
The Granule Size Mediates the In Vivo Foreign Body Response and the Integration Behavior of Bone Substitutes

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Bone Substitute Materials
2.2. In Vivo Study
2.3. Histological Workup and Staining Methods
2.4. Analysis Methods
2.5. Statistics
3. Results
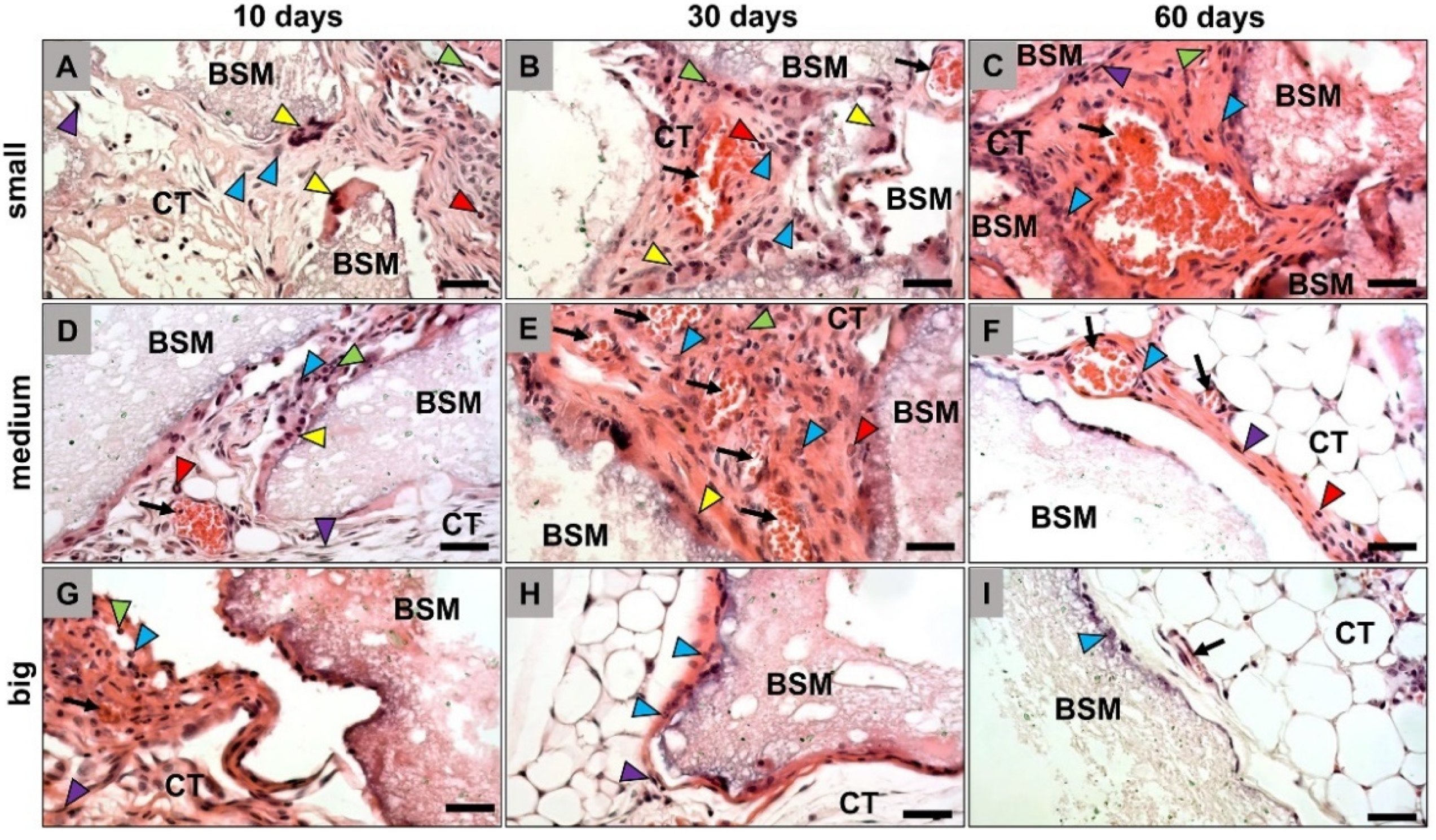
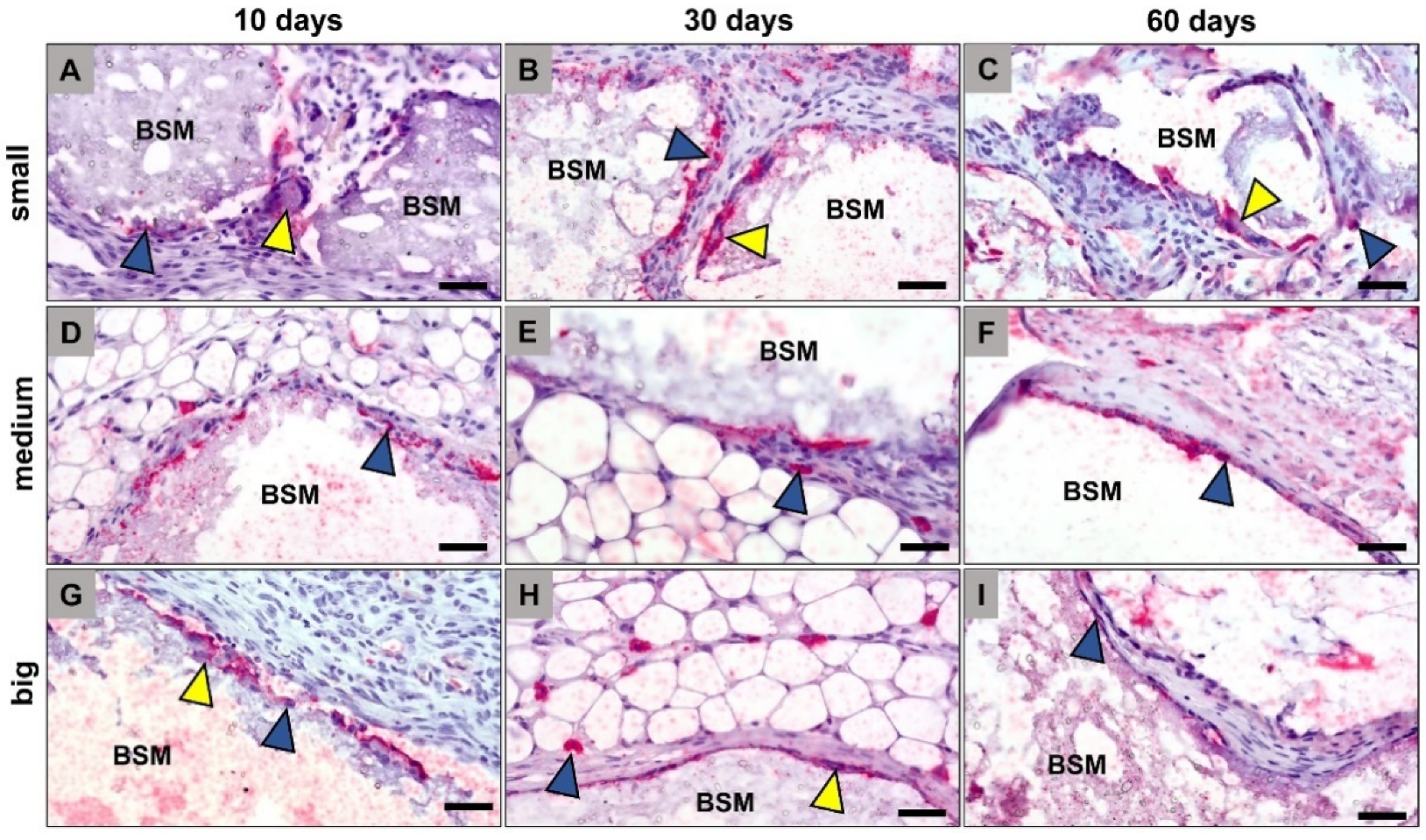
3.1. Histopathological Results
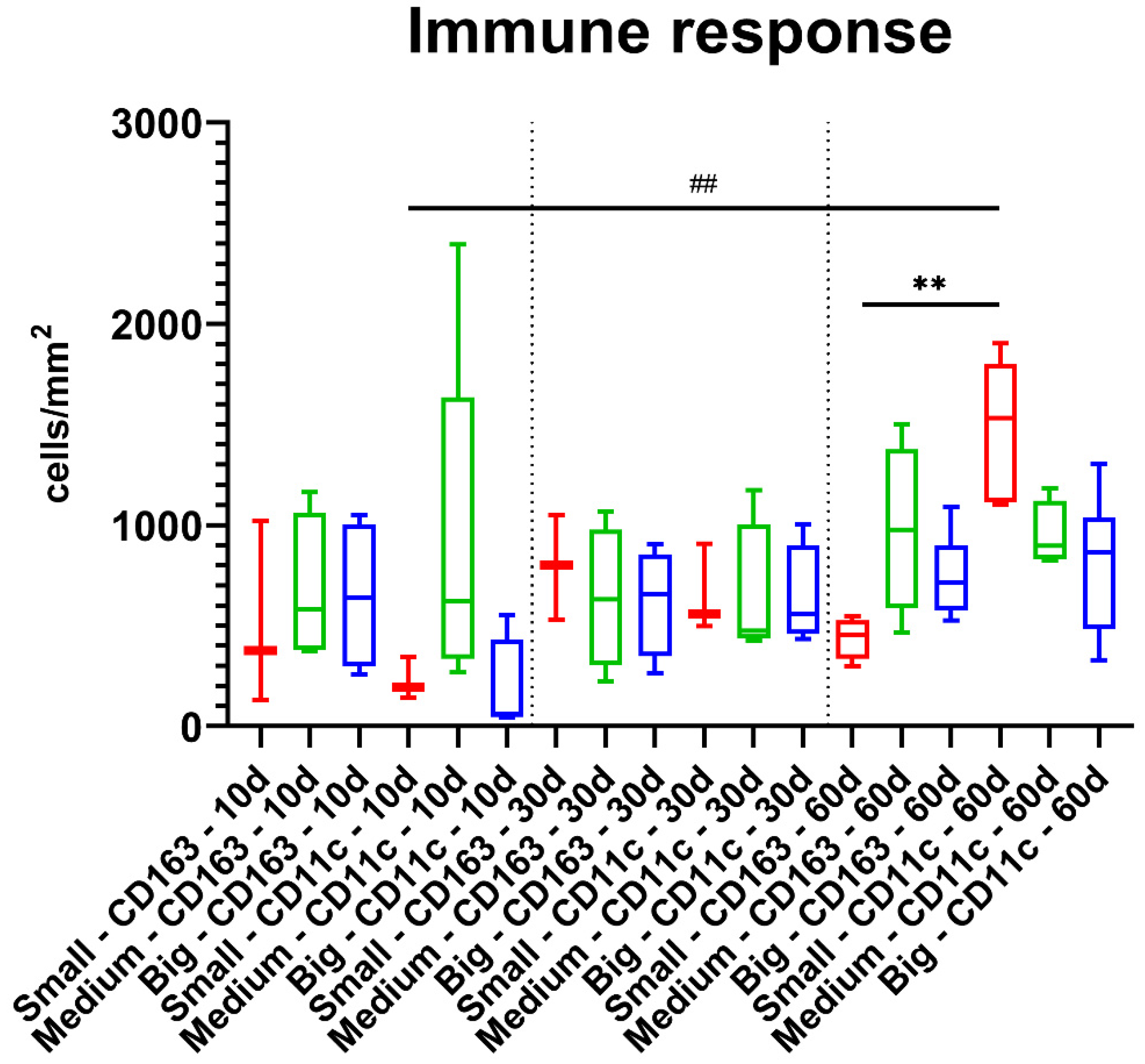
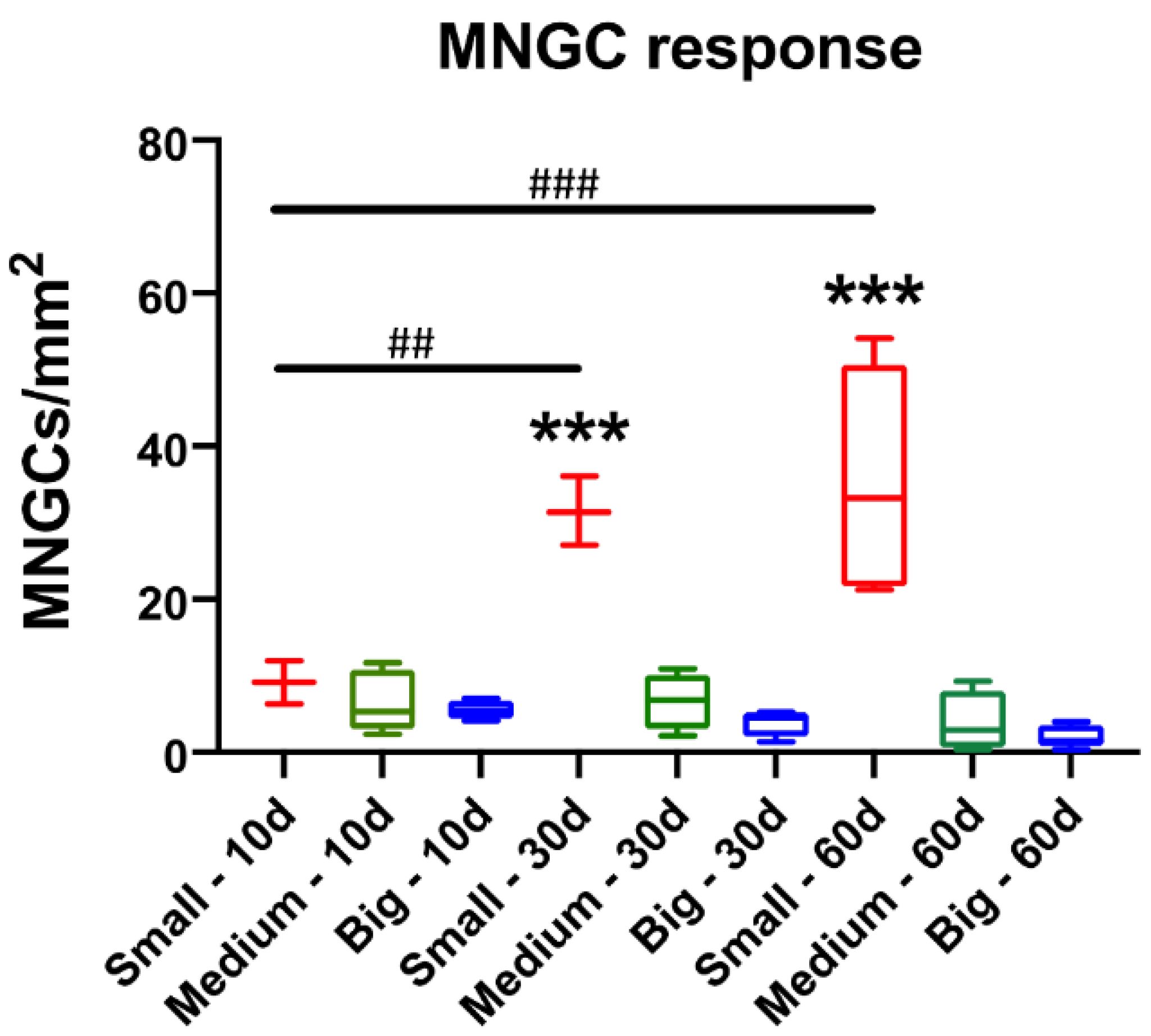
3.2. Histomorphometrical Results
4. Discussion
- (i)
