
Experimental Validation of Diffraction Lithography for Fabrication of Solid Microneedles
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
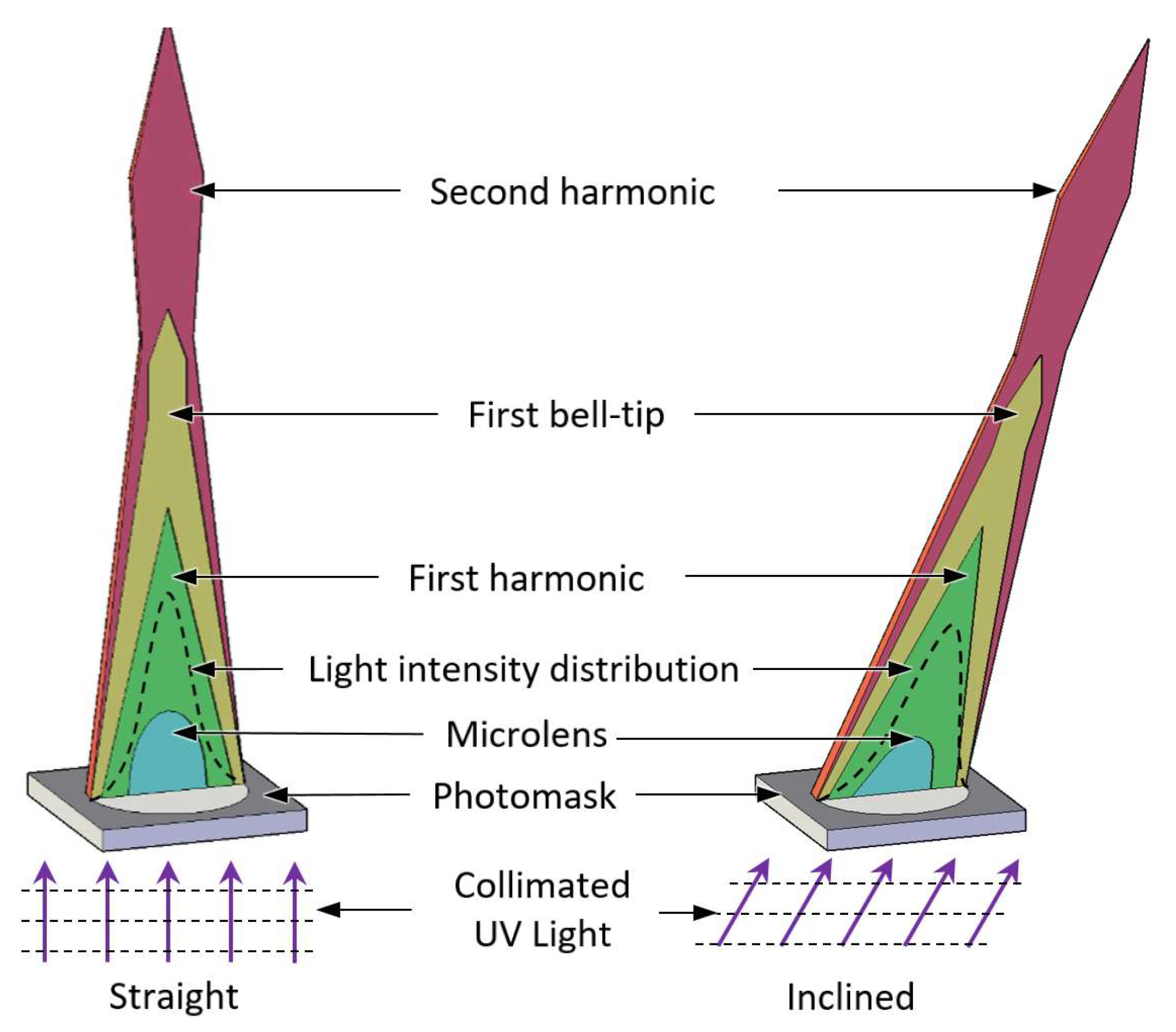
2. UV Light Propagation
2.1. Experimental Setup for UV Light Visualization
2.2. COMSOL Multiphysics Simulation Condition for UV Light Propagation
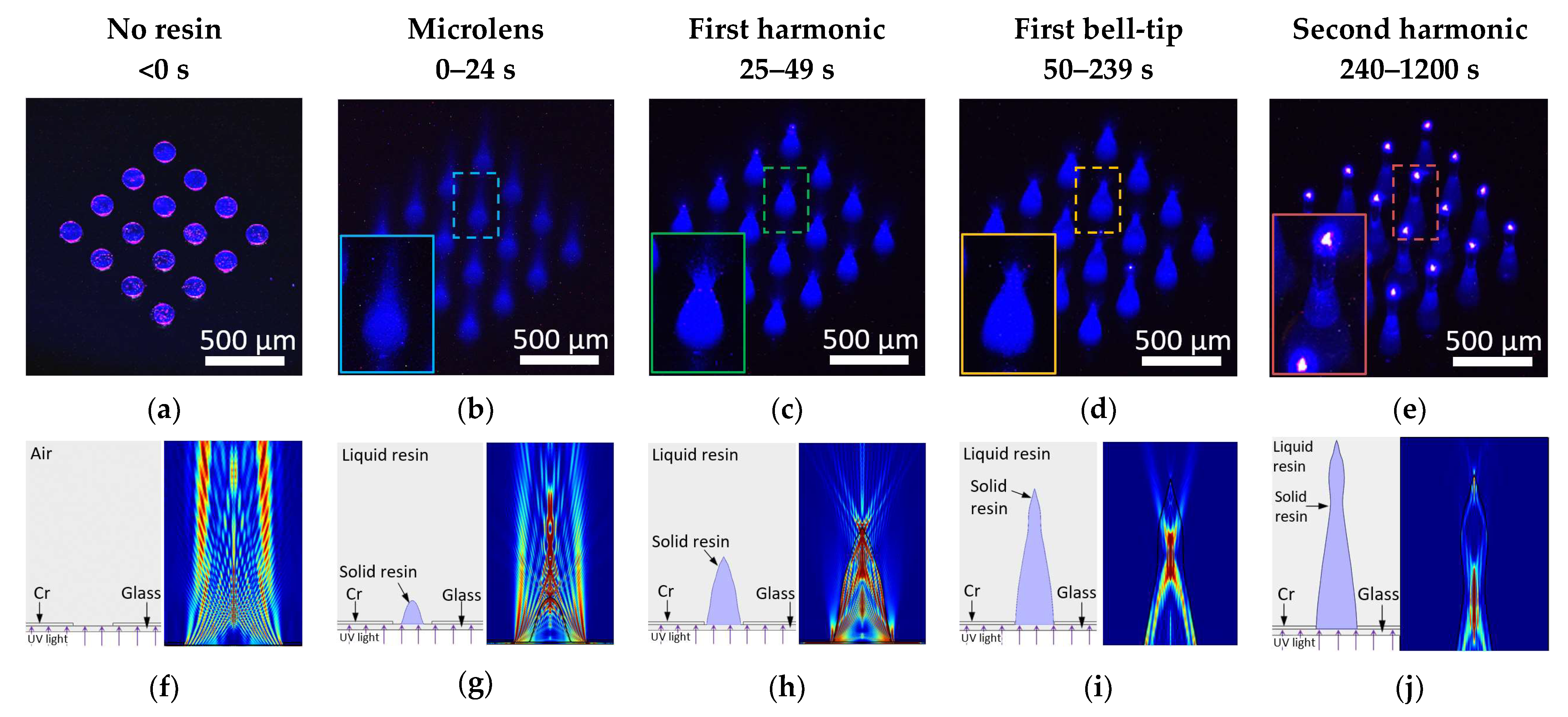
2.3. Experimental Visualization Results of UV Light Propagation
2.4. Simulation Results of UV Light Propagation
3. Fabrication
4. Results and Discussion
4.1. Photomask Patterns Size
4.2. UV Light Intensity
4.3. UV Exposure Time
4.4. Refractive Index
4.5. Large Scale Fabrication Results
4.6. Skin Insertion Tests
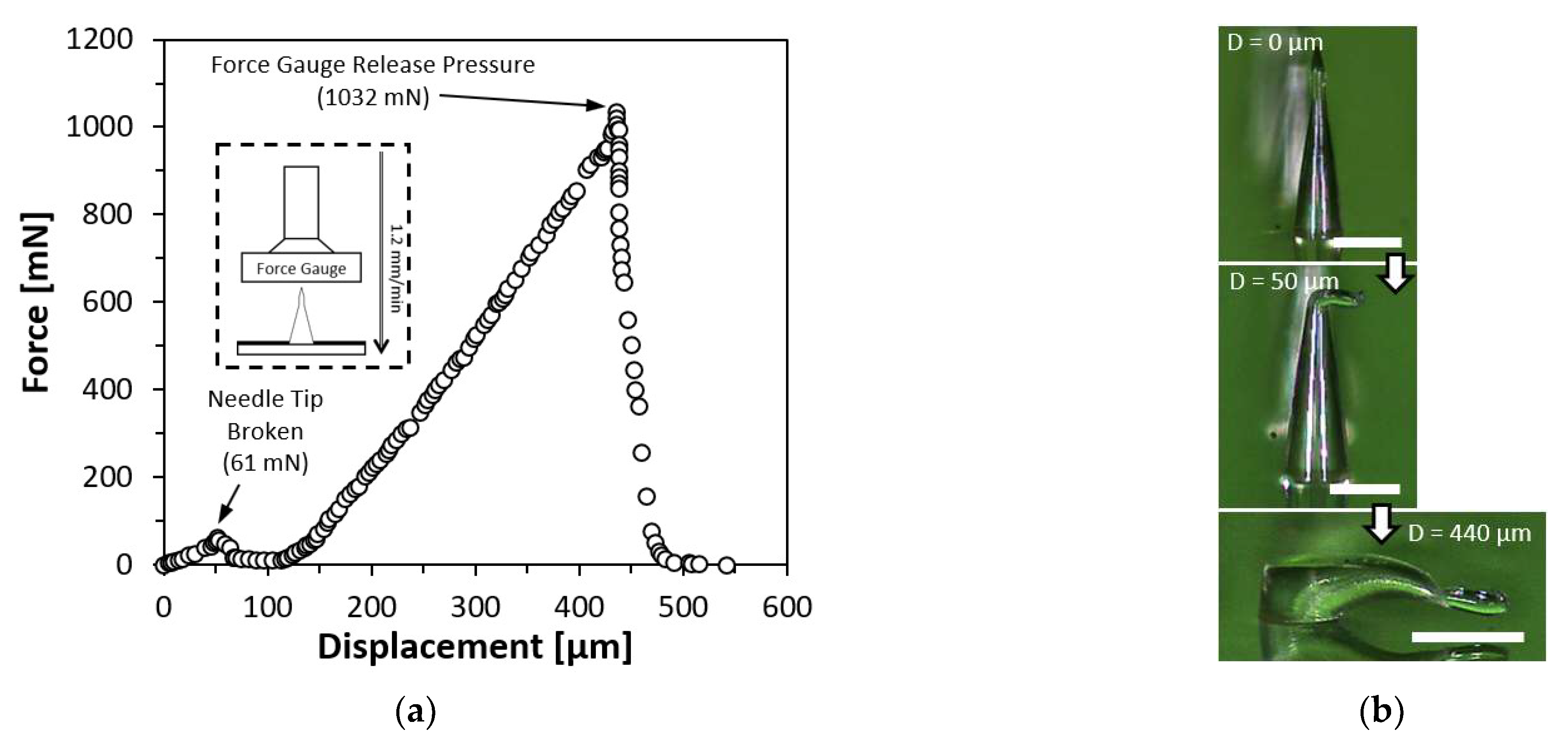
4.7. Force-Displacement Test on Straight Microneedle
4.8. Force-Displacement Test on Inclined Microneedle
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jenkins, K., II. Needle Phobia: A Psychological Perspective. BJA Br. J. Anaesth. 2014, 113, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Nir, Y.; Paz, A.; Sabo, E.; Potasman, I. Fear of Injections in Young Adults: Prevalence and Associations. Am. J. Trop. Med. Hyg. 2003, 68, 341–344. [Google Scholar] [CrossRef] [PubMed]
- Gold, K. Analysis: The Impact of Needle, Syringe, and Lancet Disposal on the Community. J. Diabetes Sci. Technol. 2011, 5, 848–850. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giudice, E.L.; Campbell, J.D. Needle-Free Vaccine Delivery. Adv. Drug Deliv. Rev. 2006, 58, 68–89. [Google Scholar] [CrossRef] [PubMed]
- Matthias, D.M.; Robertson, J.; Garrison, M.M.; Newland, S.; Nelson, C. Freezing Temperatures in the Vaccine Cold Chain: A Systematic Literature Review. Vaccine 2007, 25, 3980–3986. [Google Scholar] [CrossRef] [Green Version]
- Jeong, W.Y.; Kwon, M.; Choi, H.E.; Kim, K.S. Recent Advances in Transdermal Drug Delivery Systems: A Review. Biomater. Res. 2021, 25, 24. [Google Scholar] [CrossRef]
