
Evaluation of Marginal/Internal Fit and Fracture Load of Monolithic Zirconia and Zirconia Lithium Silicate (ZLS) CAD/CAM Crown Systems



Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of the Master and Working Dies
2.2. Preparation of Test Samples
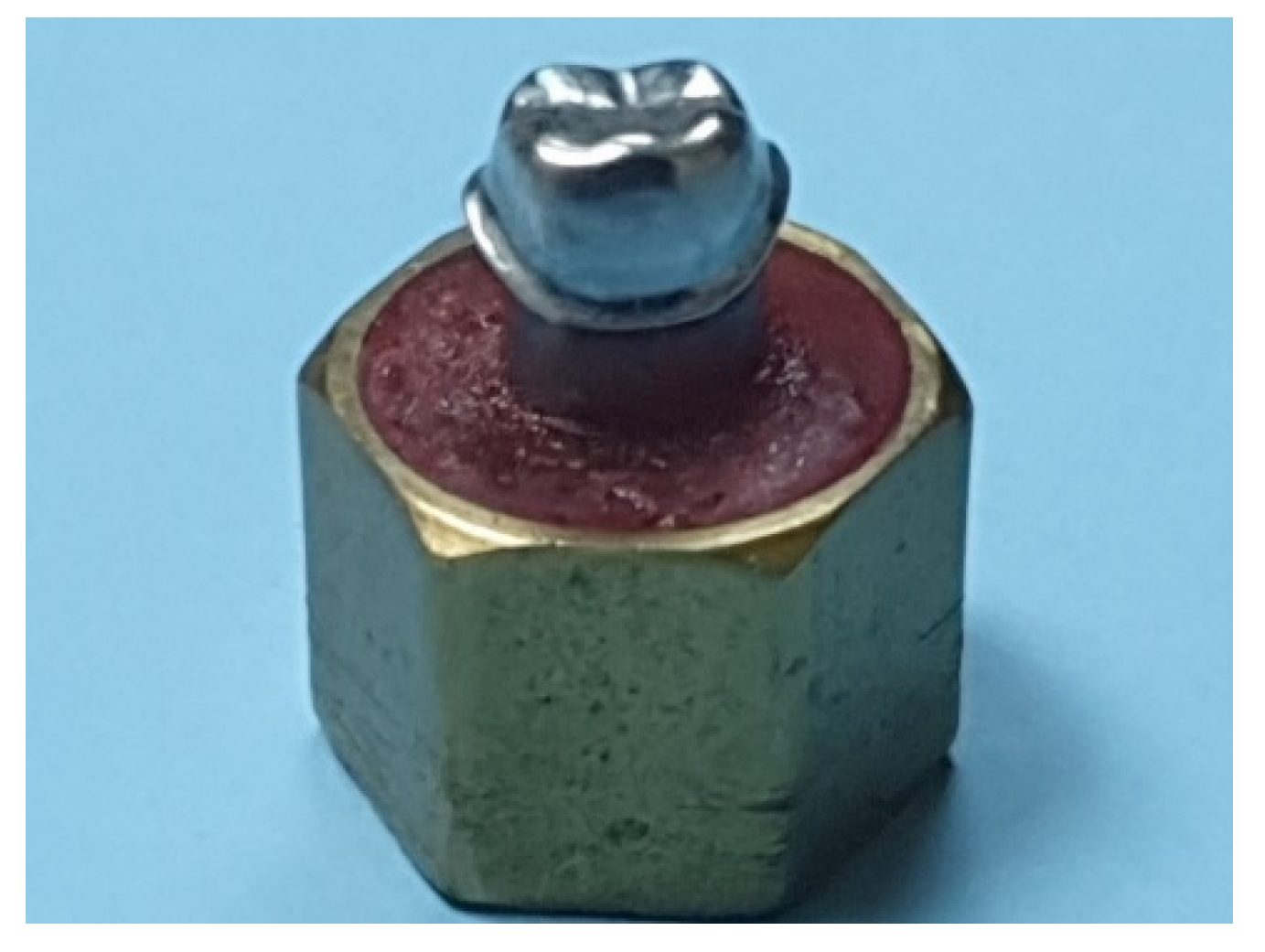
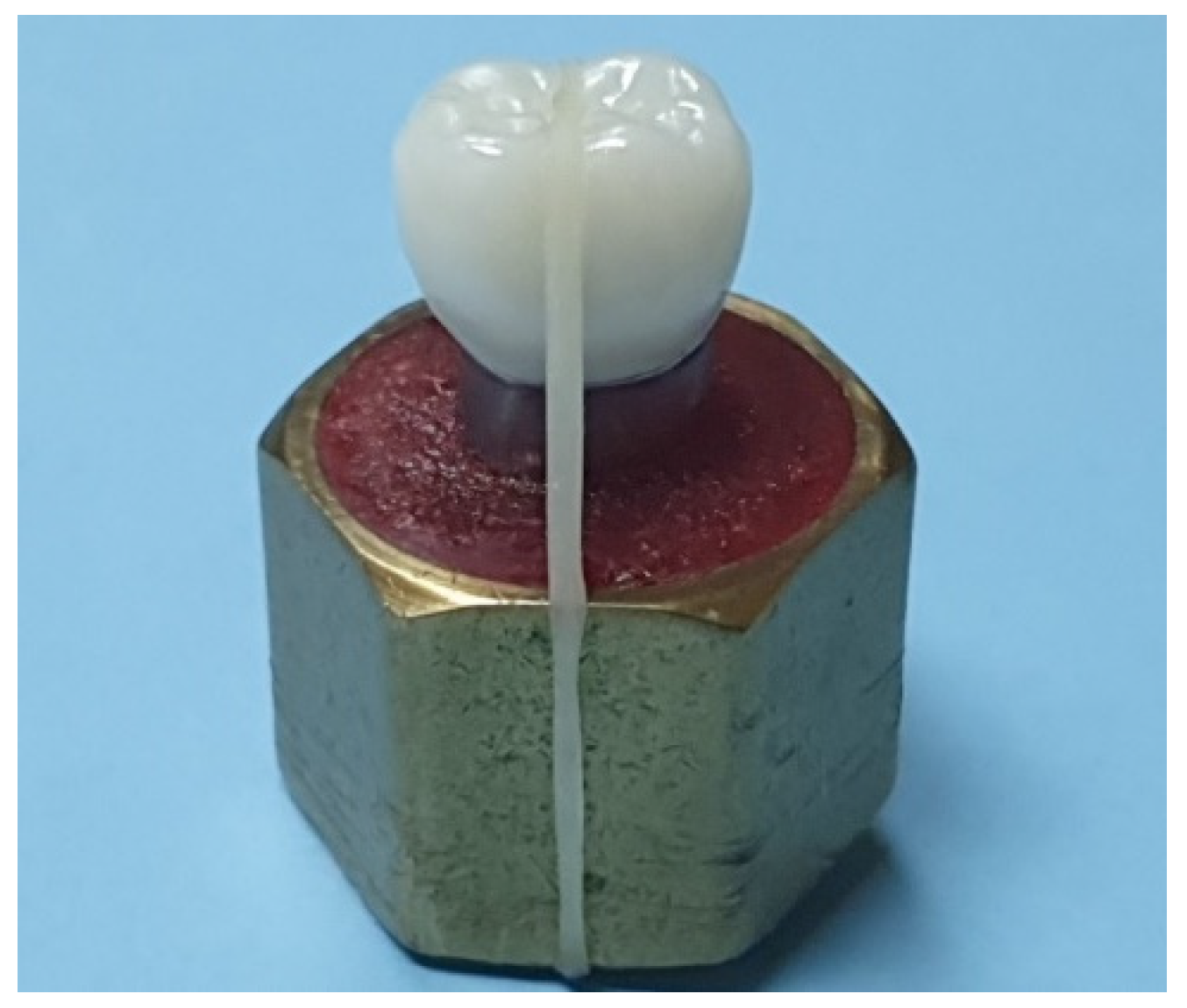
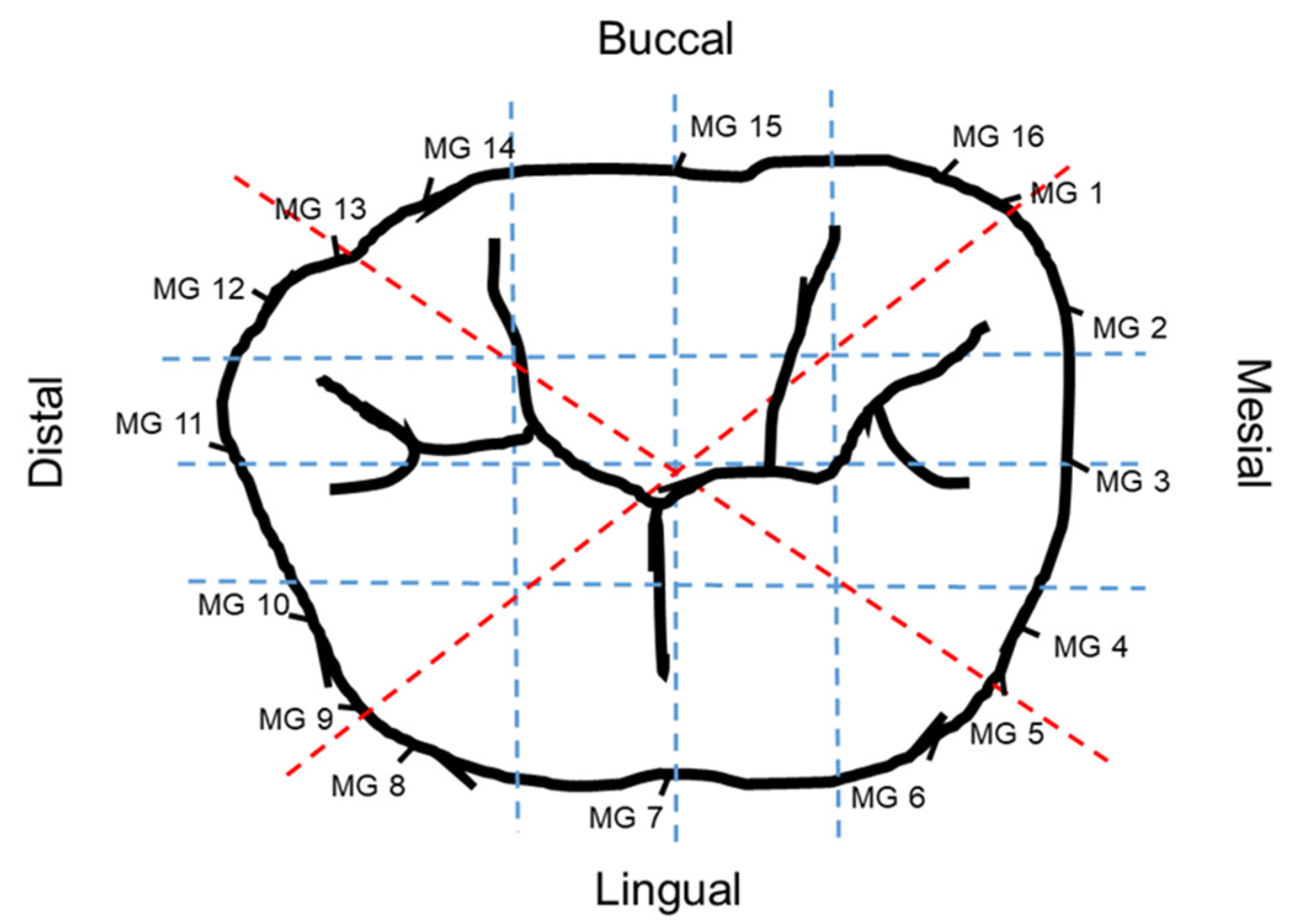
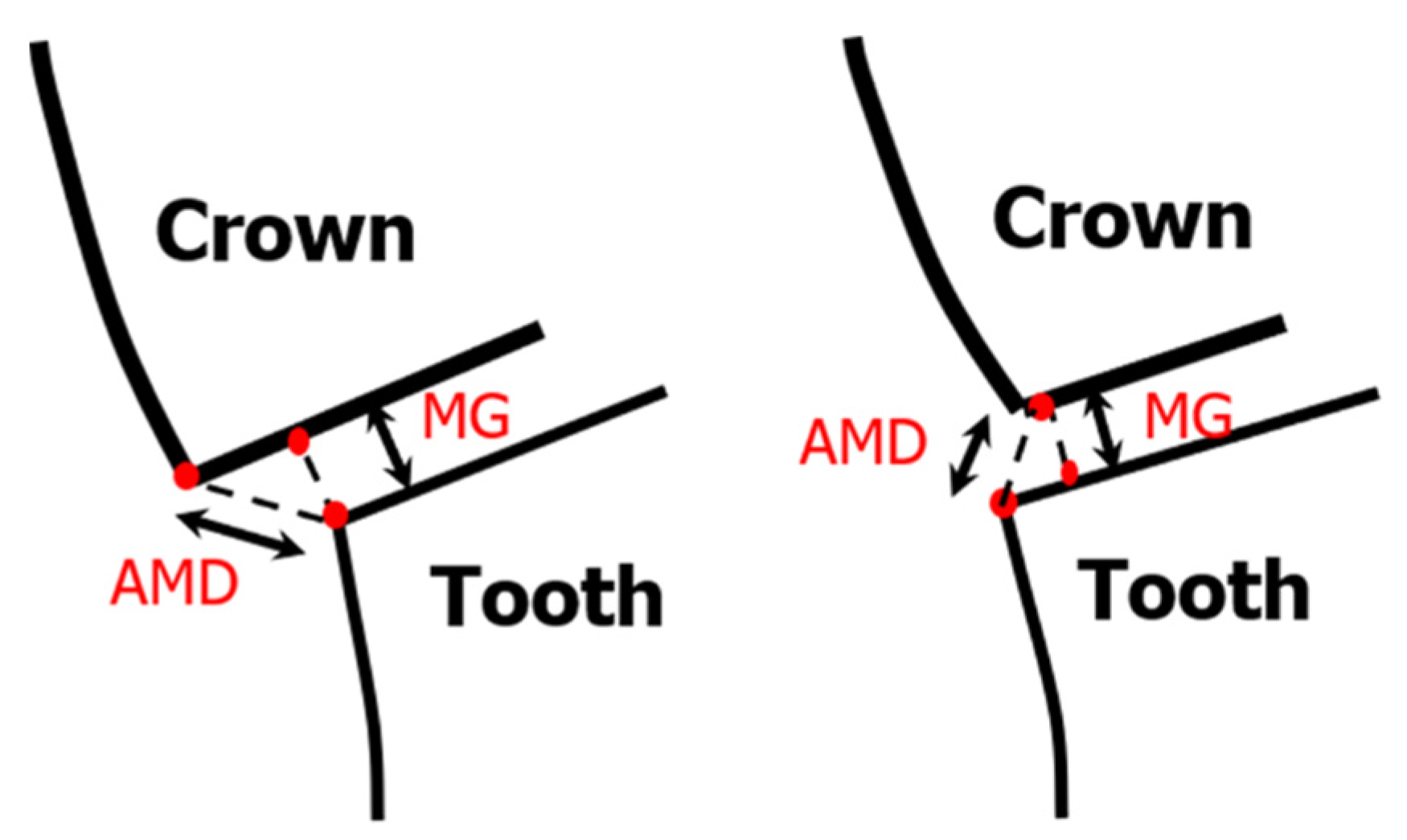
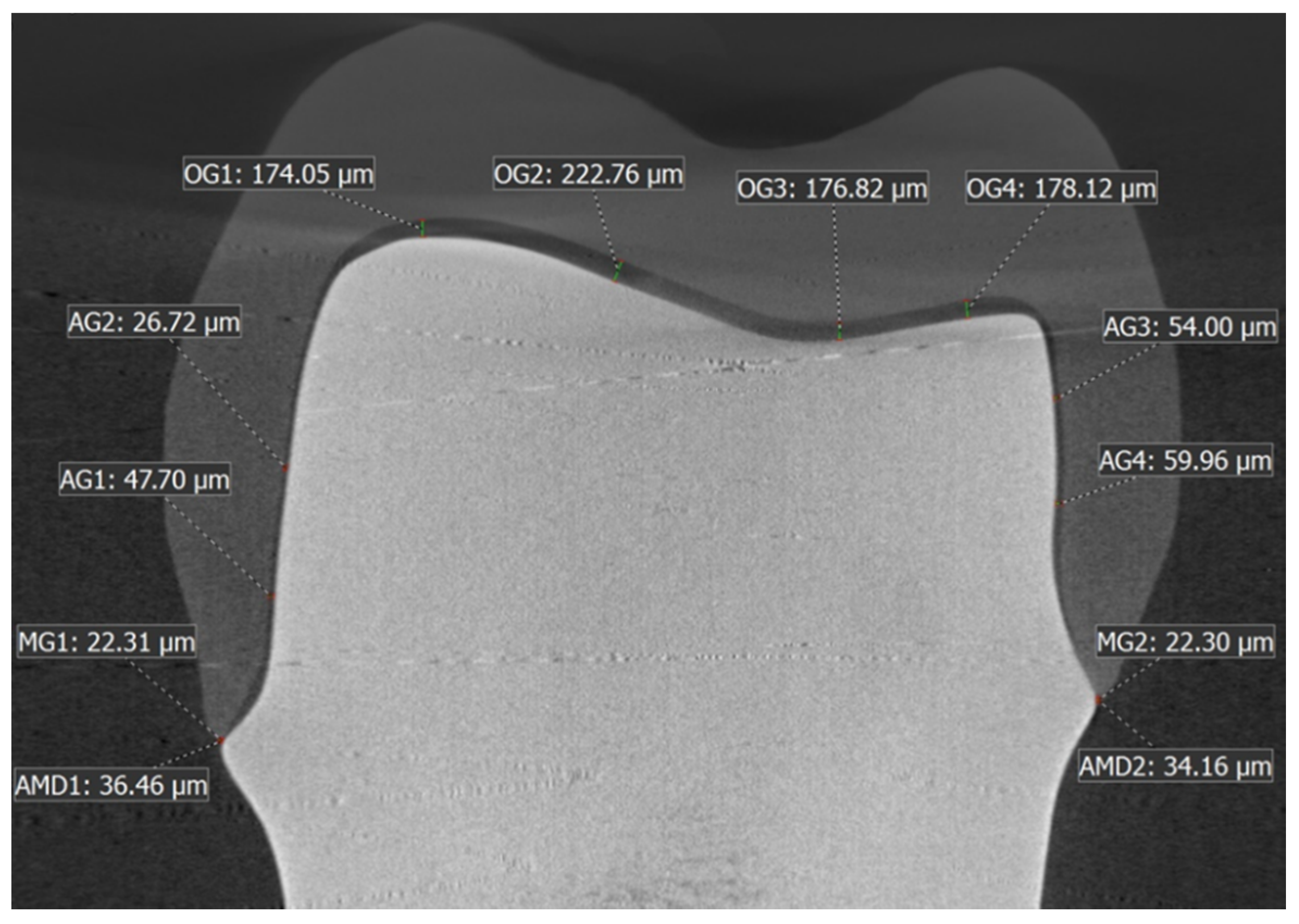
