

Bioactive Inorganic Materials for Dental Applications: A Narrative Review
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction

- (i)
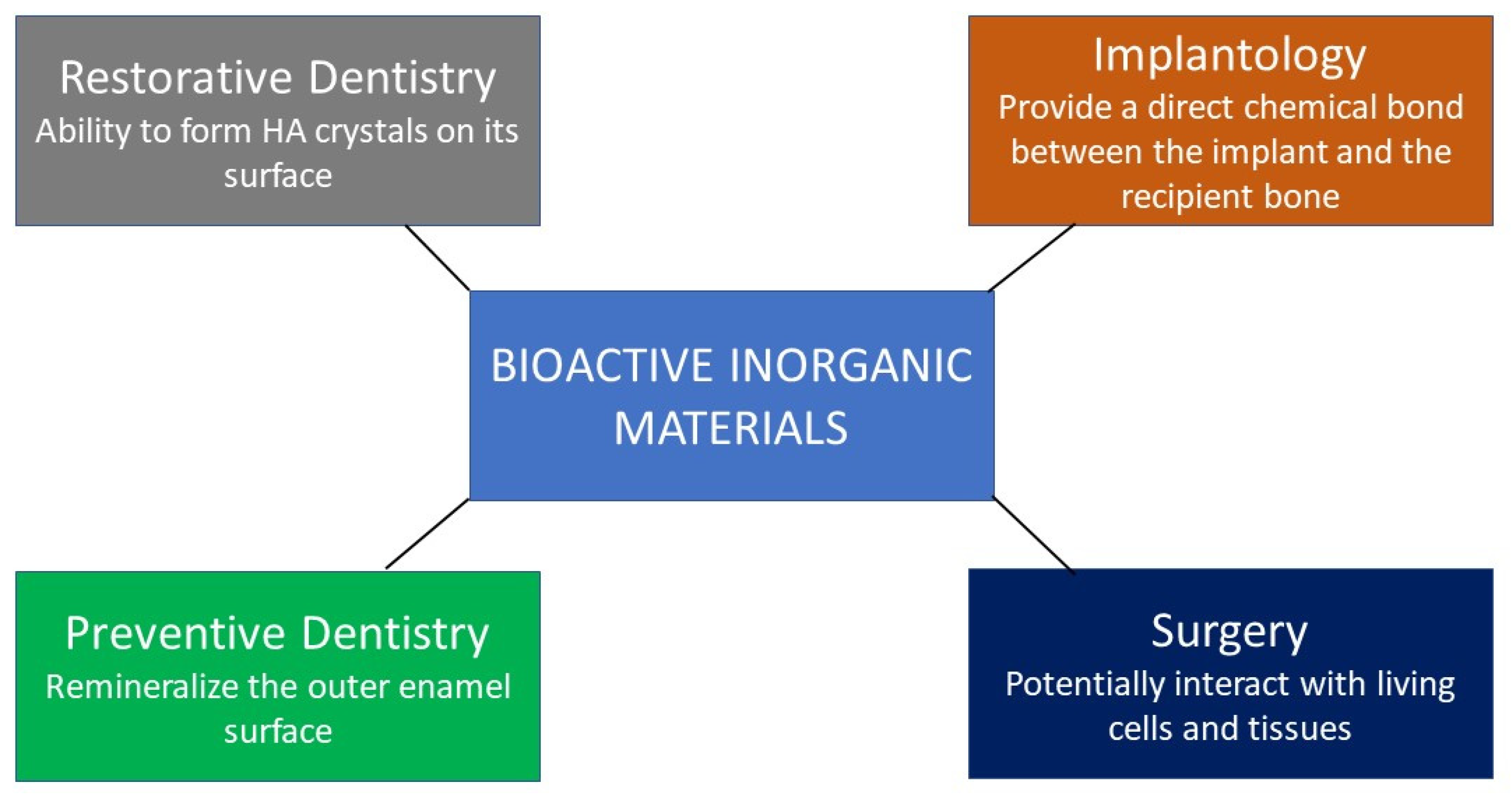
- Use of bioactive inorganic materials i.e., amorphous calcium phosphate, hydroxyapatite, tri-calcium phosphate, bioactive glass, and calcium silicate for dental applications, including restorative dentistry (adhesives and fillings), endodontics, periodontology, implantology, and surgery.
- (ii)
- Bioactive inorganic material’s studies included lab-based analysis, in vitro, in vivo, and clinical trials.
- (i)
- Studies not published in indexed journals.
- (ii)
- Grey literature and articles published in non-English language.
2. Bioactive Inorganic Materials
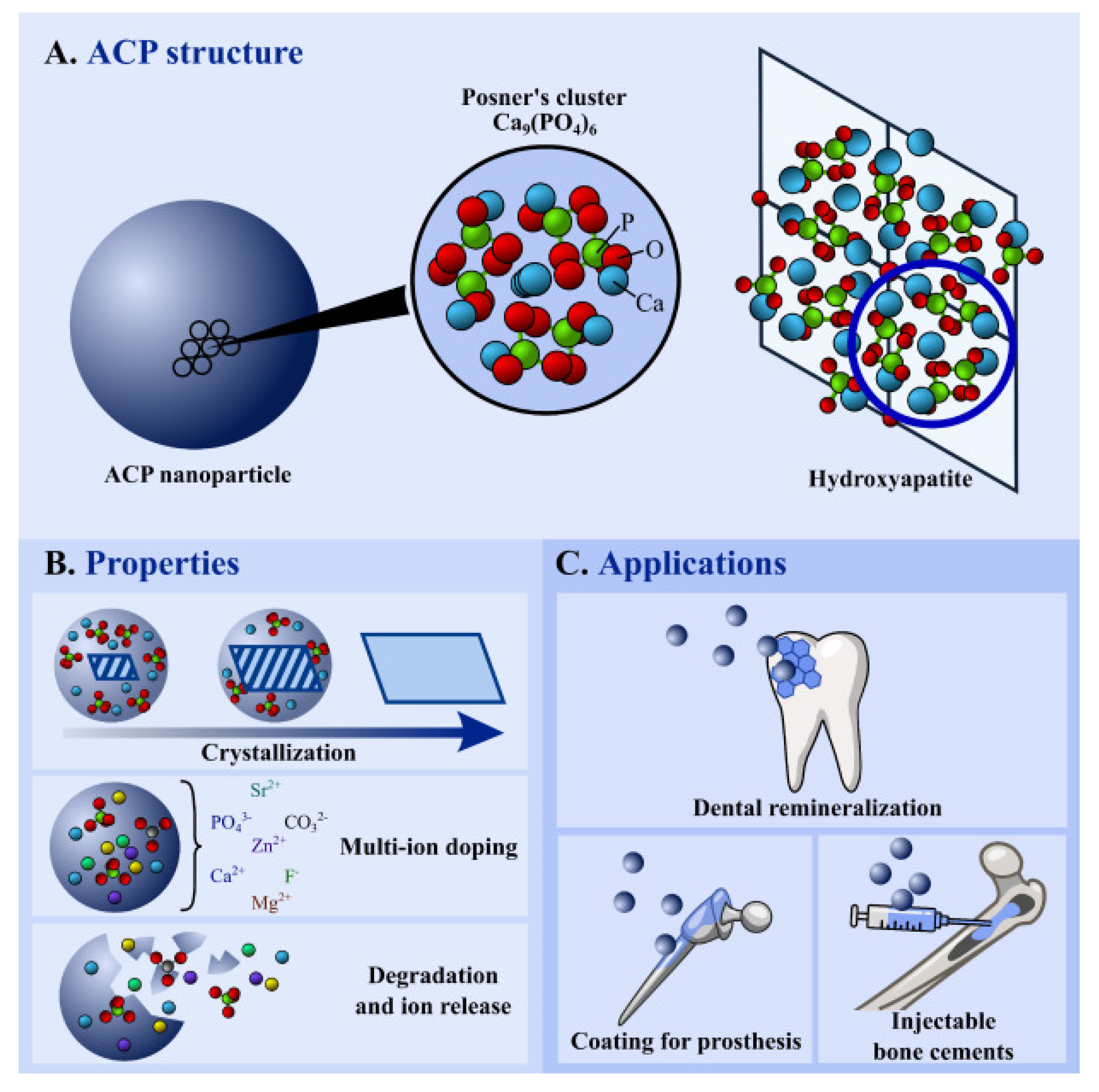
2.1. Amorphous Calcium Phosphates (ACP)
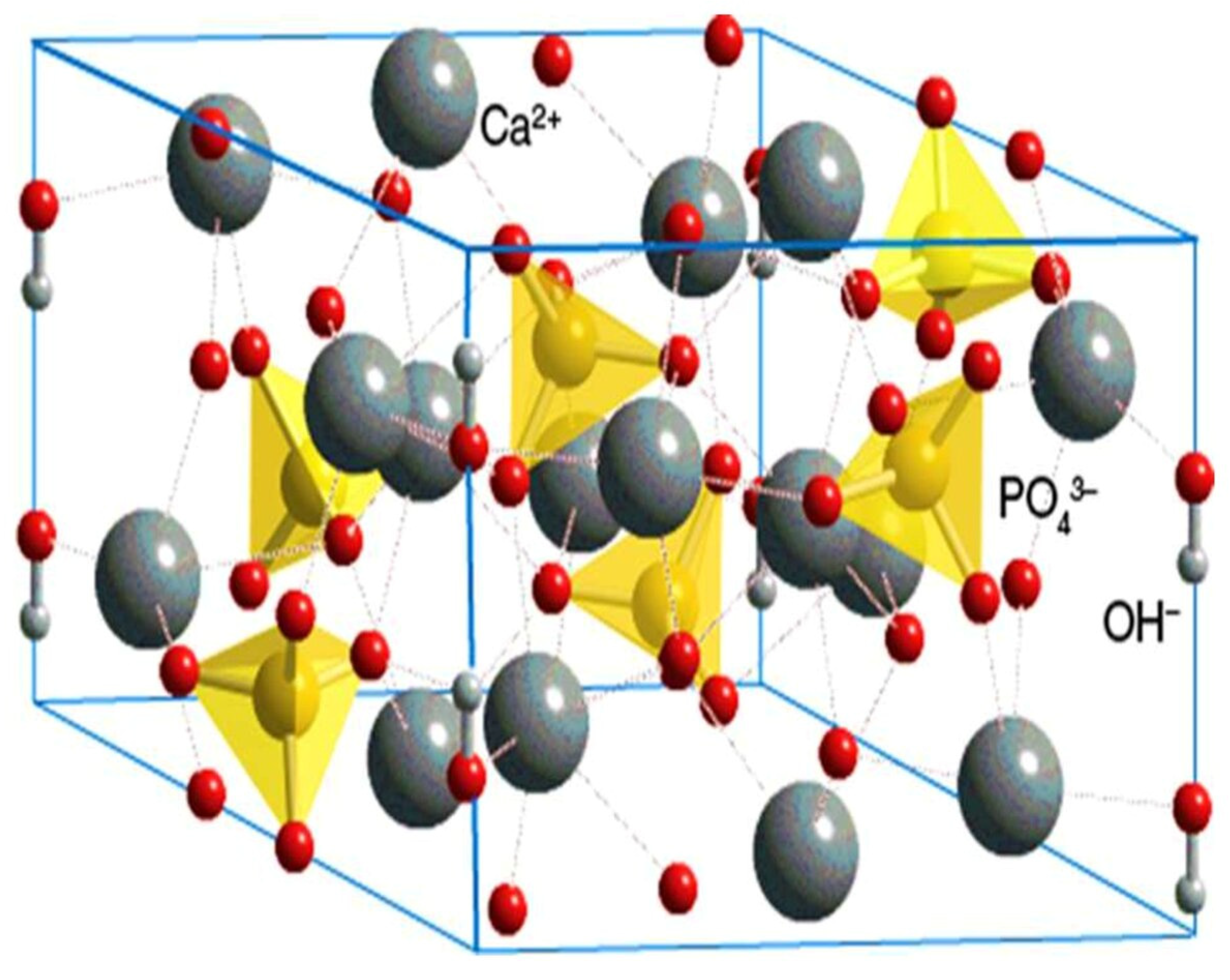
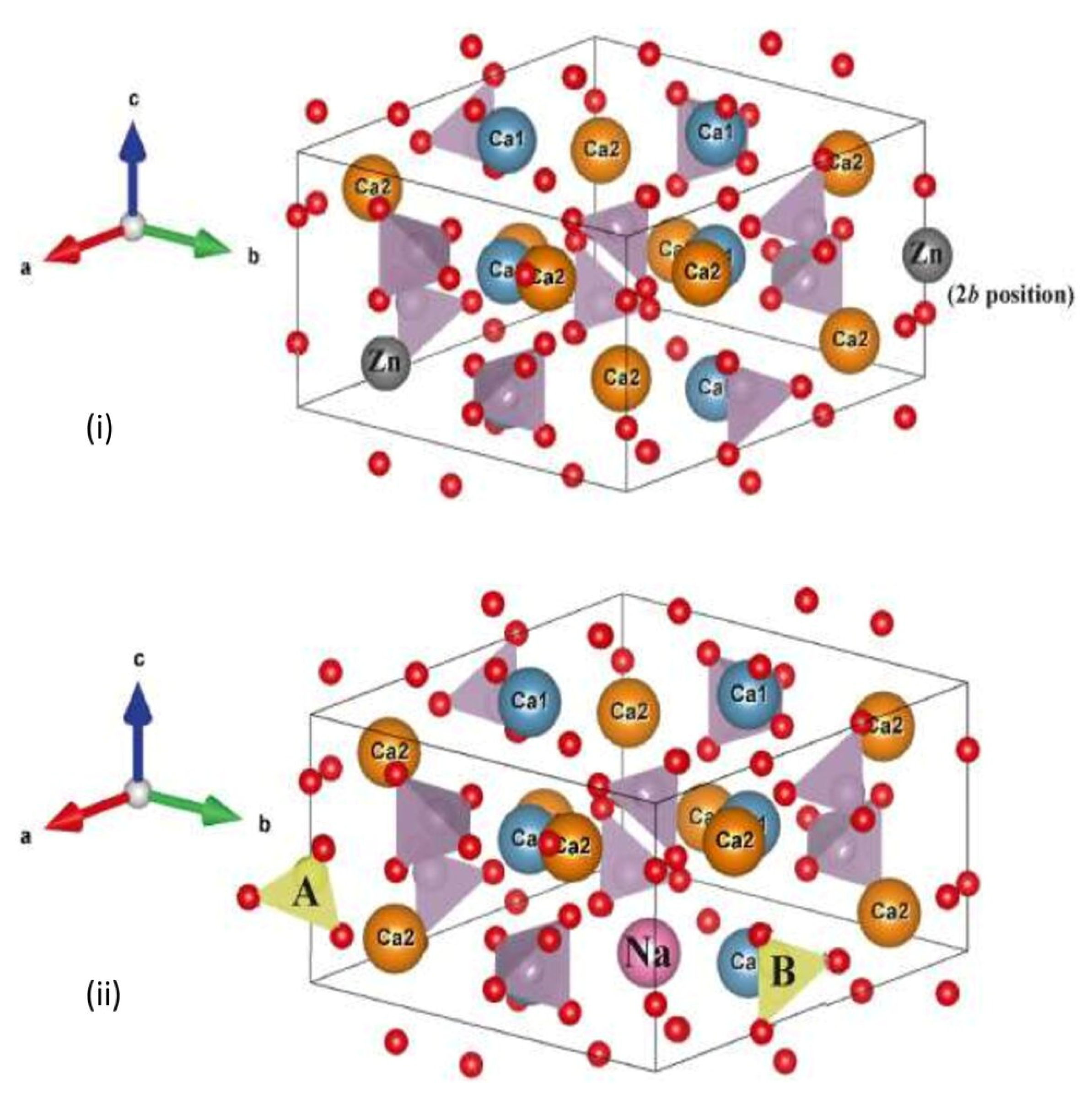
2.2. Hydroxyapatite (HA)
2.3. Tricalcium Phosphates (TCP)


2.4. Bioactive Glass

2.5. Calcium Silicate
3. Clinical Applications of Bioactive Inorganic Materials in Dentistry
3.1. Restorative Dentistry Application
3.2. Endodontic Application
3.3. Periodontal Applications
3.4. Surgical Applications
3.5. Implant Coatings
4. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gul, H.; Khan, M.; Khan, A.S. Bioceramics: Types and clinical applications. In Handbook of Ionic Substituted Hydroxyapatites; Elsevier: Amsterdam, The Netherlands, 2020; pp. 53–83. [Google Scholar]
- Piconi, C.; Maccauro, G.; Muratori, F.; Del Prever, E.B. Alumina and zirconia ceramics in joint replacements. J. Appl. Biomater. Biomech. 2003, 1, 19–32. [Google Scholar] [PubMed]
- Piconi, C.; Sprio, S. Oxide bioceramic composites in orthopedics and dentistry. J. Compos. Sci. 2021, 5, 206. [Google Scholar] [CrossRef]
- Abraham, C.M. A brief historical perspective on dental implants, their surface coatings and treatments. Open Dent. J. 2014, 8, 50–55. [Google Scholar] [CrossRef]
- Smith, L. Ceramic-plastic material as a bone substitute. Arch. Surg. 1963, 87, 653–661. [Google Scholar] [CrossRef]
- Jamari, J.; Ammarullah, M.I.; Santoso, G.; Sugiharto, S.; Supriyono, T.; Prakoso, A.T.; Basri, H.; van der Heide, E. Computational Contact Pressure Prediction of CoCrMo, SS 316L and Ti6Al4V Femoral Head against UHMWPE Acetabular Cup under Gait Cycle. J. Funct. Biomater. 2022, 13, 64. [Google Scholar] [CrossRef]
- Massin, P.; Lopes, R.; Masson, B.; Mainard, D. Does Biolox® Delta ceramic reduce the rate of component fractures in total hip replacement? Orthop. Traumatol. Surg. Res. 2014, 100, S317–S321. [Google Scholar] [CrossRef]
- Udduttula, A.; Zhang, J.V.; Ren, P.-G. Bioinert Ceramics for Biomedical Applications; Wiley: Hoboken, NJ, USA, 2019. [Google Scholar]
- Li, J.; Hastings, G. Oxide bioceramics: Inert ceramic materials in medicine and dentistry. In Handbook of Biomaterial Properties; Springer: Cham, Switzerland, 2016; pp. 339–352. [Google Scholar]
- Vallet-Regí, M. Evolution of bioceramics within the field of biomaterials. Comptes Rendus Chim. 2010, 13, 174–185. [Google Scholar] [CrossRef]
- Punj, S.; Singh, J.; Singh, K. Ceramic biomaterials: Properties, state of the art and future prospectives. Ceram. Int. 2021, 47, 28059–28074. [Google Scholar] [CrossRef]
- Khan, A.S.; Chaudhry, A.A. Handbook of Ionic Substituted Hydroxyapatites; Woodhead Publishing: Cambridge, UK, 2019. [Google Scholar]
- Khan, A.S.; Syed, M.R. A review of bioceramics-based dental restorative materials. Dent. Mater. J. 2019, 38, 163–176. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Nancollas, G.H. Calcium orthophosphates: Crystallization and dissolution. Chem. Rev. 2008, 108, 4628–4669. [Google Scholar] [CrossRef]
- Vallet-Regí, M.; González-Calbet, J.M. Calcium phosphates as substitution of bone tissues. Prog. Solid State Chem. 2004, 32, 1–31. [Google Scholar] [CrossRef]
- Gokcekaya, O.; Ergun, C.; Webster, T.J.; Bahadir, A.; Ueda, K.; Narushima, T.; Nakano, T. Effect of Precursor Deficiency Induced Ca/P Ratio on Antibacterial and Osteoblast Adhesion Properties of Ag-Incorporated Hydroxyapatite: Reducing Ag Toxicity. Materials 2021, 14, 3158. [Google Scholar] [CrossRef] [PubMed]
- Kantharia, N.; Naik, S.; Apte, S.; Kheur, M.; Kheur, S.; Kale, B. Nano-hydroxyapatite and its contemporary applications. Bone 2014, 34, 1–71. [Google Scholar] [CrossRef] [Green Version]
- Kono, T.; Sakae, T.; Nakada, H.; Kaneda, T.; Okada, H. Confusion between Carbonate Apatite and Biological Apatite (Carbonated Hydroxyapatite) in Bone and Teeth. Minerals 2022, 12, 170. [Google Scholar] [CrossRef]
- Bystrov, V.; Paramonova, E.; Avakyan, L.; Coutinho, J.; Bulina, N. Simulation and Computer Study of Structures and Physical Properties of Hydroxyapatite with Various Defects. Nanomaterials 2021, 11, 2752. [Google Scholar] [CrossRef]
- Iftikhar, S.; Jahanzeb, N.; Saleem, M.; Ur Rehman, S.; Matinlinna, J.P.; Khan, A.S. The trends of dental biomaterials research and future directions: A mapping review. Saudi Dent. J. 2021, 33, 229–238. [Google Scholar] [CrossRef]
- Spanuolo, G. Bioactive Dental Materials: The Current Status. Materials 2022, 15, 2016. [Google Scholar] [CrossRef]
- Melo, M.A.; Collares, F.; Sauro, S. Editorial: Developing Bioactive Materials for Dental Applications. Front. Mater. 2021, 8, 1618. [Google Scholar] [CrossRef]
- Kharouf, N.; Arntz, Y.; Eid, A.; Zghal, J.; Sauro, S.; Haikel, Y.; Mancino, D. Physicochemical and Antibacterial Properties of Novel, Premixed Calcium Silicate-Based Sealer Compared to Powder–Liquid Bioceramic Sealer. J. Clin. Med. 2020, 9, 3096. [Google Scholar] [CrossRef]
- Eid, A.; Mancino, D.; Rekab, M.S.; Haikel, Y.; Kharouf, N. Effectiveness of Three Agents in Pulpotomy Treatment of Permanent Molars with Incomplete Root Development: A Randomized Controlled Trial. Healthcare 2022, 10, 431. [Google Scholar] [CrossRef]
- Melo, M.A.; Mei, M.L.; Li, K.C.; Hamama, H.H. The Use of Bioactive Materials in Caries Management. Front. Oral Health 2022, 3, 832285. [Google Scholar] [CrossRef] [PubMed]
- Widbiller, M.; Jeanneau, C.; Galler, K.M.; Laurent, P. Biocompatibility and Bioactive Properties of Biodentine TM. In Biodentine™; Springer: Cham, Switzerland, 2022; pp. 31–50. [Google Scholar]
- Sequeira, D.B.; Oliveira, A.R.; Seabra, C.M.; Palma, P.J.; Ramos, C.; Figueiredo, M.H.; Santos, A.C.; Cardoso, A.L.; Peça, J.; Santos, J.M. Regeneration of pulp-dentin complex using human stem cells of the apical papilla: In vivo interaction with two bioactive materials. Clin. Oral Investig. 2021, 25, 5317–5329. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Mikos, A.G.; Reis, R.L.; Zhang, X. Translation of biomaterials from bench to clinic. Bioact. Mater. 2022, 18, 337–338. [Google Scholar] [CrossRef] [PubMed]
- Cao, W.; Hench, L.L. Bioactive materials. Ceram. Int. 1996, 22, 493–507. [Google Scholar] [CrossRef]
- Mano, J.F.; Sousa, R.A.; Boesel, L.F.; Neves, N.M.; Reis, R.L. Bioinert, biodegradable and injectable polymeric matrix composites for hard tissue replacement: State of the art and recent developments. Compos. Sci. Technol. 2004, 64, 789–817. [Google Scholar] [CrossRef] [Green Version]
- Höland, W.; Schweiger, M.; Watzke, R.; Peschke, A.; Kappert, H. Ceramics as biomaterials for dental restoration. Expert Rev. Med. Devices 2008, 5, 729–745. [Google Scholar] [CrossRef]
- Vallittu, P.K.; Boccaccini, A.R.; Hupa, L.; Watts, D.C. Bioactive dental materials-Do they exist and what does bioactivity mean? Dent. Mater. Off. Publ. Acad. Dent. Mater. 2018, 34, 693–694. [Google Scholar] [CrossRef]
- Raghavendra, S.S.; Jadhav, G.R.; Gathani, K.M.; Kotadia, P. Bioceramics in endodontics—A review. J. Istanb. Univ. Fac. Dent. 2017, 51, S128–S137. [Google Scholar] [CrossRef]