- Jeong, H.-R.; Kim, J.-Y.; Kim, S.-N.; Park, J.-H. Local Dermal Delivery of Cyclosporin A, a Hydrophobic and High Molecular Weight Drug, Using Dissolving Microneedles. Eur. J. Pharm. Biopharm. 2018, 127, 237–243. [Google Scholar] [CrossRef]
- Escobar-Chávez, J.J.; Bonilla-Martínez, D.; Angélica, M.; Villegas-González; Molina-Trinidad, E.; Casas-Alancaster, N.; Revilla-Vázquez, A.L. Microneedles: A Valuable Physical Enhancer to Increase Transdermal Drug Delivery. J. Clin. Pharmacol. 2011, 51, 964–977. [Google Scholar] [CrossRef]
- Goldberg, M.; Gomez-Orellana, I. Challenges for the Oral Delivery of Macromolecules. Nat. Rev. Drug Discov. 2003, 2, 289–295. [Google Scholar] [CrossRef]
- Singh, R.; Singh, S.; Lillard, J.W. Past, Present, and Future Technologies for Oral Delivery of Therapeutic Proteins. J. Pharm. Sci. 2008, 97, 2497–2523. [Google Scholar] [CrossRef]
- Moreira, A.F.; Rodrigues, C.F.; Jacinto, T.A.; Miguel, S.P.; Costa, E.C.; Correia, I.J. Microneedle-Based Delivery Devices for Cancer Therapy: A Review. Pharmacol. Res. 2019, 148, 104438. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, S.; Dave, K.; Venuganti, V.V.K. Microneedles in the Clinic. J. Control. Release 2017, 260, 164–182. [Google Scholar] [CrossRef] [PubMed]
- Zaid Alkilani, A.; McCrudden, M.T.C.; Donnelly, R.F. Transdermal Drug Delivery: Innovative Pharmaceutical Developments Based on Disruption of the Barrier Properties of the Stratum Corneum. Pharmaceutics 2015, 7, 438–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, J.; Gill, H.S.; Andrews, S.N.; Prausnitz, M.R. Kinetics of Skin Resealing after Insertion of Microneedles in Human Subjects. J. Control. Release 2011, 154, 148–155. [Google Scholar] [CrossRef] [Green Version]
