
Immediate Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Long-Term Results after 11 Years of Clinical Function

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Clinical Procedures
2.3. Clinical Evaluation
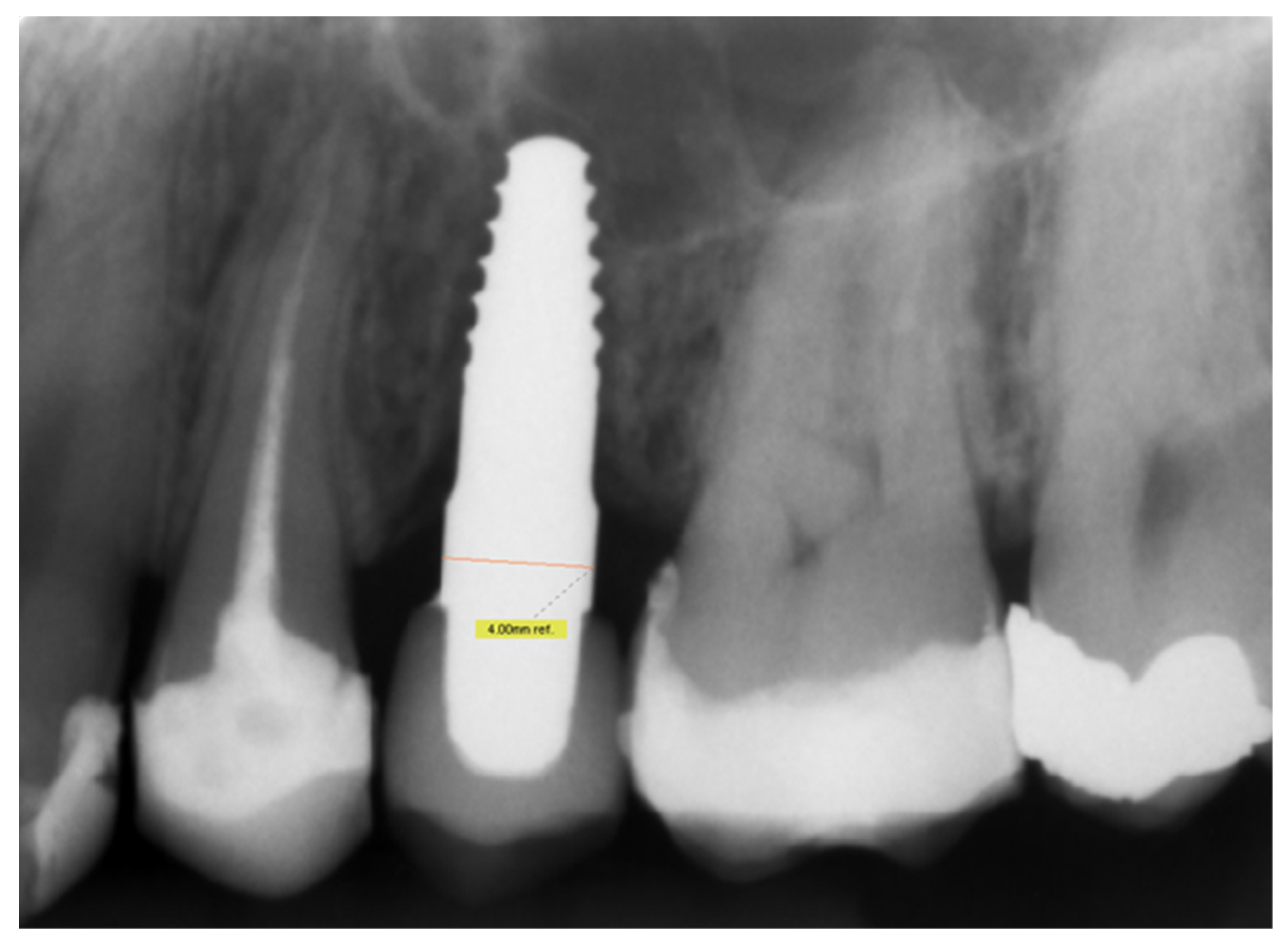
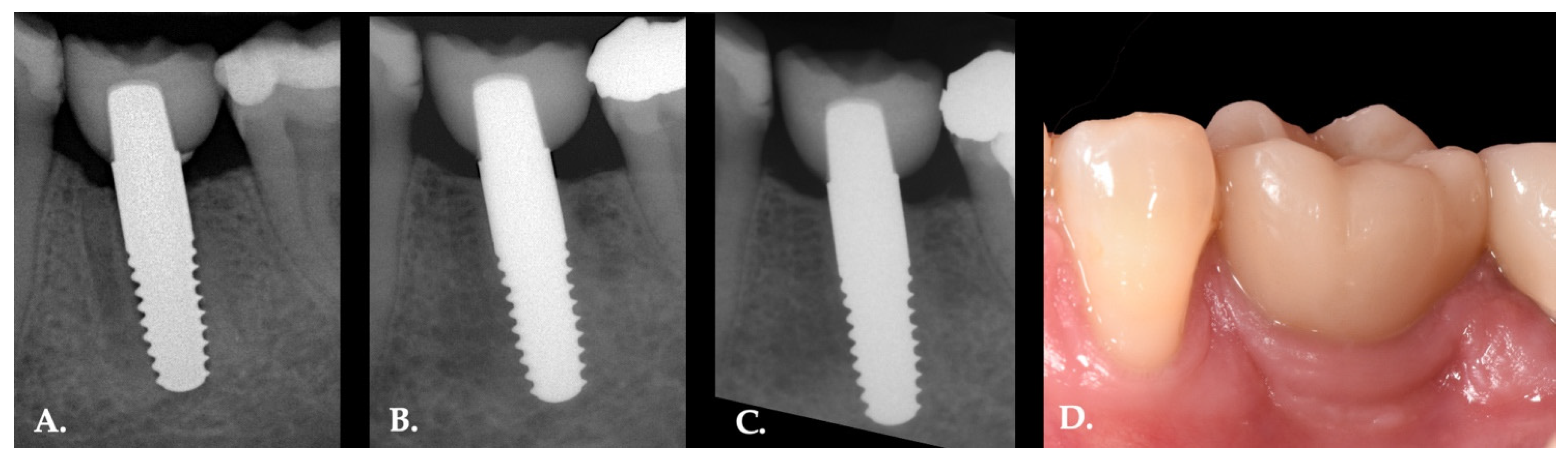
2.4. Radiographic Evaluation
2.5. Statistical Analysis
3. Results
3.1. Patient Information
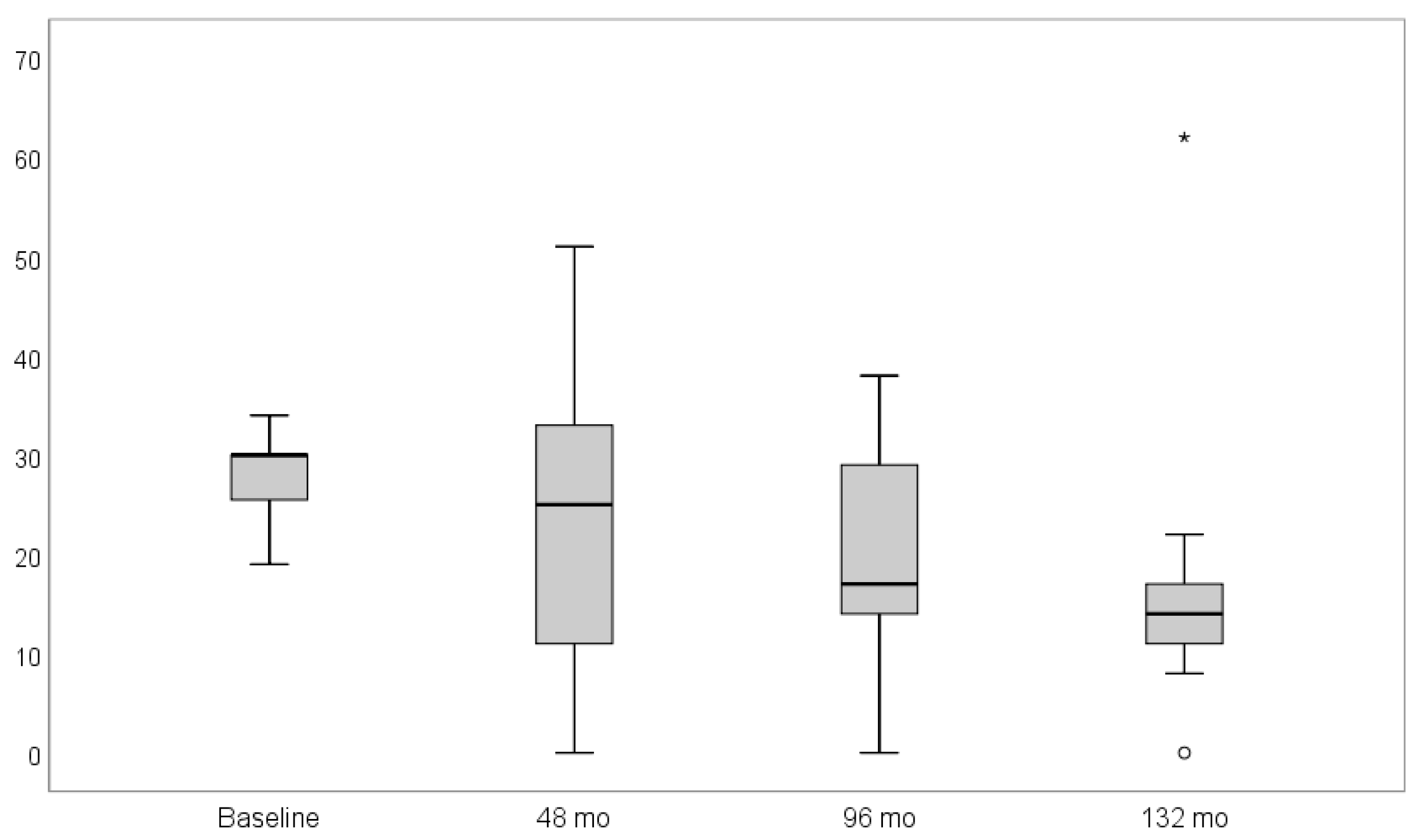
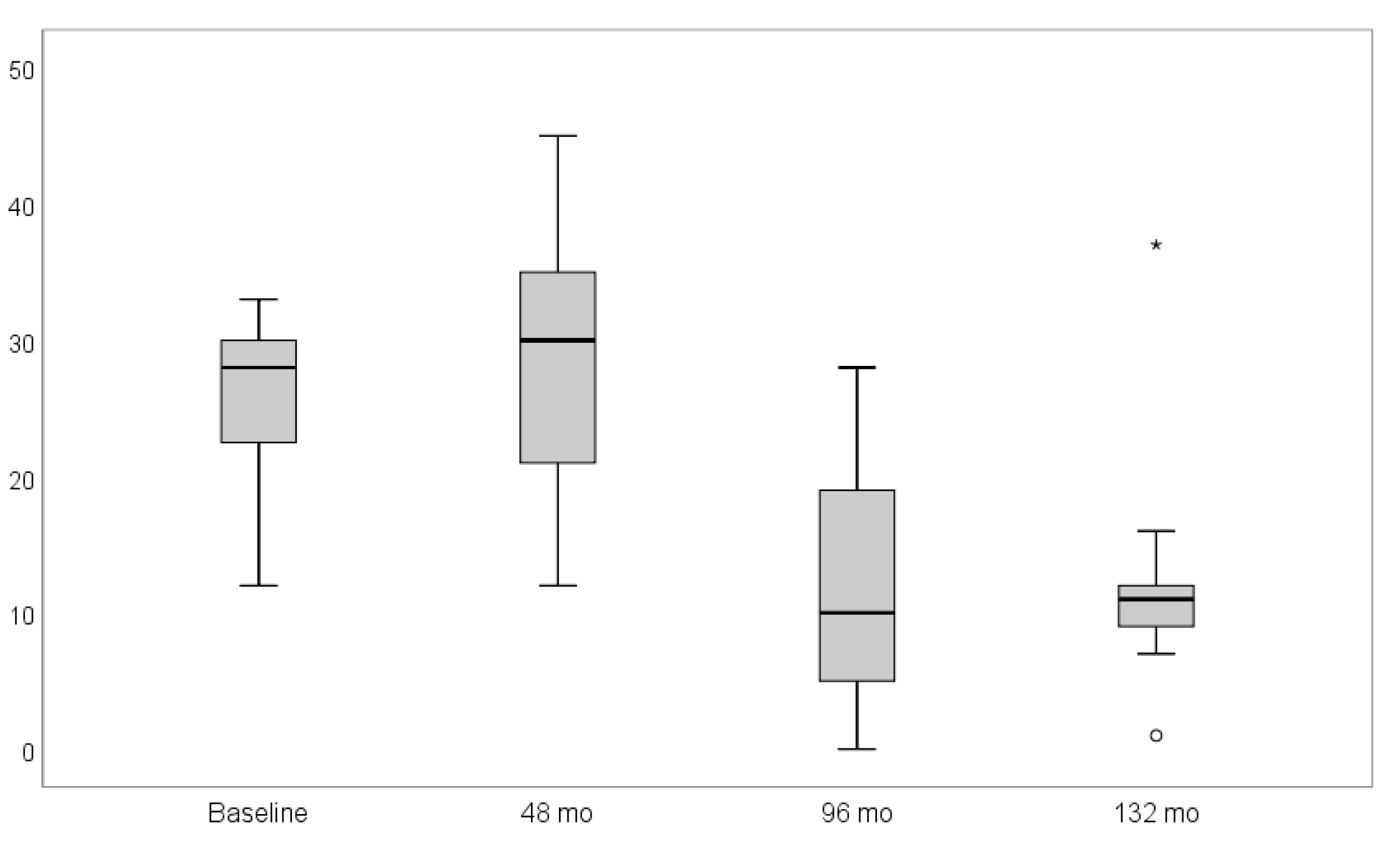
3.2. Clinical Assessments
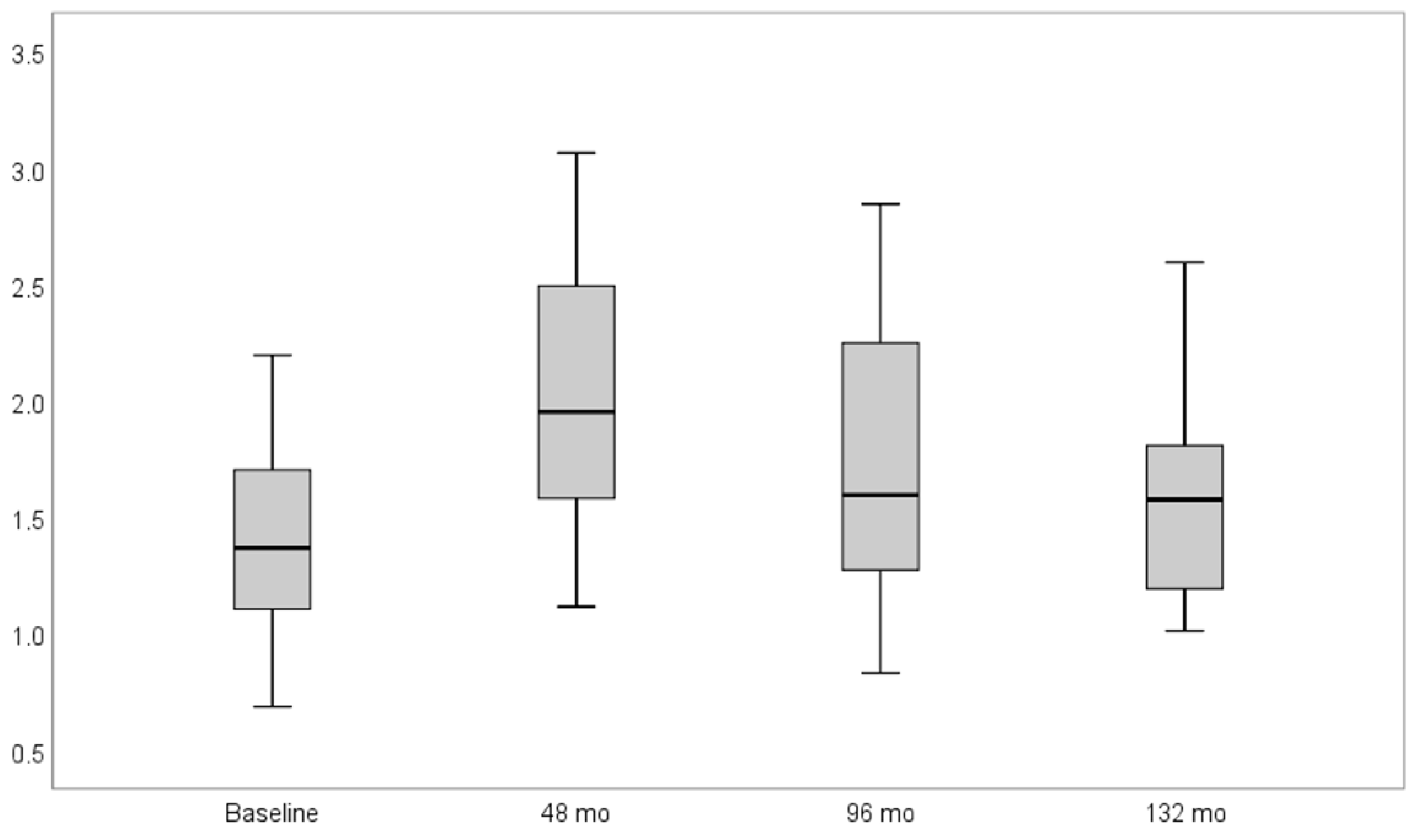
3.3. Radiographic Assessments
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bassir, S.H.; El Kholy, K.; Chen, C.-Y.; Lee, K.H.; Intini, G. Outcome of Early Dental Implant Placement versus Other Dental Implant Placement Protocols: A Systematic Review and Meta-Analysis. J. Periodontol. 2019, 90, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern Implant Dentistry Based on Osseointegration: 50 Years of Progress, Current Trends and Open Questions. Periodontology 2000 2017, 73, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; van Oosten, M.A.; Schurch, E.; Land, N.P. The Microbiota Associated with Successful or Failing Osseointegrated Titanium Implants. Oral Microbiol. Immunol. 1987, 2, 145–151. [Google Scholar] [CrossRef]
- Fretwurst, T.; Nelson, K.; Tarnow, D.P.; Wang, H.-L.; Giannobile, W.V. Is Metal Particle Release Associated with Peri-Implant Bone Destruction? An Emerging Concept. J. Dent. Res. 2018, 97, 259–265. [Google Scholar] [CrossRef]
- Safioti, L.M.; Kotsakis, G.A.; Pozhitkov, A.E.; Chung, W.O.; Daubert, D.M. Increased Levels of Dissolved Titanium Are Associated With Peri-Implantitis—A Cross-Sectional Study. J. Periodontol. 2017, 88, 436–442. [Google Scholar] [CrossRef]