2.3. Evaluation of Marginal/Internal Fit by Nano-CT
2.4. Cementation of Crown Samples on Metal Dies
2.5. Fatigue Testing (Cyclic Loading)
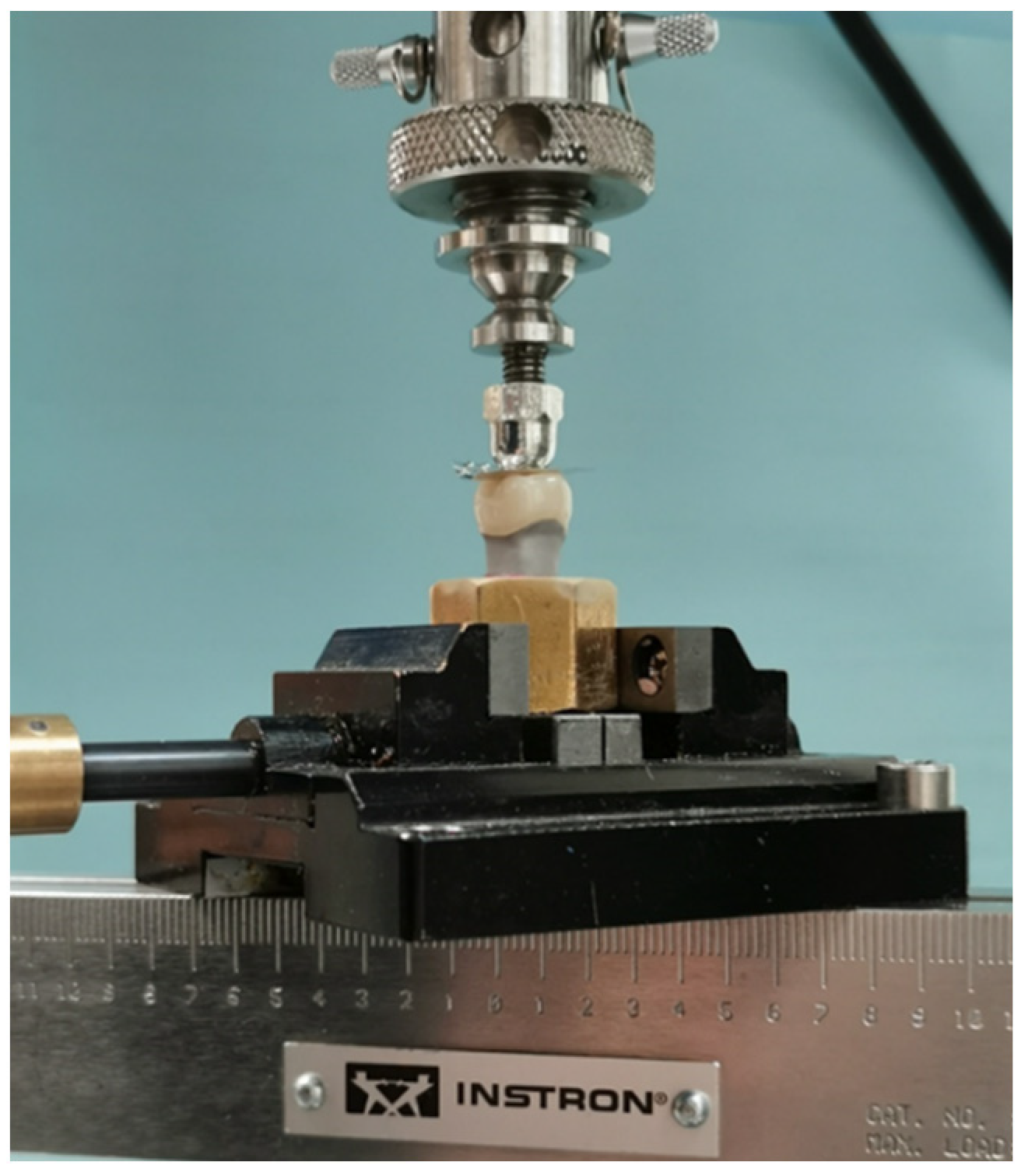
2.6. Load to Fracture
- Type I: minimal fracture or crack in the crown.