- Gill, H.S.; Denson, D.D.; Burris, B.A.; Prausnitz, M.R. Effect of Microneedle Design on Pain in Human Subjects. Clin. J. Pain 2008, 24, 585–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donnelly, R.F.; Singh, T.R.R.; Alkilani, A.Z.; McCrudden, M.T.C.; O’Neill, S.; O’Mahony, C.; Armstrong, K.; McLoone, N.; Kole, P.; Woolfson, A.D. Hydrogel-Forming Microneedle Arrays Exhibit Antimicrobial Properties: Potential for Enhanced Patient Safety. Int. J. Pharm. 2013, 451, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, J.J.; Arya, J.M.; McClain, M.A.; Frew, P.M.; Meltzer, M.I.; Prausnitz, M.R. Microneedle Patches: Usability and Acceptability for Self-Vaccination against Influenza. Vaccine 2014, 32, 1856–1862. [Google Scholar] [CrossRef] [Green Version]
- Hirobe, S.; Azukizawa, H.; Matsuo, K.; Zhai, Y.; Quan, Y.-S.; Kamiyama, F.; Suzuki, H.; Katayama, I.; Okada, N.; Nakagawa, S. Development and Clinical Study of a Self-Dissolving Microneedle Patch for Transcutaneous Immunization Device. Pharm. Res. 2013, 30, 2664–2674. [Google Scholar] [CrossRef]
- Hoesly, F.J.; Borovicka, J.; Gordon, J.; Nardone, B.; Holbrook, J.S.; Pace, N.; Ibrahim, O.; Bolotin, D.; Warycha, M.; Kwasny, M.; et al. Safety of a Novel Microneedle Device Applied to Facial Skin: A Subject- and Rater-Blinded, Sham-Controlled, Randomized Trial. Arch. Derm. 2012, 148, 711–717. [Google Scholar] [CrossRef] [Green Version]
- Jarrahian, C.; Zehrung, D.; Saxon, E.; Griswold, E.; Klaff, L. Clinical Performance and Safety of the ID Adapter, a Prototype Intradermal Delivery Technology for Vaccines, Drugs, and Diagnostic Tests. Procedia Vaccinol. 2012, 6, 125–133. [Google Scholar] [CrossRef]
- Haq, M.I.; Smith, E.; John, D.N.; Kalavala, M.; Edwards, C.; Anstey, A.; Morrissey, A.; Birchall, J.C. Clinical Administration of Microneedles: Skin Puncture, Pain and Sensation. Biomed. Microdevices 2009, 11, 35–47. [Google Scholar] [CrossRef]
- Henry, S.; McAllister, D.V.; Allen, M.G.; Prausnitz, M.R. Microfabricated Microneedles: A Novel Approach to Transdermal Drug Delivery. J. Pharm. Sci. 1998, 87, 922–925. [Google Scholar] [CrossRef] [PubMed]