- Zhou, Z.; Shi, Q.; Wang, J.; Chen, X.; Hao, Y.; Zhang, Y.; Wang, X. The Unfavorable Role of Titanium Particles Released from Dental Implants. Nanotheranostics 2021, 5, 321–332. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia Dental Implants: Where Are We Now, and Where Are We Heading? Periodontology 2000 2017, 73, 241–258. [Google Scholar] [CrossRef]
- Bosshardt, D.D.; Chappuis, V.; Buser, D. Osseointegration of Titanium, Titanium Alloy and Zirconia Dental Implants: Current Knowledge and Open Questions. Periodontology 2000 2017, 73, 22–40. [Google Scholar] [CrossRef]
- Schünemann, F.H.; Galárraga-Vinueza, M.E.; Magini, R.; Fredel, M.; Silva, F.; Souza, J.C.M.; Zhang, Y.; Henriques, B. Zirconia Surface Modifications for Implant Dentistry. Mater. Sci. Eng. C Mater. Biol. Appl. 2019, 98, 1294–1305. [Google Scholar] [CrossRef]
- Hafezeqoran, A.; Koodaryan, R. Effect of Zirconia Dental Implant Surfaces on Bone Integration: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2017, 2017, 9246721. [Google Scholar] [CrossRef]
- Kniha, K.; Heussen, N.; Modabber, A.; Hölzle, F.; Möhlhenrich, S.C. The Effect of Zirconia and Titanium Surfaces on Biofilm Formation and on Host-Derived Immunological Parameters. Int. J. Oral Maxillofac. Surg. 2021, 50, 1361–1374. [Google Scholar] [CrossRef] [PubMed]
- Al-Radha, A.S.D.; Dymock, D.; Younes, C.; O’Sullivan, D. Surface Properties of Titanium and Zirconia Dental Implant Materials and Their Effect on Bacterial Adhesion. J. Dent. 2012, 40, 146–153. [Google Scholar] [CrossRef]
- Haro Adánez, M.; Nishihara, H.; Att, W. A Systematic Review and Meta-Analysis on the Clinical Outcome of Zirconia Implant-Restoration Complex. J. Prosthodont. Res. 2018, 62, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Roehling, S.; Schlegel, K.A.; Woelfler, H.; Gahlert, M. Performance and Outcome of Zirconia Dental Implants in Clinical Studies: A Meta-Analysis. Clin. Oral Implants Res. 2018, 29 (Suppl. 16), 135–153. [Google Scholar] [CrossRef] [PubMed]