- Type II: Loss of less than half of the crown.
- Type III: Crown fracture through midline with half the crown lost.
- Type IV: Severe fracture of the crown.
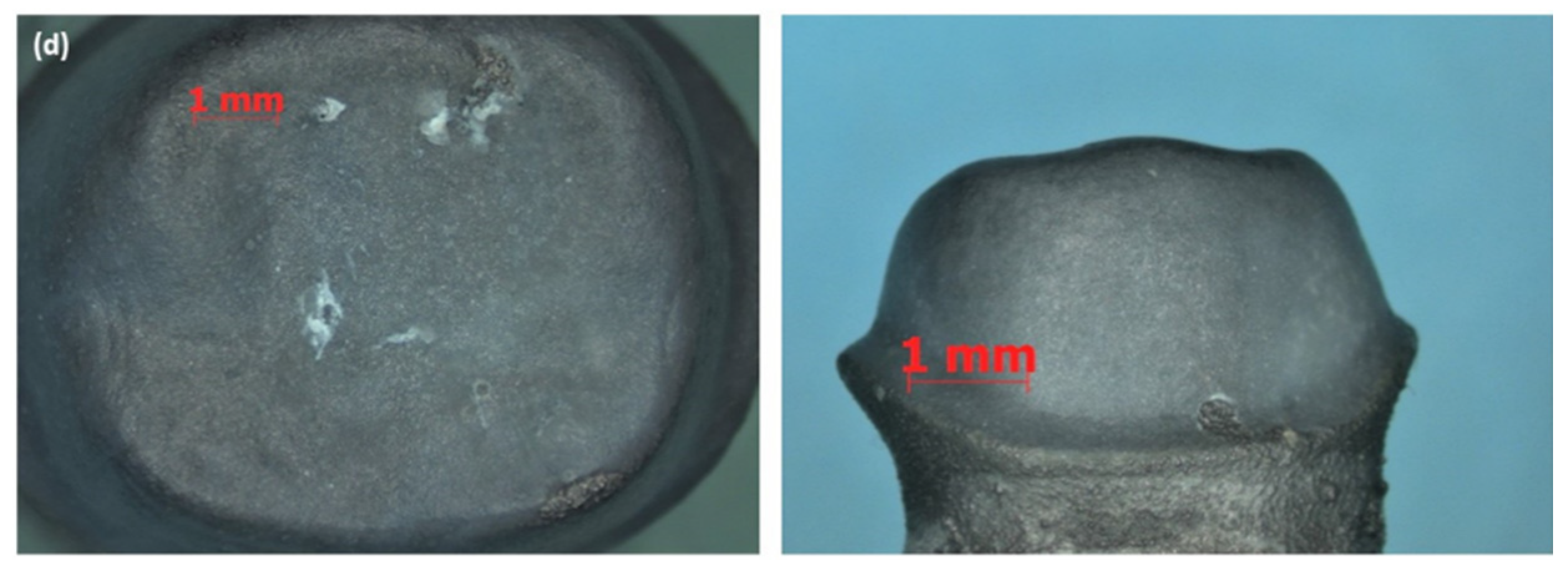
2.7. Stereomicroscopic Analysis of the Fractured Samples
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
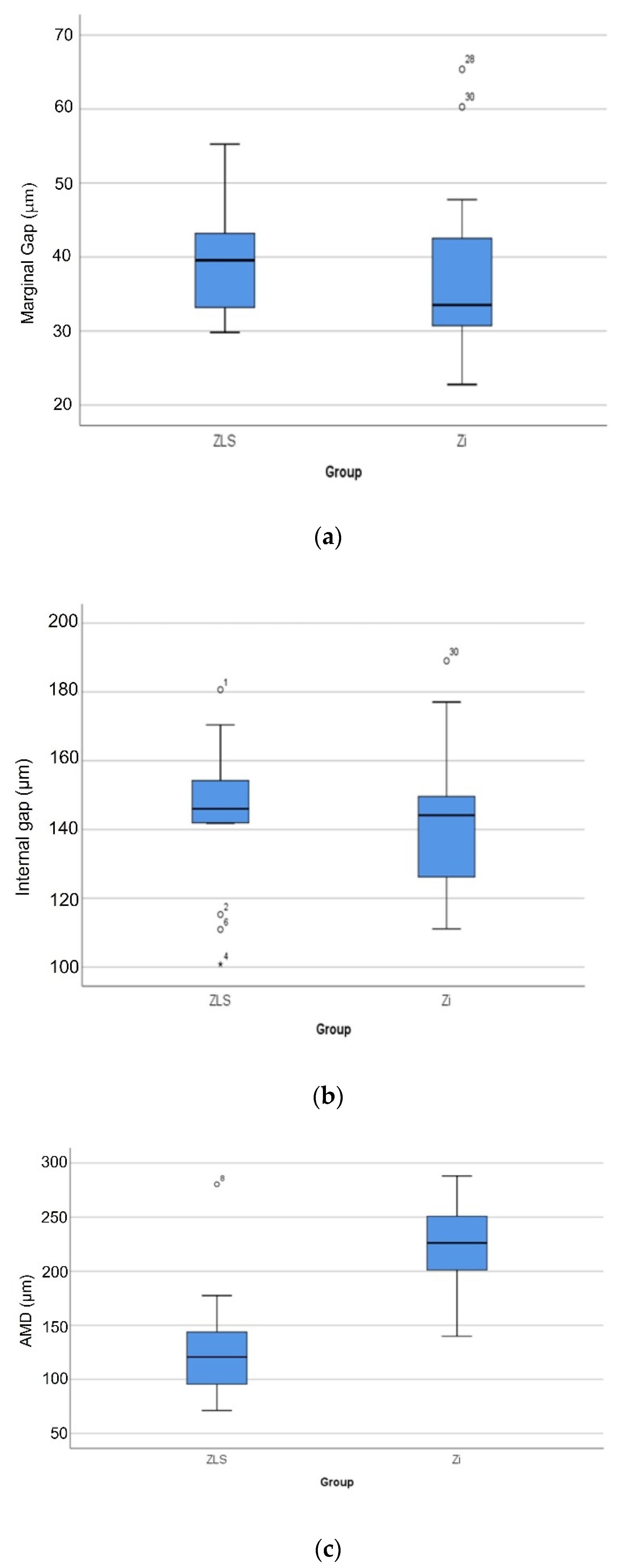
- There were no significant differences between the Zi and ZLS crowns in terms of marginal and internal gaps (p > 0.05); however, significant differences were found in the absolute marginal discrepancies between the two materials (p < 0.05).