- Nejad, H.R.; Sadeqi, A.; Kiaee, G.; Sonkusale, S. Low-Cost and Cleanroom-Free Fabrication of Microneedles. Microsyst. Nanoeng. 2018, 4, 17073. [Google Scholar] [CrossRef] [Green Version]
- Evens, T.; Malek, O.; Castagne, S.; Seveno, D.; Van Bael, A. A Novel Method for Producing Solid Polymer Microneedles Using Laser Ablated Moulds in an Injection Moulding Process. Manuf. Lett. 2020, 24, 29–32. [Google Scholar] [CrossRef]
- Gülçür, M.; Romano, J.-M.; Penchev, P.; Gough, T.; Brown, E.; Dimov, S.; Whiteside, B. A Cost-Effective Process Chain for Thermoplastic Microneedle Manufacture Combining Laser Micro-Machining and Micro-Injection Moulding. CIRP J. Manuf. Sci. Technol. 2021, 32, 311–321. [Google Scholar] [CrossRef]
- Evens, T.; Malek, O.; Castagne, S.; Seveno, D.; Van Bael, A. Controlling the Geometry of Laser Ablated Microneedle Cavities in Different Mould Materials and Assessing the Replication Fidelity within Polymer Injection Moulding. J. Manuf. Process. 2021, 62, 535–545. [Google Scholar] [CrossRef]
- Chen, Z.; Ren, L.; Li, J.; Yao, L.; Chen, Y.; Liu, B.; Jiang, L. Rapid Fabrication of Microneedles Using Magnetorheological Drawing Lithography. Acta Biomater. 2018, 65, 283–291. [Google Scholar] [CrossRef]
- Lee, K.; Lee, H.C.; Lee, D.-S.; Jung, H. Drawing Lithography: Three-Dimensional Fabrication of an Ultrahigh-Aspect-Ratio Microneedle. Adv. Mater. 2010, 22, 483–486. [Google Scholar] [CrossRef]
- Ren, L.; Jiang, Q.; Chen, Z.; Chen, K.; Xu, S.; Gao, J.; Jiang, L. Flexible Microneedle Array Electrode Using Magnetorheological Drawing Lithography for Bio-Signal Monitoring. Sens. Actuators A Phys. 2017, 268, 38–45. [Google Scholar] [CrossRef]
- Lee, C.Y.; Lee, K.; You, Y.S.; Lee, S.H.; Jung, H. Tower Microneedle Via Reverse Drawing Lithography for Innocuous Intravitreal Drug Delivery. Adv. Healthc. Mater. 2013, 2, 812–816. [Google Scholar] [CrossRef]