- scenario 1: complete resorbability of a BSM mediated by mononuclear and multinucleated phagocytes,
- (ii)
- scenario 2: MNGC-mediated fibrous encapsulation of a biomaterial without mediation of a material-associated further healing process, and
- (iii)
- scenario 3: persistence of phagocytes at the surfaces of biomaterials that may support preservation of bone tissue within the implantation bed of a BSM by continuous expression and secretion of molecules involved in the bone healing process such that no resorption is processed by these cells.
- (1)
- The surface-to-volume ratio increases with decreasing particle size, which means that a much larger surface area is “available” in case of small granules (Table 1). Thus, the increased surface area may lead to increased “binding sites” for phagocytes. To further elaborate on this, the surface of the biomaterial (in our case the BSM) is initially adsorbed with small molecules (e.g., water molecules, ions, etc.) [29,42]. Which in turn increases forces like Van der Waal, hydrophobic/hydrophilic forces and so on. This dynamic increase of forces would attract the different types of blood proteins as they are complex molecules with different forces and active sites. By then ‘competitive’ adsorption occurs and the most fitting protein will adhere to the surface [42]. Macrophages are adhering-dependent cells, which means that this cell type even in the context of the foreign body response to biomaterials survive only if they can attach to a material. If prompted, the macrophages will fuse to form MNGCs [29,43]. The fusion always requires certain molecular mediators (cytokines), as well as proper surface adhesion [44]. The more surface area a biomaterial provides, the more macrophages and also MNGCs can attach.