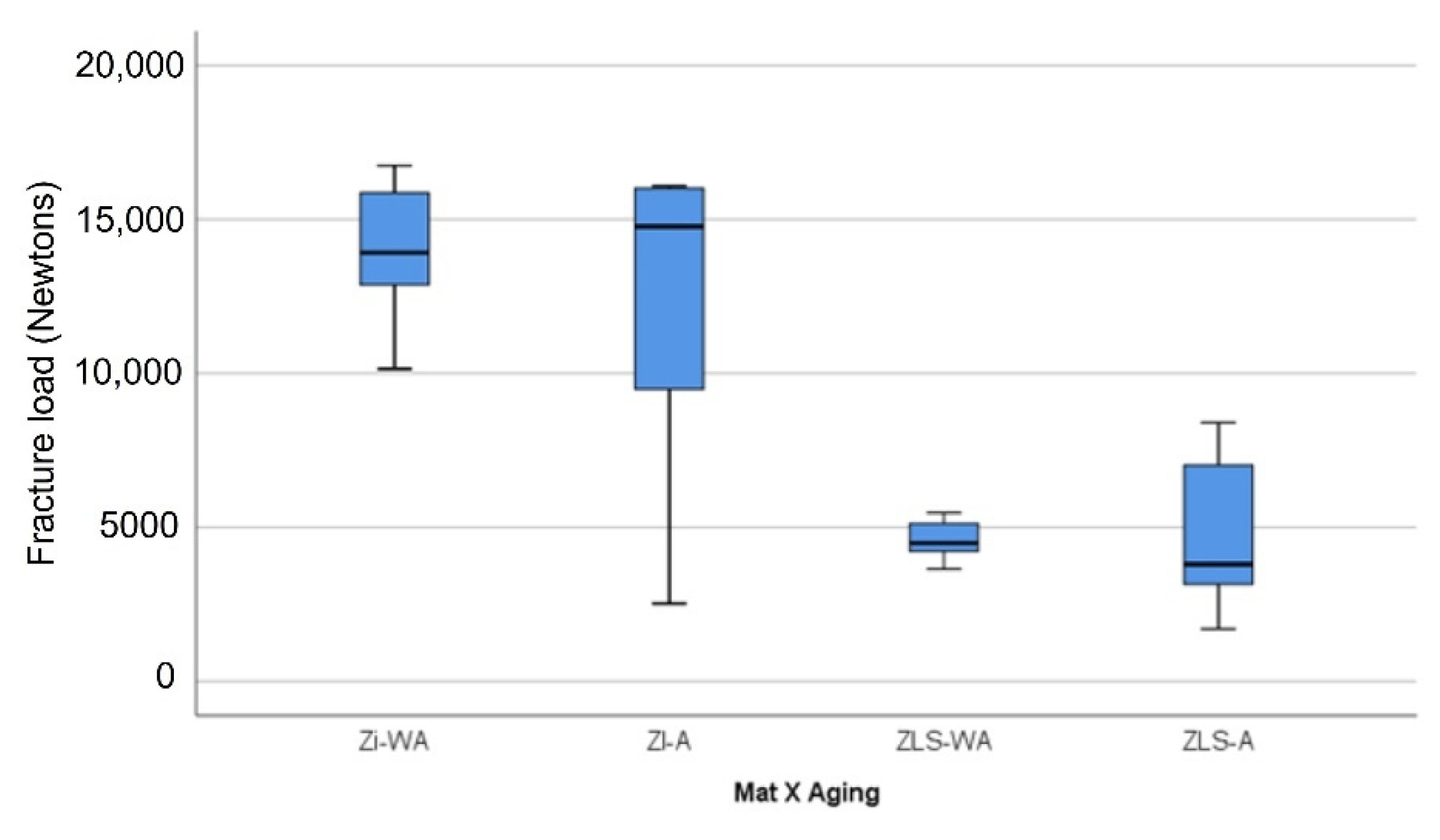
- There were significant differences in fracture loads between the Zi and ZLS crowns, regardless of mechanical aging (p < 0.05).
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sailer, I.; Makarov, N.A.; Thoma, D.S.; Zwahlen, M.P.B. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses (FDPs)? A systematic review of the survival and complication rates. Part I: Single crowns (SCs). Dent. Mater. 2015, 31, 603–623. [Google Scholar] [CrossRef] [Green Version]
- Takeichi, T.; Katsoulis, J.; Blatz, M.B. Clinical outcome of single porcelain-fused-to-zirconium dioxide crowns: A systematic review. J. Prosthet. Dent. 2013, 110, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komine, F.; Blatz, M.B.; Matsumura, H. Current status of zirconia-based fixed restorations. J. Oral Sci. 2010, 52, 531–539. [Google Scholar] [CrossRef] [Green Version]
- Kontonasaki, E.; Rigos, A.E.; Ilia, C.; Istantsos, T. Monolithic zirconia: An update to current knowledge. Optical properties, wear, and clinical performance. Dent. J. 2019, 7, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zarone, F.; Di Mauro, M.I.; Ausiello, P.; Ruggiero, G.; Sorrentino, R. Current status on lithium disilicate and zirconia: A narrative review. BMC Oral Health 2019, 19, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Saha, M.K.; Bansal, S.; Pathak, V.; Bhardwaj, S.; Chauhan, A.; Nirwan, A.S. A comparative evaluation of fracture load of monolithic and bilayered zirconia crowns with and without a cervical collar: An in vitro study. Med. Pharm. Rep. 2019, 92, 172–177. [Google Scholar] [CrossRef]
- Juntavee, N.; Dangsuwan, C. Role of coefficient of thermal expansion on bond strength of ceramic veneered yttrium-stabilized zirconia. J. Clin. Exp. Dent. 2018, 10, 279–286. [Google Scholar] [CrossRef]
- Sailer, I.; Fehér, A.; Filser, F.; Gauckler, L.J.; Lüthy, H.; Hämmerle, C.H.F. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/17695869 (accessed on 20 July 2021).
- Nasr, E.; Makhlouf, A.C.; Zebouni, E.; Makzoumé, J. All-ceramic computer-aided design and computer-aided manufacturing restorations: Evolution of structures and criteria for clinical application. J. Contemp. Dent. Pract. 2019, 20, 516–523. [Google Scholar] [CrossRef]
- Church, T.D.; Jessup, J.P.; Guillory, V.L.; Vandewalle, K.S. Translucency and strength of high-translucency monolithic zirconium oxide materials. Gen. Dent. 2017, 65, 48–52. [Google Scholar] [PubMed]
- Lucas, T.J.; Lawson, N.C.; Janowski, G.M.; Burgess, J.O. Effect of grain size on the monoclinic transformation, hardness, roughness, and modulus of aged partially stabilized zirconia. Dent. Mater. 2015, 31, 1487–1492. [Google Scholar] [CrossRef]
- Aziz, A.; El-Mowafy, O.; Paredes, S. Clinical outcomes of lithium disilicate glass-ceramic crowns fabricated with cad/cam technology: A systematic review. Dent. Med. Probl. 2020, 57, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Aldegheishem, A.; Ioannidis, G.; Att, W.; Petridis, H. Success and Survival of Various Types of All-Ceramic Single Crowns: A Critical Review and Analysis of Studies with a Mean Follow-Up of 5 Years or Longer. Int. J. Prosthodont. 2017, 30, 168–181. [Google Scholar] [CrossRef] [Green Version]
- Banh, W.; Hughes, J.; Sia, A.; Chien, D.C.H.; Tadakamadla, S.K.; Figueredo, C.M.; Ahmed, K.E. Longevity of Polymer-Infiltrated Ceramic Network and Zirconia-Reinforced Lithium Silicate Restorations: A Systematic Review and Meta-Analysis. Materials 2021, 14, 5058. [Google Scholar] [CrossRef]
- Zarone, F.; Ruggiero, G.; Leone, R.; Breschi, L.; Leuci, S.; Sorrentino, R. Zirconia-reinforced lithium silicate (ZLS) mechanical and biological properties: A literature review. J. Dent. 2021, 109, 103661. [Google Scholar] [CrossRef]
- Odén, A.; Andersson, M.; Krystek-Ondracek, I.; Magnusson, D. Five-year clinical evaluation of Procera AllCeram crowns. J. Prosthet. Dent. 1998, 80, 450–456. [Google Scholar] [CrossRef]
- Sailer, I.; Pjetursson, B.; Zwahlen, M.; Hämmerle, C.H.F. A systematic review of the survival and complication rates of all-ceramic and metal-ceramic reconstructions after an observation period of at least 3 years. Part II: Fixed dental prostheses. Clin. Oral Implants Res. 2007, 18, 86–96. [Google Scholar] [CrossRef] [PubMed]
- McLean, J.W.; Von, F. The estimation of cement film thickness by an in vivo technique. Br. Dent. J. 1971, 131, 107–111. [Google Scholar] [CrossRef]
- Contrepois, M.; Soenen, A.; Bartala, M.; Laviole, O. Marginal adaptation of ceramic crowns: A systematic review. J. Prosthet. Dent. 2013, 110, 447–454.e10. [Google Scholar] [CrossRef]
- Boitelle, P.; Mawussi, B.; Tapie, L.; Fromentin, O. A systematic review of CAD/CAM fit restoration evaluations. J. Oral Rehabil. 2014, 41, 853–874. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, M.S.; Windeler, A.S. An investigation of dental luting cement solubility as a function of the marginal gap. J. Prosthet. Dent. 1991, 65, 436–442. [Google Scholar] [CrossRef]
- Goldman, M.; Laosonthorn, P.; White, R.R. Microleakage-Full crowns and the dental pulp. J. Endod. 1992, 18, 473–475. [Google Scholar] [CrossRef]
- Sailer, I.; Fehér, A.; Filser, F.; Lüthy, H.; Gauckler, L.J.; Schärer, P.; Hämmerle, C.H.F. Prospective clinical study of zirconia posterior fixed partial dentures: 3-year follow-up. Quintessence Int. 2006, 37, 685–693. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/17017630 (accessed on 20 July 2021). [PubMed]
- Baig, M.R.; Tan, K.B.C.; Nicholls, J.I. Evaluation of the marginal fit of a zirconia ceramic computer-aided machined (CAM) crown system. J. Prosthet. Dent. 2010, 104, 216–227. [Google Scholar] [CrossRef]