- Krieger, K.J.; Bertollo, N.; Dangol, M.; Sheridan, J.T.; Lowery, M.M.; O’Cearbhaill, E.D. Simple and Customizable Method for Fabrication of High-Aspect Ratio Microneedle Molds Using Low-Cost 3D Printing. Microsyst. Nanoeng. 2019, 5, 42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Shan, W.; Yang, Y.; Joralmon, D.; Zhu, Y.; Chen, Y.; Yuan, Y.; Xu, H.; Rong, J.; Dai, R.; et al. Limpet Tooth-Inspired Painless Microneedles Fabricated by Magnetic Field-Assisted 3D Printing. Adv. Funct. Mater. 2021, 31, 2003725. [Google Scholar] [CrossRef]
- Pere, C.P.P.; Economidou, S.N.; Lall, G.; Ziraud, C.; Boateng, J.S.; Alexander, B.D.; Lamprou, D.A.; Douroumis, D. 3D Printed Microneedles for Insulin Skin Delivery. Int. J. Pharm. 2018, 544, 425–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Sayed, N.; Vaut, L.; Schneider, M. Customized Fast-Separable Microneedles Prepared with the Aid of 3D Printing for Nanoparticle Delivery. Eur. J. Pharm. Biopharm. 2020, 154, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Trautmann, A.; Roth, G.-L.; Nujiqi, B.; Walther, T.; Hellmann, R. Towards a Versatile Point-of-Care System Combining Femtosecond Laser Generated Microfluidic Channels and Direct Laser Written Microneedle Arrays. Microsyst. Nanoeng. 2019, 5, 6. [Google Scholar] [CrossRef] [Green Version]
- Plamadeala, C.; Gosain, S.R.; Purkhart, S.; Buchegger, B.; Baumgartner, W.; Heitz, J. Three-Dimensional Photonic Structures Fabricated by Two-Photon Polymerization for Microfluidics and Microneedles. In Proceedings of the 2018 20th International Conference on Transparent Optical Networks (ICTON), Bucharest, Romania, 1–5 July 2018; pp. 1–4. [Google Scholar]
- Cordeiro, A.S.; Tekko, I.A.; Jomaa, M.H.; Vora, L.; McAlister, E.; Volpe-Zanutto, F.; Nethery, M.; Baine, P.T.; Mitchell, N.; McNeill, D.W.; et al. Two-Photon Polymerisation 3D Printing of Microneedle Array Templates with Versatile Designs: Application in the Development of Polymeric Drug Delivery Systems. Pharm. Res. 2020, 37, 174. [Google Scholar] [CrossRef]