- Al-Haddad, A.; Che Ab Aziz, Z.A. Bioceramic-Based Root Canal Sealers: A Review. Int. J. Biomater. 2016, 2016, 9753210. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Bogen, G.; Lim, J.; Shon, W.J.; Kang, M.K. Bioceramic Materials and the Changing Concepts in Vital Pulp Therapy. J. Calif. Dent. Assoc. 2016, 44, 278–290. [Google Scholar]
- Prati, C.; Gandolfi, M.G. Calcium silicate bioactive cements: Biological perspectives and clinical applications. Dent. Mater. Off. Publ. Acad. Dent. Mater. 2015, 31, 351–370. [Google Scholar] [CrossRef] [PubMed]
- Ladino, L.G.; Bernal, A.; Calderón, D.; Cortés, D. Bioactive Materials in Restorative Dentistry: A Literature Review. SVOA Dent. 2021, 2, 74–81. [Google Scholar]
- Jefferies, S.R. Bioactive and biomimetic restorative materials: A comprehensive review. Part I. J. Esthet. Restor. Dent. Off. Publ. Am. Acad. Esthet. Dent. 2014, 26, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Montazerian, M.; Hosseinzadeh, F.; Migneco, C.; Fook, M.V.L.; Baino, F. Bioceramic coatings on metallic implants: An overview. Ceram. Int. 2022, 48, 8987–9005. [Google Scholar] [CrossRef]
- Arcos, D.; Vallet-Regí, M. Substituted hydroxyapatite coatings of bone implants. J. Mater. Chem. B 2020, 8, 1781–1800. [Google Scholar] [CrossRef]
- Cravens, J. Lacto-phosphate of lime; pathology and treatment of exposed dental pulps and sensitive dentine. Dent Cosm. 1876, 18, 463–469. [Google Scholar]
- Boskey, A.L. Amorphous calcium phosphate: The contention of bone. J. Dent. Res. 1997, 76, 1433. [Google Scholar] [CrossRef]
- Li, Y.-B.; Li, D.-X.; Weng, W.-J. Amorphous calcium phosphates and its biomedical application. J. Inorgan. Mater. 2007, 22, 775–782. [Google Scholar]
- Degli Esposti, L.; Iafisco, M. Amorphous calcium phosphate, the lack of order is an abundance of possibilities. Biomater. Biosyst. 2022, 5, 100037. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphates as bioceramics: State of the art. J. Funct. Biomater. 2010, 1, 22–107. [Google Scholar] [CrossRef] [Green Version]
- Skallevold, H.E.; Rokaya, D.; Khurshid, Z.; Zafar, M.S. Bioactive Glass Applications in Dentistry. Int. J. Mol. Sci. 2019, 20, 5960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsuji, T.; Onuma, K.; Yamamoto, A.; Iijima, M.; Shiba, K. Direct transformation from amorphous to crystalline calcium phosphate facilitated by motif-programmed artificial proteins. Proc. Natl. Acad. Sci. USA 2008, 105, 16866–16870. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duman, E.; Şahin Kehribar, E.; Ahan, R.E.; Yuca, E.; Şeker, U.Ö.Ş. Biomineralization of Calcium Phosphate Crystals Controlled by Protein–Protein Interactions. ACS Biomater. Sci. Eng. 2019, 5, 4750–4763. [Google Scholar] [CrossRef] [Green Version]
- Eanes, E.D. Amorphous Calcium Phosphate: Thermodynamic and Kinetic Considerations. In Calcium Phosphates in Biological and Industrial Systems; Amjad, Z., Ed.; Springer: Boston, MA, USA, 1998; pp. 21–39. [Google Scholar]
- Skrtic, D.; Antonucci, J.M.; Eanes, E.D.; Eichmiller, F.C.; Schumacher, G.E. Physicochemical evaluation of bioactive polymeric composites based on hybrid amorphous calcium phosphates. J. Biomed. Mater. Res. Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2000, 53, 381–391. [Google Scholar] [CrossRef]
- Xu, H.H.; Moreau, J.L.; Sun, L.; Chow, L.C. Nanocomposite containing amorphous calcium phosphate nanoparticles for caries inhibition. Dent. Mater. 2011, 27, 762–769. [Google Scholar] [CrossRef] [Green Version]
- Brunner, T.J.; Grass, R.N.; Bohner, M.; Stark, W.J. Effect of particle size, crystal phase and crystallinity on the reactivity of tricalcium phosphate cements for bone reconstruction. J. Mater. Chem. 2007, 17, 4072–4078. [Google Scholar] [CrossRef]
- Reynolds, E.C. Anticariogenic complexes of amorphous calcium phosphate stabilized by casein phosphopeptides: A review. Spec. Care Dent. 1998, 18, 8–16. [Google Scholar] [CrossRef]
- Yang, Y.; Xu, Z.; Guo, Y.; Zhang, H.; Qiu, Y.; Li, J.; Ma, D.; Li, Z.; Zhen, P.; Liu, B. Novel core–shell CHX/ACP nanoparticles effectively improve the mechanical, antibacterial and remineralized properties of the dental resin composite. Dent. Mater. 2021, 37, 636–647. [Google Scholar] [CrossRef]
- Gross, K.A.; Saber-Samandari, S.; Heemann, K.S. Evaluation of commercial implants with nanoindentation defines future development needs for hydroxyapatite coatings. J. Biomed. Mater. Res. Part B Appl. Biomater. 2010, 93, 1–8. [Google Scholar] [CrossRef]
- Saber-Samandari, S.; Gross, K.A. The use of thermal printing to control the properties of calcium phosphate deposits. Biomaterials 2010, 31, 6386–6393. [Google Scholar] [CrossRef]
- Saber-Samandari, S.; Gross, K.A. Amorphous calcium phosphate offers improved crack resistance: A design feature from nature? Acta Biomater. 2011, 7, 4235–4241. [Google Scholar] [CrossRef] [PubMed]
- Combes, C.; Rey, C. Amorphous calcium phosphates: Synthesis, properties and uses in biomaterials. Acta Biomater. 2010, 6, 3362–3378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huec, J.C.L.; Faundez, A.; Aunoble, S.; Sadikki, R.; Rigal, J. New Composite Material: PLLA and Tricalcium Phosphate for Orthopaedic Applications-In Vitro and In Vivo Studies (Part 1). In Biomechanics and Biomaterials in Orthopedics; Springer: Cham, Switzerland, 2016; pp. 173–180. [Google Scholar]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone substitutes: An update. Injury 2005, 36, S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Garley, A.; Hoff, S.E.; Saikia, N.; Jamadagni, S.; Baig, A.; Heinz, H. Adsorption and Substitution of Metal Ions on Hydroxyapatite as a Function of Crystal Facet and Electrolyte pH. J. Phys. Chem. C. 2019, 123, 16982–16993. [Google Scholar] [CrossRef]
- Ressler, A.; Žužić, A.; Ivanišević, I.; Kamboj, N.; Ivanković, H. Ionic substituted hydroxyapatite for bone regeneration applications: A review. Open Ceram. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Ergun, C.; Webster, T.J.; Bizios, R.; Doremus, R.H. Hydroxylapatite with substituted magnesium, zinc, cadmium, and yttrium. I. Structure and microstructure. J. Biomed. Mater. Res. 2002, 59, 305–311. [Google Scholar] [CrossRef]
- Elliott, J.C. The Crystallographic Structure of Dental Enamel and Related Apatites. Ph.D. Thesis, Queen Mary University of London, London, UK, 1964. [Google Scholar]
- Fleet, M.E.; Liu, X.; King, P.L. Accommodation of the carbonate ion in apatite: An FTIR and X-ray structure study of crystals synthesized at 2–4 GPa. Am. Mineral. 2004, 89, 1422–1432. [Google Scholar] [CrossRef]
- Krajewski, A.; Mazzocchi, M.; Buldini, P.L.; Ravaglioli, A.; Tinti, A.; Taddei, P.; Fagnano, C. Synthesis of carbonated hydroxyapatites: Efficiency of the substitution and critical evaluation of analytical methods. J. Mol. Struct. 2005, 744, 221–228. [Google Scholar] [CrossRef]
- Zhang, Q.; Chen, J.; Feng, J.; Cao, Y.; Deng, C.; Zhang, X. Dissolution and mineralization behaviors of HA coatings. Biomaterials 2003, 24, 4741–4748. [Google Scholar] [CrossRef]
- Mehdawi, I.; Neel, E.A.A.; Valappil, S.P.; Palmer, G.; Salih, V.; Pratten, J.; Spratt, D.A.; Young, A.M. Development of remineralizing, antibacterial dental materials. Acta Biomater. 2009, 5, 2525–2539. [Google Scholar] [CrossRef]
- Cacciotti, I. Multisubstituted hydroxyapatite powders and coatings: The influence of the codoping on the hydroxyapatite performances. Int. J. Appl. Ceram. Technol. 2019, 16, 1864–1884. [Google Scholar] [CrossRef]
