
Evaluation of Retention, Wear, and Maintenance of Attachment Systems for Single- or Two-Implant-Retained Mandibular Overdentures: A Systematic Review


Abstract
:1. Introduction
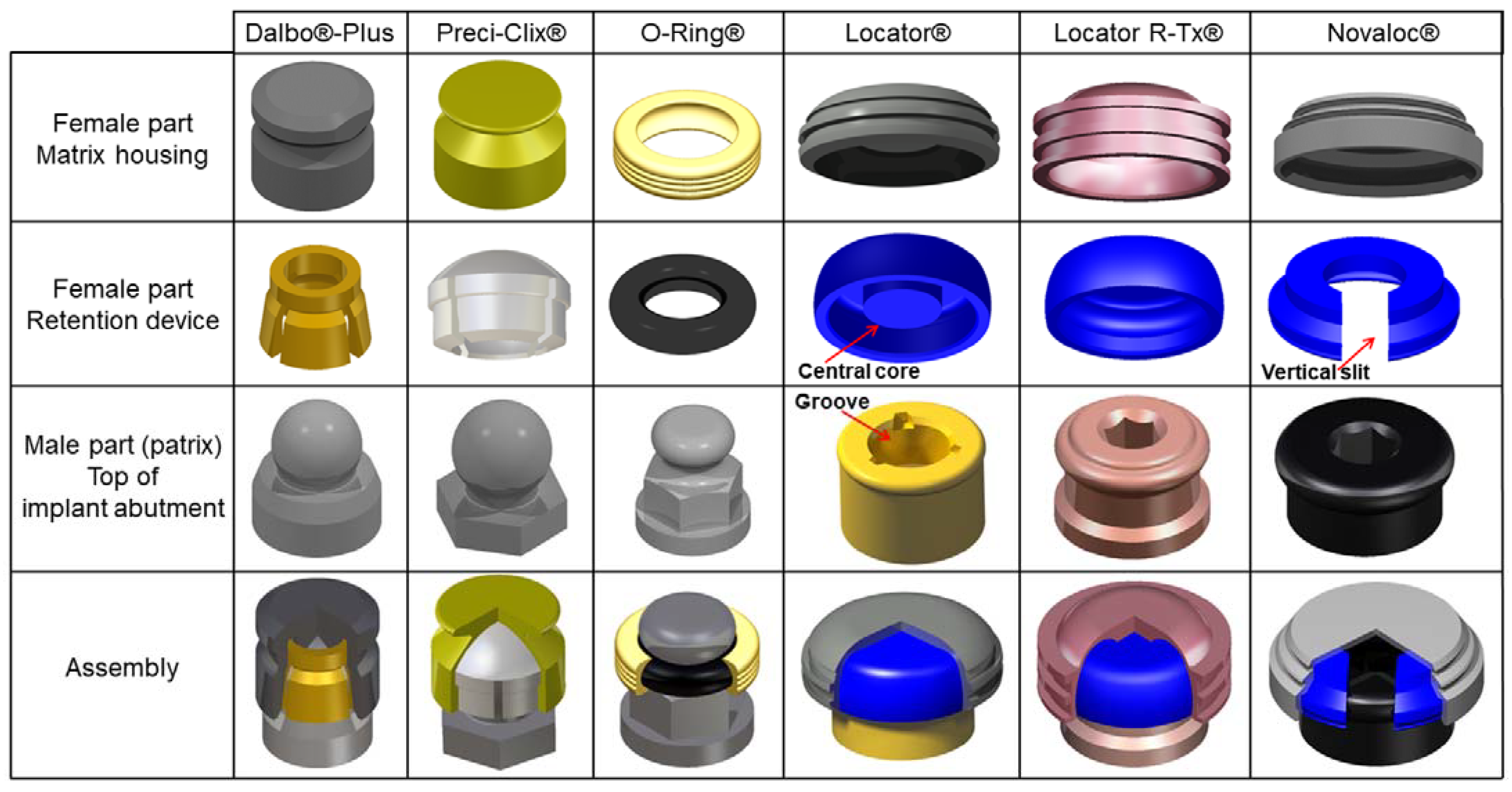
1.1. Ball Attachment Systems
1.2. Cylindrical Attachment Systems
Objectives
2. Materials and Methods
2.1. Protocol
- Participants/population: Patients with completely edentulous mandibular arch mainly opposed to edentulous maxillary arch (or partial removable denture, or fixed denture, or natural teeth).
- Intervention/exposure: 1- or 2-implant-retained mandibular overdenture using ball attachment systems (BAS) or cylindrical attachment systems (CAS) only.
- Comparator/control: Comparison between CAS and BAS and, secondarily, their subgroups.
- Outcomes: Initial retention, retention after clinical use, retention loss, wear, and maintenance.
2.2. Search Strategy for the Identification of the Studies
2.3. Eligibility Criteria
- (i)
- in vitro studies reporting on initial retention, retention loss, and wear of real or simulated 1- or 2-IRMO using stud-shaped BAS or CAS,
- (ii)
- clinical studies (i.e., prospective, retrospective, randomized controlled trials including cross-over trials) reporting on maintenance of AS (retention loss, wear) in 1 or 2-IRMO regardless of follow-up time.
- (i)
- maxillary overdenture,
- (ii)
- partial dentures,
- (iii)
- fixed overdentures,
- (iv)
- overdentures on remaining natural teeth or roots,
- (v)
- more than two implants,
- (vi)
- implant splinting,
- (vii)
- other AS (bars-clips, magnets, telescopic double crowns),
- (viii)
- anecdotal BAS and CAS.
2.4. Outcome Measures
- (i)
- the initial retention and its evolution over time of clinical use (Newton (N), loss of retention (%)), in correlation with the observed wear patterns (scanning electron microscopy with qualitative description) and the dimensional changes (μm) of AS components,
- (ii)
- the maintenance follow-up (frequencies: months/years), and maintenance procedure of AS (activation/replacement).
- (i)
- the effects of denture cleansing solutions on the retention and wear of AS,
- (ii)
- the overdenture maintenance (i.e., reline/rebase of denture, fracture repair or occlusal adjustment, denture replacement),
- (iii)
- the interimplant distance (mm) or angulation (°) and their impact on primary outcomes.
2.5. Data Extraction and Analysis
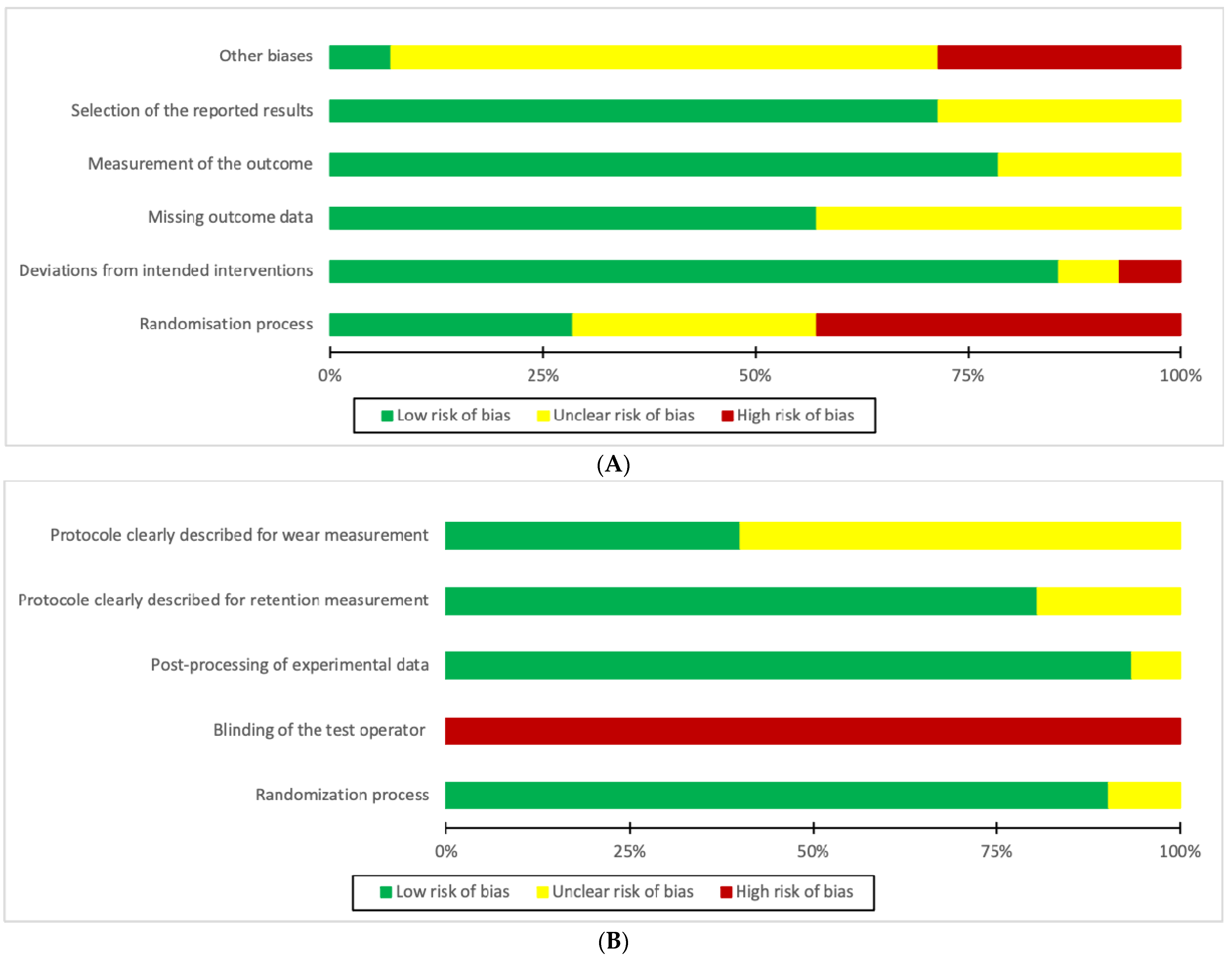
2.6. Study Quality Assessment
3. Results and Discussion
3.1. Initial Retention of BAS and CAS
3.2. Maintenance, Wear and Loss of Retention of BAS and CAS
3.3. Influence of Implant Parameters on Retention, Wear and Maintenance of AS
3.4. Influence of Experimental Conditions on Retention, Wear and Maintenance of AS
3.5. Limitations
- (i)
- prosthetic parameters (real or artificial denture, prosthetic design, implant number, interimplant distance, and angulation between implants or between implants and AS),
- (ii)
- in vitro experimental parameters (environment, loading conditions, and sample characteristics),
- (iii)
- clinical conditions in patient studies (bone loss, type of prosthetic construction on the opposing arch, dental occlusion, masticatory forces, prosthetic hygiene, and regular dental aftercare visits after setting denture).