- Takahashi, H.; Heo, Y.J.; Shimoyama, I. Scalable Fabrication of PEGDA Microneedles Using UV Exposure via a Rotating Prism. J. Microelectromech. Syst. 2017, 26, 990–992. [Google Scholar] [CrossRef]
- Lim, H.; Ha, S.; Bae, M.; Yoon, S.-H. A Highly Robust Approach to Fabricate the Mass-Customizable Mold of Sharp-Tipped Biodegradable Polymer Microneedles for Drug Delivery. Int. J. Pharm. 2021, 600, 120475. [Google Scholar] [CrossRef]
- Dardano, P.; De Martino, S.; Battisti, M.; Miranda, B.; Rea, I.; De Stefano, L. One-Shot Fabrication of Polymeric Hollow Microneedles by Standard Photolithography. Polymers 2021, 13, 520. [Google Scholar] [CrossRef]
- Kim, J.; Cheng, X.; Ahn, H.; Elles, D.S.; Yoon, Y.-K. Lithographically Defined Integrable Air-Lifted Bow-Tie Antennas. In Proceedings of the 2010 IEEE 23rd International Conference on Micro Electro Mechanical Systems (MEMS), Hong Kong, China, 24–28 January 2010; pp. 791–794. [Google Scholar]
- Tan, J.Y.; Ahn, M.; Al-Thuwaini, H.; Choi, S.; Kim, J. Diffraction Lithography for 3-D Microneedle Fabrication. In Proceedings of the 2020 IEEE 33rd International Conference on Micro Electro Mechanical Systems (MEMS), Vancouver, BC, Canada, 18–22 January 2020; pp. 921–924. [Google Scholar]
- Tan, J.Y.; Kim, A.; Kim, J. Modeling, Characterization, and Fabrication of Bell-Tip Microneedle Array by Diffraction and Self-Aligned Lens Effects. Appl. Phys. Lett. 2021, 119, 023501. [Google Scholar] [CrossRef]
- Tan, J.Y.; Li, Y.; Prakash, P.; Natarajan, B.; Kim, J. ‘Jk’ Fabrication of Solid Microneedle Using Multi-Slit Diffraction UV Lithography. In Proceedings of the 2022 IEEE 17th International Conference on Nano/Micro Engineered and Molecular Systems (NEMS), Taoyuan, Taiwan, 14–17 April 2022; pp. 357–360. [Google Scholar]
- Formlabs Inc. Using Surgical Guide Resin. Available online: http://support.formlabs.com/ (accessed on 4 November 2022).