- Pajor, K.; Pajchel, L.; Kolmas, J. Hydroxyapatite and Fluorapatite in Conservative Dentistry and Oral Implantology-A Review. Materials 2019, 12, 2683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiume, E.; Magnaterra, G.; Rahdar, A.; Verné, E.; Baino, F. Hydroxyapatite for biomedical applications: A short overview. Ceramics 2021, 4, 542–563. [Google Scholar] [CrossRef]
- Jardim, R.N.; Rocha, A.A.; Rossi, A.M.; de Almeida Neves, A.; Portela, M.B.; Lopes, R.T.; Dos Santos, T.M.P.; Xing, Y.; da Silva, E.M. Fabrication and characterization of remineralizing dental composites containing hydroxyapatite nanoparticles. J. Mech. Behav. Biomed. Mater. 2020, 109, 103817. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.S.; Awais, M. Low-cost deposition of antibacterial ion-substituted hydroxyapatite coatings onto 316L stainless steel for biomedical and dental applications. Coatings 2020, 10, 880. [Google Scholar] [CrossRef]
- Kim, H.-M.; Himeno, T.; Kokubo, T.; Nakamura, T. Process and kinetics of bonelike apatite formation on sintered hydroxyapatite in a simulated body fluid. Biomaterials 2005, 26, 4366–4373. [Google Scholar] [CrossRef]
- Kim, B.S.; Jeong, H.Y.; Kim, B.K. Surface characterizations of polyurethanes having different types of soft segment. Colloids Surf. A Physicochem. Eng. Asp. 2005, 268, 60–67. [Google Scholar] [CrossRef]
- Aljabo, A.; Abou Neel, E.A.; Knowles, J.C.; Young, A.M. Development of dental composites with reactive fillers that promote precipitation of antibacterial-hydroxyapatite layers. Mater. Sci. Eng. C 2016, 60, 285–292. [Google Scholar] [CrossRef]
- Khan, A.S.; Aamer, S.; Chaudhry, A.A.; Wong, F.S.L.; Rehman, I.U. Synthesis and characterizations of a fluoride-releasing dental restorative material. Mater. Sci. Eng. C 2013, 33, 3458–3464. [Google Scholar] [CrossRef]
- Ito, A.; Nakamura, S.; Aoki, H.; Akao, M.; Teraoka, K.; Tsutsumi, S.; Onuma, K.; Tateishi, T. Hydrothermal growth of carbonate-containing hydroxyapatite single crystals. J. Cryst. Growth 1996, 163, 311–317. [Google Scholar] [CrossRef]
- Nazir, R.; Samad Khan, A.; Ahmed, A.; Ur-Rehman, A.; Anwar Chaudhry, A.; Ur Rehman, I.; Wong, F.S.L. Synthesis and in-vitro cytotoxicity analysis of microwave irradiated nano-apatites. Ceram. Int. 2013, 39, 4339–4347. [Google Scholar] [CrossRef]
- Oudadesse, H.; Derrien, A.; Mami, M.; Martin, S.; Cathelineau, G.; Yahia, L. Aluminosilicates and biphasic HA-TCP composites: Studies of properties for bony filling. Biomed. Mater. 2007, 2, S59. [Google Scholar] [CrossRef] [PubMed]
- Dorozhkin, S.V. Dissolution mechanism of calcium apatites in acids: A review of literature. World J. Methodol. 2012, 2, 1–17. [Google Scholar] [CrossRef]
- Vogel, M.; Voigt, C.; Gross, U.M.; Müller-Mai, C.M. In vivo comparison of bioactive glass particles in rabbits. Biomaterials 2001, 22, 357–362. [Google Scholar] [CrossRef]
- Gan, S.; Lin, W.; Zou, Y.; Xu, B.; Zhang, X.; Zhao, J.; Rong, J. Nano-hydroxyapatite enhanced double network hydrogels with excellent mechanical properties for potential application in cartilage repair. Carbohydr. Polym. 2020, 229, 115523. [Google Scholar] [CrossRef]
- Chen, H.; Wang, R.; Qian, L.; Liu, H.; Wang, J.; Zhu, M. Surface modification of urchin-like serried hydroxyapatite with sol-gel method and its application in dental composites. Compos. Part B Eng. 2020, 182, 107621. [Google Scholar] [CrossRef]
- Hubadillah, S.K.; Othman, M.H.D.; Tai, Z.S.; Jamalludin, M.R.; Yusuf, N.K.; Ahmad, A.; Rahman, M.A.; Jaafar, J.; Kadir, S.H.S.A.; Harun, Z. Novel hydroxyapatite-based bio-ceramic hollow fiber membrane derived from waste cow bone for textile wastewater treatment. Chem. Eng. J. 2020, 379, 122396. [Google Scholar] [CrossRef]
- Sharan, J.; Singh, S.; Lale, S.V.; Mishra, M.; Koul, V.; Kharbanda, O.P. Applications of nanomaterials in dental science: A review. J. Nanosci. Nanotechnol. 2017, 17, 2235–2255. [Google Scholar] [CrossRef]
- Morgan, M.; Adams, G.; Bailey, D.; Tsao, C.; Fischman, S.; Reynolds, E. The anticariogenic effect of sugar-free gum containing CPP-ACP nanocomplexes on approximal caries determined using digital bitewing radiography. Caries Res. 2008, 42, 171–184. [Google Scholar] [CrossRef]
- Sharma, A.; Rao, A.; Shenoy, R.; Suprabha, B.S. Comparative evaluation of Nano-hydroxyapatite and casein Phosphopeptide-amorphous calcium phosphate on the remineralization potential of early enamel lesions: An in vitro study. J. Orofac. Sci. 2017, 9, 28. [Google Scholar]
- Habraken, W.; Habibovic, P.; Epple, M.; Bohner, M. Calcium phosphates in biomedical applications: Materials for the future? Mater. Today 2016, 19, 69–87. [Google Scholar] [CrossRef]
- Carrodeguas, R.G.; De Aza, A.H.; Turrillas, X.; Pena, P.; De Aza, S. New Approach to the β→ α Polymorphic Transformation in Magnesium-Substituted Tricalcium Phosphate and its Practical Implications. J. Am. Ceram. Soc. 2008, 91, 1281–1286. [Google Scholar] [CrossRef] [Green Version]
- Brunner, T.J. Application of Nanoparticulate Biomaterials for Injectable Bone Cements and Dental Repair. Ph.D. Thesis, ETH Zurich, Zurich, Switzerland, 2007. [Google Scholar]
- Bohner, M. Physical and chemical aspects of calcium phosphates used in spinal surgery. Eur. Spine J. 2001, 10, S114–S121. [Google Scholar] [PubMed] [Green Version]
- Thamaraiselvi, T.; Rajeswari, S. Biological evaluation of bioceramic materials-a review. Carbon 2004, 24, 172. [Google Scholar]
- Fadeeva, I.V.; Deyneko, D.V.; Barbaro, K.; Davydova, G.A.; Sadovnikova, M.A.; Murzakhanov, F.F.; Fomin, A.S.; Yankova, V.G.; Antoniac, I.V.; Barinov, S.M.; et al. Influence of Synthesis Conditions on Gadolinium-Substituted Tricalcium Phosphate Ceramics and Its Physicochemical, Biological, and Antibacterial Properties. Nanomaterials 2022, 12, 852. [Google Scholar] [CrossRef]
- Banerjee, S.S.; Tarafder, S.; Davies, N.M.; Bandyopadhyay, A.; Bose, S. Understanding the influence of MgO and SrO binary doping on the mechanical and biological properties of β-TCP ceramics. Acta Biomater. 2010, 6, 4167–4174. [Google Scholar] [CrossRef]
- Kokubo, T. Bioceramics and Their Clinical Applications; Elsevier: Amsterdam, The Netherlands, 2008. [Google Scholar]
- Samavedi, S.; Whittington, A.R.; Goldstein, A.S. Calcium phosphate ceramics in bone tissue engineering: A review of properties and their influence on cell behavior. Acta Biomater. 2013, 9, 8037–8045. [Google Scholar] [CrossRef]
- Ginebra, M.P. Calcium phosphate bone cements. In Orthopaedic Bone Cements; Woodhead Publishing: Cambridge, UK, 2008; pp. 206–230. [Google Scholar]
- Tsai, H.-C.; Li, Y.-C.; Young, T.-H.; Chen, M.-H. Novel microinjector for carrying bone substitutes for bone regeneration in periodontal diseases. J. Formos. Med. Assoc. 2016, 115, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, K.; Miyaji, H.; Kato, A.; Kosen, Y.; Momose, T.; Yoshida, T.; Nishida, E.; Miyata, S.; Murakami, S.; Takita, H. Periodontal tissue engineering by nano beta-tricalcium phosphate scaffold and fibroblast growth factor-2 in one-wall infrabony defects of dogs. J. Periodontal Res. 2016, 51, 758–767. [Google Scholar] [CrossRef]
- Roca-Millan, E.; Jané-Salas, E.; Marí-Roig, A.; Jiménez-Guerra, Á.; Ortiz-García, I.; Velasco-Ortega, E.; López-López, J.; Monsalve-Guil, L. The Application of Beta-Tricalcium Phosphate in Implant Dentistry: A Systematic Evaluation of Clinical Studies. Materials 2022, 15, 655. [Google Scholar] [CrossRef]
- Nyan, M. Alpha tricalcium phosphate biomaterials for potential clinical application in bone regeneration. Myanmar Dent. J. 2016, 23, 4–9. [Google Scholar]