- (2)
- Ion-induced MNGC formation is present in case of the small BSM granules. It is well known that Calcium phosphate-based biomaterials release Ca2+- and PO43−-ions over time [45,46]. Calcium ions bind to membrane associated soluble N-ethylmaleimide-sensitive-factor attachment receptor (SNARE) complexes found on secreting cells [44]. The binding results in the formation of channels that release water, which leads to a destabilization of the cell membrane. Finally, destabilization leads to membrane fusion [44,47]. Thus, it is conceivable that the increased surface area-to-volume leads to increased release of calcium ions, encouraging the fusion of the adherent macrophages.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rolvien, T.; Barbeck, M.; Wenisch, S.; Amling, M.; Krause, M. Cellular Mechanisms Responsible for Success and Failure of Bone Substitute Materials. Int. J. Mol. Sci. 2018, 19, 2893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titsinides, S.; Agrogiannis, G.; Karatzas, T. Bone grafting materials in dentoalveolar reconstruction: A comprehensive review. Jpn. Dent. Sci. Rev. 2018, 55, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Zizzari, V.L.; Zara, S.; Tetè, G.; Vinci, R.; Gherlone, E.; Cataldi, A. Biologic and clinical aspects of integration of different bone substitutes in oral surgery: A literature review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, 392–402. [Google Scholar] [CrossRef]
- Mardas, N.; Chadha, V.; Donos, N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin. Oral Implant. Res. 2010, 21, 688–698. [Google Scholar] [CrossRef] [PubMed]
- Tosta, M.; Cortes, A.R.G.; Corrêa, L.; Pinto, D.D.S.; Tumenas, I.; Katchburian, E. Histologic and histomorphometric evaluation of a synthetic bone substitute for maxillary sinus grafting in humans. Clin. Oral Implant. Res. 2011, 24, 866–870. [Google Scholar] [CrossRef]
- Barbeck, M.; Dard, M.; Kokkinopoulou, M.; Markl, J.; Booms, P.; Sader, R.A.; Kirkpatrick, C.J.; Ghanaati, S. Small-sized granules of biphasic bone substitutes support fast implant bed vascularization. Biomatter 2015, 5, e1056943. [Google Scholar] [CrossRef] [Green Version]
- Jang, J.-W.; Yun, J.-H.; Lee, K.I.; Jung, U.-W.; Kim, C.-S.; Choi, S.-H.; Cho, K.-S. Osteoinductive activity of biphasic calcium phosphate with different rhBMP-2 doses in rats. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2011, 113, 480–487. [Google Scholar] [CrossRef]
- Leiblein, M.; Koch, E.; Winkenbach, A.; Schaible, A.; Nau, C.; Büchner, H.; Schröder, K.; Marzi, I.; Henrich, D. Size matters: Effect of granule size of the bone graft substitute (Herafill®) on bone healing using Masquelet’s induced membrane in a critical size defect model in the rat’s femur. J. Biomed. Mater. Res. Part B: Appl. Biomater. 2019, 108, 1469–1482. [Google Scholar] [CrossRef] [Green Version]
- Malard, O.; Bouler, J.M.; Guicheux, J.; Heymann, D.; Pilet, P.; Coquard, C.; Daculsi, G. Influence of biphasic calcium phosphate granulometry on bone ingrowth, ceramic resorption, and inflammatory reactions: Preliminary in vitro and in vivo study. J. Biomed. Mater. Res. 1999, 46, 103–111. [Google Scholar] [CrossRef]
- Dondossola, E.; Holzapfel, B.M.; Alexander, S.; Filippini, S.; Hutmacher, D.W.; Friedl, P. Examination of the foreign body response to biomaterials by nonlinear intravital microscopy. Nat. Biomed. Eng. 2016, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Al-Maawi, S.; Wang, X.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Biomaterial-induced multinucleated giant cells express proinflammatory signaling molecules: A histological study in humans. J. Biomed. Mater. Res. Part A 2018, 107, 780–790. [Google Scholar] [CrossRef]
- Barbeck, M.; Jung, O.; Smeets, R.; Gosau, M.; Schnettler, R.; Rider, P.; Houshmand, A.; Korzinskas, T. Implantation of an Injectable Bone Substitute Material Enables Integration Following the Principles of Guided Bone Regeneration. In Vivo 2020, 34, 557–568. [Google Scholar] [CrossRef] [Green Version]
