
Repeated SARS-CoV-2 Positivity: Analysis of 123 Cases

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search and Selection
2.2. Data Extraction
2.3. Statistical Analysis
2.4. Data Quality
2.5. Assessment of Risk of Bias
3. Results
3.1. Characteristics of the Included Studies
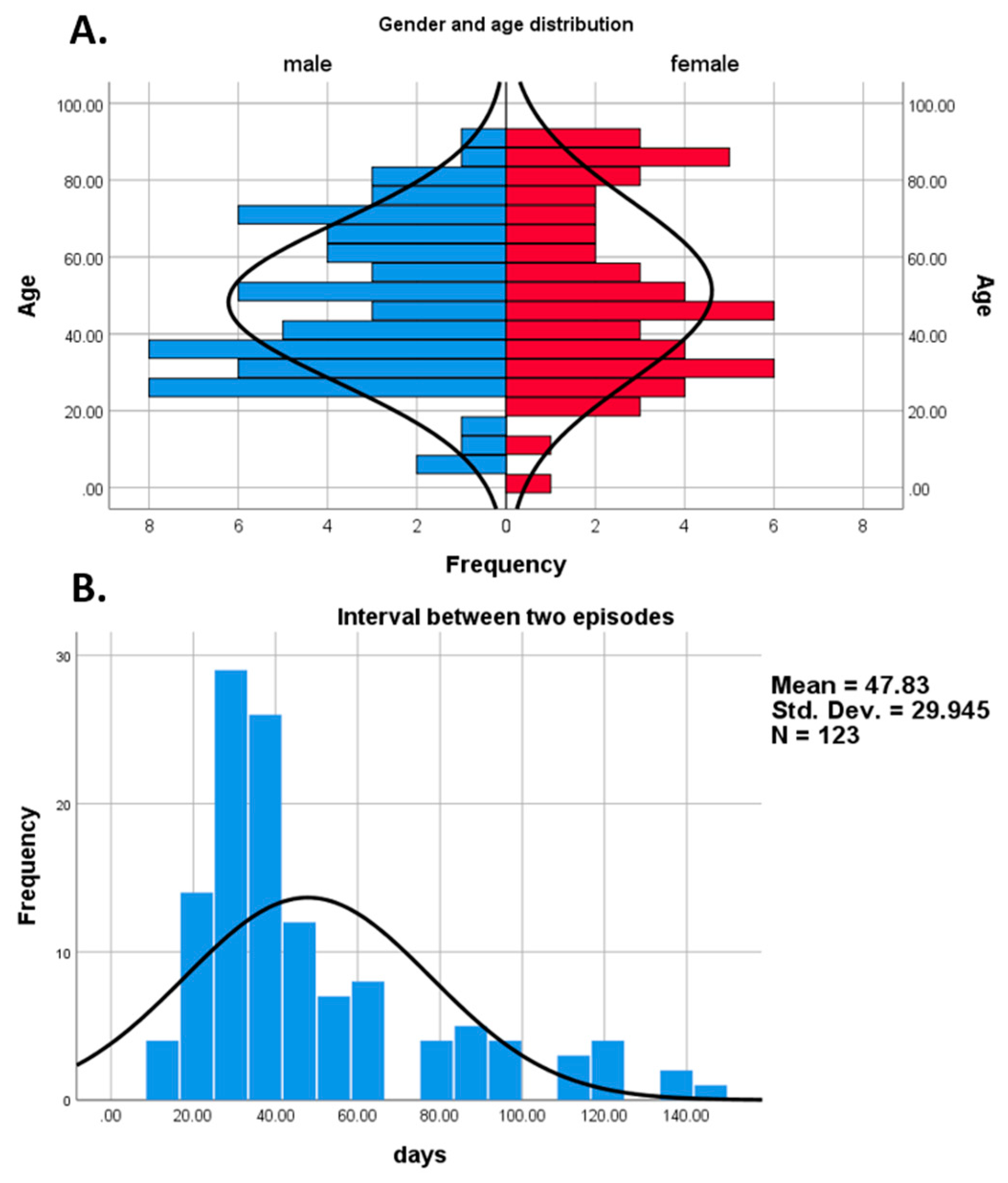
3.2. Characteristics of the Cohort
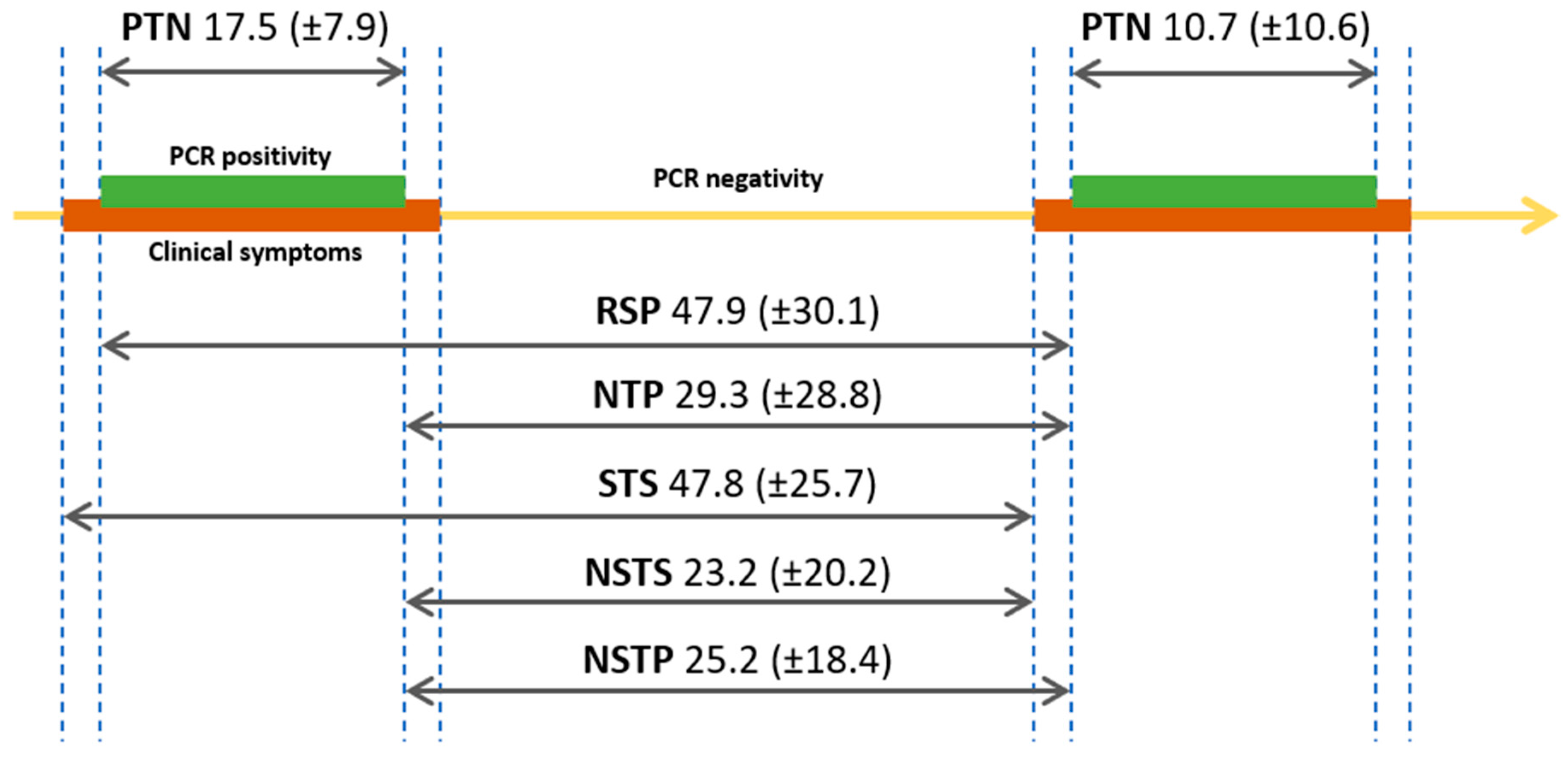
3.3. Length of Positivity and Intervals between Episodes
3.4. Comparing Patients with below and above 60 Days of RSP
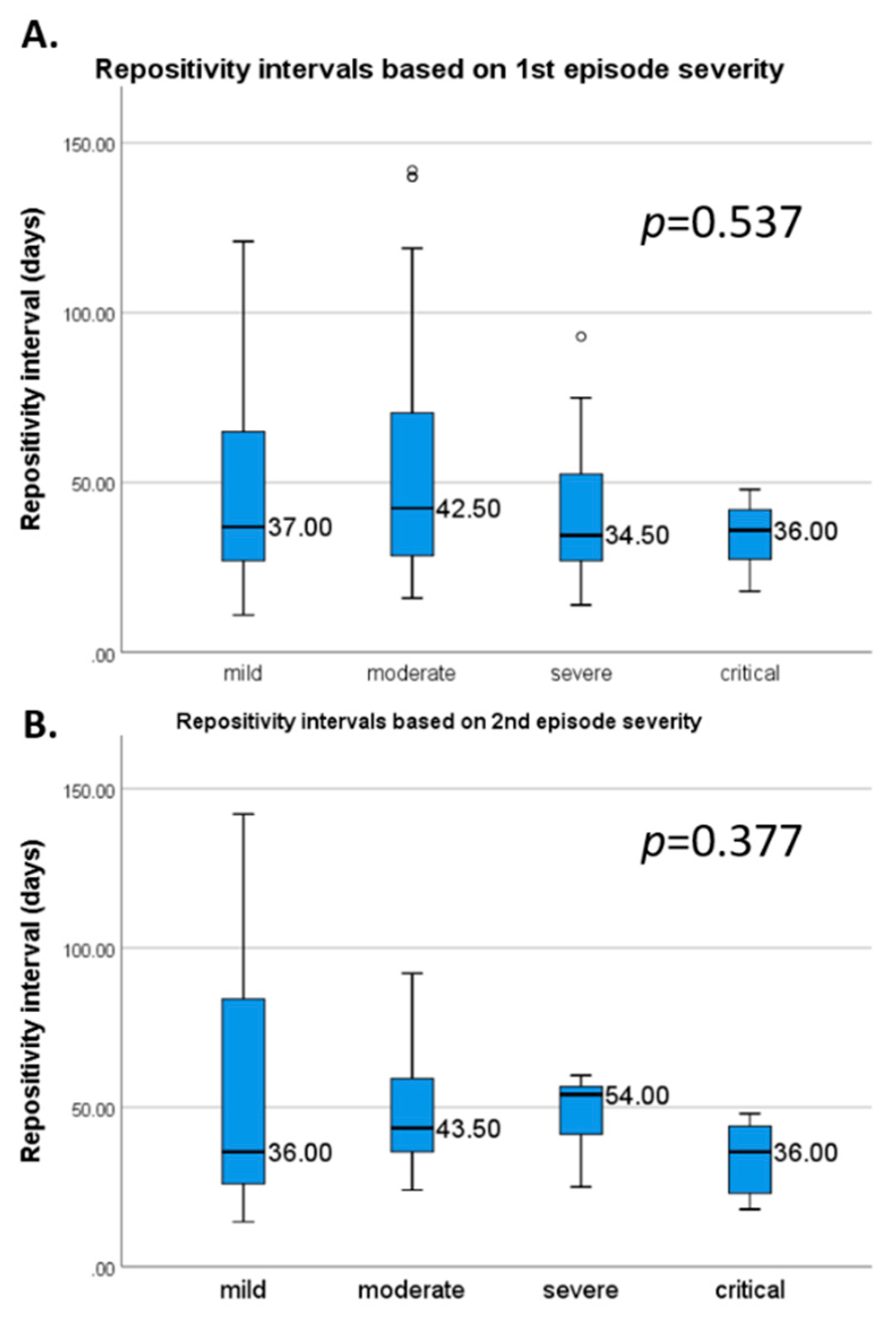
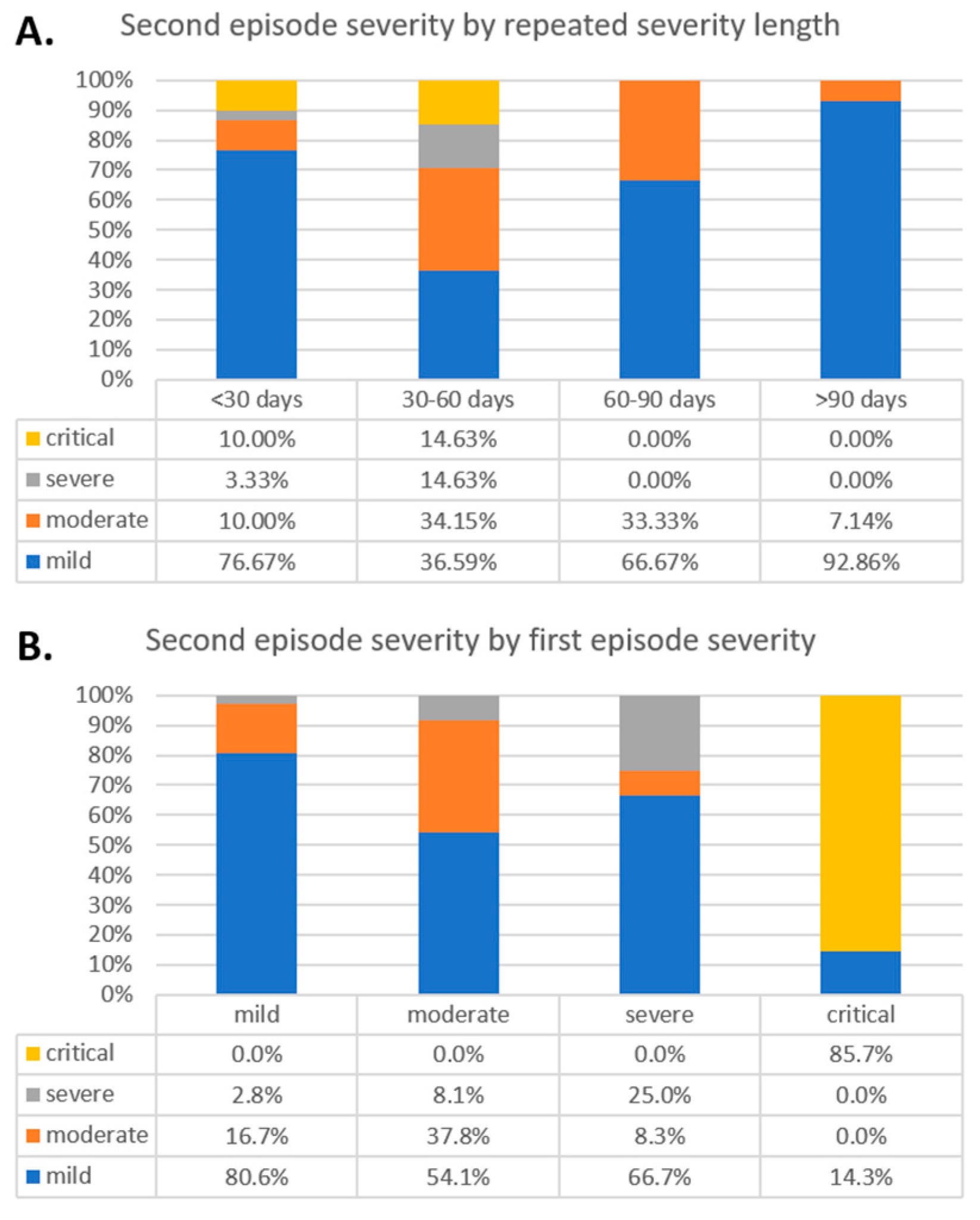
3.5. Comparison Based on Intervals
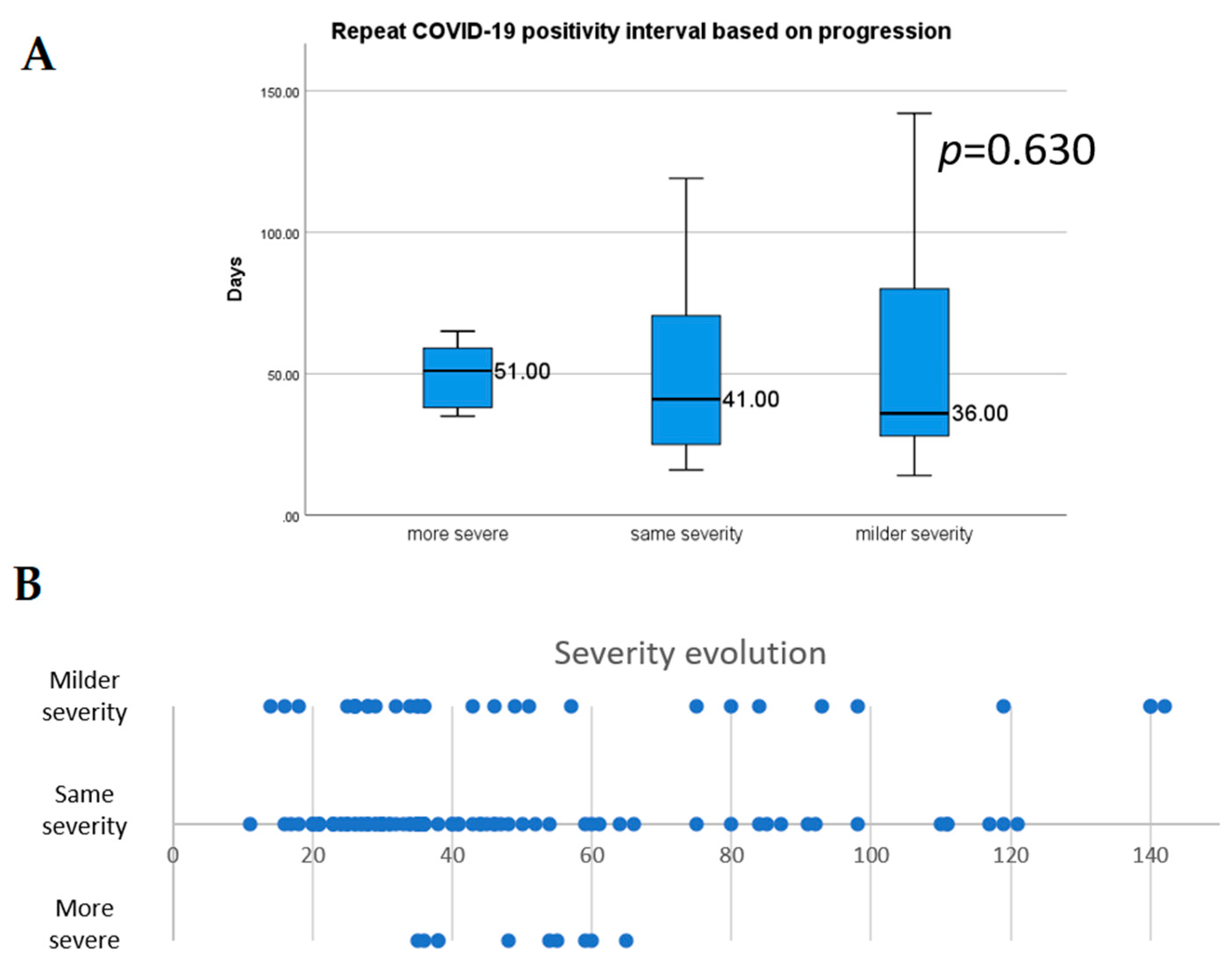
3.6. The Severity of the First and Second Episodes
3.7. Risk of Bias Assessment
4. Discussion
4.1. Strengths and Limitations
4.2. Implication for Research
4.3. Implication for Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- WHO. Coronavirus Disease (COVID-19). 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 2 February 2021).
- Lurie, N.; Saville, M.; Hatchett, R.; Halton, J. Developing Covid-19 Vaccines at Pandemic Speed. N. Engl. J. Med. 2020, 382, 1969–1973. [Google Scholar] [CrossRef] [PubMed]
- Dao, T.L.; Hoang, V.T.; Gautret, P. Recurrence of SARS-CoV-2 viral RNA in recovered COVID-19 patients: A narrative review. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 13–25. [Google Scholar] [CrossRef]
- Lu, J.; Peng, J.; Xiong, Q.; Liu, Z.; Lin, H.; Tan, X.; Kang, M.; Yuan, R.; Zeng, L.; Zhou, P.; et al. Clinical, immunological and virological characterization of COVID-19 patients that test re-positive for SARS-CoV-2 by RT-PCR. EBioMed 2020, 59, 102960. [Google Scholar] [CrossRef]
- ECDC. European Centre for Disease Prevention and Control. Reinfection with SARS-CoV: Considerations for Public Health Response. Available online: https://www.ecdc.europa.eu/en/publications-data/threat-assessment-brief-reinfection-sars-cov-2 (accessed on 25 January 2021).
- Van Elslande, J.; Vermeersch, P.; Vandervoort, K.; Wawina-Bokalanga, T.; Vanmechelen, B.; Wollants, E.; Laenen, L.; André, E.; Van Ranst, M.; Lagrou, K.; et al. Symptomatic SARS-CoV-2 reinfection by a phylogenetically distinct strain. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tillett, R.L.; Sevinsky, J.R.; Hartley, P.D.; Kerwin, H.; Crawford, N.; Gorzalski, A.; Laverdure, C.; Verma, S.C.; Rossetto, C.C.; Jackson, D.; et al. Genomic evidence for reinfection with SARS-CoV-2: A case study. Lancet Infect. Dis. 2021, 21, 52–58. [Google Scholar] [CrossRef]