- Bienz, S.P.; Hilbe, M.; Hüsler, J.; Thoma, D.S.; Hämmerle, C.H.F.; Jung, R.E. Clinical and Histological Comparison of the Soft Tissue Morphology between Zirconia and Titanium Dental Implants under Healthy and Experimental Mucositis Conditions-A Randomized Controlled Clinical Trial. J. Clin. Periodontol. 2021, 48, 721–733. [Google Scholar] [CrossRef]
- Lughi, V.; Sergo, V. Low Temperature Degradation-Aging-of Zirconia: A Critical Review of the Relevant Aspects in Dentistry. Dent. Mater. 2010, 26, 807–820. [Google Scholar] [CrossRef]
- Hashim, D.; Cionca, N.; Courvoisier, D.S.; Mombelli, A. A Systematic Review of the Clinical Survival of Zirconia Implants. Clin. Oral Investig. 2016, 20, 1403–1417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lorusso, F.; Noumbissi, S.; Francesco, I.; Rapone, B.; Khater, A.G.A.; Scarano, A. Scientific Trends in Clinical Research on Zirconia Dental Implants: A Bibliometric Review. Materials 2020, 13, 5534. [Google Scholar] [CrossRef]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Dolci, M.; Calvo-Guirado, J.L.; Delgado Ruiz, R.A.; Maiorana, C. Evaluation of the Success Criteria for Zirconia Dental Implants: A Four-Year Clinical and Radiological Study. Int. J. Dent. 2013, 2013, 463073. [Google Scholar] [CrossRef]
- Bethke, A.; Pieralli, S.; Kohal, R.-J.; Burkhardt, F.; von Stein-Lausnitz, M.; Vach, K.; Spies, B.C. Fracture Resistance of Zirconia Oral Implants In Vitro: A Systematic Review and Meta-Analysis. Materials 2020, 13, 562. [Google Scholar] [CrossRef] [Green Version]