- Al-Sanabani, J.S.; Madfa, A.A.; Al-Sanabani, F.A. Application of calcium phosphate materials in dentistry. Int. J. Biomater. 2013, 2013, 876132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, R.; Criss, Z.K.; Feller, L.; Modi, S.P.; Hardy, J.G.; Schmidt, C.E.; Suggs, L.J.; Murphy, M.B. Mechanical properties of α-tricalcium phosphate-based bone cements incorporating regenerative biomaterials for filling bone defects exposed to low mechanical loads. J. Biomed. Mater. Res. Part B Appl. Biomater. 2016, 104, 149–157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrodeguas, R.G.; De Aza, S. α-Tricalcium phosphate: Synthesis, properties and biomedical applications. Acta Biomater. 2011, 7, 3536–3546. [Google Scholar] [CrossRef] [PubMed]
- Gunawidjaja, P.N.; Lo, A.Y.; Izquierdo-Barba, I.; García, A.; Arcos, D.; Stevensson, B.; Grins, J.; Vallet-Regi, M.; Edén, M. Biomimetic apatite mineralization mechanisms of mesoporous bioactive glasses as probed by multinuclear 31P, 29Si, 23Na and 13C solid-state NMR. J. Phys. Chem. C 2010, 114, 19345–19356. [Google Scholar] [CrossRef]
- Hench, L.L. The story of Bioglass®. J. Mater. Sci. Mater. Med. 2006, 17, 967–978. [Google Scholar] [CrossRef]
- Hench, L.L. Opening paper 2015–some comments on Bioglass: Four eras of discovery and development. Biomed. Glasses 2015, 1, 1–11. [Google Scholar] [CrossRef]
- Hench, L.L. Chronology of bioactive glass development and clinical applications. New J. Glass Ceram. 2013, 3, 30885. [Google Scholar] [CrossRef] [Green Version]
- Tilocca, A. Structural models of bioactive glasses from molecular dynamics simulations. Proc. R. Soc. A Math. Phys. Eng. Sci. 2009, 465, 1003–1027. [Google Scholar] [CrossRef]
- Hench, L.L.; Jones, J.R. Bioactive glasses: Frontiers and challenges. Front. Bioeng. Biotechnol. 2015, 3, 194. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.T.; Ain, Q.; Chaudhry, A.A.; Khan, A.F.; Iqbal, B.; Ahmad, S.; Siddiqi, S.A.; ur Rehman, I. A study of the effect of precursors on physical and biological properties of mesoporous bioactive glass. J. Mater. Sci. 2015, 50, 1794–1804. [Google Scholar] [CrossRef]
- Gupta, B.; Papke, J.B.; Mohammadkhah, A.; Day, D.E.; Harkins, A.B. Effects of Chemically Doped Bioactive Borate Glass on Neuron Regrowth and Regeneration. Ann. Biomed. Eng. 2016, 44, 3468–3477. [Google Scholar] [CrossRef] [PubMed]
- Ning, J.; Yao, A.; Wang, D.; Huang, W.; Fu, H.; Liu, X.; Jiang, X.; Zhang, X. Synthesis and in vitro bioactivity of a borate-based bioglass. Mater. Lett. 2007, 61, 5223–5226. [Google Scholar] [CrossRef]
- Jayakumar, R.; Menon, D.; Manzoor, K.; Nair, S.; Tamura, H. Biomedical applications of chitin and chitosan based nanomaterials—A short review. Carbohydr. Polym. 2010, 82, 227–232. [Google Scholar] [CrossRef]
- Bauer, J.; Carvalho, E.M.; Carvalho, C.N.; Meier, M.M.; de Souza, J.P.; de Carvalho, R.M.; Loguercio, A.D. Development of a simplified etch-and-rinse adhesive containing niobiophosphate bioactive glass. Int. J. Adhes. Adhes. 2016, 69, 110–114. [Google Scholar] [CrossRef]
- De Caluwé, T.; Vercruysse, C.; Declercq, H.; Schaubroeck, D.; Verbeeck, R.; Martens, L. Bioactivity and biocompatibility of two fluoride containing bioactive glasses for dental applications. Dent. Mater. 2016, 32, 1414–1428. [Google Scholar] [CrossRef]
- Kumar, P.H.; Singh, V.K.; Kumar, P.; Yadav, G.; Chaturvedi, R. Effect of Al 2 O 3 on leucite based bioactive glass ceramic composite for dental veneering. Ceram. Int. 2016, 42, 3591–3597. [Google Scholar] [CrossRef]
- Hyun, H.-K.; Ferracane, J.L. Influence of biofilm formation on the optical properties of novel bioactive glass-containing composites. Dent. Mater. 2016, 32, 1144–1151. [Google Scholar] [CrossRef] [Green Version]
- Silver, I.A.; Deas, J.; Erecińska, M. Interactions of bioactive glasses with osteoblasts in vitro: Effects of 45S5 Bioglass®, and 58S and 77S bioactive glasses on metabolism, intracellular ion concentrations and cell viability. Biomaterials 2001, 22, 175–185. [Google Scholar] [CrossRef]
- Valerio, P.; Pereira, M.M.; Goes, A.M.; Leite, M.F. The effect of ionic products from bioactive glass dissolution on osteoblast proliferation and collagen production. Biomaterials 2004, 25, 2941–2948. [Google Scholar] [CrossRef]
- Bellantone, M.; Coleman, N.J.; Hench, L.L. Bacteriostatic action of a novel four-component bioactive glass. J. Biomed. Mater. Res. Part A 2000, 51, 484–490. [Google Scholar] [CrossRef]
- Wilson, J.; Low, S.B. Bioactive ceramics for periodontal treatment: Comparative studies in the Patus monkey. J. Appl. Biomater. 1992, 3, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Zahid, S.; Shah, A.T.; Jamal, A.; Chaudhry, A.A.; Khan, A.S.; Khan, A.F.; Muhammad, N.; ur Rehman, I. Biological behavior of bioactive glasses and their composites. RSC Adv. 2016, 6, 70197–70214. [Google Scholar] [CrossRef]
- Gorustovich, A.; Rosenbusch, M.; Guglielmotti, M.B. Characterization of bone around titanium implants and bioactive glass particles: An experimental study in rats. Int. J. Oral Maxillofac. Implant. 2002, 17, 644–650. [Google Scholar]
- Kucukkolbasi, H.; Mutlu, N.; Isik, K.; Celik, I.; Oznurlu, Y. Histological evaluation of the effects of bioglass, hydroxyapatite, or demineralized freeze-dried bone, grafted alone or as composites, on the healing of tibial defects in rabbits. Saudi Med. J. 2009, 30, 329–333. [Google Scholar]
- Gasparini Ribeiro, L.L.; Bosco, A.F.; Nagata, M.J.H.; Nascimento de Melo, L.G. Influence of bioactive glass and/or acellular dermal matrix on bone healing of surgically created defects in rat tibiae: A histological and histometric study. Int. J. Oral Maxillofac. Implant. 2008, 23, 811–817. [Google Scholar]
- Newman, S.D.; Lotfibakhshaiesh, N.; O’Donnell, M.; Walboomers, X.F.; Horwood, N.; Jansen, J.A.; Amis, A.A.; Cobb, J.P.; Stevens, M.M. Enhanced osseous implant fixation with strontium-substituted bioactive glass coating. Tissue Eng. Part A 2014, 20, 1850–1857. [Google Scholar] [CrossRef] [PubMed]
- Veis, A.A.; Dabarakis, N.N.; Parisis, N.A.; Tsirlis, A.T.; Karanikola, T.G.; Printza, D.V. Bone regeneration around implants using spherical and granular forms of bioactive glass particles. Implant Dent. 2006, 15, 386–394. [Google Scholar] [CrossRef]
- Yu, H.; Ning, C.; Lin, K.; Chen, L. Preparation and characterization of PLLA/CaSiO3/apatite composite films. Int. J. Appl. Ceram. Technol. 2012, 9, 133–142. [Google Scholar] [CrossRef]
- Rahaman, M.N.; Day, D.E.; Bal, B.S.; Fu, Q.; Jung, S.B.; Bonewald, L.F.; Tomsia, A.P. Bioactive glass in tissue engineering. Acta Biomater. 2011, 7, 2355–2373. [Google Scholar] [CrossRef]
- Wang, G.C.; Lu, Z.F.; Zreiqat, H. 8—Bioceramics for skeletal bone regeneration. In Bone Substitute Biomaterials; Mallick, K., Ed.; Woodhead Publishing: Cambridge, UK, 2014; pp. 180–216. [Google Scholar]
- Siriphannon, P.; Hayashi, S.; Yasumori, A.; Okada, K. Preparation and sintering of CaSiO 3 from coprecipitated powder using NaOH as precipitant and its apatite formation in simulated body fluid solution. J. Mater. Res. 1999, 14, 529–536. [Google Scholar] [CrossRef]
- Mobasherpour, I.; Hashjin, M.S.; Toosi, S.R.; Kamachali, R.D. Effect of the addition ZrO 2–Al 2 O 3 on nanocrystalline hydroxyapatite bending strength and fracture toughness. Ceram. Int. 2009, 35, 1569–1574. [Google Scholar] [CrossRef]
- Chen, C.-C.; Ho, C.-C.; Chen, C.-H.D.; Ding, S.-J. Physicochemical properties of calcium silicate cements for endodontic treatment. J. Endod. 2009, 35, 1288–1291. [Google Scholar] [CrossRef] [PubMed]
- Ilić, D.V.; Antonijević, Đ.; Biočanin, V.; Čolović, B.M.; Danilović, V.; Komlev, V.; Teterina, A.; Jokanović, V.R. Physico-chemical and biological properties of dental calcium silicate cements-literature review. Hem. Ind. 2019, 73, 281–294. [Google Scholar] [CrossRef]