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AS | attachment system |
| BAS | ball attachment systems |
| CAS | cylindrical attachment systems |
| CC | chewing cycle |
| IRC | Insertion–removal cycle |
| IRMO | implant-retained mandibular overdenture |
| PEEK | polyetheretherketone |
| RD | retention device |
| RoB | risk of bias |
| SR | systematic review |
References
- Payne, A.G.; Alsabeeha, N.H.; Atieh, M.A.; Esposito, M.; Ma, S.; Anas El-Wegoud, M. Interventions for Replacing Missing Teeth: Attachment Systems for Implant Overdentures in Edentulous Jaws. Cochrane Database Syst. Rev. 2018, 10, CD008001. [Google Scholar] [CrossRef] [PubMed]
- Büttel, A.E.; Bühler, N.M.; Marinello, C.P. Locator or ball attachment: A guide for clinical decision making. Schweiz. Mon. Zahnmed. Rev. Mens. Suisse Odonto-Stomatol. Riv. Mens. Svizz. Odontol. E Stomatol. 2009, 119, 901–918. [Google Scholar]
- Alsabeeha, N.H.M.; Payne, A.G.T.; De Silva, R.K.; Thomson, W.M. Mandibular Single-Implant Overdentures: Preliminary Results of a Randomised-Control Trial on Early Loading with Different Implant Diameters and Attachment Systems. Clin. Oral Implants Res. 2011, 22, 330–337. [Google Scholar] [CrossRef] [PubMed]
- Alsabeeha, N.H.M.; Swain, M.V.; Payne, A.G.T. Clinical Performance and Material Properties of Single-Implant Overdenture Attachment Systems. Int. J. Prosthodont. 2011, 24, 247–254. [Google Scholar] [PubMed]
- Wolf, K.; Ludwig, K.; Hartfil, H.; Kern, M. Analysis of Retention and Wear of Ball Attachments. Quintessence Int. Berl. Ger. 2009, 40, 405–412. [Google Scholar]
- Krennmair, G.; Seemann, R.; Fazekas, A.; Ewers, R.; Piehslinger, E. Patient Preference and Satisfaction with Implant-Supported Mandibular Overdentures Retained with Ball or Locator Attachments: A Crossover Clinical Trial. Int. J. Oral Maxillofac. Implants 2012, 27, 1560–1568. [Google Scholar]
- Kleis, W.K.; Kämmerer, P.W.; Hartmann, S.; Al-Nawas, B.; Wagner, W. A Comparison of Three Different Attachment Systems for Mandibular Two-Implant Overdentures: One-Year Report. Clin. Implant Dent. Relat. Res. 2010, 12, 209–218. [Google Scholar] [CrossRef]
- Mackie, A.; Lyons, K.; Thomson, W.M.; Payne, A.G.T. Mandibular Two-Implant Overdentures: Prosthodontic Maintenance Using Different Loading Protocols and Attachment Systems. Int. J. Prosthodont. 2011, 24, 405–416. [Google Scholar]
- Cristache, C.M.; Muntianu, L.A.S.; Burlibasa, M.; Didilescu, A.C. Five-Year Clinical Trial Using Three Attachment Systems for Implant Overdentures. Clin. Oral Implants Res. 2014, 25, e171–e178. [Google Scholar] [CrossRef]
- Sultana, N.; Bartlett, D.W.; Suleiman, M. Retention of Implant-Supported Overdentures at Different Implant Angulations: Comparing Locator and Ball Attachments. Clin. Oral Implants Res. 2017, 28, 1406–1410. [Google Scholar] [CrossRef]
- Alsabeeha, N.; Atieh, M.; Swain, M.V.; Payne, A.G.T. Attachment Systems for Mandibular Single-Implant Overdentures: An in vitro Retention Force Investigation on Different Designs. Int. J. Prosthodont. 2010, 23, 160–166. [Google Scholar] [PubMed]
- Walton, J.N. A Randomized Clinical Trial Comparing Two Mandibular Implant Overdenture Designs: 3-Year Prosthetic Outcomes Using a Six-Field Protocol. Int. J. Prosthodont. 2003, 16, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Abi Nader, S.; de Souza, R.F.; Fortin, D.; De Koninck, L.; Fromentin, O.; Albuquerque Junior, R.F. Effect of Simulated Masticatory Loading on the Retention of Stud Attachments for Implant Overdentures. J. Oral Rehabil. 2011, 38, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Salehi, R.; Shayegh, S.S.; Johnston, W.M.; Hakimaneh, S.M.R. Effects of Interimplant Distance and Cyclic Dislodgement on Retention of LOCATOR and Ball Attachments: An in vitro Study. J. Prosthet. Dent. 2019, 122, 550–556. [Google Scholar] [CrossRef]
- Jabbour, Z.; Fromentin, O.; Lassauzay, C.; Abi Nader, S.; Correa, J.A.; Feine, J.; de Albuquerque Junior, R.F. Effect of Implant Angulation on Attachment Retention in Mandibular Two-Implant Overdentures: A Clinical Study. Clin. Implant Dent. Relat. Res. 2014, 16, 565–571. [Google Scholar] [CrossRef]
- Kobayashi, M.; Srinivasan, M.; Ammann, P.; Perriard, J.; Ohkubo, C.; Müller, F.; Belser, U.C.; Schimmel, M. Effects of in vitro Cyclic Dislodging on Retentive Force and Removal Torque of Three Overdenture Attachment Systems. Clin. Oral Implants Res. 2014, 25, 426–434. [Google Scholar] [CrossRef]
- Fromentin, O.; Lassauzay, C.; Nader, S.A.; Feine, J.; de Albuquerque, R.F. Wear of Ball Attachments after 1 to 8 Years of Clinical Use: A Qualitative Analysis. Int. J. Prosthodont. 2011, 24, 270–272. [Google Scholar]
- Ortegón, S.M.; Thompson, G.A.; Agar, J.R.; Taylor, T.D.; Perdikis, D. Retention Forces of Spherical Attachments as a Function of Implant and Matrix Angulation in Mandibular Overdentures: An in vitro Study. J. Prosthet. Dent. 2009, 101, 231–238. [Google Scholar] [CrossRef] [Green Version]
- Yang, T.-C.; Maeda, Y.; Gonda, T.; Kotecha, S. Attachment Systems for Implant Overdenture: Influence of Implant Inclination on Retentive and Lateral Forces. Clin. Oral Implants Res. 2011, 22, 1315–1319. [Google Scholar] [CrossRef]
- Schittly, J.; Russe, P.; Hafian, H. Prothèses amovibles stabilisées sur implants: Indications et modes d’utilisation de l’attachement Locator®. Cah. Prothèse 2008, 142, 33–46. [Google Scholar]
- Rutkunas, V.; Mizutani, H.; Takahashi, H.; Iwasaki, N. Wear Simulation Effects on Overdenture Stud Attachments. Dent. Mater. J. 2011, 30, 845–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, M.; Schimmel, M.; Kobayashi, M.; Badoud, I.; Ammann, P.; Herrmann, F.R.; Müller, F. Influence of Different Lubricants on the Retentive Force of LOCATOR(®) Attachments—an in vitro Pilot Study. Clin. Oral Implants Res. 2016, 27, 771–775. [Google Scholar] [CrossRef] [PubMed]
- Gamborena, J.I.; Hazelton, L.R.; NaBadalung, D.; Brudvik, J. Retention of ERA Direct Overdenture Attachments before and after Fatigue Loading. Int. J. Prosthodont. 1997, 10, 123–130. [Google Scholar] [PubMed]