- Lafaie, L.; Célarier, T.; Goethals, L.; Pozzetto, B.; Grange, S.; Ojardias, E.; Annweiler, C.; Botelho-Nevers, E. Recurrence or Relapse of COVID-19 in Older Patients: A Description of Three Cases. J. Am. Geriatr. Soc. 2020, 68, 2179–2183. [Google Scholar] [CrossRef] [PubMed]
- Murchu, E.O.; Byrne, P.; Walsh, K.A.; Carty, P.G.; Connolly, M.; De Gascun, C.; Jordan, K.; Keoghan, M.; O’Brien, K.K.; O’Neill, M.; et al. Immune response following infection with SARS-CoV-2 and other coronaviruses: A rapid review. Rev. Med. Virol. 2020, n/a, e2162. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, A. What reinfections mean for COVID-19. Lancet Infect. Dis. 2021, 21, 3–5. [Google Scholar] [CrossRef]
- Gidari, A.; Nofri, M.; Saccarelli, L.; Bastianelli, S.; Sabbatini, S.; Bozza, S.; Camilloni, B.; Fusco-Moffa, I.; Monari, C.; De Robertis, E.; et al. Is recurrence possible in coronavirus disease 2019 (COVID-19)? Case series and systematic review of literature. Eur. J. Clin. Microbiol. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Lumley, S.F.; O’Donnell, D.; Stoesser, N.E.; Matthews, P.C.; Howarth, A.; Hatch, S.B.; Marsden, B.D.; Cox, S.; James, T.; Warren, F.; et al. Antibody Status and Incidence of SARS-CoV-2 Infection in Health Care Workers. N. Engl. J. Med. 2020. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus Disease 2019 (COVID-19): A Perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef] [Green Version]
- Gagnier, J.J.; Kienle, G.; Altman, D.G.; Moher, D.; Sox, H.; Riley, D.; CARE Group. The CARE guidelines: Consensus-based clinical case reporting guideline development. J. Med. Case Rep. 2013, 7, 223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, J.; Ji, P.; Pang, J.; Zhong, Z.; Li, H.; He, C.; Zhang, J.; Zhao, C. Clinical characteristics of 3062 COVID-19 patients: A meta-analysis. J. Med. Virol. 2020, 92, 1902–1914. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yahav, D.; Yelin, D.; Eckerle, I.; Eberhardt, C.S.; Wang, J.; Cao, B.; Kaiser, L. Definitions for coronavirus disease 2019 reinfection, relapse and PCR re-positivity. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Sokolowska, M.; Lukasik, Z.M.; Agache, I.; Akdis, C.A.; Akdis, D.; Akdis, M.; Barcik, W.; Brough, H.A.; Eiwegger, T.; Eljaszewicz, A.; et al. Immunology of COVID-19: Mechanisms, clinical outcome, diagnostics, and perspectives-A report of the European Academy of Allergy and Clinical Immunology (EAACI). Allergy 2020, 75, 2445–2476. [Google Scholar] [CrossRef] [PubMed]