- Sanz, J.L.; Guerrero-Gironés, J.; Pecci-Lloret, M.P.; Pecci-Lloret, M.R.; Melo, M. Biological interactions between calcium silicate-based endodontic biomaterials and periodontal ligament stem cells: A systematic review of in vitro studies. Int. Endod. J. 2021, 54, 2025–2043. [Google Scholar] [CrossRef]
- Srikar, P.; Sathish, T.; Khan, P.I.; Reddy, Y.K.; Kondaiah, V.V.; Rao, M.A.; Dumpala, R.; Sunil, B.R. Zinc-calcium silicate composites produced by ball milling and sintering for degradable implant applications. Mater. Today Proc. 2021, 44, 1584–1588. [Google Scholar] [CrossRef]
- Yoo, K.-H.; Kim, Y.-I.; Yoon, S.-Y. Physicochemical and Biological Properties of Mg-Doped Calcium Silicate Endodontic Cement. Materials 2021, 14, 1843. [Google Scholar] [CrossRef]
- Zafar, K.; Jamal, S.; Ghafoor, R. Bio-active cements-Mineral Trioxide Aggregate based calcium silicate materials: A narrative review. JPMA J. Pak. Med. Assoc. 2020, 70, 497. [Google Scholar] [CrossRef]
- Primus, C.M.; Tay, F.R.; Niu, L.-n. Bioactive tri/dicalcium silicate cements for treatment of pulpal and periapical tissues. Acta Biomater. 2019, 96, 35–54. [Google Scholar] [CrossRef]
- Chitra, S.; Mathew, N.K.; Jayalakshmi, S.; Balakumar, S.; Rajeshkumar, S.; Ramya, R. Strategies of Bioceramics, Bioactive Glasses in Endodontics: Future Perspectives of Restorative Dentistry. BioMed. Res. Int. 2022, 2530156. [CrossRef]
- Cui, W.; Cao, L.; Zhang, X. Bioceramics: Materials, properties, and applications. Elsevier: 2022; pp. 65-110. In Ceramic Science and Engineering; Elsevier: Amsterdam, The Netherlands, 2022; pp. 65–110. [Google Scholar]
- Frencken, J.E.; Peters, M.C.; Manton, D.J.; Leal, S.C.; Gordan, V.V.; Eden, E. Minimal Intervention Dentistry (MID) for managing dental caries—A review: Report of a FDI task group. Int. Dent. J. 2012, 62, 223–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrtic, D.; Antonucci, J.; Eanes, E. Amorphous Calcium Phosphate-Based Bioactive Polymeric Composites for Mineralised Tissue Regeneration. J. Res. Nat. Inst. Stand. Technol. 2003, 108, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Swami, V.; Sable, R. Comparative Study of Amorphous Calcium Phosphate-containing Orthodontic Composite and Conventional Orthodontic Adhesive on Enamel Demineralization around Orthodontic Brackets–An in vivo Study. Orthod. J. Nepal 2014, 3, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Melo, M.; Weir, M.; Passos, V.; Powers, M.; Xu, H. pH-activatable nano-amorphous calcium phosphate to reduce dental enamel demineralization. Dent. Mater. 2016, 32, e64. [Google Scholar] [CrossRef]
- Chow, C.K.W.; Wu, C.D.; Evans, C.A. In vitro properties of orthodontic adhesives with fluoride or amorphous calcium phosphate. Int. J. Dent. 2011, 2011, 583521. [Google Scholar] [CrossRef] [Green Version]
- Zero, D.T. Recaldent™—Evidence for clinical activity. Adv. Dent. Res. 2009, 21, 30–34. [Google Scholar] [CrossRef]
- Minick, G.T.; Oesterle, L.J.; Newman, S.M.; Shellhart, W.C. Bracket bond strengths of new adhesive systems. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 771–776. [Google Scholar] [CrossRef]
- Choudhary, P.K.; Tandon, S.; Ganesh, M.R.; Mehra, A. Evaluation of the remineralization potential of amorphous calcium phosphate and fluoride containing pit and fissure sealants using scanning electron microscopy. Indian J. Dent. Res. Off. Publ. Indian Soc. Dent. Res. 2012, 23, 157–163. [Google Scholar] [CrossRef]
- Kumar, V.; Itthagarun, A.; King, N. The effect of casein phosphopeptide-amorphous calcium phosphate on remineralization of artificial caries-like lesions: An in vitro study. Aust. Dent. J. 2008, 53, 34–40. [Google Scholar] [CrossRef]
- Antonucci, J.; O’Donnell, J.; Schumacher, G.; Skrtic, D. Amorphous calcium phosphate composites and their effect on composite–adhesive–dentin bonding. J. Adhes. Sci. Technol. 2009, 23, 1133–1147. [Google Scholar] [CrossRef]
- Skrtic, D.; Antonucci, J.; Eanes, E.; Eidelman, N. Dental composites based on hybrid and surface-modified amorphous calcium phosphates. Biomaterials 2004, 25, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Marovic, D.; Tarle, Z.; Hiller, K.A.; Müller, R.; Ristic, M.; Rosentritt, M.; Skrtic, D.; Schmalz, G. Effect of silanized nanosilica addition on remineralizing and mechanical properties of experimental composite materials with amorphous calcium phosphate. Clin. Oral Investig. 2014, 18, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Skrtic, D.; Antonucci, J.M. Dental Composites: Bioactive Polymeric Amorphous Calcium Phosphate-Based. Encycl. Biomed. Polym. Polym. Biomater. 2015, 2015, 2443–2462. [Google Scholar]
- Zhao, J.; Liu, Y.; Sun, W.-b.; Zhang, H. Amorphous calcium phosphate and its application in dentistry. Chem. Cent. J. 2011, 5, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, H. Dental Composites Comprising Nanoparticles of Amorphous Calcium Phosphate. U.S. Patent No 8,889,196, 18 November 2014. [Google Scholar]
- Zhang, L.; Weir, M.D.; Chow, L.C.; Antonucci, J.M.; Chen, J.; Xu, H.H.K. Novel rechargeable calcium phosphate dental nanocomposite. Dent. Mater. 2016, 32, 285–293. [Google Scholar] [CrossRef] [Green Version]
- Park, M.; Eanes, E.; Antonucci, J.; Skrtic, D. Mechanical properties of bioactive amorphous calcium phosphate/methacrylate composites. Dent. Mater. 1998, 14, 137–141. [Google Scholar] [CrossRef]
- Okazaki, M.; Ohmae, H. Mechanical and biological properties of apatite composite resins. Biomaterials 1988, 9, 345–348. [Google Scholar] [CrossRef]
- Santos, C.; Luklinska, Z.B.; Clarke, R.L.; Davy, K.W. Hydroxyapatite as a filler for dental composite materials: Mechanical properties and in vitro bioactivity of composites. J. Mater. Sci. Mater. Med. 2001, 12, 565–573. [Google Scholar] [CrossRef]
- Arcís, R.W.; López-Macipe, A.; Toledano, M.; Osorio, E.; Rodríguez-Clemente, R.; Murtra, J.; Fanovich, M.A.; Pascual, C.D. Mechanical properties of visible light-cured resins reinforced with hydroxyapatite for dental restoration. Dent. Mater. 2002, 18, 49–57. [Google Scholar] [CrossRef]
- Domingo, C.; Arcis, R.W.; Lopez-Macipe, A.; Osorio, R.; Rodriguez-Clemente, R.; Murtra, J.; Fanovich, M.A.; Toledano, M. Dental composites reinforced with hydroxyapatite: Mechanical behavior and absorption/elution characteristics. J. Biomed. Mater. Res. 2001, 56, 297–305. [Google Scholar] [CrossRef]
- Domingo, C.; Arcís, R.W.; Osorio, E.; Osorio, R.; Fanovich, M.A.; Rodríguez-Clemente, R.; Toledano, M. Hydrolytic stability of experimental hydroxyapatite-filled dental composite materials. Dent. Mater. 2003, 19, 478–486. [Google Scholar] [CrossRef]
- Lung, C.Y.K.; Sarfraz, Z.; Habib, A.; Khan, A.S.; Matinlinna, J.P. Effect of silanization of hydroxyapatite fillers on physical and mechanical properties of a bis-GMA based resin composite. J. Mech. Behav. Biomed. Mater. 2016, 54, 283–294. [Google Scholar] [CrossRef]
- Uygunoglu, T.; Gunes, I.; Brostow, W. Physical and Mechanical Properties of Polymer Composites with High Content of Wastes Including Boron. Mater. Res. 2015, 18, 1188–1196. [Google Scholar] [CrossRef] [Green Version]
- Cramer, N.B.; Stansbury, J.W.; Bowman, C.N. Recent Advances and Developments in Composite Dental Restorative Materials. J. Dent. Res. 2011, 90, 402–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadat-Shojai, M.; Atai, M.; Nodehi, A.; Khanlar, L.N. Hydroxyapatite nanorods as novel fillers for improving the properties of dental adhesives: Synthesis and application. Dent. Mater. 2010, 26, 471–482. [Google Scholar] [CrossRef]
- Sadat-Shojai, M.; Atai, M.; Nodehi, A. Method for Production of Biocompatible Nanoparticles Containing Dental Adhesive. U.S. Patent No 8,357,732, 22 January 2013. [Google Scholar]