- Silva, N.R.F.A.; Coelho, P.G.; Fernandes, C.A.O.; Navarro, J.M.; Dias, R.A.; Thompson, V.P. Reliability of One-Piece Ceramic Implant. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 419–426. [Google Scholar] [CrossRef]
- Kohal, R.-J.; Spies, B.C.; Vach, K.; Balmer, M.; Pieralli, S. A Prospective Clinical Cohort Investigation on Zirconia Implants: 5-Year Results. J. Clin. Med. 2020, 9, 2585. [Google Scholar] [CrossRef] [PubMed]
- Balmer, M.; Spies, B.C.; Kohal, R.-J.; Hämmerle, C.H.-F.; Vach, K.; Jung, R.E. Zirconia Implants Restored with Single Crowns or Fixed Dental Prostheses: 5-Year Results of a Prospective Cohort Investigation. Clin. Oral Implants Res. 2020, 31, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Payer, M.; Arnetzl, V.; Kirmeier, R.; Koller, M.; Arnetzl, G.; Jakse, N. Immediate Provisional Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Results after 24 Months of Clinical Function. Clin. Oral Implants Res. 2013, 24, 569–575. [Google Scholar] [CrossRef]
- Beger, B.; Goetz, H.; Morlock, M.; Schiegnitz, E.; Al-Nawas, B. In Vitro Surface Characteristics and Impurity Analysis of Five Different Commercially Available Dental Zirconia Implants. Int. J. Implant Dent. 2018, 4, 13. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The Plaque Control Record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Naert, I.; Quirynen, M.; van Steenberghe, D.; Darius, P. A Six-Year Prosthodontic Study of 509 Consecutively Inserted Implants for the Treatment of Partial Edentulism. J. Prosthet. Dent. 1992, 67, 236–245. [Google Scholar] [CrossRef]
- Snauwaert, K.; Duyck, J.; van Steenberghe, D.; Quirynen, M.; Naert, I. Time Dependent Failure Rate and Marginal Bone Loss of Implant Supported Prostheses: A 15-Year Follow-up Study. Clin. Oral Investig. 2000, 4, 13–20. [Google Scholar] [CrossRef]