- Petropoulos, V.C.; Mante, F.K. Comparison of Retention and Strain Energies of Stud Attachments for Implant Overdentures. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2011, 20, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Stephens, G.J.; di Vitale, N.; O’Sullivan, E.; McDonald, A. The Influence of Interimplant Divergence on the Retention Characteristics of Locator Attachments, a Laboratory Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2014, 23, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, C.T.; Masri, R.; Driscoll, C.F.; Romberg, E. The Effect of Denture Cleansing Solutions on the Retention of Pink Locator Attachments: An in vitro Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2010, 19, 226–230. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.-W.; Yun, B.-H.; Jeong, C.-M.; Huh, J.-B. Retentive Properties of Two Stud Attachments with Polyetherketoneketone or Nylon Insert in Mandibular Implant Overdentures. Int. J. Oral Maxillofac. Implants 2018, 33, 1079–1088. [Google Scholar] [CrossRef]
- de Souza, R.F.; Bedos, C.; Esfandiari, S.; Makhoul, N.M.; Dagdeviren, D.; Abi Nader, S.; Jabbar, A.A.; Feine, J.S. Single-Implant Overdentures Retained by the Novaloc Attachment System: Study Protocol for a Mixed-Methods Randomized Cross-over Trial. Trials 2018, 19, 243. [Google Scholar] [CrossRef] [Green Version]
- Passia, N.; Ghazal, M.; Kern, M. Long-Term Retention Behaviour of Resin Matrix Attachment Systems for Overdentures. J. Mech. Behav. Biomed. Mater. 2016, 57, 88–94. [Google Scholar] [CrossRef]
- Maniewicz, S.; Badoud, I.; Herrmann, F.R.; Chebib, N.; Ammann, P.; Schimmel, M.; Müller, F.; Srinivasan, M. In vitro Retention Force Changes during Cyclic Dislodging of Three Novel Attachment Systems for Implant Overdentures with Different Implant Angulations. Clin. Oral Implants Res. 2020, 31, 315–327. [Google Scholar] [CrossRef]
- Higgins, J.P.; Savović, J.; Page, M.J.; Elbers, R.G.; Sterne, J.A. Chapter 8: Assessing Risk of Bias in a Randomized Trial. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2 (updated February 2021); Cochrane: London, UK, 2021. [Google Scholar]
- Türk, P.E.; Geckili, O.; Türk, Y.; Günay, V.; Bilgin, T. In vitro Comparison of the Retentive Properties of Ball and Locator Attachments for Implant Overdentures. Int. J. Oral Maxillofac. Implants 2014, 29, 1106–1113. [Google Scholar] [CrossRef] [PubMed]
- Scherer, M.D.; McGlumphy, E.A.; Seghi, R.R.; Campagni, W.V. Comparison of Retention and Stability of Two Implant-Retained Overdentures Based on Implant Location. J. Prosthet. Dent. 2014, 112, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.-H.; Chung, C.-Y.; Cagna, D.R.; Cronin, R.J. Retention Characteristics of Attachment Systems for Implant Overdentures. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2004, 13, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, B.; Ozkir, E.; Johnston, W.M.; McGlumphy, E. Dislodgement Force Analysis of an Overdenture Attachment System. J. Prosthet. Dent. 2020, 123, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Gonuldas, F.; Tokar, E.; Ozturk, C. Evaluation of the Retention Characteristics of Various Stud Attachment Systems for Implant Retained Overdenture. Acta Bioeng. Biomech. 2018, 20, 135–141. [Google Scholar]
- Cune, M.S.; Verhoeven, J.W.; Meijer, G.J. A Prospective Evaluation of Frialoc Implants with Ball-Abutments in the Edentulous Mandible: 1-Year Results. Clin. Oral Implants Res. 2004, 15, 167–173. [Google Scholar] [CrossRef]
- Nogueira, T.E.; Aguiar, F.M.O.; de Barcelos, B.A.; Leles, C.R. A 2-Year Prospective Study of Single-Implant Mandibular Overdentures: Patient-Reported Outcomes and Prosthodontic Events. Clin. Oral Implants Res. 2018, 29, 541–550. [Google Scholar] [CrossRef]
- Passia, N.; Wolfart, S.; Kern, M. Ten-Year Clinical Outcome of Single Implant-Retained Mandibular Overdentures-A Prospective Pilot Study. J. Dent. 2019, 82, 63–65. [Google Scholar] [CrossRef]
- You, W.; Masri, R.; Romberg, E.; Driscoll, C.F.; You, T. The Effect of Denture Cleansing Solutions on the Retention of Pink Locator Attachments after Multiple Pulls: An in vitro Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2011, 20, 464–469. [Google Scholar] [CrossRef]
- Fromentin, O.; Lassauzay, C.; Nader, S.A.; Feine, J.; de Albuquerque, R.F. Clinical Wear of Overdenture Ball Attachments after 1, 3 and 8 Years. Clin. Oral Implants Res. 2011, 22, 1270–1274. [Google Scholar] [CrossRef]
- Al-Ghafli, S.A.; Michalakis, K.X.; Hirayama, H.; Kang, K. The in vitro Effect of Different Implant Angulations and Cyclic Dislodgement on the Retentive Properties of an Overdenture Attachment System. J. Prosthet. Dent. 2009, 102, 140–147. [Google Scholar] [CrossRef]
- Yabul, A.; Dayan, C.; Geckili, O.; Bilhan, H.; Tuncer, N. Evaluation of Volumetric Wear of Abutments on the Retention Loss of Ball Attachment Systems in Implant-Retained Overdentures: An in vitro Study. Clin. Implant Dent. Relat. Res. 2018, 20, 778–784. [Google Scholar] [CrossRef] [PubMed]
- Fromentin, O.; Lassauzay, C.; Nader, S.A.; Feine, J.; de Albuquerque, R.F. Wear of Matrix Overdenture Attachments after One to Eight Years of Clinical Use. J. Prosthet. Dent. 2012, 107, 191–198. [Google Scholar] [CrossRef]
- Branchi, R.; Vangi, D.; Virga, A.; Guertin, G.; Fazi, G. Resistance to Wear of Four Matrices with Ball Attachments for Implant Overdentures: A Fatigue Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2010, 19, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Tehini, G.; Baba, N.Z.; Majzoub, Z.; Nahas, P.; Berberi, A.; Rifai, K. In vitro Effect of Mastication on the Retention and Wear of Locator Attachments in a Flat Mandibular Ridge Model. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, e744–e751. [Google Scholar] [CrossRef]