- Chen, L.; Yu, Q.; Wang, Y.; Li, H. BisGMA/TEGDMA dental composite containing high aspect-ratio hydroxyapatite nanofibers. Dent. Mater. 2011, 27, 1187–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Darvell, B.W. Mechanical properties of hydroxyapatite whisker-reinforced bis-GMA-based resin composites. Dent. Mater. 2012, 28, 824–830. [Google Scholar] [CrossRef]
- Calabrese, L.; Fabiano, F.; Currò, M.; Borsellino, C.; Bonaccorsi, L.; Fabiano, V.; Ientile, R.; Proverbio, E. Hydroxyapatite Whiskers Based Resin Composite versus Commercial Dental Composites: Mechanical and Biocompatibility Characterization. Adv. Mater. Sci. Eng. 2016, 2016, 2172365. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, Y. The effect of hydroxyapatite presence on the degree of conversion and polymerization rate in a model self-etching adhesive. Dent. Mater. 2012, 28, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, Y. Hydroxyapatite Effect on Photopolymerization of Self-etching Adhesives with Different Aggressiveness. J. Dent. 2012, 40, 564–570. [Google Scholar] [CrossRef] [Green Version]
- Khalid, H.; Syed, M.; Iqbal, H.; Rehman, I.; Khan, A. Monomer leaching and degree of conversion of bioactive dental composites. Dent. Mater. 2016, 32, e61–e62. [Google Scholar] [CrossRef]
- Khan, A.S.; Hassan, K.R.; Bukhari, S.F.; Wong, F.S.; Rehman, I.U. Structural and in vitro adhesion analysis of a novel covalently coupled bioactive composite. J. Biomed. Mater. Res. Part B Appl. Biomater. 2012, 100, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.; Wong, F.; McKay, I.; Whiley, R.; Rehman, I. Structural, mechanical, and biocompatibility analyses of a novel dental restorative nanocomposite. J. Appl. Polym. Sci. 2013, 127, 439–447. [Google Scholar] [CrossRef]
- Khan, A.; Sidra, L.; Sarfraz, Z.; Mustafa, W. Synthesis of electrospun bioactive carbon nanotube based dental resin-based composites. Dent. Mater. 2015, 31, e45–e46. [Google Scholar] [CrossRef]
- Pagano, S.; Lombardo, G.; Costanzi, E.; Balloni, S.; Bruscoli, S.; Flamini, S.; Coniglio, M.; Valenti, C.; Cianetti, S.; Marinucci, L. Morpho-functional effects of different universal dental adhesives on human gingival fibroblasts: An in vitro study. Odontology 2021, 109, 524–539. [Google Scholar] [CrossRef]
- Murray, P.E.; García Godoy, C.; García Godoy, F. How is the biocompatibilty of dental biomaterials evaluated? Med. Oral Patol. Oral Cirugía Bucal 2007, 12, 258–266. [Google Scholar]
- Shahi, S.; Özcan, M.; Maleki Dizaj, S.; Sharifi, S.; Al-Haj Husain, N.; Eftekhari, A.; Ahmadian, E. A review on potential toxicity of dental material and screening their biocompatibility. Toxicol. Mech. Methods 2019, 29, 368–377. [Google Scholar] [CrossRef]
- Hofmann, M.P.; Young, A.M.; Gbureck, U.; Nazhat, S.N.; Barralet, J.E. FTIR-monitoring of a fast setting brushite bone cement: Effect of intermediate phases. J. Mater. Chem. 2006, 16, 3199–3206. [Google Scholar] [CrossRef]
- Aljabo, A.; Xia, W.; Liaqat, S.; Khan, M.A.; Knowles, J.C.; Ashley, P.; Young, A.M. Conversion, shrinkage, water sorption, flexural strength and modulus of re-mineralizing dental composites. Dent. Mater. 2015, 31, 1279–1289. [Google Scholar] [CrossRef] [Green Version]
- Panpisut, P.; Liaqat, S.; Zacharaki, E.; Xia, W.; Petridis, H.; Young, A.M. Dental Composites with Calcium/Strontium Phosphates and Polylysine. PLoS ONE 2016, 11, e0164653. [Google Scholar] [CrossRef] [Green Version]
- Kessler, S.; Lee, S. Use of Bioactive Glass in Dental Filling Material. U.S. Patent No 7,090,720, 6 March 2013. [Google Scholar]
- Choi, J.-Y.; Lee, H.-H.; Kim, H.-W. Bioactive sol–gel glass added ionomer cement for the regeneration of tooth structure. J. Mater. Sci. Mater. Med. 2008, 19, 3287–3294. [Google Scholar] [CrossRef] [PubMed]
- Schulze, K.A.; Oliveira, S.A.; Wilson, R.S.; Gansky, S.A.; Marshall, G.W.; Marshall, S.J. Effect of hydration variability on hybrid layer properties of a self-etching versus an acid-etching system. Biomaterials 2005, 26, 1011–1018. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-J.; Jang, J.-H.; Woo, S.U.; Choi, K.-K.; Kim, S.-Y.; Ferracane, J.L.; Lee, J.-H.; Choi, D.; Choi, S.; Kim, S. Effect of novel bioactive glass-containing dentin adhesive on the permeability of demineralized dentin. Materials 2021, 14, 5423. [Google Scholar] [CrossRef] [PubMed]
- Tezvergil-Mutluay, A.; Seseogullari-Dirihan, R.; Feitosa, V.P.; Cama, G.; Brauer, D.S.; Sauro, S. Effects of Composites Containing Bioactive Glasses on Demineralized Dentin. J. Dent. Res. 2017, 96, 999–1005. [Google Scholar] [CrossRef] [PubMed]
- Sauro, S.; Osorio, R.; Watson, T.F.; Toledano, M. Therapeutic effects of novel resin bonding systems containing bioactive glasses on mineral-depleted areas within the bonded-dentine interface. J. Mater. Sci. Mater. Med. 2012, 23, 1521–1532. [Google Scholar] [CrossRef] [PubMed]
- Profeta, A.C.; Mannocci, F.; Foxton, R.M.; Thompson, I.; Watson, T.F.; Sauro, S. Bioactive effects of a calcium/sodium phosphosilicate on the resin–dentine interface: A microtensile bond strength, scanning electron microscopy, and confocal microscopy study. Eur. J. Oral Sci. 2012, 120, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Sauro, S.; Watson, T.F.; Thompson, I.; Banerjee, A. One-bottle self-etching adhesives applied to dentine air-abraded using bioactive glasses containing polyacrylic acid: An in vitro microtensile bond strength and confocal microscopy study. J. Dent. 2012, 40, 896–905. [Google Scholar] [CrossRef]
- Sauro, S.; Watson, T.F.; Thompson, I.; Toledano, M.; Nucci, C.; Banerjee, A. Influence of air-abrasion executed with polyacrylic acid-Bioglass 45S5 on the bonding performance of a resin-modified glass ionomer cement. Eur. J. Oral Sci. 2012, 120, 168–177. [Google Scholar] [CrossRef]
- Khvostenko, D.; Mitchell, J.; Hilton, T.; Ferracane, J.; Kruzic, J. Mechanical performance of novel bioactive glass containing dental restorative composites. Dent. Mater. 2013, 29, 1139–1148. [Google Scholar] [CrossRef] [Green Version]
- Malkondu, Ö.; Kazandağ, M.K.; Kazazoğlu, E. A Review on Biodentine, a Contemporary Dentine Replacement and Repair Material. BioMed Res. Int. 2014, 2014, 160951. [Google Scholar] [CrossRef] [Green Version]
- Gopikrishna, V. Preclinical Manual of Conservative Dentistry and Endodontics E-Book. Elsevier: New Delhi, India, 2019. [Google Scholar]
- Cannon, M.; Gerodias, N.; Vieira, A.; Percinoto, C.; Jurado, R. Primate pulpal healing after exposure and TheraCal application. J. Clin. Pediatric Dent. 2014, 38, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Deepa, V.L.; Dhamaraju, B.; Bollu, I.P.; Balaji, T.S. Shear bond strength evaluation of resin composite bonded to three different liners: TheraCal LC, Biodentine, and resin-modified glass ionomer cement using universal adhesive: An in vitro study. J. Conserv. Dent. JCD 2016, 19, 166–170. [Google Scholar] [CrossRef] [PubMed]
- Midentistry. Activa BioACTIVE. Dent. Mater. Device Regist. 2021, 5, 43–46. [Google Scholar]
- Croll, T.P.; Berg, J.H.; Donly, K.J. Dental repair material: A resin-modified glass ionomer bioactive ionic resin-based composite. Compend. Cont. Educ. Dent. 2015, 36, 602–607. [Google Scholar]
- Abdel-Maksoud, H.B.; Bahanan, A.W.; Alkhattabi, L.J.; Bakhsh, T.A. Evaluation of Newly Introduced Bioactive Materials in Terms of Cavity Floor Adaptation: OCT Study. Materials 2021, 14, 7668. [Google Scholar] [CrossRef]
- Pameijer, C.H.; Garcia-Godoy, F.; Morrow, B.R.; Jefferies, S.R. Flexural strength and flexural fatigue properties of resin-modified glass ionomers. J. Clin. Dent. 2015, 26, 23–27. [Google Scholar]