- Seow, J.; Graham, C.; Merrick, B.; Acors, S.; Steel, K.J.A.; Hemmings, O.; O’Bryne, A.; Kouphou, N.; Pickering, S.; Galao, R.P.; et al. Longitudinal evaluation and decline of antibody responses in SARS-CoV-2 infection. medRxiv 2020. [Google Scholar] [CrossRef]
- Elsayed, S.M.; Reddy, M.K.; Murthy, P.M.; Gupta, I.; Valiuskyte, M.; Sánchez, D.F.; Diaz, M.A.J.C. The Possibility and Cause of Relapse After Previously Recovering From COVID-19: A Systematic Review. Cureus 2020, 12. [Google Scholar] [CrossRef]
- Yuan, B.; Liu, H.-Q.; Yang, Z.-R.; Chen, Y.-X.; Liu, Z.-Y.; Zhang, K.; Wang, C.; Li, W.-X.; An, Y.-W.; Wang, J.-C.; et al. Recurrence of positive SARS-CoV-2 viral RNA in recovered COVID-19 patients during medical isolation observation. Sci. Rep. 2020, 10, 11887. [Google Scholar] [CrossRef] [PubMed]
- Arafkas, M.; Khosrawipour, T.; Kocbach, P.; Zielinski, K.; Schubert, J.; Mikolajczyk, A.; Celinska, M.; Khosrawipour, V. Current meta-analysis does not support the possibility of COVID-19 reinfections. J. Med. Virol. 2021, 93, 1599–1604. [Google Scholar] [CrossRef] [PubMed]
- CDC. Centers for Disease Control and Prevention: Common Investigation Protocol for Investigating Suspected SARS-CoV-2 Reinfection. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/reinfection.html (accessed on 25 January 2021).
- HPSC. Health Protection Surveillence Centre: Guidance on the Management of Weak Positive (High Ct Value) PCR Results in the Setting of Testing Individuals for SARS-CoV-2. Available online: https://www.hpsc.ie/a-z/respiratory/coronavirus/novelcoronavirus/guidance/outbreakmanagementguidance/ (accessed on 25 January 2021).
- Colson, P.; Finaud, M.; Levy, N.; Lagier, J.-C.; Raoult, D. Evidence of SARS-CoV-2 re-infection with a different genotype. J. Infect. 2020. [Google Scholar] [CrossRef]
- Goldman, J.D.; Wang, K.; Roltgen, K.; Nielsen, S.C.A.; Roach, J.C.; Naccache, S.N.; Yang, F.; Wirz, O.F.; Yost, K.E.; Lee, J.-Y.; et al. Reinfection with SARS-CoV-2 and Failure of Humoral Immunity: A case report. medRxiv 2020. [Google Scholar] [CrossRef]