- Buch, R.S.R.; Weibrich, G.; Wagner, W. Criteria of success in implantology. Mund-Kiefer-Und Gesichtschirurgie MKG 2003, 7, 42–46. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. J. Am. Stat. Assoc. 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Palta, M.; McHugh, R. Adjusting for Losses to Follow-up in a Sample Size Determination for Cohort Studies. J. Chronic Dis. 1979, 32, 315–326. [Google Scholar] [CrossRef]
- Kern, J.-S.; Kern, T.; Wolfart, S.; Heussen, N. A Systematic Review and Meta-Analysis of Removable and Fixed Implant-Supported Prostheses in Edentulous Jaws: Post-Loading Implant Loss. Clin. Oral Implants Res. 2016, 27, 174–195. [Google Scholar] [CrossRef]
- Borgonovo, A.E.; Arnaboldi, O.; Censi, R.; Dolci, M.; Santoro, G. Edentulous Jaws Rehabilitation with Yttrium-Stabilized Zirconium Dioxide Implants: Two Years Follow-up Experience. Minerva Stomatol 2010, 59, 381–392. [Google Scholar]
- Zinelis, S.; Thomas, A.; Syres, K.; Silikas, N.; Eliades, G. Surface Characterization of Zirconia Dental Implants. Dent Mater. 2010, 26, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.-L.; Shiau, H.J.; Reynolds, M.A. Survival of Dental Implants at Sites after Implant Failure: A Systematic Review. J. Prosthet. Dent. 2020, 123, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Duddeck, D.U.; Albrektsson, T.; Wennerberg, A.; Larsson, C.; Beuer, F. On the Cleanliness of Different Oral Implant Systems: A Pilot Study. J. Clin. Med. 2019, 8, 1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olate, S.; Lyrio, M.C.N.; de Moraes, M.; Mazzonetto, R.; Moreira, R.W.F. Influence of Diameter and Length of Implant on Early Dental Implant Failure. J. Oral Maxillofac. Surg. 2010, 68, 414–419. [Google Scholar] [CrossRef] [PubMed]
- Schiegnitz, E.; Al-Nawas, B. Narrow-Diameter Implants: A Systematic Review and Meta-Analysis. Clin. Oral Implant. Res. 2018, 29, 21–40. [Google Scholar] [CrossRef] [Green Version]