- Neves, F.D.; Prado, C.J.; Prudente, M.S.; Carneiro, T.A.; Zancope, K.; Davi, L.R.; Mendonca, G.; Cooper, L.; Soares, C. Micro-computed tomography evaluation of marginal fit of lithium disilicate crowns fabricated by using chairside CAD/CAM systems or the heat-pressing technique. J. Prosthet. Dent. 2014, 112, 1134–1140. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.R.; Gonzalez, M.A.G.; Abu Kasim, N.H.; Abu Kassim, N.L.; Farook, M.S. Effect of operators’ experience and cement space on the marginal fit of an in-office digitally produced monolithic ceramic crown system. Quintessence Int. 2016, 47, 181–191. [Google Scholar] [CrossRef] [PubMed]
- Gomes, R.S.; de Souza, C.M.C.; Bergamo, E.T.P.; Bordin, D.; Del Bel Cury, A.A. Misfit and fracture load of implant-supported monolithic crowns in zirconia-reinforced lithium silicate. J. Appl. Oral Sci. 2017, 25, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Preis, V.; Behr, M.; Hahnel, S.; Rosentritt, M. Influence of cementation on in vitro performance, marginal adaptation and fracture resistance of CAD/CAM-fabricated ZLS molar crowns. Dent. Mater. 2015, 31, 1363–1369. [Google Scholar] [CrossRef] [PubMed]
- Vasiliu, R.D.; Porojan, S.D.; Porojan, L. In Vitro study of comparative evaluation of marginal and internal fit between heat-pressed and CAD-CAM monolithic glass-ceramic restorations after thermal aging. Materials 2020, 13, 4239. [Google Scholar] [CrossRef]
- Yildirim, G.; Uzun, I.H.; Keles, A. Evaluation of marginal and internal adaptation of hybrid and nanoceramic systems with microcomputed tomography: An in vitro study. J. Prosthet. Dent. 2017, 118, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Kassem, A.S.; Atta, O.; El-Mowafy, O. Fatigue Resistance and Microleakage of CAD/CAM Ceramic and Composite Molar Crowns. J. Prosthodont. 2012, 21, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Mouhat, M.; Nergård, J.M.; Lægreid, S.J.; Kanno, T.; Milleding, P.; Örtengren, U. Effect of cements on fracture resistance of monolithic zirconia crowns. Acta Biomater. Odontol. Scand. 2016, 2, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Baig, M.R.; Al-Tarakemah, Y.; Kasim, N.; Omar, R. Evaluation of the marginal fit of a CAD/CAM zirconia-based ceramic crown system. Int. J. Prosthodont. 2021. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, E.M.; Longhini, D.; Antonio, S.G.; Adabo, G.L. The effects of mechanical and hydrothermal aging on microstructure and biaxial flexural strength of an anterior and a posterior monolithic zirconia. J. Dent. 2017, 63, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Azarbal, A.; Azarbal, M.; Engelmeier, R.L.; Kunkel, T.C. Marginal Fit Comparison of CAD/CAM Crowns Milled from Two Different Materials. J. Prosthodont. 2018, 27, 421–428. [Google Scholar] [CrossRef] [Green Version]
- Alammari, M.R.; Abdelnabi, M.H.; Swelem, A.A. Effect of total occlusal convergence on fit and fracture resistance of zirconia-reinforced lithium silicate crowns. Clin. Cosmet. Investig. Dent. 2019, 11, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamza, T.A.; Sherif, R.M. In vitro evaluation of marginal discrepancy of monolithic zirconia restorations fabricated with different CAD-CAM systems. J. Prosthet. Dent. 2017, 117, 762–766. [Google Scholar] [CrossRef] [PubMed]
- Borba, M.; Miranda, W.G.; Cesar, P.F.; Griggs, J.A.; Della, B.Á. Evaluation of the adaptation of zirconia-based fixed partial dentures using micro-CT technology. Braz. Oral Res. 2013, 27, 396–402. [Google Scholar] [CrossRef] [Green Version]
- Amir Rad, F.A.; Succaria, F.G.; Morgano, S.M. Fracture resistance of porcelain veneered zirconia crowns with exposed lingual zirconia for anterior teeth after thermal cycling: An in vitro study. Saudi Dent. J. 2015, 27, 63–69. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.-W.; Kim, S.-Y.; Bae, J.-H.; Bae, E.-B.; Huh, J.-B. In vitro study of the fracture resistance of monolithic lithium disilicate, monolithic zirconia, and lithium disilicate pressed on zirconia for three-unit fixed dental prostheses. J. Adv. Prosthodont. 2017, 9, 244–251. [Google Scholar] [CrossRef]
- Sotto-Maior, B.S.; Carneiro, R.C.; Francischone, C.E.; Assis, N.M.S.P.; Devito, K.L.; Senna, P.M. Fatigue Behavior of Different CAD/CAM Materials for Monolithic, Implant-Supported Molar Crowns. J. Prosthodont. 2019, 28, e548–e551. [Google Scholar] [CrossRef]
- Sarikaya, I.; Hayran, Y. Effects of dynamic aging on the wear and fracture strength of monolithic zirconia restorations. BMC Oral Health 2018, 18, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tsuyuki, Y.; Sato, T.; Nomoto, S.; Yotsuya, M.; Koshihara, T.; Takemoto, S.; Yoshinari, M. Effect of occlusal groove on abutment, crown thickness, and cement-type on fracture load of monolithic zirconia crowns. Dent. Mater. J. 2018, 37, 843–850. [Google Scholar] [CrossRef] [Green Version]
- Juntavee, N.; Kornrum, S. Effect of Marginal Designs on Fracture Strength of High Translucency Monolithic Zirconia Crowns. Int. J. Dent. 2020, 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Garoushi, S.; Säilynoja, E.; Vallittu, P.; Lassila, L. Fracture-behavior of CAD/CAM ceramic crowns before and after cyclic fatigue aging. Int. J. Prosthodont. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mayinger, F.; Pfefferle, R.; Reichert, A.; Stawarczyk, B. Impact of High-Speed Sintering of Three-Unit 3Y-TZP and 4Y-TZP Fixed Dental Prostheses on Fracture Load With and Without Artificial Aging. Int. J. Prosthodont. 2021, 47–53. [Google Scholar] [CrossRef]
- Zahran, M.; El-Mowafy, O.; Tam, L.; Watson, P.A.; Finer, Y. Fracture strength and fatigue resistance of all-ceramic molar crowns manufactured with CAD/CAM technology. J. Prosthodont. 2008, 17, 370–377. [Google Scholar] [CrossRef]
- D’Addazio, G.; Santilli, M.; Rollo, M.L.; Cardelli, P.; Rexhepi, I.; Murmura, G.; Husain, N.A.-H.; Sinjari, B.; Traini, T.; Özcan, M.; et al. Fracture resistance of Zirconia-reinforced lithium silicate ceramic crowns cemented with conventional or adhesive systems: An in vitro study. Materials 2020, 13, 2012. [Google Scholar] [CrossRef]