- Zmener, O.; Pameijer, C.H.; Hernandez, S. Resistance against bacterial leakage of four luting agents used for cementation of complete cast crowns. Am. J. Dent. 2014, 27, 51–55. [Google Scholar]
- Slowikowski, L.; John, S.; Finkleman, M.; Perry, R.; Harsono, M.; Kugel, G. Fluoride ion release and recharge over time in three restoratives. J. Dent. Res. 2014, 93, 268. [Google Scholar]
- Bansal, R.; Burgess, J.; Lawson, N.C. Wear of an enhanced resin-modified glass-ionomer restorative material. Am. J. Dent. 2016, 29, 171–174. [Google Scholar]
- Berg, J.H.; Croll, T.P. Glass ionomer restorative cement systems: An update. Pediatric Dent. 2015, 37, 116–124. [Google Scholar]
- Jun, S.-K.; Lee, J.-H.; Lee, H.-H. The biomineralization of a bioactive glass-incorporated light-curable pulp capping material using human dental pulp stem cells. BioMed Res. Int. 2017, 2017, 2495282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lardani, L.; Derchi, G.; Marchio, V.; Carli, E. One-Year Clinical Performance of Activa™ Bioactive-Restorative Composite in Primary Molars. Children 2022, 9, 433. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lozano, F.J.; Collado-González, M.; Tomás-Catalá, C.J.; García-Bernal, D.; López, S.; Oñate-Sánchez, R.E.; Moraleda, J.M.; Murcia, L. GuttaFlow Bioseal promotes spontaneous differentiation of human periodontal ligament stem cells into cementoblast-like cells. Dent. Mater. 2019, 35, 114–124. [Google Scholar] [CrossRef]
- Benrashed, M.A.; Alyousef, N.I.; AlQahtani, N.H.; AlMaimouni, Y.K.; Khan, M.; Khan, A.S. Conventional to advanced endodontics: Use of bioactive materials. In Biomaterials in Endodontics; Elsevier: Amsterdam, The Netherlands, 2022; pp. 169–194. [Google Scholar]
- Baras, B.H.; Wang, S.; Melo, M.A.S.; Tay, F.; Fouad, A.F.; Arola, D.D.; Weir, M.D.; Xu, H.H.K. Novel bioactive root canal sealer with antibiofilm and remineralization properties. J. Dent. 2019, 83, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Almaimouni, Y.K.; Hamid, S.K.; Ilyas, K.; Shah, A.T.; Majeed, A.; Khan, A.S. Structural, fluoride release, and 3D interfacial adhesion analysis of bioactive endodontic sealers. Dent. Mater. J. 2020, 39, 483–489. [Google Scholar] [CrossRef] [Green Version]
- Washio, A.; Miura, H.; Morotomi, T.; Ichimaru-Suematsu, M.; Miyahara, H.; Hanada-Miyahara, K.; Yoshii, S.; Murata, K.; Takakura, N.; Akao, E. Effect of bioactive glass-based root canal sealer on the incidence of postoperative pain after root canal obturation. Int. J. Environ. Res. Public Health 2020, 17, 8857. [Google Scholar] [CrossRef]
- Hegde, S.; Sowmya, B.; Mathew, S.; Bhandi, S.; Nagaraja, S.; Dinesh, K. Clinical evaluation of mineral trioxide aggregate and biodentine as direct pulp capping agents in carious teeth. J. Conserv. Dent. 2017, 20, 91–95. [Google Scholar] [CrossRef]
- Gandolfi, M.; Taddei, P.; Tinti, A.; Prati, C. Apatite-forming ability (bioactivity) of ProRoot MTA. Int. Endod. J. 2010, 43, 917–929. [Google Scholar] [CrossRef]
- Chau, J.Y.; Hutter, J.W.; Mork, T.O.; Nicoll, B.K. An in vitro study of furcation perforation repair using calcium phosphate cement. J. Endod. 1997, 23, 588–592. [Google Scholar] [CrossRef]
- Lee, S.-J.; Monsef, M.; Torabinejad, M. Sealing ability of a mineral trioxide aggregate for repair of lateral root perforations. J. Endod. 1993, 19, 541–544. [Google Scholar] [CrossRef]
- Guneser, M.B.; Akbulut, M.B.; Eldeniz, A.U. Effect of various endodontic irrigants on the push-out bond strength of biodentine and conventional root perforation repair materials. J. Endod. 2013, 39, 380–384. [Google Scholar] [CrossRef]
- Kakani, A.K.; Veeramachaneni, C.; Majeti, C.; Tummala, M.; Khiyani, L. A review on perforation repair materials. J. Clin. Diagn. Res. JCDR 2015, 9, ZE09. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M.; Dummer, P. Mineral trioxide aggregate and other bioactive endodontic cements: An updated overview—Part I: Vital pulp therapy. Int. Endod. J. 2018, 51, 177–205. [Google Scholar] [CrossRef] [PubMed]
- Guagnano, R.; Romano, F.; Defabianis, P. Evaluation of Biodentine in Pulpotomies of Primary Teeth with Different Stages of Root Resorption Using a Novel Composite Outcome Score. Materials 2021, 14, 2179. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Hughes, F.; Ghuman, M.; Talal, A. Periodontal regeneration: A challenge for the tissue engineer? Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2010, 224, 1345–1358. [Google Scholar] [CrossRef]
- Sumer, M.; Keles, G.C.; Cetinkaya, B.O.; Balli, U.; Pamuk, F.; Uckan, S. Autogenous cortical bone and bioactive glass grafting for treatment of intraosseous periodontal defects. Eur. J. Dent. 2013, 7, 6–14. [Google Scholar]
- Keles, G.C.; Sumer, M.; Cetinkaya, B.O.; Tutkun, F.; Simsek, S.B. Effect of Autogenous Cortical Bone Grafting in Conjunction with Guided Tissue Regeneration in the Treatment of Intraosseous Periodontal Defects. Eur. J. Dent. 2010, 4, 403–411. [Google Scholar] [CrossRef] [Green Version]
- Froum, S.J.; Wallace, S.S.; Tarnow, D.P.; Cho, S.-C. Effect of platelet-rich plasma on bone growth and osseointegration in human maxillary sinus grafts: Three bilateral case reports. Int. J. Periodontics Restor. Dent. 2002, 22, 45–54. [Google Scholar]
- Chacko, N.L.; Abraham, S.; Rao, H.N.; Sridhar, N.; Moon, N.; Barde, D.H. A Clinical and Radiographic Evaluation of Periodontal Regenerative Potential of PerioGlas(R): A Synthetic, Resorbable Material in Treating Periodontal Infrabony Defects. J. Int. Oral Health 2014, 6, 20–26. [Google Scholar]
- Villar, C.C.; Cochran, D.L. Regeneration of Periodontal Tissues: Guided Tissue Regeneration. Dent. Clin. N. Am. 2010, 54, 73–92. [Google Scholar] [CrossRef] [PubMed]
- Nery, E.; Lynch, K.; Hirthe, W.; Mueller, K. Bioceramic implants in surgically produced infrabony defects. J. Periodontol. 1975, 46, 328–347. [Google Scholar] [CrossRef] [PubMed]
- Nery, E.B.; Lynch, K.L.; Rooney, G.E. Alveolar ridge augmentation with tricalcium phosphate ceramic. J. Prosthet. Dent. 1978, 40, 668–675. [Google Scholar] [CrossRef]
- Denissen, H.W.; de Groot, K. Immediate dental root implants from synthetic dense calcium hydroxylapatite. J. Prosthet. Dent. 1979, 42, 551–556. [Google Scholar] [CrossRef]
- Reynolds, M.A.; Aichelmann-Reidy, M.E.; Branch-Mays, G.L. Regeneration of periodontal tissue: Bone replacement grafts. Dent. Clin. N. Am. 2010, 54, 55–71. [Google Scholar] [CrossRef]
- Hench, L.L.; Thompson, I. Twenty-first century challenges for biomaterials. J. R. Soc. Interface 2010, 7, S379–S391. [Google Scholar] [CrossRef] [Green Version]
- Froum, S.; Cho, S.-C.; Rosenberg, E.; Rohrer, M.; Tarnow, D. Histological comparison of healing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: A pilot study. J. Periodontol. 2002, 73, 94–102. [Google Scholar] [CrossRef]
- Kaur, G.; Pandey, O.P.; Singh, K.; Homa, D.; Scott, B.; Pickrell, G. A review of bioactive glasses: Their structure, properties, fabrication and apatite formation. J. Biomed. Mater. Res. Part A 2014, 102, 254–274. [Google Scholar] [CrossRef]
- Hum, J.; Boccaccini, A.R. Bioactive glasses as carriers for bioactive molecules and therapeutic drugs: A review. J. Mater. Sci. Mater. Med. 2012, 23, 2317–2333. [Google Scholar] [CrossRef]
- Cannillo, V.; Salvatori, R.; Bergamini, S.; Bellucci, D.; Bertoldi, C. Bioactive Glasses in Periodontal Regeneration: Existing Strategies and Future Prospects—A Literature Review. Materials 2022, 15, 2194. [Google Scholar] [CrossRef]
- Sunandhakumari, V.J.; Vidhyadharan, A.K.; Alim, A.; Kumar, D.; Ravindran, J.; Krishna, A.; Prasad, M. Fabrication and in vitro characterization of bioactive glass/nano hydroxyapatite reinforced electrospun poly (ε-caprolactone) composite membranes for guided tissue regeneration. Bioengineering 2018, 5, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