- Mulder, M.; van der Vegt, D.S.J.M.; Oude Munnink, B.B.; GeurtsvanKessel, C.H.; van de Bovenkamp, J.; Sikkema, R.S.; Jacobs, E.M.G.; Koopmans, M.P.G.; Wegdam-Blans, M.C.A. Reinfection of Severe Acute Respiratory Syndrome Coronavirus 2 in an Immunocompromised Patient: A Case Report. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Tao, W.; Wang, X.; Zhang, G.; Guo, M.; Ma, H.; Zhao, D.; Sun, Y.; He, J.; Liu, L.; Zhang, K.; et al. Re-detectable positive SARS-CoV-2 RNA tests in patients who recovered from COVID-19 with intestinal infection. Protein Cell 2020. [Google Scholar] [CrossRef]
- To, K.K.-W.; Hung, I.F.-N.; Ip, J.D.; Chu, A.W.-H.; Chan, W.-M.; Tam, A.R.; Fong, C.H.-Y.; Yuan, S.; Tsoi, H.-W.; Ng, A.C.-K.; et al. Coronavirus Disease 2019 (COVID-19) Re-infection by a Phylogenetically Distinct Severe Acute Respiratory Syndrome Coronavirus 2 Strain Confirmed by Whole Genome Sequencing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Li, Q.; Zheng, X.-S.; Shen, X.-R.; Si, H.-R.; Wang, X.; Wang, Q.; Li, B.; Zhang, W.; Zhu, Y.; Jiang, R.-D.; et al. Prolonged shedding of severe acute respiratory syndrome coronavirus 2 in patients with COVID-19. Emerg. Microbes Infect. 2020, 9, 2571–2577. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, V.; Venkatakrishnan, A.J.; Puranik, A.; Kirkup, C.; Lopez-Marquez, A.; Challener, D.W.; Theel, E.S.; O’Horo, J.C.; Binnicker, M.J.; Kremers, W.K.; et al. Long-term SARS-CoV-2 RNA shedding and its temporal association to IgG seropositivity. Cell Death Discov. 2020, 6, 138. [Google Scholar] [CrossRef]
- Ra, S.H.; Lim, J.S.; Kim, G.-u.; Kim, M.J.; Jung, J.; Kim, S.-H. Upper respiratory viral load in asymptomatic individuals and mildly symptomatic patients with SARS-CoV-2 infection. Thorax 2021, 76, 61. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Li, F.; Chen, F.; Liu, H.; Zheng, J.; Lei, C.; Wu, X. Viral dynamics in asymptomatic patients with COVID-19. Int. J. Infect. Dis. 2020, 96, 288–290. [Google Scholar] [CrossRef] [PubMed]
- Mokhtar, K.M. Improved RT-PCR SARS-Cov2 results interpretation by indirect determination of cut-off cycle threshold value. medRxiv 2020. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Overall n/N (% Total) | ≤60 Days n/N (% Total) | >60 Days n/N (% Total) | p-Value |
|---|---|---|---|---|
| Total number N | 123 | 96 | 27 | |