- Quirynen, M.; Abarca, M.; Van Assche, N.; Nevins, M.; van Steenberghe, D. Impact of Supportive Periodontal Therapy and Implant Surface Roughness on Implant Outcome in Patients with a History of Periodontitis. J. Clin. Periodontol. 2007, 34, 805–815. [Google Scholar] [CrossRef]
- Koller, M.; Steyer, E.; Theisen, K.; Stagnell, S.; Jakse, N.; Payer, M. Two-Piece Zirconia versus Titanium Implants after 80 Months: Clinical Outcomes from a Prospective Randomized Pilot Trial. Clin. Oral Implants Res. 2020, 31, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The Long-Term Efficacy of Currently Used Dental Implants: A Review and Proposed Criteria of Success. Int. J. Oral Maxillofac. Implants 1986, 1, 11–25. [Google Scholar] [PubMed]
- Borgonovo, A.E.; Censi, R.; Vavassori, V.; Arnaboldi, O.; Maiorana, C.; Re, D. Zirconia Implants in Esthetic Areas: 4-Year Follow-Up Evaluation Study. Int. J. Dent. 2015, 2015, 415029. [Google Scholar] [CrossRef]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for Replacing Missing Teeth: Different Times for Loading Dental Implants. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, J.Y.K.; Rungcharassaeng, K.; Deflorian, M.; Weinstein, T.; Wang, H.-L.; Testori, T. Immediate Implant Placement and Provisionalization of Maxillary Anterior Single Implants. Periodontology 2000 2018, 77, 197–212. [Google Scholar] [CrossRef]
- Payer, M.; Heschl, A.; Wimmer, G.; Wegscheider, W.; Kirmeier, R.; Lorenzoni, M. Immediate Provisional Restoration of Screw-Type Implants in the Posterior Mandible: Results after 5 Years of Clinical Function. Clin. Oral Implant. Res. 2010, 21, 815–821. [Google Scholar] [CrossRef]