- Formlabs Inc. Creating 3D Printed Lenses and a 3D Printed Camera with Stereolithography. Available online: https://formlabs.com/blog/creating-camera-lenses-with-stereolithography/ (accessed on 2 November 2022).
- Formlabs Surgical Guide Resin Safety Data Sheet 2019. Available online: https://dental-media.formlabs.com/datasheets/Surgical-Guide-USA-English.pdf/ (accessed on 6 October 2022).
- Shiba, S.F.; Tan, J.Y.; Kim, J. Multidirectional UV-LED Lithography Using an Array of High-Intensity UV-LEDs and Tilt-Rotational Sample Holder for 3-D Microfabrication. Micro Nano Syst. Lett. 2020, 8, 5. [Google Scholar] [CrossRef]
- Rousseau, E.; Felbacq, D. Concept of a Generalized Law of Refraction: A Phenomenological Model. ACS Photonics 2020, 7, 1649–1654. [Google Scholar] [CrossRef]
- Park, J.-H.; Allen, M.G.; Prausnitz, M.R. Biodegradable Polymer Microneedles: Fabrication, Mechanics and Transdermal Drug Delivery. J. Control. Release 2005, 104, 51–66. [Google Scholar] [CrossRef] [PubMed]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, J.Y.; Li, Y.; Chamani, F.; Tharzeen, A.; Prakash, P.; Natarajan, B.; Sheth, R.A.; Park, W.M.; Kim, A.; Yoon, D.; et al. Experimental Validation of Diffraction Lithography for Fabrication of Solid Microneedles. Materials 2022, 15, 8934. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15248934
Tan JY, Li Y, Chamani F, Tharzeen A, Prakash P, Natarajan B, Sheth RA, Park WM, Kim A, Yoon D, et al. Experimental Validation of Diffraction Lithography for Fabrication of Solid Microneedles. Materials. 2022; 15(24):8934. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15248934
Chicago/Turabian StyleTan, Jun Ying, Yuankai Li, Faraz Chamani, Aabila Tharzeen, Punit Prakash, Balasubramaniam Natarajan, Rahul A. Sheth, Won Min Park, Albert Kim, Donghoon Yoon, and et al. 2022. "Experimental Validation of Diffraction Lithography for Fabrication of Solid Microneedles" Materials 15, no. 24: 8934. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15248934