| Female | 55/122 (45.1) | 42/96 (43.8) | 13/26 (50) | 0.570 |
| Age (mean, SD, range) | 49.7 (21.9) | 51 (22.3) | 45.2 (20.2) | 0.228 |
| Mean repeated positivity interval (SD) | 47.9 (30.1) | 34.1 (11.4) | 97 (24) | 0.001 |
| Comorbidities | ||||
| Hypertension | 22/82 (26.8) | 20/ 61 (32.8) | 2/ 21 (9.5) | 0.038 |
| Chronic heart disease | 14/84 (16.7 | 11/ 63 (17.5) | 3/ 21 (14.3) | 0.735 |
| Arrhythmia | 11/84 (13.1) | 8/ 63 (12.7) | 3/ 21 (14.3) | 0.852 |
| T2DM | 19/82 (23.2) | 15/ 61 (24.6) | 4/ 21 (19.1) | 0.604 |
| COPD | 6/82 (7.3) | 4/ 61 (6.6) | 2/ 21 (9.5) | 0.653 |
| Chronic kidney disease | 5/82 (6.1) | 5/ 61 (8.2) | 0/ 21 (0) | 0.176 |
| Chronic liver disease | 2/82 (2.4) | 1/ 61 (1.6) | 1/ 21 (4.8) | 0.424 |
| Immunosuppression | 13/82 (15.9) | 9/ 63 (14.3) | 4/ 19 (21.1) | 0.479 |
| Cancer | 3/84 (3.6) | 1/ 63 (1.6) | 2/ 21 (9.5) | 0.090 |
| Other | 31/78(39.7) | 21/ 58 (36.2) | 10/ 20 (50) | 0.277 |
| First episode | ||||
| Mean days of positivity (Mean, SD) | 17.5 (7.9) | 16.5 (6.9) | 21.1 (10) | 0.016 |
| Mild COVID-19 | 46/109 (42.2) | 32/ 82 (39) | 14/ 27 (51.9) | 0.208 |
| Moderate COVID-19 | 40/109 (36.7) | 29/ 82 (35.4) | 11/ 27 (40.7) | |
| Severe COVID-19 | 16/109 (14.7) | 14/ 82 (17.1) | 2/ 27 (7.4) | |
| Critical COVID-19 | 7/109 (6.4) | 7/ 82 (8.5) | 0/ 27 (0) | |
| Hospitalization | 95/119 (77.2) | 79/ 92 (85.9) | 16/ 27 (59.3) | 0.002 |
| Pneumonia | 46/62 (74.2) | 39/51 (76.5) | 7/11 (63.3) | 0.452 |
| Fever | 76/108 (70.4) | 60/ 81 (74.1) | 16/ 27 (59.3) | 0.144 |
| Cough | 67/108 (62) | 52/ 81 (64.2) | 15/ 27 (55.6) | 0.423 |
| Dyspnea | 28/105 (26.7) | 20/ 78 (25.6) | 8/ 27 (29.6) | 0.686 |
| Arthromyalgia | 20/108 (18.5) | 15/ 81 (18.5) | 5/ 27 (18.5) | 1.000 |
| Headache | 13/108 (12) | 9/ 81 (11.1) | 4/ 27 (14.8) | 0.609 |
| General cold symptoms | 19/108 (17.6) | 15/ 81 (18.5) | 4/ 27 (14.8) | 0.662 |
| Asthenia | 14/109 (12.8) | 11/ 82 (13.4) | 3/ 27 (11.1) | 0.756 |
| Gastrointestinal symptoms | 20/109 (18.3) | 20/ 82 (24.4) | 0/ 27 (0) | 0.005 |
| Second episode | ||||
| Mean days of positivity (Mean, SD) | 10.7 (10.6) | 10.6 (10.7) | 10.9 (10.9) | 0.928 |
| Mild COVID-19 | 59/97 (60.8) | 38/ 71 (53.5) | 21/ 26 (80.8) | 0.039 |
| Moderate COVID-19 | 22/97 (22.7) | 17/ 71 (23.9) | 5/ 26 (19.2) | |
| Severe COVID-19 | 7/97 (7.2) | 7/ 71 (9.9) | 0/ 26 (0) | |
| Critical COVID-19 | 9/97 (9.3) | 9/ 71 (12.7) | 0/ 26 (0) | |