- Grandi, T.; Garuti, G.; Guazzi, P.; Tarabini, L.; Forabosco, A. Survival and Success Rates of Immediately and Early Loaded Implants: 12-Month Results from a Multicentric Randomized Clinical Study. J. Oral Implantol. 2012, 38, 239–249. [Google Scholar] [CrossRef] [PubMed]
- Ghoul, W.E.; Chidiac, J.J. Prosthetic Requirements for Immediate Implant Loading: A Review. J. Prosthodont. 2012, 21, 141–154. [Google Scholar] [CrossRef]
- Staubli, N.; Walter, C.; Schmidt, J.C.; Weiger, R.; Zitzmann, N.U. Excess Cement and the Risk of Peri-Implant Disease–A Systematic Review. Clin. Oral Implant. Res. 2017, 28, 1278–1290. [Google Scholar] [CrossRef]
- Kim, J.H.; Lee, S.J.; Park, J.S.; Ryu, J.J. Fracture Load of Monolithic CAD/CAM Lithium Disilicate Ceramic Crowns and Veneered Zirconia Crowns as a Posterior Implant Restoration. Implant. Dent. 2013, 22, 66–70. [Google Scholar] [CrossRef]
- Guess, P.C.; Zavanelli, R.A.; Silva, N.R.; Bonfante, E.A.; Coelho, P.G.; Thompson, V.P. Monolithic CAD/CAM Lithium Disilicate versus Veneered Y-TZP Crowns: Comparison of Failure Modes and Reliability after Fatigue. Int. J. Prosthodont. 2010, 23, 434–442. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender/Age | N | % | Age Min | Age Max | Age Mean | SD |
|---|---|---|---|---|---|---|
| Female | 8 | 40 | 31 | 70 | 42.9 | 12.7 |
| Male | 12 | 60 | 25 | 69 | 43.7 | 16.1 |
| Total | 20 | 100 | 26 | 70 | 43.3 | 14.5 |
| Implant Site | N | % |
|---|---|---|
| 11 | 1 | 5 |
| 12 | 1 | 5 |
| 13 | 1 | 5 |
| 14 | 2 | 10 |
| 21 | 2 | 10 |
| 24 | 2 | 10 |
| 25 | 2 | 10 |
| 35 | 1 | 5 |
| 36 | 3 | 15 |
| 46 | 5 | 25 |
| Implant Diameter (mm) | ||||
|---|---|---|---|---|
| 3.5 | 4 | 4.5 | ||
| Implant length (mm) | 10 | 2 | - | - |
| 12 | 4 | 6 | 3 | |
| 14 | 2 | 2 | 1 | |
| Implant Diameter (mm) | ||||
|---|---|---|---|---|
| 3.5 | 4 | 4.5 | ||
| Implant length (mm) | 10 | 2 | - | - |