- Elsyad, M.A.; Emera, R.M.; Ashmawy, T.M. Effect of Distal Implant Inclination on Dislodging Forces of Different Locator Attachments Used for Mandibular Overdentures: An In vitro Study. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2019, 28, e666–e674. [Google Scholar] [CrossRef] [Green Version]
- Elsyad, M.A.; Abo Hatem, O.E.; Shawky, A.F.; Emera, R.M.K. Effect of Different Degrees of Mesial Implant Inclination on the Retention and Stability of Two-Implant Mandibular Overdentures Retained with Stud Attachments: An In vitro Study. Int. J. Oral Maxillofac. Implants 2018, 33, 259–268. [Google Scholar] [CrossRef] [Green Version]
- Rabbani, S.; Juszczyk, A.S.; Clark, R.K.; Radford, D.R. Investigation of Retentive Force Reduction and Wear of the Locator Attachment System with Different Implant Angulations. Int. J. Oral Maxillofac. Implants 2015, 30, 556–563. [Google Scholar] [CrossRef] [Green Version]
- Kürkcüoğlu, I.; Özkir, S.E.; Köroğlu, A.; Sahin, O.; Yilmaz, B. Effect of Denture Cleansing Solutions on Different Retentive Attachments. J. Prosthet. Dent. 2016, 115, 606–610. [Google Scholar] [CrossRef]
- Ayyıldız, S.; Şahin, C.; Emir, F.; Ersu, B. Effect of Denture Cleansing Solutions on the Retention of Locator Attachments Over Time. J. Prosthodont. Off. J. Am. Coll. Prosthodont. 2020, 29, 237–242. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Studies | 1 or 2-IRMO | Inter-Implant Distance (mm) | Initial and Final Number and Type of Cycles | Cross-Head Speed (mm/min) Medium | Attachments System, Manufacturer | Materials | Retention Setup Before the Test (N) | Retention Force (N) | Retention Loss (%) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male Part | Retentive Device | Initial | Final | ||||||||
| Branchi et al., 2010 | 1 | - | 1 55000 IRC | 54 - | Ball Ø 2.20 mm Sweden & Martina | Ti | Teflon matrix | - | 13.92 | 17.75 | 27 |
| Red O-ring® rubber | - | 10.20 | 2.45 | 75 | |||||||
| Gold | - | 15.30 | 24.42 | −50 | |||||||
| Titanium | - | 13.24 | 4.31 | 68 | |||||||
| Yabul et al., 2018 | 2 | 19 | 10 5000 IRC | 54 - | Ball, Biohorizons | Ti | Plastic | - | 34.12 ± 4.99 | 11.19 ± 2.8 | 67.3 ± 5.74 |
| Ball, DTI, Istantbul | Plastic | - | 26.41 ± 5.8 | 10.58 ± 2.96 | 58.9 ± 12.21 | ||||||
| Ball, Straumann | Gold alloy | - | 48.16 ± 6.46 | 43.0 ± 6.30 | 10.5 ± 7.91 | ||||||
| Ball, Straumann | Titanium | - | 50.39 ± 4.81 | 5.59 ± 2.27 | 88.7 ± 5.11 | ||||||
| Elsyad et al., 2016 | 2 | 22 | 1 540 IRC | 50 Dry | Locator®, Zest Anchors | Ti + TiN | Blue | - | 19.64 ± 1.16 | 14.80 ± 0.83 | 24.64 |
| Pink | 51.20 ± 0.83 | 33.60 ± 2.30 | 34.37 | ||||||||
| White | 65.20 ± 1.30 | 39.80 ± 1.48 | 38.95 | ||||||||
| Gamborena et al., 1997 | 1 | - | 1 5500 IRC | 50 Water | ERA®, Sterngold | Gold alloy | White | 14.91 ± 3.43 | 2.25 ± 0.49 | 85 | |
| Orange | 24.71 ± 3.14 | 2.74 ± 0.88 | 88 | ||||||||
| Blue | 22.75 ± 2.84 | 3.73 ± 0.69 | 85 | ||||||||
| Gray | 24.03 ± 3.53 | 3.43 ± 0.98 | 87 | ||||||||
| Stephens et al., 2014 | 2 | 22 | 1 5500 IRC | 60 Artificial saliva | Locator®, Zest Anchors | Ti + TiN | Blue | 21.81 ± 7.44 | 15.97 ± 3.96 | 5.84 ± 4.45 | |
| Choi et al., 2018 | 2 | 22 | 1 400,000 CC 1080 IRC | 50 Demineralized water | Locator®, Zest Anchors | Ti + TiN | Blue | - | 20.1 ± 2.87 | 20.58 ± 3.09 | −2.81 ± 4.07 |
| Pink | 24.55 ± 2.14 | 37.42 ± 2.79 | −52.78 ± 7.78 | ||||||||
| White | 69.87 ± 5.73 | 42.56 ± 3.27 | 38.81 ± 5.32 | ||||||||
| CM Loc®, Cendres & Métaux | Ti | Light Green | 12.45 ± 1.27 | 12.83 ± 1.39 | −3.01 ± 1.92 | ||||||
| Red | 17.79 ± 1.70 | 21.48 ± 1.20 | −22.31 ± 17.18 | ||||||||
| Green | 39.35 ± 3.45 | 36.99 ± 1.75 | 5.57 ± 5.28 | ||||||||
| Blue | 44.07 ± 3.07 | 43.80 ± 2.45 | 0.52 ± 1.92 | ||||||||
| Maniewicz et al., 2020 | 2 | 20 | 1 10,000 IRC | - Artificial saliva | CM Loc®, Cendres & Métaux | Ti | Red | 81.8 ± 18.5 | 49.2 ± 12.6 | 39.85 | |
| Locator R-Tx®, Zest Anchors | Ti + TiN | Pink | 75.5 ± 24.9 | 60.0 ± 19.6 | 20.53 | ||||||
| Novaloc®, Straumann AG | Ti + ADLC | Yellow | 57.7 ± 31.0 | 59.4 ± 16.0 | −2.95 | ||||||
| Yilmaz et al., 2020 | 2 | - | 1 1440 IRC | 50 - | Locator®, Zest Anchors | Ti + TiN | Pink | 13.6 | 10.0 | 26.5 | |
| Locator R-Tx®, Zest Anchors | Ti + TiN | Pink | 20.1 | 14.0 | 30.4 | ||||||
| Tehini et al., 2020 | 2 | 22 | 1 100,000 CC | 60 Dry | Locator®, Zest Anchors | Ti + TiN | Blue | 9.95 ± 1.91 | 6.37 ± 2.64 | −37 ± 0.22 | |
| Pink | 15.43 ± 4.08 | 14.00 ± 3.89 | 9 ± 0.15 | ||||||||
| White | 41.73 ± 9.29 | 38.20 ± 5.11 | 7 ± 0.12 | ||||||||
| Chung et al., 2004 | 2 | - | 1 | 50 - | ERA®, Sterngold | Gold alloy | White | 23.76 ± 1.02 | |||
| Grey | 35.24 ± 1.99 | ||||||||||
| Locator®, Zest Anchors | Ti + TiN | Pink | 12.33 ± 1.28 | ||||||||
| White | 28.95 ± 0.78 | ||||||||||
| Jabbour et al., 2014 RCT/crossover | 2 | - | 6 months | Clinical conditions | Retentive anchor, Straumann | Ti | Gold matrix | 34.58 * | 24.58 * | 28.92 * | |
| 12 months | 20.27 * | 41.38 * | |||||||||
| 6 months | Locator®, Zest Anchors | Ti + TiN | White | - | 39.27 * | 15.47 * | 60.61 * | ||||
| 12 months | 12.00 * | 66.54 * | |||||||||
| Gonuldas et al., 2018 | 2 | 22 | 1 2160 IRC | 50 Dry | Ball, T.A.G. Medical Products | Ti | Orange plastic cap | 30.7 ± 2.82 | 21.64 ± 1.23 | 29.51 | |
| White plastic cap | 47.9 ± 2.62 | 26.24 ± 0.71 | 45.22 | ||||||||
| Locator®, Zest Anchors | Ti + TiN | Blue | 61.39 ± 4.26 | 5.87 ± 2.42 | 90.44 | ||||||
| Pink | 79.14 ± 3.63 | 10.4 ± 2.46 | 86.86 | ||||||||
| White | 93.75 ± 11.23 | 18.28 ± 2.25 | 80.50 | ||||||||
| Sultana et al., 2017 | 2 | 22 | 10 10,000 IRC | 45 Dry | Ball, Dentsply | Ti | Red plastic cap Clix® | - | 56.2 ± 6.12 | 46.0 ± 4.74 | 18.1 |
| Locator®, Zest Anchors | Ti + TiN | Pink | 108.9 ± 29.78 | 20.2 ± 5.74 | 81.5 | ||||||
| Green | 82.3 ± 14.15 | 17.3 ± 3.73 | 79.0 | ||||||||
| Türk et al., 2014 | 2 | 22 | 10 5000 IRC | 50 Dry | Ball, O-Ring®, Biohorizons | Ti | Plastic cap Clix® | - | 32.91 ± 5.30 | 9.70 ± 7.94 | 69.43 ± 27.61 |
| Locator®, Zest Anchors | Ti + TiN | Pink | - | 52.47 ± 6.70 | 21.70 ± 10.13 | 57.56 ± 21.65 | |||||