| Hospitalization | 87/111 (70.7) | 73/ 88 (83) | 14/ 23 (60.9) | 0.043 |
| Pneumonia | 51/61 (83.6) | 49/53 (92.5) | 2/8 (25) | 0.001 |
| Fever | 30/100 (30) | 24/ 74 (32.4) | 6/ 26 (23.1) | 0.371 |
| Cough | 29/97 (29.9) | 24/ 71 (33.8) | 5/ 26 (19.2) | 0.165 |
| Dyspnea | 27/100 (27) | 24/ 74 (32.4) | 3/ 26 (11.5) | 0.039 |
| Arthromyalgia | 19/99 (19.2) | 14/ 73 (19.2) | 5/ 26 (19.2) | 1.000 |
| Headache | 10/100 (10) | 7/ 74 (9.5) | 3/ 26 (11.5) | 0.717 |
| General cold symptoms | 16/100 (16) | 12/ 74 (16.2) | 4/ 26 (15.4) | 1.000 |
| Asthenia | 8/100 (8) | 5/ 74 (6.8) | 3/ 26 (11.5) | 0.425 |
| Gastrointestinal symptoms | 9/100 (9) | 8/ 74 (10.8) | 1/ 26 (3.8) | 0.439 |
| Parameter | Number with and without Assessed Parameter | Mean RSP (SD) Parameter Present | Mean RSP (SD) Parameter Absent | p-Value |
|---|---|---|---|---|
| Female | 55 | 47.7 (31.6) | − | 0.651 |
| Male | 67 | 46.7 (26.9) | − | |
| Comorbidities | ||||
| Hypertension | 22 vs. 60 | 44.8 (24.8) | 55.8 (32.5) | 0.379 |
| Chronic heart disease | 14 vs. 70 | 46.8 (20.2) | 53.6 (32.3) | 0.773 |
| Arrhythmia | 11 vs. 73 | 49.2 (23.3) | 53 (31.7) | 0.974 |
| T2DM | 19 vs. 63 | 46.2 (22.6) | 54.9 (32.8) | 0.271 |
| COPD | 6 vs. 76 | 61.8 (39.8) | 52.2 (30.3) | 0.345 |
| Chronic kidney disease | 5 vs. 77 | 46.6 (9.6) | 53.3 (31.7) | 0.651 |
| Chronic liver disease | 2 vs. 80 | 58 (38.2) | 52.7 (30.9) | 0.939 |
| Immunosuppression | 13 vs. 69 | 52.9 (33.7) | 51.6 (30.3) | 0.899 |
| Cancer | 3 vs. 81 | 72.7 (23.1) | 51.7 (30.7) | 0.123 |
| Other | 31 vs. 47 | 53.8 (27.3) | 52.7 (32.5) | 0.434 |
| First episode | ||||
| Mild COVID-19 | 46 | 51.3 (32.9) | − | 0.537 |
| Moderate COVID-19 | 40 | 54 (34.7) | − | |
| Severe COVID-19 | 16 | 41.1 (20.6) | − | |
| Critical COVID-19 | 7 | 34.4 (11.4) | − | |
| Hospitalization | 95 vs. 24 | 44.2 (29.3) | 64.6 (29.8) | 0.001 |
| Pneumonia | 46 vs. 16 | 42.8 (28.2) | 42.2 (28.9) | 0.342 |
| Fever | 76 vs. 32 | 48.1 (31.4) | 53.1 (32.1) | 0.638 |
| Cough | 67 vs. 41 | 47.7 (32.6) | 52.6 (30) | 0.209 |
| Dyspnea | 28 vs. 77 | 48.4 (25.6) | 50.7 (34) | 0.873 |
| Arthromyalgia | 20 vs. 88 | 46.7 (20.8) | 50.2 (33.6) | 0.687 |
| Headache | 13 vs. 95 | 63.8 (38.8) | 47.6 (30.1) | 0.042 |
| General cold symptoms | 19 vs. 89 | 53.6 (35.9) | 48.7 (30.7) | 0.475 |
| Asthenia | 14 vs. 95 | 46.2 (28) | 49.8 (32.1) | 0.942 |