- Lindner, C.; Pröhl, A.; Abels, M.; Löffler, T.; Batinic, M.; Jung, O.; Barbeck, M. Specialized Histological and Histomorphometrical Analytical Methods for Biocompatibility Testing of Biomaterials for Maxillofacial Surgery in (Pre-) Clinical Studies. In Vivo 2020, 34, 3137–3152. [Google Scholar] [CrossRef] [PubMed]
- Bohner, M.; Santoni, B.L.G.; Döbelin, N. β-tricalcium phosphate for bone substitution: Synthesis and properties. Acta Biomater. 2020, 113, 23–41. [Google Scholar] [CrossRef] [PubMed]
- Hettich, G.; Schierjott, R.A.; Epple, M.; Gbureck, U.; Heinemann, S.; Mozaffari-Jovein, H.; Grupp, T.M. Calcium Phosphate Bone Graft Substitutes with High Mechanical Load Capacity and High Degree of Interconnecting Porosity. Materials 2019, 12, 3471. [Google Scholar] [CrossRef] [Green Version]
- Heinemann, S.; Rössler, S.; Lemm, M.; Ruhnow, M.; Nies, B. Properties of injectable ready-to-use calcium phosphate cement based on water-immiscible liquid. Acta Biomater. 2012, 9, 6199–6207. [Google Scholar] [CrossRef] [PubMed]
- Jung, O.; Radenkovic, M.; Stojanović, S.; Lindner, C.; Batinic, M.; Görke, O.; Pissarek, J.; Pröhl, A.; Najman, S.; Barbeck, M. In Vitro and In Vivo Biocompatibility Analysis of a New Transparent Collagen-based Wound Membrane for Tissue Regeneration in Different Clinical Indications. In Vivo 2020, 34, 2287–2295. [Google Scholar] [CrossRef] [PubMed]
- Steigmann, L.; Jung, O.; Kieferle, W.; Stojanovic, S.; Proehl, A.; Görke, O.; Emmert, S.; Najman, S.; Barbeck, M.; Rothamel, D. Biocompatibility and Immune Response of a Newly Developed Volume-Stable Magnesium-Based Barrier Membrane in Combination with a PVD Coating for Guided Bone Regeneration (GBR). Biomedicines 2020, 8, 636. [Google Scholar] [CrossRef]
- Oberdiek, F.; Vargas, C.; Rider, P.; Batinic, M.; Görke, O.; Radenković, M.; Najman, S.; Baena, J.; Jung, O.; Barbeck, M. Ex Vivo and In Vivo Analyses of Novel 3D-Printed Bone Substitute Scaffolds Incorporating Biphasic Calcium Phosphate Granules for Bone Regeneration. Int. J. Mol. Sci. 2021, 22, 3588. [Google Scholar] [CrossRef]
- Miron, R.J.; Bosshardt, D.D. Multinucleated Giant Cells: Good Guys or Bad Guys? Tissue Eng. Part B Rev. 2018, 24, 53–65. [Google Scholar] [CrossRef]
- Christo, S.N.; Diener, K.; Bachhuka, A.; Vasilev, K.; Hayball, J.D. Innate Immunity and Biomaterials at the Nexus: Friends or Foes. BioMed Res. Int. 2015, 2015, 342304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbeck, M.; Booms, P.; Unger, R.; Hoffmann, V.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. Multinucleated giant cells in the implant bed of bone substitutes are foreign body giant cells-New insights into the material-mediated healing process. J. Biomed. Mater. Res. Part A 2017, 105, 1105–1111. [Google Scholar] [CrossRef]
- Harkins, H.N. Simplified Technic of Onlay Grafts. J. Am. Med. Assoc. 1937, 109, 1501–1506. [Google Scholar] [CrossRef]
- Phemister, D.B. The fate of transplanted bone and regenerative power of its various constituents. Surg. Gynecol. Obstet. 1914, 19, 303–314. [Google Scholar]
- Ghanaati, S.; Barbeck, M.; Detsch, R.; Deisinger, U.; Hilbig, U.; Rausch, V.; Sader, R.; Unger, R.E.; Ziegler, G.; Kirkpatrick, C.J. The chemical composition of synthetic bone substitutes influences tissue reactions in vivo: Histological and histomorphometrical analysis of the cellular inflammatory response to hydroxyapatite, beta-tricalcium phosphate and biphasic calcium phosphate ceramics. Biomed. Mater. 2012, 7, 15005. [Google Scholar]
- Rider, P.; Kačarević, P.; Alkildani, S.; Retnasingh, S.; Schnettler, R.; Barbeck, M. Additive Manufacturing for Guided Bone Regeneration: A Perspective for Alveolar Ridge Augmentation. Int. J. Mol. Sci. 2018, 19, 3308. [Google Scholar] [CrossRef] [Green Version]
