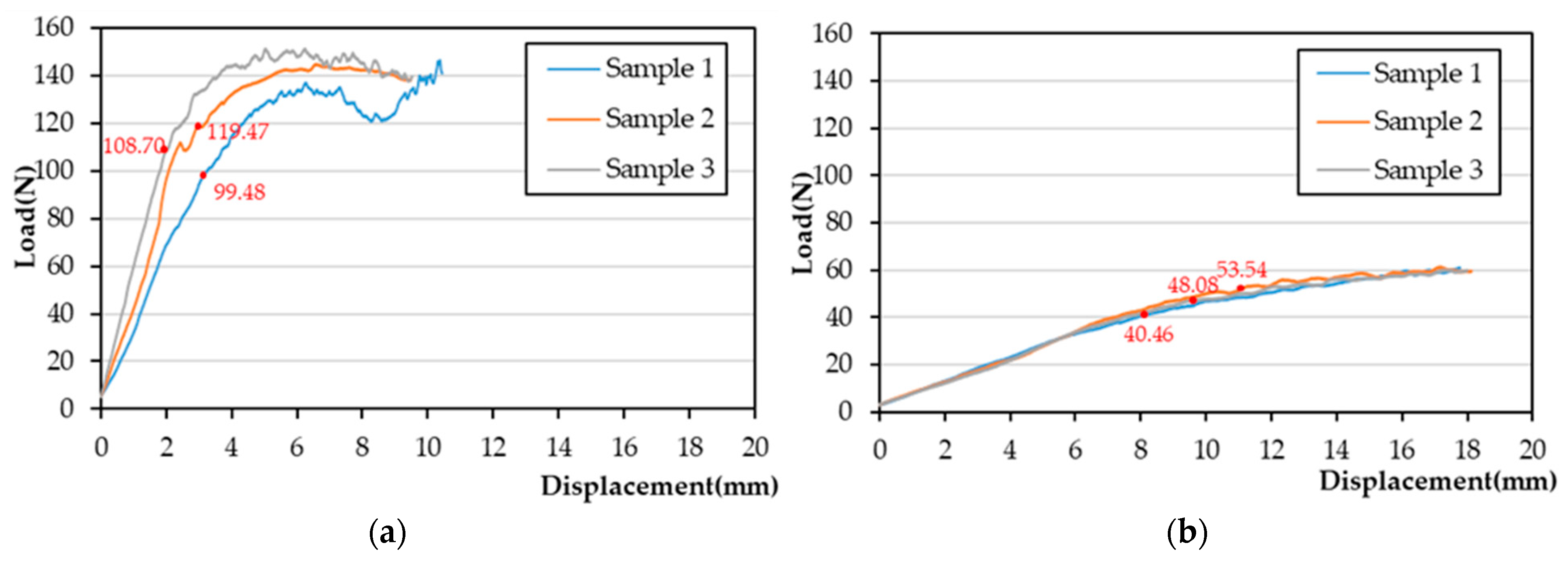
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Int. J. Care Inj. 2016, 37, 691–697. [Google Scholar] [CrossRef]
- Kevin, L.; Boyer, M.; Goldfarb, C. Dorsal locked plate fixation of distal radius fractures. J. Hand Surg. 2013, 38, 414–1422. [Google Scholar]
- Rikli, D.A.; Regazzoni, P. The double plating technique for distal radius fractures. Tech. Hand Up. Extrem. Surg. 2000, 4, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Chen, A.; Kuo, H.N.; Yu, T.C.; Sun, M.T.; Lin, C.L. Biomechanical evaluation of a modified dorsal double-plating fixation with adjustable joint and microthread designs for comminuted extra-articular distal radius fractures. J. Med. Biol. Eng. 2013, 33, 29–34. [Google Scholar] [CrossRef]
- Liu, H.C.; Jiang, J.S.; Lin, C.L. Biomechanical investigation of a novel hybrid dorsal double plating for distal radius fractures by integrating topology optimization and finite element analysis. Injury 2020, 51, 1271–1280. [Google Scholar] [CrossRef]
- Reed, J.D.; Stanbury, S.J.; Menorca, R.M.; Elfar, J.C. The emerging utility of composite bone models in biomechanical studies of the hand and upper extremity. J. Hand Surg. Am. 2013, 38, 583–587. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.; Lin, Y.H.; Kuo, H.N.; Yu, T.C.; Sun, M.T.; Lin, C.L. Design optimisation and experimental evaluation of dorsal double plating fixation for distal radius fracture. Int. J. Care Inj. 2013, 44, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Schorler, H.; Wendlandt, R.; Jürgens, C.; Schulz, A.P.; Kaddick, C.; Capanni, F. Bone plate-screw constructs for osteosynthesis—Recommendations for standardized mechanical torsion and bending tests. Biomed. Tech. 2018, 63, 719–727. [Google Scholar] [CrossRef]
- Lin, C.L.; Lin, Y.H.; Chen, A. Buttressing angle of the double-plating fixation of a distal radius fracture: A finite element study. Med. Bio. Eng. Comput. 2006, 44, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Chao, E.Y.; Opgrande, J.D.; Axmear, F.E. Three-dimensional force analysis of finger joints in selected isometric hand functions. J. Biomech. 1976, 9, 387–396. [Google Scholar] [CrossRef]