| Wolf et al., 2009 | 1 | - | 10 50,000 IRC | - Water | Ball, Dalbo Plus®, Cendres & Métaux | Gold alloy | Gold alloy strip | 7 | 8.86 ± 2.2 | 2.31 ± 1.0 | 77.54 |
| Ti | Gold alloy strip | 7 | 9.87 ± 1.6 | 11.61 ± 3.7 | −5.58 | ||||||
| Ball Ecco®, Unor | Gold alloy | Green plastic cap | 8 | 6.97 ± 4.6 | 1.13 ± 0.8 | 88.55 | |||||
| Ball Tima®, Unor | Gold alloy | Stainless steel ring | 8 | 11.92 ± 3.1 | 1.55 * ± 1.4 | 89.82 | |||||
| Ball, Pro-Snap®, Metalor Dental | Gold alloy | Green plastic cap | 10 | 8.52 ± 2.1 | 3.40 ± 1.5 | 54.23 | |||||
| Locator®, Zest Anchors | Ti + TiN | Pink | - | 13.250 ± 6.6 | 2.462 ± 1.8 | 85.66 | |||||
| Alsabeeha et al., 2010 | 1 | - | 10 IRC | 50 - | Ball Ø 2.25 mm, Southern | Ti | Gold alloy strip | - | 17.32 ± 3.68 | - | |
| Ball Ø 5.9 mm, Southern | Pure Ti + TiN | Plastic cap | - | 32.06 ± 2.59 | |||||||
| Locator®, Zest Anchors | Ti + TiN | Blue | - | 3.83 ± 0.64 | |||||||
| Pink | 9.40 ± 0.74 | ||||||||||
| White | 12.39 ± 0.55 | ||||||||||
| Yang et al., 2011 | 1 | - | 1 IRC | 60 - | Dal-ro®, Biomet 3i | Ti | Gold alloy strip | - | 6.48 ± 0.34 | ||
| Locator, Zest Anchors | Ti + TiN | Blue | - | 15.36 ± 1.4 | |||||||
| Abi Nader et al., 2011 | 2 | 15 | 1 400,000 CC | 15 Dry | Ball Ø 2.25 mm, Nobel Biocare | Ti | Gold alloy | 1 turn | 10.6 ± 3.6 | 7.9 ± 4.3 | 25.47 |
| Locator®, Zest Anchors | Ti + TiN | White | - | 66.4 ± 16.0 | 21.6 ± 17.0 | 67.47 | |||||
| Petropoulos et al., 2011 | 2 | - | 1 | 50.8 - | Ball Ø 3.5 mm, Nobel Biocare | Ti | Rubber O-ring® | - | 24.3 | ||
| Ball Ø 2.25 mm, Nobel Biocare | Ti | Ti cap/Ti spring | - | 17.8 | |||||||
| Zest®, Zest Anchors | - | - | - | 10.8 | |||||||
| ZAAG®, Zest Anchors | - | - | - | 37.2 | |||||||
| ERA®, Sterngold | - | White | - | 12.7 | |||||||
| Orange | 18.5 | ||||||||||
| Kobayashi et al., 2014 | 2 | 20 | 10 14,600 IRC | 4000 NaCl 0.9% | Retentive Anchor, Straumann | Ti | Gold alloy | 7 (0.5 turn) | 40.3 ± 15.83 | 67.9 * ± 15.83 | −68.48 (ns) |
| Locator®, Zest Anchors | Ti + TiN | Blue | - | 33.5 ± 9.77 | 24.57 ± 12.35 | 26.66 | |||||
| Saheli et al., 2019 | 2 | 19 | 1 1440 IRC | 50 - | Ball, Dio Implant, Dio Corp | Ti | - | - | 15.6 | 9.3 | 40.38 |
| 23 | 15.3 | 8.0 | 46.20 | ||||||||
| 29 | 13.8 | 10.2 | 26.07 | ||||||||
| 19 | Locator®, Zest Anchors | Ti + TiN | - | - | 17.1 | 5.2 | 69.59 | ||||
| 23 | 33.5 | 8.0 | 76.12 | ||||||||
| 29 | 33.1 | 6.8 | 79.46 | ||||||||
| Scherer et al., 2014 | 2 | Inter-canine | 1 IRC | 50.8 | Ball, Zimmer Dental | Ti | White cap | - | 35.23 | - | |
| Ball O-ring® Saturno Standard, Zest Anchors | Ti | Rubber ring | 13.13 | ||||||||
| ERA®, Sterngold | - | Orange | 9.36 | ||||||||
| Locator®, Zest Anchors | Ti + TiN | Pink | 26.64 | ||||||||
| Rutkunas et al., 2011 | 1 | 1 15,000 IRC | 50 Demineralized water | OP Anchor®, Inoue A. Co. Ltd. | Gold alloy | Rubber ring | - | 3.15 ± 0.6 | 3.70 ± 0.2 | −17.4 | |
| ERA®, Sterngold | Gold alloy | White | - | 13.12 ± 3.3 | 2.89 ± 0.7 | 87 | |||||
| Orange | 12.63 ± 1.4 | 2.86 ± 0.5 | 88 | ||||||||
| Locator® Root, Zest Anchors | Stainless steel + TiN | Blue | 16.50 ± 9.4 | 6.24 ± 6.1 | 62.18 | ||||||
| Pink | 15.20 ± 6.9 | 11.95 ± 3.5 | 21.38 | ||||||||
| White | 16.61 ± 2.2 | 10.28 ± 3.9 | 38.11 | ||||||||
| Clinical Studies Types Follow-Up | Attachment Systems (Male Part/Female Part/Manufacturer) | 1 or 2-IRMO | Number of Patients | Maintenance of the Attachment System | Maintenance of the Overdenture | Total Number of Events | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Activated RD | Replaced RD | Replaced Matrix Housing | Tightened or Replaced Patrix | Relined Denture | Fracture or Occlusal Adjustment | Replaced Denture | |||||
| Cune et al., 2004 Prospective 1 year | Titanium ball/Gold alloy RD/Friadent, Mannheim, Germany | 2 | 18 | 7 | - | 1 | 1+4 | nc | nc | nc | 13 |
| Mackie et al., 2011 RCT 8 years | Titanium ball Ø 2.25-mm/Gold RD/Straumann, Basel, Switzerland | 2 | 17 | 9.6 ± 13.5 | 1.1 ± 3.2 | nc | nc | nc | nc | nc | 3.9 ± 2.1 |
| Titanium ball Ø 2.25-mm/Gold RD/Brånemark, Nobel Biocare | 10 | 18.0 ± 19.8 | 5.5 ± 7.7 | nc | nc | nc | nc | nc | 28.8 ± 12.6 | ||
| Titanium ball Ø 2.25-mm/Gold-platinum RD/Southern Implants | 11 | 11.9 ± 11.8 | 2.2 ± 4.4 | nc | nc | nc | nc | nc | 16.4 ± 7.5 | ||
| Titanium ball Ø 2.25-mm/Titanium RD/Straumann, Basel, Switzerland | 9 | - | 13.7 ± 14.7 | nc | nc | nc | nc | nc | 24.9 ± 10.7 | ||
| Titanium ball Ø 3.95-mm/Plastic RD/Southern Implants | 22 | - | 4.3 ± 7.6 | nc | nc | nc | nc | nc | 8.7 ± 4.2 | ||
| Titanium ball Ø 2.2-mm/Rubber ring RD/Steri-Oss (Locator®/Zest Anchors after 6 years) | 21 | - | 29.2 ± 24.3 | nc | nc | nc | nc | nc | 32.2 ± 14.5 | ||
| Nogueira et al., 2018 Prospective 2 years | Nitrite-coated titanium ball/Nylon RD/Neodent, Curitiba, Paraná, Brazil Titanium ball/Rubber ring/Conexão Sistemas de Prótese, Arujá, Brazil | 1 | 45 | - | 66 | 12+7 | 7+6 | 3 | 23 | nc | 124 |
| Passia et al., 2019 Prospective 10 years | Titanium ball, Camlog Biotechnologies, Switzerland/Gold RD, Dalbo- Plus Elliptic, Cendres & Métaux, Biel, Switzerland | 1 | 11 | 29 | 23 | nc | 5+4 | 14 | 8 | nc | 83 |
| Walton et al., 2009 RCT 1 year | Titanium retentive anchor/Gold RD/Straumann, Basel, Switzerland | 1 | 42 | 37 | 4 | 0 | 5 | 60 | 4+5+2 | nc | 159 |
| 2 | 44 | 34 | 4 | 2 | 1 | 44 | 2+2 | nc | 81 | ||
| Alsabeeha et al., 2011b RCT 1 year | Uncoated standard titanium ball Ø 2.25-mm/Dalla Bona–type Gold alloy RD/Southern Implants | 1 | 12 | 13 | 0 | nc | 0+2 | nc | nc | nc | 15 |
| Titanium nitride–coated ball Ø 5.9-mm/Plastic cap RD/Southern Implants | 12 | - | 2 | nc | 0 | nc | nc | nc | 2 | ||
| Titanium nitride–coated abutment/Blue nylon cap RD/Locator®, Zest Anchors, Escondido, CA, USA | 12 | - | 16 | nc | 0 | nc | nc | nc | 16 | ||
| Cristache et al., 2014 RCT 5 years | Titanium retentive anchor, H 3.4 mm/Gold RD Elitor®/Straumann, Basel, Switzerland | 2 | 12 | 144 | 8 | nc | 1 | 4 | 2+0 | 2 | 161 |
| Titanium retentive anchor H 3.4 mm/Titanium RD and stainless steel spring, 6.86–10.79 N/Straumann, Basel, Switzerland | 11 | - | 0 | 0 | 2 | 2 | 1+0 | 1 | 6 | ||