- Okuda, T.; Ioku, K.; Yonezawa, I.; Minagi, H.; Gonda, Y.; Kawachi, G.; Kamitakahara, M.; Shibata, Y.; Murayama, H.; Kurosawa, H.; et al. The slow resorption with replacement by bone of a hydrothermally synthesized pure calcium-deficient hydroxyapatite. Biomaterials 2008, 29, 2719–2728. [Google Scholar] [CrossRef] [PubMed]
- Barbeck, M.; Udeabor, S.; Lorenz, J.; Schlee, M.; Holthaus, M.G.; Raetscho, N.; Choukroun, J.; Sader, R.; Kirkpatrick, C.J.; Ghanaati, S. High-Temperature Sintering of Xenogeneic Bone Substitutes Leads to Increased Multinucleated Giant Cell Formation: In Vivo and Preliminary Clinical Results. J. Oral Implant. 2015, 41, e212–e222. [Google Scholar] [CrossRef]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [Green Version]
- Brown, B.N.; Ratner, B.D.; Goodman, S.B.; Amar, S.; Badylak, S.F. Macrophage polarization: An opportunity for improved outcomes in biomaterials and regenerative medicine. Biomaterials 2012, 33, 3792–3802. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, M.M.; Liu, J.; de Santiago, G.T.; Cha, B.-H.; Vishwakarma, A.; Ghaemmaghami, A.; Khademhosseini, A. Delivery strategies to control inflammatory response: Modulating M1–M2 polarization in tissue engineering applications. J. Control. Release 2016, 240, 349–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klopfleisch, R. Macrophage reaction against biomaterials in the mouse model–Phenotypes, functions and markers. Acta Biomater. 2016, 43, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, R.; Cameron, A.; Kelly, D.; Kearney, C.; O’Brien, F.J. Biomaterial based modulation of macrophage polarization: A review and suggested design principles. Mater. Today 2015, 18, 313–325. [Google Scholar] [CrossRef]
- Barbeck, M.; Schröder, M.-L.; Alkildani, S.; Jung, O.; Unger, R. Exploring the Biomaterial-Induced Secretome: Physical Bone Substitute Characteristics Influence the Cytokine Expression of Macrophages. Int. J. Mol. Sci. 2021, 22, 4442. [Google Scholar] [CrossRef] [PubMed]
- Ghanaati, S.; Barbeck, M.; Orth, C.; Willershausen, I.; Thimm, B.W.; Hoffmann, C.; Rasic, A.; Sader, R.A.; Unger, R.E.; Peters, F. Influence of β-tricalcium phosphate granule size and morphology on tissue reaction in vivo. Acta Biomater. 2010, 6, 4476–4487. [Google Scholar] [CrossRef]
- Jung, I.-H.; Choi, S.-H.; Pang, E.-K.; Kim, C.-S.; Cho, K.-S. The Effect of Varying the Particle Size of Beta Tricalcium Phosphate Carrier of Recombinant Human Bone Morphogenetic Protein-4 on Bone Formation in Rat Calvarial Defects. J. Periodontol. 2006, 77, 765–772. [Google Scholar] [CrossRef]
- Shrivastava, P.; Bagchi, T. IL-10 Modulates In Vitro Multinucleate Giant Cell Formation in Human Tuberculosis. PLoS ONE 2013, 8, e77680. [Google Scholar] [CrossRef] [Green Version]
- Shi, Z.; Huang, X.; Cai, Y.; Tang, R.; Yang, D. Size effect of hydroxyapatite nanoparticles on proliferation and apoptosis of osteoblast-like cells. Acta Biomater. 2009, 5, 338–345. [Google Scholar] [CrossRef]
- Sun, J.-S.; Liu, H.-C.; Chang, W.H.; Li, J.; Lin, F.-H.; Tai, H.-C. Influence of hydroxyapatite particle size on bone cell activities: Anin vitro study. J. Biomed. Mater. Res. 1998, 39, 390–397. [Google Scholar] [CrossRef]
- Coathup, M.J.; Cai, Q.; Campion, C.; Buckland, T.; Blunn, G.W. The effect of particle size on the osteointegration of injectable silicate-substituted calcium phosphate bone substitute materials. J. Biomed. Mater. Res. Part B Appl. Biomater. 2013, 101B, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Carvalho, A.L.; Faria, P.E.P.; Grisi, M.F.M.; Souza, S.L.S.; Taba, M.J.; Palioto, D.B.; Novaes, A.B.J.; Fraga, A.F.; Ozyegin, L.S.; Oktar, F.N.; et al. Effects of Granule Size on the Osteoconductivity of Bovine and Synthetic Hydroxyapatite: A Histologic and Histometric Study in Dogs. J. Oral Implant. 2007, 33, 267–276. [Google Scholar] [CrossRef]
- Aiyelabegan, H.T.; Sadroddiny, E. Fundamentals of protein and cell interactions in biomaterials. Biomed. Pharmacother. 2017, 88, 956–970. [Google Scholar] [CrossRef] [PubMed]