| Gastrointestinal symptoms | 20 vs. 89 | 33.8 (10.5) | 52.8 (33.6) | 0.061 |
| Second episode | ||||
| Mild COVID-19 | 59 | 55.1 (37.8) | − | 0.377 |
| Moderate COVID-19 | 22 | 48.5 (18.7) | − | |
| Severe COVID-19 | 7 | 47.9 (13.1) | − | |
| Critical COVID-19 | 9 | 33.9 (11.4) | − | |
| Hospitalization | 87 vs. 24 | 44 (27.9) | 56.4 (37) | 0.148 |
| Pneumonia | 51 vs. 10 | 35.3 (12.9) | 70.8 (41) | 0.012 |
| Fever | 30 vs. 70 | 48.9 (26.1) | 51.9 (33) | 0.798 |
| Cough | 29 vs. 68 | 47.2 (26) | 53.5 (33.3) | 0.750 |
| Dyspnea | 27 vs. 73 | 48.3 (25) | 52 (33.1) | 0.661 |
| Arthromyalgia | 19 vs. 80 | 53 (28.2) | 50.6 (32) | 0.344 |
| Headache | 10 vs. 90 | 60.8 (35.3) | 49.9 (30.5) | 0.186 |
| General cold symptoms | 16 vs. 84 | 58.8 (36.6) | 49.5 (29.9) | 0.220 |
| Asthenia | 8 vs. 92 | 65.3 (38.1) | 49.8 (30.3) | 0.155 |
| Gastrointestinal symptoms | 9 vs. 91 | 39.1 (15.2) | 52.2 (32) | 0.511 |
| Parameter | ≤30 Days | 31 to 60 Days | 61 to 90 Days | >90 Days | p-Value |
|---|---|---|---|---|---|
| Total number | 42 | 54 | 12 | 15 | |
| Female | 22/42 (52.4) | 20/54 (37) | 5/12 (41.7) | 8/14 (57.1) | 0.363 |
| Age (mean, SD, range) | 43.9 (22.9) | 56.4 (20.5) | 55.9 (20.3) | 36.6 (16.1) | 0.001 |
| Mean repeated positivity interval (SD) | 24.1 (4.9) | 41.9 (8.5) | 75.5 (9.3) | 114.1 (17) | 0.001 |
| Comorbidities | |||||
| Hypertension | 31.25% | 33.33% | 11.11% | 8.33% | 0.118 |
| Chronic heart disease | 17.65% | 17.39% | 33.33% | 0.00% | 0.238 |
| Arrhythmia | 11.76% | 13.04% | 33.33% | 0.00% | 0.166 |
| T2DM | 25.00% | 24.44% | 33.33% | 8.33% | 0.557 |
| COPD | 0.00% | 8.89% | 11.11% | 8.33% | 0.651 |
| Chronic kidney disease | 0.00% | 11.11% | 0.00% | 0.00% | 0.223 |
| Chronic liver disease | 0.00% | 2.22% | 11.11% | 0.00% | 0.314 |
| Immunosuppression | 17.65% | 13.04% | 42.86% | 8.33% | 0.199 |
| Cancer | 0.00% | 2.17% | 22.22% | 0.00% | 0.015 |
| Other | 37.50% | 35.71% | 66.67% | 36.36% | 0.377 |
| First episode | |||||
| Mean days of positivity (Mean, SD) | 13.5 (5.3) | 19.3 (7) | 23.3 (9.8) | 19.2 (10.2) | 0.001 |
| Mild COVID-19 | 40.00% | 38.30% | 50.00% | 53.33% | 0.797 |
| Moderate COVID-19 | 37.14% | 34.04% | 41.67% | 40.00% | |
| Severe COVID-19 | 17.14% | 17.02% | 8.33% | 6.67% | |
| Critical COVID-19 | 5.71% | 10.64% | 0.00% | 0.00% | |
| Hospitalization | 95.0% | 78.8% | 58.3% | 60.0% | 0.005 |