| 12 | 1 | - | - | |
| 14 | 1 | - | - | |
| N | Min | Max | Mean | SD | p Value | ||
|---|---|---|---|---|---|---|---|
| BOP | baseline | 16 | 19 | 34 | 27.9 | 4.0 | |
| 4 years | 13 | 0 | 51.0 | 23.8 | 15.6 | p > 0.05 | |
| 8 years | 10 | 0 | 38 | 19.1 | 13.1 | p > 0.05 | |
| 11 years | 9 | 0 | 62 | 18.2 | 17.6 | p = 0.165 | |
| PI | baseline | 16 | 12 | 33 | 25.3 | 5.7 | |
| 4 years | 13 | 12 | 45 | 28.5 | 11.0 | p > 0.05 | |
| 8 years | 10 | 0 | 28 | 12.6 | 9.4 | p > 0.05 | |
| 11 years | 9 | 1 | 37 | 12.6 | 10.0 | p < 0.001 | |
| MBL | baseline | 16 | 0.69 | 2.19 | 1.40 | 0.43 | |
| 4 years | 14 | 1.12 | 3.07 | 1.99 | 0.57 | p = 0.001 | |
| 8 years | 12 | 0.83 | 2.85 | 1.70 | 0.64 | p = 0.019 | |
| 11 years | 11 | 1.01 | 2.60 | 1.59 | 0.53 | p = 0.027 | |
| resorption | 14 | −0.55 | 1.27 | 0.43 | 0.48 | p = 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steyer, E.; Herber, V.; Koller, M.; Végh, D.; Mukaddam, K.; Jakse, N.; Payer, M. Immediate Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Long-Term Results after 11 Years of Clinical Function. Materials 2021, 14, 6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226738
Steyer E, Herber V, Koller M, Végh D, Mukaddam K, Jakse N, Payer M. Immediate Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Long-Term Results after 11 Years of Clinical Function. Materials. 2021; 14(22):6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226738
Chicago/Turabian StyleSteyer, Elisabeth, Valentin Herber, Martin Koller, Dániel Végh, Khaled Mukaddam, Norbert Jakse, and Michael Payer. 2021. "Immediate Restoration of Single-Piece Zirconia Implants: A Prospective Case Series—Long-Term Results after 11 Years of Clinical Function" Materials 14, no. 22: 6738. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14226738