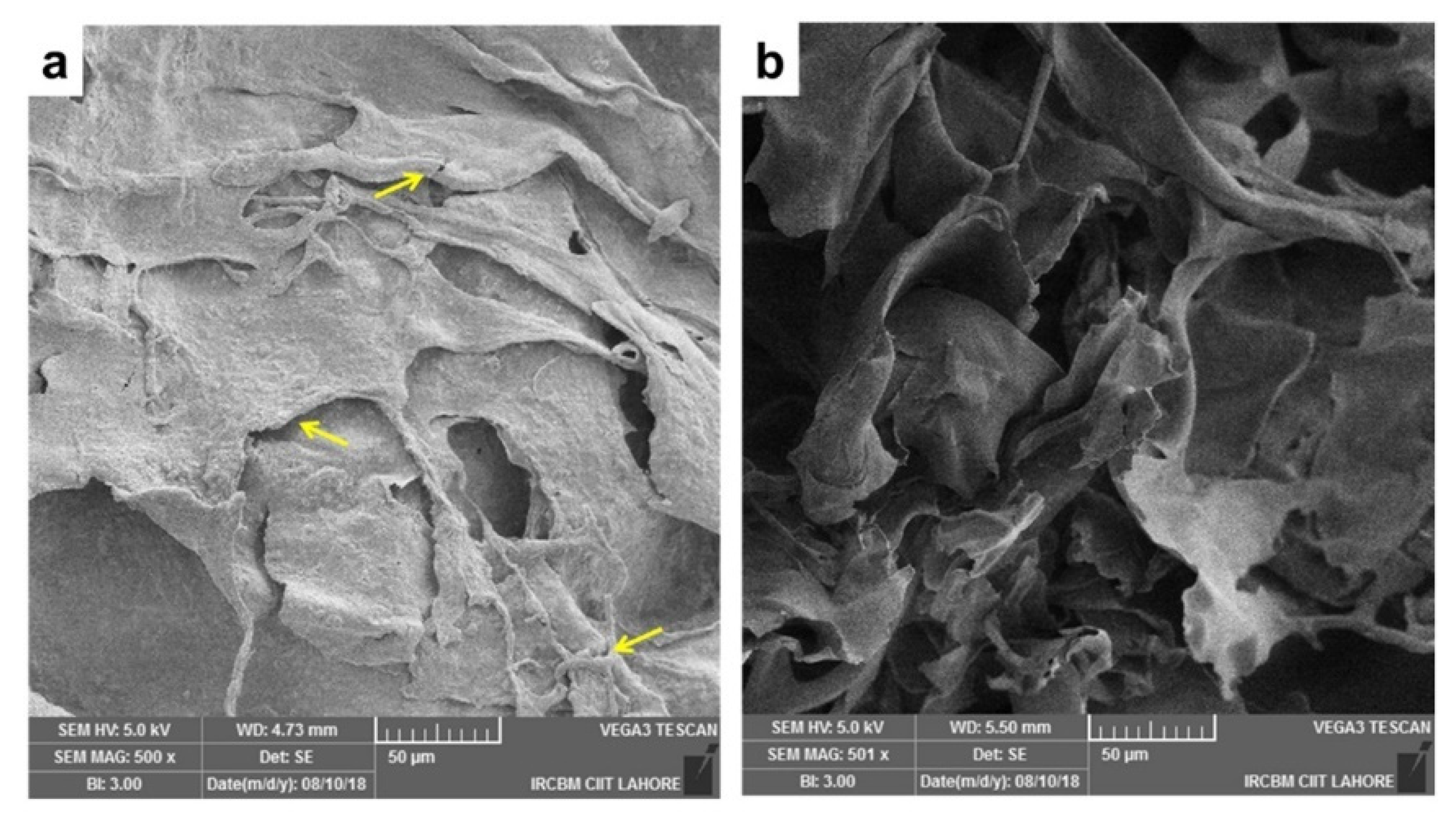
- Zahid, S.; Khan, A.S.; Chaudhry, A.A.; Ghafoor, S.; Ain, Q.U.; Raza, A.; Rahim, M.I.; Goerke, O.; Rehman, I.U.; Tufail, A. Fabrication, in vitro and in vivo studies of bilayer composite membrane for periodontal guided tissue regeneration. J. Biomater. Appl. 2019, 33, 967–978. [Google Scholar] [CrossRef] [PubMed]
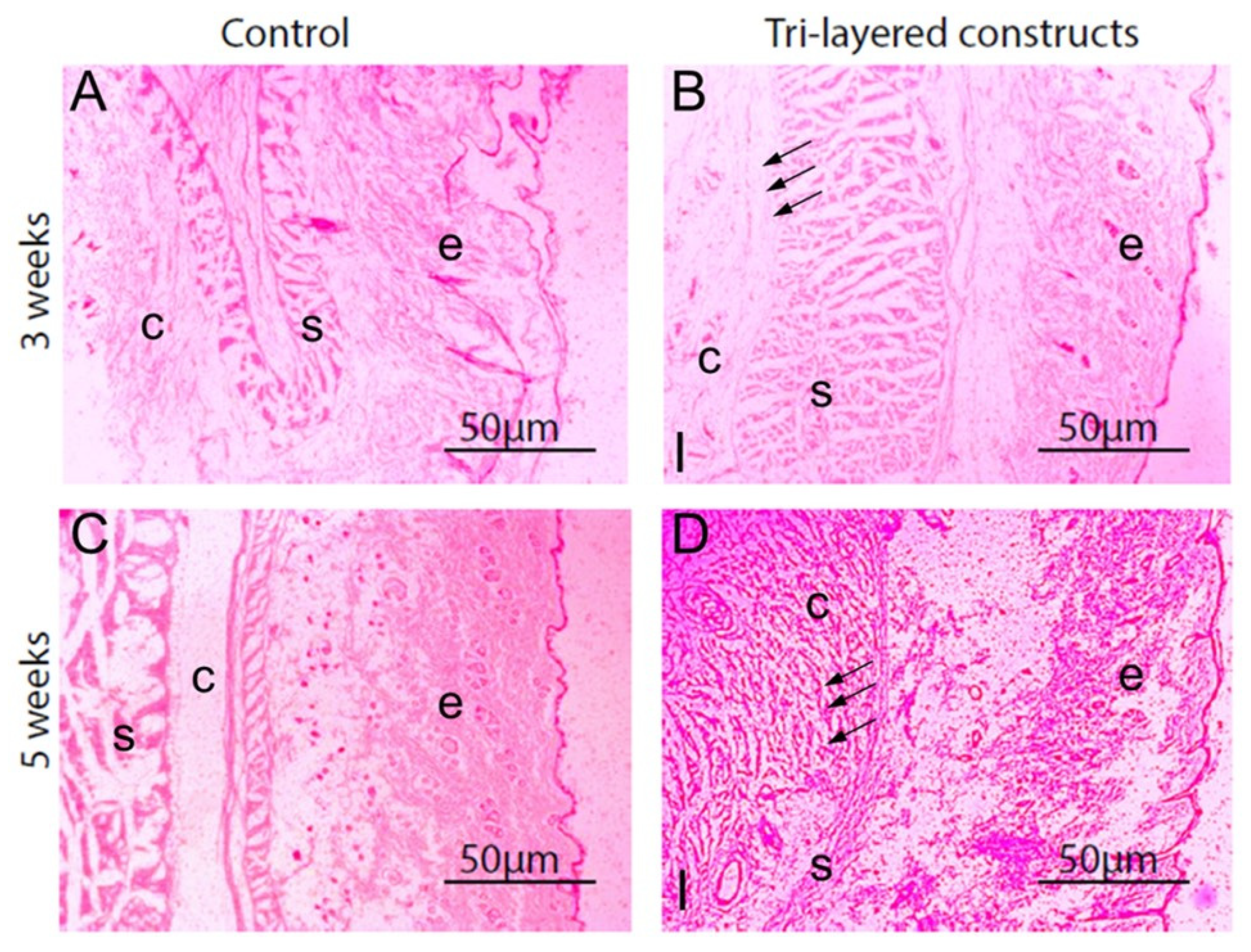
- Shah, A.T.; Zahid, S.; Ikram, F.; Maqbool, M.; Chaudhry, A.A.; Rahim, M.I.; Schmidt, F.; Goerke, O.; Khan, A.S.; ur Rehman, I. Tri-layered functionally graded membrane for potential application in periodontal regeneration. Mater. Sci. Eng. C 2019, 103, 109812. [Google Scholar] [CrossRef] [PubMed]
- Macedo, N.L.d.; Matuda, F.d.S.; Macedo, L.G.S.d.; Gonzales, M.B.; Ouchi, S.M.; Carvalho, Y.R. Bone defect regeneration with bioactive glass implantation in rats. J. Appl. Oral Sci. 2004, 12, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Vega-Ruiz, B.; Ramos-Zúñiga, R.; Duran, I.S.; Ursiel-Ortega, Y. Biomaterials and surgical applications: The translational perspective. Transl. Surg. 2017, 2, 85. [Google Scholar]
- García, D.; García, L.; Pérez, M.; Suarez, M.; Delgado, J.; García, R.; Rodríguez, Y.; Fernández, I.; Márquez, D. Filling of Post-Extraction Dental Socket with Hydroxyapatite Granules APAFILL-G TM. Key Eng. Mater. 2001, 192–195, 925–928. [Google Scholar] [CrossRef]
- Opris, H.; Bran, S.; Dinu, C.; Baciut, M.; Prodan, D.A.; Mester, A.; Baciut, G. Clinical applications of avian eggshell-derived hydroxyapatite. Bosn. J. Basic Med. Sci. 2020, 20, 430. [Google Scholar] [CrossRef]
- Maria, N.L.; Andreea-Simona, B.-P.; Mihai, H.R.; Mona, K.; Elena, C.L. Comparison of Three Calcium Silicate Cements Used as Retrograde Filling Materials. An In Vitro Study. Res. Clin. Med. 2020, 4, 32–36. [Google Scholar]
- Franceschini, F.; Oliveira, R.d.S.; Lopes, A.P.A.; Silva, C.E.X.d.S.R.d. Evaluation of Bone Repair in the Mandible of Rabbits Using Biphasic Calcium Phosphate Micro-Macroporous Hydroxyapatite Bioceramics and Beta-Tricalcium Phosphate. Pesqui. Bras. Em Odontopediatria Clínica Integr. 2019, 19. [Google Scholar] [CrossRef]
- Resende, R.F.B.; Sartoretto, S.C.; Uzeda, M.J.; Alves, A.T.N.N.; Calasans-Maia, J.A.; Rossi, A.M.; Granjeiro, J.M.; Calasans-Maia, M.D. Randomized Controlled Clinical Trial of Nanostructured Carbonated Hydroxyapatite for Alveolar Bone Repair. Materials 2019, 12, 3645. [Google Scholar] [CrossRef] [Green Version]
- Cannio, M.; Bellucci, D.; Roether, J.A.; Boccaccini, D.; Cannillo, V. Bioactive Glass Applications: A Literature Review of Human Clinical Trials. Materials 2021, 14, 5440. [Google Scholar] [CrossRef] [PubMed]
- Profeta, A.C.; Huppa, C. Bioactive-glass in Oral and Maxillofacial Surgery. Craniomaxillofac Trauma Reconstr 2016, 9, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinnunen, I.; Aitasalo, K.; Pöllönen, M.; Varpula, M. Reconstruction of orbital floor fractures using bioactive glass. J. Cranio-Maxillofac. Surg. 2000, 28, 229–234. [Google Scholar] [CrossRef]
- Sheikh, Z.; Sima, C.; Glogauer, M. Bone Replacement Materials and Techniques Used for Achieving Vertical Alveolar Bone Augmentation. Materials 2015, 8, 2953–2993. [Google Scholar] [CrossRef]
- Lin, H.K.; Pan, Y.H.; Salamanca, E.; Lin, Y.T.; Chang, W.J. Prevention of Bone Resorption by HA/β-TCP + Collagen Composite after Tooth Extraction: A Case Series. Int. J. Environ. Res. Public Health 2019, 16, 4616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
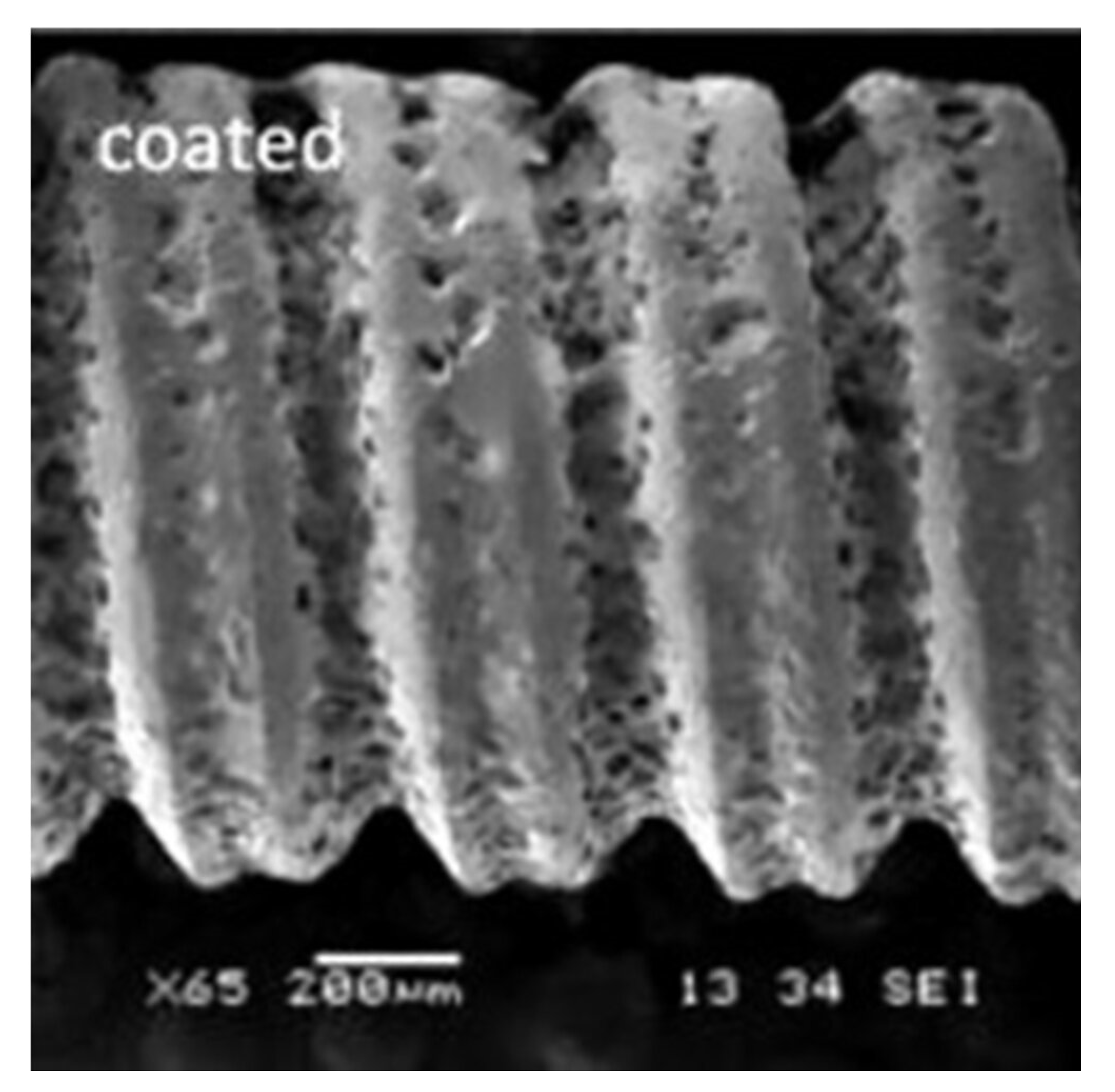
- Zafar, M.S.; Farooq, I.; Awais, M.; Najeeb, S.; Khurshid, Z.; Zohaib, S. Chapter 11—Bioactive Surface Coatings for Enhancing Osseointegration of Dental Implants. In Biomedical, Therapeutic and Clinical Applications of Bioactive Glasses; Kaur, G., Ed.; Woodhead Publishing: Cambridge, UK, 2019; pp. 313–329. [Google Scholar]
- Dong, H.; Liu, H.; Zhou, N.; Li, Q.; Yang, G.; Chen, L.; Mou, Y. Surface Modified Techniques and Emerging Functional Coating of Dental Implants. Coatings 2020, 10, 1012. [Google Scholar] [CrossRef]
- Pobloth, A.-M.; Mersiowsky, M.J.; Kliemt, L.; Schell, H.; Dienelt, A.; Pfitzner, B.M.; Burgkart, R.; Detsch, R.; Wulsten, D.; Boccaccini, A.R.; et al. Bioactive coating of zirconia toughened alumina ceramic implants improves cancellous osseointegration. Sci. Rep. 2019, 9, 16692. [Google Scholar] [CrossRef] [Green Version]
- Habibah, T.U.; Amlani, D.V.; Brizuela, M. Hydroxyapatite Dental Material. 2021 Sep 18. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Al-Noaman, A.; Rawlinson, S.C.F.; Hill, R.G. MgF2- containing glasses as a coating for titanium dental implant. I- Glass powder. J. Mech. Behav. Biomed. Mater. 2022, 125, 104948. [Google Scholar] [CrossRef]
- Oliver, J.-a.N.; Su, Y.; Lu, X.; Kuo, P.-H.; Du, J.; Zhu, D. Bioactive glass coatings on metallic implants for biomedical applications. Bioact. Mater. 2019, 4, 261–270. [Google Scholar] [CrossRef]
- Rohr, N.; Nebe, J.B.; Schmidli, F.; Müller, P.; Weber, M.; Fischer, H.; Fischer, J. Influence of bioactive glass-coating of zirconia implant surfaces on human osteoblast behavior in vitro. Dent. Mater. 2019, 35, 862–870. [Google Scholar] [CrossRef]
- Zhang, M.; Pu, X.; Chen, X.; Yin, G. In-vivo performance of plasma-sprayed CaO–MgO–SiO2-based bioactive glass-ceramic coating on Ti–6Al–4V alloy for bone regeneration. Heliyon 2019, 5, e02824. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Li, K.; Xie, Y.; Pan, H.; Zhao, J.; Huang, L.; Zheng, X. Different response of osteoblastic cells to Mg(2+), Zn(2+) and Sr(2+) doped calcium silicate coatings. J. Mater. Sci. Mater. Med. 2016, 27, 56. [Google Scholar] [CrossRef] [PubMed]
- Santos-Coquillat, A.; Mohedano, M.; Martinez-Campos, E.; Arrabal, R.; Pardo, A.; Matykina, E. Bioactive multi-elemental PEO-coatings on titanium for dental implant applications. Mater. Sci. Eng. C 2019, 97, 738–752. [Google Scholar] [CrossRef] [PubMed]
- Menzies, K.L.; Jones, L. The impact of contact angle on the biocompatibility of biomaterials. Optom. Vis. Sci. 2010, 87, 387–399. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Li, Y.; Min, Y.; Hao, J.; Liang, C.; Li, H.; Wang, G.; Liu, S.; Wang, H. Synergistic effects of hierarchical hybrid micro/nanostructures on the biological properties of titanium orthopaedic implants. RSC Adv. 2015, 5, 49552–49558. [Google Scholar] [CrossRef]
- Quinn, J.; McFadden, R.; Chan, C.-W.; Carson, L. Titanium for orthopedic applications: An overview of surface modification to improve biocompatibility and prevent bacterial biofilm formation. IScience 2020, 23, 101745. [Google Scholar] [CrossRef]












Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almulhim, K.S.; Syed, M.R.; Alqahtani, N.; Alamoudi, M.; Khan, M.; Ahmed, S.Z.; Khan, A.S. Bioactive Inorganic Materials for Dental Applications: A Narrative Review. Materials 2022, 15, 6864. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15196864
Almulhim KS, Syed MR, Alqahtani N, Alamoudi M, Khan M, Ahmed SZ, Khan AS. Bioactive Inorganic Materials for Dental Applications: A Narrative Review. Materials. 2022; 15(19):6864. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15196864
Chicago/Turabian StyleAlmulhim, Khalid S., Mariam Raza Syed, Norah Alqahtani, Marwah Alamoudi, Maria Khan, Syed Zubairuddin Ahmed, and Abdul Samad Khan. 2022. "Bioactive Inorganic Materials for Dental Applications: A Narrative Review" Materials 15, no. 19: 6864. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15196864