| Pneumonia | 63.0% | 91.7% | 75.0% | 57.1% | 0.452 |
| Fever | 69.44% | 77.78% | 58.33% | 60.00% | 0.422 |
| Cough | 69.44% | 60.00% | 50.00% | 60.00% | 0.641 |
| Dyspnea | 22.86% | 27.91% | 41.67% | 20.00% | 0.569 |
| Arthromyalgia | 16.67% | 20.00% | 33.33% | 6.67% | 0.349 |
| Headache | 2.78% | 17.78% | 8.33% | 20.00% | 0.147 |
| General cold symptoms | 16.67% | 20.00% | 16.67% | 13.33% | 0.941 |
| Asthenia | 10.81% | 15.56% | 8.33% | 13.33% | 0.884 |
| Gastrointestinal symptoms | 24.32% | 24.44% | 0.00% | 0.00% | 0.045 |
| Second episode | |||||
| Mean days of positivity (Mean, SD) | 10.1 (10.5) | 11.2 (11.1) | 5.7 (6) | 16.1 (12.7) | 0.238 |
| Mild COVID-19 | 76.67% | 36.59% | 66.67% | 92.86% | 0.005 |
| Moderate COVID-19 | 10.00% | 34.15% | 33.33% | 7.14% | |
| Severe COVID-19 | 3.33% | 14.63% | 0.00% | 0.00% | |
| Critical COVID-19 | 10.00% | 14.63% | 0.00% | 0.00% | |
| Hospitalization | 82.5% | 83.3% | 55.6% | 64.3% | 0.135 |
| Pneumonia | 87.5% | 96.6% | 50.0% | 0.0% | 0.001 |
| Fever | 25.81% | 37.21% | 33.33% | 14.29% | 0.417 |
| Cough | 33.33% | 34.15% | 25.00% | 14.29% | 0.505 |
| Dyspnea | 16.13% | 44.19% | 8.33% | 14.29% | 0.011 |
| Arthromyalgia | 12.90% | 23.81% | 33.33% | 7.14% | 0.257 |
| Headache | 3.23% | 13.95% | 8.33% | 14.29% | 0.423 |
| General cold symptoms | 12.90% | 18.60% | 8.33% | 21.43% | 0.778 |
| Asthenia | 3.23% | 9.30% | 8.33% | 14.29% | 0.487 |
| Gastrointestinal symptoms | 6.45% | 13.95% | 8.33% | 0.00% | 0.521 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Váncsa, S.; Dembrovszky, F.; Farkas, N.; Szakó, L.; Teutsch, B.; Bunduc, S.; Nagy, R.; Párniczky, A.; Erőss, B.; Péterfi, Z.; et al. Repeated SARS-CoV-2 Positivity: Analysis of 123 Cases. Viruses 2021, 13, 512. https://0-doi-org.brum.beds.ac.uk/10.3390/v13030512
Váncsa S, Dembrovszky F, Farkas N, Szakó L, Teutsch B, Bunduc S, Nagy R, Párniczky A, Erőss B, Péterfi Z, et al. Repeated SARS-CoV-2 Positivity: Analysis of 123 Cases. Viruses. 2021; 13(3):512. https://0-doi-org.brum.beds.ac.uk/10.3390/v13030512
Chicago/Turabian StyleVáncsa, Szilárd, Fanni Dembrovszky, Nelli Farkas, Lajos Szakó, Brigitta Teutsch, Stefania Bunduc, Rita Nagy, Andrea Párniczky, Bálint Erőss, Zoltán Péterfi, and et al. 2021. "Repeated SARS-CoV-2 Positivity: Analysis of 123 Cases" Viruses 13, no. 3: 512. https://0-doi-org.brum.beds.ac.uk/10.3390/v13030512