- Vignery, A. Macrophage fusion. J. Exp. Med. 2005, 202, 337–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheikh, Z.; Brooks, P.J.; Barzilay, O.; Fine, N.; Glogauer, M. Macrophages, Foreign Body Giant Cells and Their Response to Implantable Biomaterials. Materials 2015, 8, 5671–5701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witek, L.; Shi, Y.; Smay, J. Controlling calcium and phosphate ion release of 3D printed bioactive ceramic scaffolds: An in vitro study. J. Adv. Ceram. 2017, 6, 157–164. [Google Scholar] [CrossRef] [Green Version]
- Monchau, F.; Lefèvre, A.; Descamps, M.; Belquin-Myrdycz, A.; Laffargue, P.; Hildebrand, H. In vitro studies of human and rat osteoclast activity on hydroxyapatite, β-tricalcium phosphate, calcium carbonate. Biomol. Eng. 2002, 19, 143–152. [Google Scholar] [CrossRef]
- Allolio, C.; Harries, D. Calcium ions promote membrane fusion by forming negative-curvature inducing clusters on specific anionic lipids. ACS Nano 2020, 15, 12880–12887. [Google Scholar] [CrossRef]
- de Vernejoul, M.C. Bone remodelling in osteoporosis. Clin. Rheumatol. 1989, 8 (Suppl. 2), 13–15. [Google Scholar] [CrossRef]
- Kang, Y.; Zhang, Z.-J.; Zhao, X.-Y.; Zhang, Z.-Q.; Sheng, P.-Y.; Liao, W.-M. Total hip arthroplasty for vascular necrosis of the femoral head in patients with systemic lupus erythematosus: A midterm follow-up study of 28 hips in 24 patients. Eur. J. Orthop. Surg. Traumatol. 2012, 23, 73–79. [Google Scholar] [CrossRef]
- Ambard, A.J.; Mueninghoff, L. Calcium Phosphate Cement: Review of Mechanical and Biological Properties. J. Prosthodont. 2006, 15, 321–328. [Google Scholar] [CrossRef]
- Tamimi, F.; Torres, J.; Bassett, D.; Barralet, J.; Cabarcos, E.L. Resorption of monetite granules in alveolar bone defects in human patients. Biomaterials 2010, 31, 2762–2769. [Google Scholar] [CrossRef] [PubMed]
- Mayer, Y.; Ben-Dor, A.; Zigdon-Giladi, H.; Gutmacher, Z. Dimensional changes in the sinus membrane following maxillary sinus augmentation. Quintessence Int. 2018, 49, 841–847. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Granulate | Granulate Diameter [mm] | Surface Area to Volume Ratio [mm−1] |
|---|---|---|
| Small | 0.355–0.500 | 12–16.9 |
| Medium | 0.500–1.000 | 6–12 |
| Big | 1.000–2.000 | 3–6 |
| Timepoint/Size | Small | Medium | Big | |||
|---|---|---|---|---|---|---|
| CD163+ | CD11c+ | CD163+ | CD11c+ | CD163+ | CD11c+ | |
| Day 10 | 508.6 ± 459.2 | 226.8 ± 104.7 | 793.6 ± 259.8 | 654.9 ± 221.1 | 435.9 ± 101.6 | 1473.0 ± 353.3 |
| Day 30 | 692.6 ± 354.1 | 912.7 ± 860.3 | 638.9 ± 350.9 | 637.9 ± 357.6 | 981.7 ± 422.0 | 949.3 ± 161.9 |
| Day 60 | 646.7 ± 372.7 | 180.6 ± 250.4 | 619.8 ± 268.7 | 638.2 ± 251.4 | 744.5 ± 209.4 | 807.5 ± 343.1 |
| Small (MNGCs/mm2) | Medium (MNGCs/mm2) | Big (MNGCs/mm2) | |
|---|---|---|---|
| Day 10 | 9.15 ± 2.82 | 6.59 ± 4.01 | 5.54 ± 1.25 |
| Day 30 | 31.53 ± 4.49 | 6.67 ± 3.64 | 3.94 ± 1.77 |
| Day 60 | 35.60 ± 14.73 | 3.87 ± 3.98 | 1.96 ± 1.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abels, M.; Alkildani, S.; Pröhl, A.; Xiong, X.; Krastev, R.; Korzinskas, T.; Stojanovic, S.; Jung, O.; Najman, S.; Barbeck, M. The Granule Size Mediates the In Vivo Foreign Body Response and the Integration Behavior of Bone Substitutes. Materials 2021, 14, 7372. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14237372
Abels M, Alkildani S, Pröhl A, Xiong X, Krastev R, Korzinskas T, Stojanovic S, Jung O, Najman S, Barbeck M. The Granule Size Mediates the In Vivo Foreign Body Response and the Integration Behavior of Bone Substitutes. Materials. 2021; 14(23):7372. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14237372
Chicago/Turabian StyleAbels, Manuel, Said Alkildani, Annica Pröhl, Xin Xiong, Rumen Krastev, Tadas Korzinskas, Sanja Stojanovic, Ole Jung, Stevo Najman, and Mike Barbeck. 2021. "The Granule Size Mediates the In Vivo Foreign Body Response and the Integration Behavior of Bone Substitutes" Materials 14, no. 23: 7372. https://0-doi-org.brum.beds.ac.uk/10.3390/ma14237372