- Nishioka, G.; Prochnow, C.; Firmino, A.; Amaral, M.; Bottino, M.A.; Valandro, L.F.; Renata Marques de, M. Fatigue strength of several dental ceramics indicated for CAD-CAM monolithic restorations. Braz. Oral Res. 2018, 32, e53. [Google Scholar] [CrossRef]
- Silvestri, T.; Pereira, G.K.R.; Guilardi, L.F.; Rippe, M.P.; Valandro, L.F. Effect of grinding and multi-stimuli aging on the fatigue strength of a Y-TZP ceramic. Braz. Dent. J. 2018, 29, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.O.; Bruzi, G.; Giannini, M.; Magne, P. Fatigue resistance of CAD/CAM complete crowns with a simplified cementation process. J. Prosthet. Dent. 2014, 111, 310–317. [Google Scholar] [CrossRef]
- Guilardi, L.F.; Pereira, G.K.R.; Wandscher, V.F.; Rippe, M.P.; Valandro, L.F. Mechanical behavior of yttria-stabilized tetragonal zirconia polycrystal: Effects of different aging regimens. Braz. Oral Res. 2017, 31, e94. [Google Scholar] [CrossRef] [Green Version]
- Beuer, F.; Stimmelmayr, M.; Gueth, J.F.; Edelhoff, D.; Naumann, M. In vitro performance of full-contour zirconia single crowns. Dent. Mater. 2012, 28, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Tekin, Y.H.; Hayran, Y. Fracture resistance and marginal fit of the zirconia crowns with varied occlusal thickness. J. Adv. Prosthodont. 2020, 12, 283–290. [Google Scholar] [CrossRef]
- Mitov, G.; Anastassova-Yoshida, Y.; Nothdurft, F.P.; Von See, C.; Pospiech, P. Influence of the preparation design and artificial aging on the fracture resistance of monolithic zirconia crowns. J. Adv. Prosthodont. 2016, 8, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Øilo, M.; Kvam, K.; Gjerdet, N.R. Load at fracture of monolithic and bilayered zirconia crowns with and without a cervical zirconia collar. J. Prosthet. Dent. 2016, 115, 630–636. [Google Scholar] [CrossRef] [PubMed]
- Furtado de Mendonca, A.; Shahmoradi, M.; de Gouvêa, C.V.D.; De Souza, G.M.; Ellakwa, A. Microstructural and Mechanical Characterization of CAD/CAM Materials for Monolithic Dental Restorations. J. Prosthodont. 2019, 28, e587–e594. [Google Scholar] [CrossRef]
- Ellakwa, A.; Martin, F.E.; Klineberg, I. Influence of Implant Abutment Angulations and Two Types of Fibers on the Fracture Resistance of Ceramage Single Crowns. J. Prosthodont. 2012, 21, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Meirowitz, A.; Bitterman, Y.; Levy, S.; Mijiritsky, E.; Dolev, E. An in vitro evaluation of marginal fit zirconia crowns fabricated by a CAD-CAM dental laboratory and a milling center. BMC Oral Health 2019, 19, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, W.M.; Abdallah, M.N.; McCullagh, A.P.; Wyatt, C.C.L.; Troczynski, T.; Carvalho, R.M. Marginal Discrepancies of Monolithic Zirconia Crowns: The Influence of Preparation Designs and Sintering Techniques. J. Prosthodont. 2019, 28, 288–298. [Google Scholar] [CrossRef]
- Kale, E.; Yilmaz, B.; Seker, E.; Özcelik, T.B. Effect of fabrication stages and cementation on the marginal fit of CAD-CAM monolithic zirconia crowns. J. Prosthet. Dent. 2017, 118, 736–741. [Google Scholar] [CrossRef]
- Kale, E.; Seker, E.; Yilmaz, B.; Özcelik, T.B. Effect of cement space on the marginal fit of CAD-CAM-fabricated monolithic zirconia crowns. J. Prosthet. Dent. 2016, 116, 890–895. [Google Scholar] [CrossRef]
- Nakamura, T.; Nakano, Y.; Usami, H.; Okamura, S.; Wakabayashi, K.; Yatani, H. In vitro investigation of fracture load and aging resistance of high-speed sintered monolithic tooth-borne zirconia crowns. J. Prosthodont. Res. 2020, 64, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Cunali, R.S.; Saab, R.C.; Correr, G.M.; Da Cunha, L.F.; Ornaghi, B.P.; Ritter, A.V.; Gonzaga, C.C. Marginal and internal adaptation of zirconia crowns: A comparative study of assessment methods. Braz. Dent. J. 2017, 28, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Paul, N.; Raghavendra Swamy, K.; Dhakshaini, M.; Sowmya, S.; Meravini, M. Marginal and internal fit evaluation of conventional metal-ceramic versus zirconia CAD/CAM crowns. J. Clin. Exp. Dent. 2020, 12, e31–e37. [Google Scholar] [CrossRef] [PubMed]
- Ben-Izhack, G.; Shely, A.; Koton, O.; Meirowitz, A.; Levartovsky, S.; Dolev, E. (In-vitro comparison between closed versus open CAD/CAM systems) comparison between closed and open CAD/CAM systems by evaluating the marginal fit of zirconia-reinforced lithium silicate ceramic crowns. Appl. Sci. 2021, 11, 4534. [Google Scholar] [CrossRef]
- Hasanzade, M.; Sahebi, M.; Zarrati, S.; Payaminia, L.; Alikhasi, M. Comparative Evaluation of the Internal and Marginal Adaptations of CAD/CAM Endocrowns and Crowns Fabricated from Three Different Materials. Int. J. Prosthodont. 2021, 34, 341–347. [Google Scholar] [CrossRef] [PubMed]
- Pedroche, L.O.; Bernardes, S.R.; Leão, M.P.; Kintopp, C.C.d.A.; Correr, G.M.; Ornaghi, B.P.; Gonzaga, C.C. Marginal and internal fit of zirconia copings obtained using different digital scanning methods. Braz. Oral Res. 2016, 30, e113. [Google Scholar] [CrossRef]
- Ortega, R.; Gonzalo, E.; Gomez-Polo, M.; Lopez-Suarez, C.; Suarez, M.J. SEM evaluation of the precision of fit of CAD/CAM zirconia and metal-ceramic posterior crowns. Dent. Mater. J. 2017, 36, 387–393. [Google Scholar] [CrossRef] [PubMed]
- Gold, S.A.; Ferracane, J.L.; da Costa, J. Effect of Crystallization Firing on Marginal Gap of CAD/CAM Fabricated Lithium Disilicate Crowns. J. Prosthodont. 2018, 27, 63–66. [Google Scholar] [CrossRef] [Green Version]
- Morneburg, T.R.; Pröschel, P.A. Measurement of masticatory forces and implant loads: A methodologic clinical study. Int. J. Prosthodont. 2002, 15, 20–27. Available online: https://pubmed.ncbi.nlm.nih.gov/11887595/ (accessed on 20 July 2021).