- Lill, H.; Hepp, P.; Korne, J.; Kassi, J.P.; Verheyden, A.P.; Josten, C.; Duda, G.N. Proximal humeral fractures: How stiff should an implant be? A comparative mechanical study with new implants in human specimens. Arch. Orthop. Trauma Surg. 2003, 123, 74–81. [Google Scholar] [CrossRef]
- Putnam, M.D.; Meyer, N.J.; Nelson, E.W.; Gesensway, D.; Lewis, J.L. Distal radial metaphyseal forces in an extrinsic grip model: Implications for post fracture rehabilitation. J. Hand Surg. Am. 2000, 25, 469–475. [Google Scholar] [CrossRef]
- Caiti, G.; Dobbe, J.G.G.; Bervoets, E.; Beerens, M.; Strackee, S.D.; Strijker, G.J.; Streekstra, G.J. Biomechanical considerations in the design of patient-specific fixation plates for the distal radius. Med. Biol. Eng. Comput. 2019, 57, 1099–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, H.Y.K.; Lin, C.L.; Lin, Y.H.; Chen, A. Biomechanical evaluation of the modified double-plating fixation for the distal radius fracture. Clin. Biomech. 2007, 22, 510–517. [Google Scholar] [CrossRef] [PubMed]
- Trease, C.; McIff, T.; Toby, E.B. Locking versus nonlocking T-plates for dorsal and volar fixation of dorsally comminuted distal radius fractures: A biomechanical study. J. Hand Surg. Am. 2005, 30, 756–763. [Google Scholar] [CrossRef]
- Ruch, D.S.; Papadonikolakis, A. Volar versus dorsal plating in the management of intra-articular distal radius fractures. J. Hand Surg. Am. 2006, 31, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Gondusky, J.S.; Carney, J.; Erpenbach, J.; Robertson, C.; Mahar, A.; Oka, R.; Thompson, M.; Mazurek, M. Biomechanical comparison of locking versus nonlocking volar and dorsal T-plates for fixation of dorsally comminuted distal radius fractures. J. Orthop. Trauma 2011, 25, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Ozer, K. Failure of volar locking plate fixation of an extraarticular distal radius fracture: A case report. Patient Saf. Surg. 2010, 4, 19. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Wu, W.D.; Fang, Y.F.; Zhang, M.C.; Huang, W.H. Biomechanical comparison of osteoporotic distal radius fractures fixed by distal locking screws with different length. PLoS ONE 2014, 9, e103371. [Google Scholar] [CrossRef]
- Cooney, W.P., 3rd; Chao, E.Y.S. Biomechanical analysis of static forces in the thumb during hand function. J. Bone Jt. Surg. Am. 1977, 59, 27–36. [Google Scholar] [CrossRef]
- Horii, E.; Garcia-Elias, M.; An, K.N.; Bishop, A.T.; Cooney, W.P.; Linscheid, R.L.; Chao, E.Y.S. Effect on force transmission across the carpus in procedures used to treat Kienbock’s disease. J. Hand Surg. Am. 1990, 15, 393–400. [Google Scholar] [CrossRef]
- Peine, R.; Rikli, D.A.; Hoffmann, R.; Duda, G.; Regazzoni, P. Comparison of three different plating techniques for the dorsum of the distal radius: A biomechanical study. J. Hand Surg. Am. 2000, 25, 29–33. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
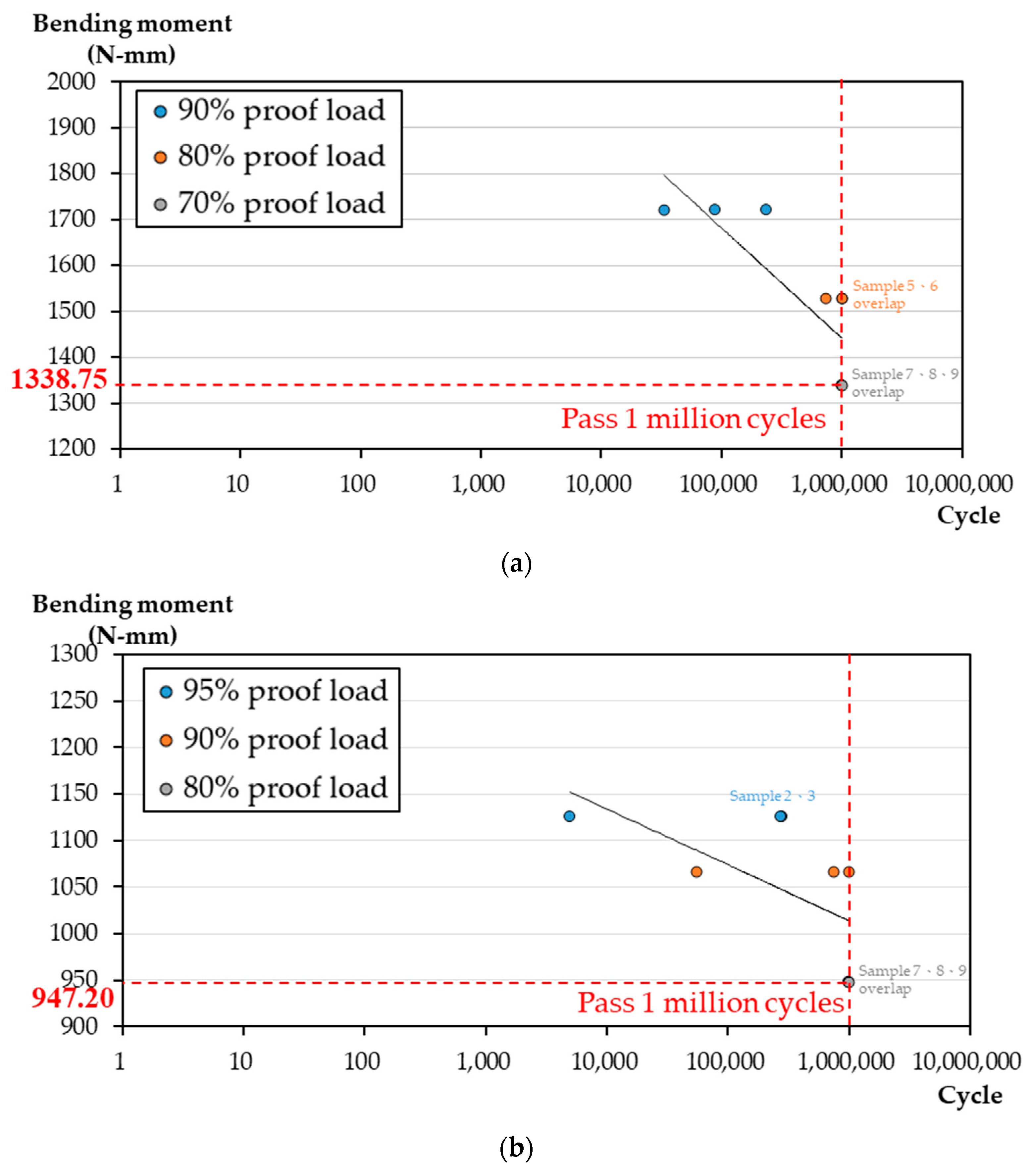
| % of Proof Load | Load (N) (Equal to Torque (N/mm)) | Sample Number | Cycle | Result | Temp/Humidity (°C/%) | |
|---|---|---|---|---|---|---|
| HDDP | 90% | 9.83~98.30 (172.03~1720.25) | 1 | 33,000 | Failure | 22 °C/70% |
| 2 | 89,000 | Failure | 22 °C/70% | |||
| 3 | 237,000 | Failure | 22 °C/70% | |||
| 80% | 8.74~87.40 (152.95~1529.5) | 4 | 729,000 | Failure | 22 °C/70% | |
| 5 | 1,000,000 | Pass | 22 °C/70% | |||
| 6 | 1,000,000 | Pass | 22 °C/70% | |||
| 70% | 7.65~76.50 (133.88~1338.75) | 7 | 1,000,000 | Pass | 22 °C/70% | |
| 8 | 1,000,000 | Pass | 22 °C/70% | |||
| 9 | 1,000,000 | Pass | 22 °C/70% | |||
| Synthes Dorsal Plate | 95% | 4.50~45.00 (112.50~1125.00) | 1 | 5000 | Failure | 22 °C/70% |
| 2 | 281,921 | Failure | 22 °C/70% | |||
| 3 | 272,272 | Failure | 22 °C/70% | |||
| 90% | 2.26~42.62 (106.56~1065.60) | 4 | 54,998 | Failure | 22 °C/70% | |