| Titanium nitride–coated abutment H 3 mm/Pink nylon cap/Locator®, Zest Anchors, Inc., Escondido, CA, USA | 23 | - | 22 | nc | 0 | 1 | 0 | 1 | 24 | ||
| Kleis et al., 2010 RCT 1 year | Dal-Ro®, Biomet 3i Implant Innovations, Palm Beach Gardens, FL, USA | 2 | 25 | 4 | 0 | 0 | 1 | nc | 1 | nc | 6 |
| TG-O-Ring® ball/Rubber ring RD/ Cendres & Metaux SA, Biel-Bienne, Switzerland | 8 | - | 10 | 3 | 1 | nc | 0 | nc | 14 | ||
| Locator®, Zest Anchors, Escondido, CA, USA | 23 | - | 24 | 4+4 | 2 | nc | 1 | nc | 35 | ||
| Krenmair et al., 2012 RCT/crossover 1 year | Ball abutment/Gold RD/Camlog, Screw-line, Altatec) | 2 | 10 | 2 | 0 | nc | 1+1 | 5 | 0+1 | 0 | 10 |
| Locator® abutment/Pink RD/Zest Anchors, Inc., Escondido, CA, USA | 9 | - | 4 | nc | 1 | 4+1 | 1 | 0 | 11 | ||
| Studies Types 1- or 2-IRMO Follow-up | Attachment System, Manufacturer | Number of AS | Assessed Parameters/Methods | Results and Location | |
|---|---|---|---|---|---|
| Patrix | Matrix | ||||
| Alsabeeha et al., 2011b RCT 1-IRMO 1 year | Titanium nitride–coated ball Ø 5.9-mm/Plastic cap RD/Southern Implants | 5/12 | Wear patterns/SEM Composition of particles/Energy dispersive spectrometer | Unaffected | Slight signs of wear |
| Uncoated standard titanium ball Ø 2.25-mm/Dalla Bona–type Gold alloy RD/Southern Implants | 5/12 | Extensive material loss and abrasion along the path of insertion–removal and across the circumference | Extensive plastic deformation, material flaking and sloughing | ||
| Titanium nitride–coated abutment/Blue nylon cap RD/Locator®, Zest Anchors | 5/12 | Unaffected | Surface rupture and material loss (central core) | ||
| Fromentin et al., 2011a Retrospective clinical study 2-IRMO 8 years | Titanium ball anchor/Gold alloy RD Elitor®/Straumann | 144 (male and female parts) | Wear patterns/SEM Composition of particles/Energy dispersive spectrometer | Year 1: Slight scratches only at the equator Year 3: Slightly deformed profile, scratches at the equator and the summit Year 8: deformed and off-center ball | Year 1: Roughening, and material loss in the form of flakes Year 3: Blunt and deformed lamellae edge along their entire length Year 8: Fatigue cracks or fracture, increased matting of the inner surface, welding of the lamellae |
| Fromentin et al., 2011b Retrospective clinical study 2-IRMO 8 years | Titanium ball anchor (Ø 2262 to 2267 µm)/Gold alloy RD/Straumann, Basel, Switzerland | 69 patrices + 10 controls | Measure of ball Ø, calculation of Ø loss and deviation from circularity in 3 different axes (Vertical V, Mesio-Distal MD, Bucco-Lingual BL)/Coordinate measuring machine with a touch trigger probe | Year 1 (24 AS): Ø 5 to 7 µm (20–23%). Significant more loss in BL but no significant difference in Ø reduction Year 3 (29 AS): Ø 19 to 22 µm (61–91%), significant more loss in BL, 90% at the equator Year 8 (16 AS): Ø 22 to 31 µm. Significant more loss in BL and V | |
| Fromentin et al., 2012 Retrospective clinical study 2-IRMO 8 years | Titanium ball anchor, Straumann AG, Basel, Switzerland/Gold alloy RD (Ø 2973/2214/2300 µm, E 380/336 µm), Cendres+Metaux, Biel, Switzerland | 70 matrices + 10 controls | Measure of the external, internal upper and internal lower matrix Ø and deviations from circularity. Calculation of the upper and lower thickness (E) and the thickness loss of the lamellae tip/Coordinate measuring machine with a touch trigger probe | Year 1 (26 AS): Ø 2989/2232/2298 µm; E 373/342 µm, loss 7 µm. Significant increase of the internal upper Ø, no difference of deviation of circularity in the 3 different areas Year 3 (28 AS): Ø 2937/2282/2309 µm, E 33/316 µm, loss 47 µm. Year 8 (16 AS): Ø 2944/2304/2307 µm, E 310/308 µm, loss 70 µm. In years 3 and 8: increase of the internal upper Ø while the external Ø were significantly lower. Significant increase of deviation from circularity | |
| Jabbour et al., 2014 RCT/Crossover 2-IRMO 1 year x2 | Retentive Anchor/Gold RD/Straumann, Burlington, ON, Canada | 48 | Wear patterns/SEM | No significant scratches, minor flattening (equatorial zone) | nc |
| Locator® abutment/White nylon RD/Zest Anchors, Escondido, CA, USA | 48 | Wear patterns/SEM + high-resolution µCT | No significant scratches and spots | Significant wear and plastic deformation (peripheral notch edge, central core edge) | |
| Abi Nader et al., 2011 In vitro 2-IRMO 400,000 CC (1 year) Dry condition | Titanium ball/Gold lamellae RD/Nobel Biocare | 4/16 | Wear patterns/SEM | Discrete wear (top and lateral zone part of ball) | Slight wear and discrete deformation, probably due to the activator tool (internal surfaces, corners of retentive lamellae) |
| Titanium nitride-coated abutment/nylon RD/Locator®, Zest Anchors, Escondido, CA, USA | 4/16 | Deformation possibly caused by the specific tool (inner surface of the retentive area) | Severe wear (central core and periphery) | ||
| Choi et al., 2018 In vitro 2-IRMO 400,000 CC and 1080 IRC (1 year) Deionized water | Pure titanium abutment/Green, Red, Light Green and Blue PEEK RD/CM Loc®, Cendres & Métaux | 1/20 | Wear patterns/SEM | No noticeable abrasion | Slight wear, probably from tools used for placement (top and along the vertical split) |
| Titanium nitride–coated abutment/Blue, Pink and White nylon cap RD/Locator®, Zest Anchors | 1/20 | No noticeable abrasion | Severe wear, plastic deformation, surface irregularities, loss of materials more than PEKK RD (retention area, top of central core and periphery) | ||
| Gamborena et al., 1997 In vitro 1-IRMO 5500 IRC (3 years) Water | White, Orange, Blue and Grey RD/ERA®, APM-Sterngold | 3/5 | Wear patterns and dimensional Ø changes (top and middle part of central core, metal inner ring of matrix housing)/Traveling three-dimensional microscope | No difference between new and worn matrix housing. Ø loss of central core: −1.80 to +3.54%. The difference (statistical) in Ø between the matrix housing and the middle portion of the RD ranged from 72 to 126 µm | |