- Ferrario, V.F.; Sforza, C.; Zanotti, G.; Tartaglia, G.M. Maximal bite forces in healthy young adults as predicted by surface electromyography. J. Dent. 2004, 32, 451–457. [Google Scholar] [CrossRef]
- Dos Santos Calderon, P.; Kogawa, E.M.; Lauris, J.R.P.; Conti, P.C.R. The influence of gender and bruxism on the human maximum bite force. J. Appl. Oral Sci. 2006, 14, 448–453. [Google Scholar] [CrossRef]
- Weyhrauch, M.; Igiel, C.; Scheller, H.; Weibrich, G.; Lehmann, K. Fracture Strength of Monolithic All-Ceramic Crowns on Titanium Implant Abutments. Int. J. Oral Maxillofac. Implants. 2016, 31, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Arslan, M.; Tosun, İ. Fracture load and microcrack comparison of crowns manufactured from tooth-shaped and traditional blocks. Microsc. Res. Tech. 2021, 84, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, J.B.; Oliani, M.G.; Guilardi, L.F.; Prochnow, C.; Pereira, G.K.R.; Bottino, M.A.; de Melo, R.M.; Valandro, L.F. Fatigue failure load of zirconia-reinforced lithium silicate glass ceramic cemented to a dentin analogue: Effect of etching time and hydrofluoric acid concentration. J. Mech. Behav. Biomed. Mater. 2018, 77, 375–382. [Google Scholar] [CrossRef] [Green Version]
- Sieper, K.; Wille, S.; Kern, M. Fracture strength of lithium disilicate crowns compared to polymer-infiltrated ceramic-network and zirconia reinforced lithium silicate crowns. J. Mech. Behav. Biomed. Mater. 2017, 74, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Harada, A.; Inagaki, R.; Kanno, T.; Niwano, Y.; Milleding, P.; Ørtengren, U.T. Fracture resistance of monolithic zirconia molar crowns with reduced thickness. Acta Odontol. Scand. 2015, 73, 602–608. [Google Scholar] [CrossRef] [PubMed]
- Scherrer, S.S.; Rijik, W.G. The fracture resistance of all-ceramic crowns on supporting structures with different elastic moduli. Int. J. Prosthodont. 1993, 6, 462–467. Available online: https://pubmed.ncbi.nlm.nih.gov/8297457/ (accessed on 20 July 2021).
- Yucel, M.T.; Yondem, I.; Aykent, F.; Eraslan, O. Influence of the supporting die structures on the fracture strength of all-ceramic materials. Clin. Oral Investig. 2012, 16, 1105–1110. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Wilson, P.R. Fracture strength of all-ceramic crowns with varying core elastic moduli. Aust. Dent. J. 2000, 25, 103–107. Available online: https://pubmed.ncbi.nlm.nih.gov/10925505/ (accessed on 20 July 2021).
- Nakamura, K.; Ankyu, S.; Nilsson, F.; Kanno, T.; Niwano, Y.; von Steyern, P.V.; Örtengren, U. Critical considerations on load-to-failure test for monolithic zirconia molar crowns. J. Mech. Behav. Biomed. Mater. 2018, 87, 180–189. [Google Scholar] [CrossRef]
- Attia, A.; Kern, M. Influence of cyclic loading and luting agents on the fracture load of two all-ceramic crown systems. J. Prosthet Dent. 2004, 92, 551–556. [Google Scholar] [CrossRef]
- Goujat, A.; Abouelleil, H.; Colon, P.; Jeannin, C.; Pradelle, N.; Seux, D.; Grosgogeat, B. Marginal and internal fit of CAD-CAM inlay/onlay restorations: A systematic review of in vitro studies. J. Prosthet. Dent. 2019, 121, 590–597.e3. [Google Scholar] [CrossRef] [PubMed]
- Pagano, S.; Lombardo, G.; Caponi, S.; Costanzi, E.; Di Michele, A.; Bruscoli, S.; Xhimitiku, I.; Coniglio, M.; Valenti, C.; Mattarelli, M.; et al. Bio-mechanical characterization of a CAD / CAM PMMA resin for digital removable prostheses. Dent. Mater. 2021, 37, e118–e130. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Value |
|---|---|
| VOXEL | 11.111 Nm |
| VOLTAGE | 120 kV |
| CURRENT | 150 µA |
| POWER | 18 W |
| FILTER (Cu + Al) | 1 mm |
| GRABAR TIME | 750 ms |
| TIME | 1.45 h |
| ROTATION | 360° |
| NO. OF IMAGES | 2000 |
| Material | Marginal Gap (µm) | Internal Gap (µm) | AMD (µm) |
|---|---|---|---|
| Zi | 37.71 ± 11.73 | 141.61 ± 20.92 | 224.92 ± 7.33 |
| ZLS | 39.49 ± 7.42 | 144.85 ± 21.07 | 128.13 ± 49.09 |
| Parameter | F | Sig. | T | Df | Sig. (2-Tailed) | Mean Difference | Std. Error Mean | 95% Confidence Interval of the Difference | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Upper | Lower | |||||||||
| MG | Equal variances assumed | 1.679 | 0.205 | 0.511 | 30 | 0.613 | 1.773 | 3.47 | −5.314 | 8.859 |
| Equal variances not assumed | - | - | 0.511 | 25.342 | 0.614 | 1.773 | 3.47 | −5.369 | 8.915 | |
| IG | Equal variances assumed | 0.084 | 0.774 | 0.436 | 30 | 0.666 | 3.234 | 7.424 | −11.928 | 18.396 |
| Equal variances not assumed | - | - | 0.436 | 30 | 0.666 | 3.234 | 7.424 | −11.928 | 18.396 | |
| AMD | Equal variances assumed | 0.168 | 0.684 | −6.278 | 30 | 0.000 | −96.794 | 15.417 | −128.279 | −65.309 |
| Equal variances not assumed | - | - | −6.278 | 28 | 0.000 | −96.794 | 15.417 | −128.375 | −65.214 | |
| Material | Mean (SD) | Minimum | Maximum | Median | IQR |
|---|---|---|---|---|---|
| Zi-WMA | 14,023 (2167) | 10,141 | 16,741 | 13,916.50 a | 3361 |
| Zi-MA | 12,390 (5465) | 2525 | 16,084 | 14,766 a | 8887 |
| ZLS-WMA | 4600 (618) | 3651 | 5473 | 4489.50 b | 1073 |
| ZLS-MA | 4754 (2471) | 1700 | 8400 | 3800 b | 4542 |
| Material | Type I | Type II | Type III | Type IV |
|---|---|---|---|---|
| Zi | 1 | 3 | 4 | 8 |
| ZLS | 0 | 0 | 3 | 13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sadeqi, H.A.; Baig, M.R.; Al-Shammari, M. Evaluation of Marginal/Internal Fit and Fracture Load of Monolithic Zirconia and Zirconia Lithium Silicate (ZLS) CAD/CAM Crown Systems. Materials 2021, 14, 6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14216346
Sadeqi HA, Baig MR, Al-Shammari M. Evaluation of Marginal/Internal Fit and Fracture Load of Monolithic Zirconia and Zirconia Lithium Silicate (ZLS) CAD/CAM Crown Systems. Materials. 2021; 14(21):6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14216346
Chicago/Turabian StyleSadeqi, Haneen A., Mirza Rustum Baig, and Mohammad Al-Shammari. 2021. "Evaluation of Marginal/Internal Fit and Fracture Load of Monolithic Zirconia and Zirconia Lithium Silicate (ZLS) CAD/CAM Crown Systems" Materials 14, no. 21: 6346. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14216346