| 5 | 1,000,000 | Pass | 22 °C/70% | |||
| 6 | 739,758 | Failure | 22 °C/70% | |||
| 80% | 2.49~37.89 (94.72~947.20) | 7 | 1,000,000 | Pass | 22 °C/70% | |
| 8 | 1,000,000 | Pass | 22 °C/70% | |||
| 9 | 1,000,000 | Pass | 22 °C/70% |
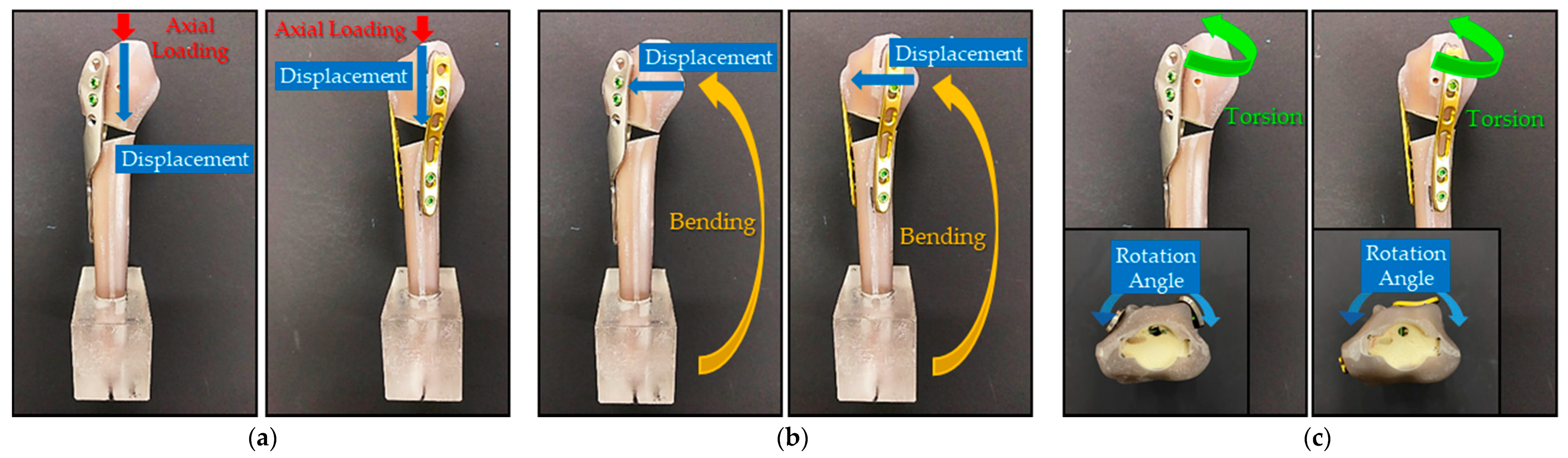
| Axial Loading Maximum Axial Displacement (mm) | Bending Maximum Bending Displacement (mm) | Torsion Maximum Angular Displacement (Degree) | ||||
|---|---|---|---|---|---|---|
| HDDP | DDP | HDDP | DDP | HDDP | DDP | |
| Sample 1 | 0.3797 | 0.8941 | 1.8203 | 1.4245 | 2.3499 | 2.7659 |
| Sample 2 | 0.3818 | 0.3076 | 1.8911 | 3.2378 | 1.3718 | 1.5019 |
| Sample 3 | 0.5039 | 0.3471 | 1.5754 | 1.4113 | 2.1659 | 1.2032 |
| Average Value (Standard deviation) | 0.4218 (0.0581) | 0.5162 (0.2676) | 1.7623 (0.1353) | 2.0245 (0.8579) | 1.9625 (0.4244) | 1.8237 (0.6774) |
| t-test (α = 0.05) | p-value = 0.3370 > 0.05 no significant difference | p-value = 0.3555 > 0.05 no significant difference | p-value = 0.4109 > 0.05 no significant difference | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.-C.; Zeng, Y.-H.; Lin, C.-L. Mechanical Comparison of a Novel Hybrid and Commercial Dorsal Double Plating for Distal Radius Fracture: In Vitro Fatigue Four-Point Bending and Biomechanical Testing. Materials 2021, 14, 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14206189
Liu H-C, Zeng Y-H, Lin C-L. Mechanical Comparison of a Novel Hybrid and Commercial Dorsal Double Plating for Distal Radius Fracture: In Vitro Fatigue Four-Point Bending and Biomechanical Testing. Materials. 2021; 14(20):6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14206189
Chicago/Turabian StyleLiu, Hsuan-Chih, Yu-Hui Zeng, and Chun-Li Lin. 2021. "Mechanical Comparison of a Novel Hybrid and Commercial Dorsal Double Plating for Distal Radius Fracture: In Vitro Fatigue Four-Point Bending and Biomechanical Testing" Materials 14, no. 20: 6189. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14206189