| Rabbani et al., 2015 In vitro 2-IRMO 2160 IRC (nc) Artificial saliva | Blue, Pink and White RD/Locator®, Zest Anchors, Inc., Escondido, CA | 30 | Wear patterns/SEM | nc | Significant wear (retention area, central core, periphery) |
| Rutkunas et al., 2011 In vitro 1-IRMO 15,000 IRC (nc) Demineralized water | Gold alloy ball/rubber ring/OP Anchor®, Inoue Attachments Co., Tokyo, Japan | 2/5 | Wear patterns and dimensional changes/SEM | No Ø loss: 0.52% | |
| Gold alloy abutment/nylon RD (Orange, White)/ERA®, Sterngold, Attleboro, USA | 2/5 | Ø loss: 0 to 2.48%, smooth surfaces (central core and inner peripherical surface) | |||
| Stainless steel TiN coated abutment/nylon RD (Blue, Pink, White), Locator® Root, Zest Anchors, Escondido, USA | 2/5 | Ø loss: 0.22 to 5.34%, surface particle loss and irregular surface (central core and inner peripherical) | |||
| Stephens et al., 2014 In vitro 5500 IRC (nc) Artificial saliva | Blue RD/Locator®, Zest Anchors, Inc., Escondido, CA | 20 | Wear patterns/SEM | No visible wear | Severe wear (central core > matrix housing) |
| Türk et al., 2014 In vitro 5000 IRC (nc) | Ball abutment/Rubber ring RD/O-Ring®, Biohorizons | 10 | Dimensional changes (outer and inner diameters of the abutments)/SEM | nc | Ø loss: outer (0.14 ± 0.07mm) and inner (0.08 ± 0.08 mm) |
| Locator®, Zest Anchors, Inc., Escondido, CA | 10 | nc | Ø loss: outer (0.17 ± 0.11 mm), inner: 0.11 ± 0.14 mm. No significant difference between the two AS | ||
| Wolf et al., 2009 In vitro 1-IRMO 50,000 IRC (nc) Water | Precious alloy ball/Titanium matrix housing with precious alloy RD/Dalbo-Plus®, Cendres & Metaux | 1 | Wear patterns/SEM | Noticeable signs of abrasion | nc |
| Titanium ball/Titanium matrix housing with precious alloy RD/Straumann | 1 | Slight grooves at the equator without any measurable changes in Ø | Minor wear at the tips of the metal lamellae | ||
| Precious alloy ball/Titanium matrix housing with Green plastic RD/Ecco®, Unor | 1 | Large grooves at the equator without any Ø loss | Obvious damages | ||
| Precious alloy ball/Titanium matrix housing with stainless steel spring/Tima®, Unor | 1 | Extensive signs of wear at the equators with Ø loss | Fractures of the retention springs | ||
| Precious alloy ball/Titanium matrix housing with Red plastic RD/Pro-Snap®, Metalor | 1 | Little signs of abrasion at the equator | nc | ||
| Titanium-nickel coating abutment/Stainless steel housing with Pink RD/Locator®, Zest Anchor | 1 | Little abrasion at the equator | Considerable signs of wear | ||
| Yabul et al., 2018 In vitro 2-IRMO 5000 IRC (4.5 years) | Ball/Gold RD/Straumann AG, Basel, Switzerland | 24 | Wear patterns and volumetric loss of ball/Three-dimensional laser scanner | 0.7 ± 0.47% | |
| Ball/Titanium RD/Straumann AG, Basel, Switzerland | 24 | 25.38 ± 5.41% | |||
| Ball/Plastic RD/Biohorizons, Birmingham, Alabama | 24 | 12.94 ± 1% | |||
| Ball/Plastic RD/DTI, Istanbul, Turkey | 24 | 10.47 ± 1.7% | |||
| In Vitro Studies | 1 or 2 IRMO | Inter-implant Distance (mm) | Angulation | Initial and Final Number and Type of Cycles | Cross-Head Speed (mm/min) | Medium | Attachment Systems/Retentive Device | Implant Angulation α (°) | Retention Force (N) | Retention Loss (%) | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Initial | Final | ||||||||||
| Ortégon et al., 2009 | 2 | 20 | Distal | 1 3500 IRC | 50 | nc | Ball Astra-Tech/PreciClix® RD | 0 (0 RD) | nc | 20.11 ± 2.51 | nc |
| 10 (0 RD) | nc | 21.31 ± 1.79 | nc | ||||||||
| 15 (0 RD) | nc | 18.73 ± 4.14 | nc | ||||||||
| 10 (10 RD) | nc | 19.93 ± 1.38 | nc | ||||||||
| 15 (15 RD) | nc | 16.84 ± 1.77 | nc | ||||||||
| Elsyad et al., 2018 | 2 | 22 | Mesial | 1 540 IRC | 50 | nc | Locator®/Blue | 0 | 20.63 ± 0.70 | 3.52 ± 0.46 | 82.94 |
| 5 | 15.90 ± 0.65 | 24.02 ± 0.97 | 51.07 | ||||||||
| 10 | 28.07 ± 1.01 | 26.28 ± 0.62 | 63.77 | ||||||||
| 20 | 47.44 ± 0.51 | 30.56 ± 0.51 | 35.58 | ||||||||
| Locator®/Pink | 0 | 40.07 ± 0.90 | 19.15 ± 0.78 | 52.21 | |||||||
| 5 | 30.13 ± 0.82 | 31.23 ± 0.68 | −3.65 | ||||||||
| 10 | 31.57 ± 0.51 | 16.16 ± 1.04 | 48.81 | ||||||||
| 20 | 56.18 ± 0.75 | 36.45 ± 1.50 | 35.12 | ||||||||
| Locator®/White | 0 | 49.20 ± 0.72 | 32.01 ± 0.01 | 34.94 | |||||||
| 5 | 40.26 ± 1.10 | 41.14 ± 1.03 | −2.18 | ||||||||
| 10 | 41.06 ± 1.00 | 19.05 ± 0.93 | 53.60 | ||||||||
| 20 | 57.28 ± 0.63 | 19.99 ± 1.00 | 65.10 | ||||||||
| Elsyad et al., 2019 | 2 | 22 | Distal | 1 540 IRC | 50 | nc | Locator®/Blue | 0 | 20.63 ± 0.70 | 3.52 ± 0.47 | 82.94 |
| 5 | 15.29 ± 0.61 | 9.13 ± 0.81 | 40.29 | ||||||||
| 10 | 30.16 ± 1.25 | 2.97 ± 1.05 | 90.15 | ||||||||
| 20 | 17.08 ± 0.88 | 30.26 ± 0.65 | −77.17 | ||||||||
| Locator®/Pink | 0 | 40.07 ± 0.90 | 19.15 ± 0.78 | 51.40 | |||||||
| 5 | 34.60 ± 0.53 | 16.31 ± 1.14 | 52.86 | ||||||||
| 10 | 47.10 ± 0.85 | 9.11 ± 1.02 | 80.66 | ||||||||
| 20 | 39.12 ± 1.02 | 21.10 ± 1.01 | 46.06 | ||||||||
| Locator®/White | 0 | 48.20 ± 0.72 | 32.02 ± 1.00 | 33.57 | |||||||
| 5 | 43.13 ± 1.20 | 44.01 ± 1.00 | −2.04 | ||||||||
| 10 | 49.25 ± 1.39 | 40.18 ± 1.05 | 18.42 | ||||||||
| 20 | 40.30 ± 1.13 | 41.32 ± 1.50 | −2.53 | ||||||||
| Locator®/Green | 20 | 27.50 ± 0.50 | 15.42 ± 0.52 | 43.93 | |||||||
| Locator®/Red | 20 | 38.23 ± 1.08 | 20.14 ± 1.03 | 47.32 | |||||||
| Rabbani et al., 2015 | 2 | 23 | Mesial | 1 2160 IRC | nc | nc | Locator®/Blue | 0/0 | 77 ± 13.5 | 25.8 ± 5.2 | 65.5 ± 10.2 |
| 0/10 | 66.4 ± 26.7 | 14.7 ± 7.9 | 70.6 ± 22.9 | ||||||||
| 5/5 | 73.7 ± 10.1 | 18.4 ± 3.7 | 74.1 ± 7.9 | ||||||||
| Locator®/Pink | 0/0 | 72.7 ± 1.3 | 27.7 ± 8.2 | 62.1 ± 10.7 | |||||||
| 0/10 | 74.8 ± 6.7 | 31.3 ± 4.1 | 35.1 ± 2.4 | ||||||||
| 5/5 | 71.4 ± 3.4 | 29.4 ± 2.7 | 30.2 ± 2.7 | ||||||||
| Locator®/White | 0/0 | 83.8 ± 10.9 | 32.0 ± 10.7 | 62.1 ± 9.6 | |||||||
| 0/10 | 101.32 ± 12.0 | 35.1 ± 2.4 | 65.1 ± 4.2 | ||||||||
| 5/5 | 89.5 ± 15.7 | 30.2 ± 2.7 | 65.1 ± 9.4 | ||||||||
| Stephens et al., 2014 | 2 | 22 | Distal | 1 5500 IRC | 60 | Artificial saliva | Locator®/Blue | 0 | 21.81 ± 7.44 | 15.97 ± 3.96 | 26.78 |
| 5 | 30.03 ± 6.24 | 15.43 ± 1.59 | 48.62 | ||||||||
| 10 | 24.75 ± 6.83 | 14.22 ± 2.43 | 42.54 | ||||||||
| Al-Ghafi et al., 2009 | 2 | 15 | nc | 1 14,400 IRC | nc | nc | Locator®/Green | 0 | 81.75 | nc | nc |
| 5 | 91.74 | nc | nc | ||||||||
| 10 | 104.72 | nc | nc | ||||||||
| 15 | 84.86 | nc | nc | ||||||||
| 20 | 78.04 | nc | nc | ||||||||
| Passia et al., 2016 | 1 | - | nc | 10 30,000 IRC | nc | Water | Locator®/Green | 0 | 21.5 | nc | 66 |
| 20 | 24.4 | nc | 75 | ||||||||
| CM Loc®/Green | 0 | 22.5 | nc | 32 | |||||||
| 20 | 27.4 | nc | 47 | ||||||||
| Choi et Jeong, 2018 | 2 | 22 | Distal | 1 400,000 CC & 1080 IRC | 50 | Deionized water | Locator®/Blue | 0 | 20.1 ± 2.87 | 20.58 ± 3.09 | −2.81 ± 4.07 |
| 10 | 22.94 ± 1.48 | 25.03 ± 2.59 | −8.93 ± 5.99 | ||||||||
| Locator®/Pink | 0 | 24.55 ± 2.14 | 37.42 ± 2.79 | −52.78 ± 7.78 | |||||||
| 10 | 47.13 ± 8.96 | 30.33 ± 4.18 | 34.77 ± 6.82 | ||||||||
| Locator®/White | 0 | 69.87 ± 5.73 | 42.56 ± 3.27 | 38.81 ± 5.32 | |||||||
| 10 | 56.86 ± 4.44 | 39.55 ± 2.95 | 30.19 ± 5.50 | ||||||||
| CM Loc®/Green (extralight) | 0 | 12.45 ± 1.27 | 12.83 ± 1.39 | −3.01 ± 1.92 | |||||||
| 10 | 12.11 ± 1.28 | 15.52 ± 1.41 | −30.52 ± 23.84 | ||||||||
| CM Loc/Red (light) | 0 | 17.79 ± 1.70 | 21.48 ± 1.20 | −22.31 ± 17.18 | |||||||
| 10 | 27.63 ± 2.28 | 26.74 ± 2.42 | 3.25 ± 2.69 | ||||||||
| CM Loc®/Green (medium) | 0 | 39.35 ± 3.45 | 36.99 ± 1.75 | 5.57 ± 5.28 | |||||||
| 10 | 46.96 ± 1.70 | 43.84 ± 1.99 | 6.55 ± 5.01 | ||||||||
| CM Loc®/Blue (high) | 0 | 44.07 ± 3.07 | 43.80 ± 2.45 | 0.52 ± 1.92 | |||||||
| 10 | 45.73 ± 4.29 | 39.44 ± 8.23 | 14.69 ± 11.22 | ||||||||
| Manie wicz et al., 2020 | 2 | 20 | Mesial | 1 10,000 IRC | nc | Artificial saliva | CM Loc®/Red (light) | 0 | 81.8 ± 18.5 | 49.2 ± 12.6 | 39.85 |
| 10 | 47.1 ± 8.6 | 42.4 ± 13.5 | 9.99 | ||||||||
| 20 | 47.4 ± 8.9 | 35.4 ± 9.6 | 25.32 | ||||||||
| 30 | 44.4 ± 10.8 | 41.2 ± 14.8 | 7.21 | ||||||||
| Novaloc®/Yellow | 0 | 57.7 ± 31.0 | 59.4 ± 16.0 | −2.95 | |||||||
| 10 | 41.8 ± 14.8 | 54.4 ± 15.8 | −30.14 | ||||||||
| 20 | 48.9 ± 13.9 | 52.6 ± 8.4 | −7.57 | ||||||||
| 30 | 76.6 ± 44.5 | 47.7 ± 18.6 | −37.73 | ||||||||
| Locator R-Tx®/Pink (medium) | 0 | 75.5 ± 24.9 | 60.0 ± 19.6 | 20.53 | |||||||
| 10 | 66.3 ± 16.9 | 45.5 ± 11.9 | 31.37 | ||||||||
| 20 | 62.3 ± 22.1 | 33.6 ± 11.4 | 46.07 | ||||||||
| 30 | 78.6 ± 33.3 | 29.9 ± 18.1 | 61.96 | ||||||||
| Yilmaz et al., 2020 | 2 | nc | Distal | 1 1440 IRC | 50 | nc | Locator®/Pink | 0/0 | 13.6 | 10.0 | 26.5 |
| 0/30 | 18.3 | 12.8 | 30.0 | ||||||||
| 30/30 | 50.2 | 21.7 | 56.8 | ||||||||
| Locator R-Tx®/Pink | 0/0 | 20.1 | 14.0 | 30.3 | |||||||
| 0/30 | 17.5 | 10.6 | 39.4 | ||||||||
| 30/30 | 33.3 | 20.0 | 39.9 | ||||||||
| Yang et al., 2011 | 1 | nc | 1 IRC | 60 | nc | Dal-ro®/Gold alloy strip | 0 | 6.48 ± 0.34 | |||
| 15 | 6.25 ± 0.2 | ||||||||||
| 30 | 5.76 ± 0.16 | ||||||||||
| 45 | 4.75 ± 0.92 | ||||||||||
| Locator®/Blue | 0 | 15.36 ± 1.4 | |||||||||
| 15 | 14.67 ± 0.74 | ||||||||||
| 30 | 13.3 ± 1.7 | ||||||||||
| 45 | 6.58 ± 0.34 | ||||||||||
| Sultana et al., 2017 | 2 | 22 | Distal | 10 10,000 IRC | 50 | Dry condition | Ball Dentsply/plastic Red Clix® | 0 | 56.2 ± 6.12 | 46.0 ± 4.74 | 18.1 |
| 20 | 45.7 ± 8.03 | 40.7 ± 2.88 | 10.9 | ||||||||
| Locator®/Pink | 0 | 108.9 ± 29.78 | 20.2 ± 5.74 | 81.5 | |||||||
| Locator®/Green | 20 | 82.3 ± 14.15 | 17.3 ± 3.73 | 79.0 | |||||||
| In Vitro Studies 1 or 2-IRMO | Cross-Head Speed (mm/min) | Immersion Time, Number and Type of Cycles | RD | Tap Water | Artificial Saliva | NaCl 0.9% | Cool Mint Listerine | NaOCl 6.15% | Aktident | Efferdent | Protefix | Corega | Polident | Polident Overnight |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sodium Chloride | Menthol Derivatives | Sodium Hypochlorite | Sodium Bicarbonate | Sodium Bicarbonate, Perborate, or Percarbonate, Sodium Carbonate, Potassium Monopersulfate, Citric Acid, EDTA… | ||||||||||
| Ayyıldız et al., 2020 2-IRMO | 2 50 | 12 M 1 IRC | Blue | 41.1 ± 3.9 N | 33.3 ± 4.7 N | 44.3 ± 4.1 N | 52.5 ± 5.9 N | |||||||
| Pink | 58.7 ± 6.5 N | 39.7 ± 3.8 N | 58.5 ± 4.3 N | 58.3 ± 6.8 N | ||||||||||
| White | 76.7 ± 8.4 N | 52.3 ± 8.5 N | 89.0 ± 8.7 N | 93.7 ± 5.8 N | ||||||||||
| Kürkcüoglu et al., 2016 1-IRM0 | 50 | 6 M 12 IRC | Blue | 22.1 ± 1.2 N | 10.4 ± 3.6 N | 7.7 ± 2.2 N | 13.8 ± 1.5 N | |||||||
| Pink | 27.3 ± 2.2 N | 29.2 ± 3.3 N | 25.5 ± 1.5 N | 27.6 ± 1.6 N | ||||||||||
| White | 36.7 ± 4.0 N | 38.3 ± 1.8 N | 23.5 ± 2.5 N | 33.6 ± 2.7 N | ||||||||||
| Nguyen et al., 2010 2-IRMO | 50 | 6 M 1 IRC | Pink | 45.3 ± 3.5 N | 51.1 ± 5.3 N | 7.8 ± 2.5 N | 40.8 ± 2.6 N | 45.0 ± 2.3 N | 45.0 ± 5.2 N | |||||
| Srinivasan et al., 2016 2-IRMO | 120 | 10 IRC 10,000 IRC | Blue | 35.6 ± 7.5 N 29.8 ± 11.1 N | 43.3 ± 16.0 N 37.5 ± 11.9 N | |||||||||
| You et al., 2011 1-IRMO | 50 | 6 M 1 IRC 548 IRC | Pink | 22.2 ± 2.3 N 10.5 ± 2.9 N 53 ±12% * | 22.3 ± 3.1 N 15.8 ± 4.7 N 29 ± 9% * | 12.6 ± 1.5 N 7.3 ± 1.0 N 42 ± 11% * | 21.5 ± 1.5 N 11.0 ± 2.2 N 49 ± 9% * | 21.8 ± 2.4 N 14.4 ± 3.6 N 34 ± 18% * | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wakam, R.; Benoit, A.; Mawussi, K.B.; Gorin, C. Evaluation of Retention, Wear, and Maintenance of Attachment Systems for Single- or Two-Implant-Retained Mandibular Overdentures: A Systematic Review. Materials 2022, 15, 1933. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15051933
Wakam R, Benoit A, Mawussi KB, Gorin C. Evaluation of Retention, Wear, and Maintenance of Attachment Systems for Single- or Two-Implant-Retained Mandibular Overdentures: A Systematic Review. Materials. 2022; 15(5):1933. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15051933
Chicago/Turabian StyleWakam, Raphaël, Aurélie Benoit, Kwamivi Bernardin Mawussi, and Caroline Gorin. 2022. "Evaluation of Retention, Wear, and Maintenance of Attachment Systems for Single- or Two-Implant-Retained Mandibular Overdentures: A Systematic Review" Materials 15, no. 5: 1933. https://0-doi-org.brum.beds.ac.uk/10.3390/ma15051933