
In Vitro Assessment of the Antiviral Activity of Ketotifen, Indomethacin and Naproxen, Alone and in Combination, against SARS-CoV-2

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study 1. Cytopathic Effect (CPE) Assay
- X = test or control article concentration;
- Y = percent cell protection;
- Min = minimum;
- Max = maximum;
- D = slope coefficient.
2.2. Study 2. Yield Reduction Assay
2.3. Study 3. Cytotoxicity Assay
3. Results
3.1. Study 1. Cytopathic Effect (CPE) Assay
3.2. Study 2. Yield Reduction Assay
3.3. Study 3. Cytotoxicity Assay
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zumla, A.; Chan, J.; Azhar, A.; Hui, D.; Yuen, Y. Coronaviruses—drug discovery and therapeutic options. Nature Rev. 2016, 15, 327–347. [Google Scholar] [CrossRef] [Green Version]
- Pal, M.; Berhanu, G.; Desalegn, C.; Kandi, V. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): An update. Cureus 2020, 12, e7423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ksiazek, T.; Erdman, D.; Goldsmith, C.; Zaki, S.; Peret, T.; Emery, S.; Tong, S.; Urbani, C.; Comer, J.; Lim, W.; et al. A novel coronavirus associated with severe acute respiratory syndrome. N. Engl. J. Med. 2003, 348, 1953–1966. [Google Scholar] [CrossRef]
- ECDC Technical Report: Interim Guidance for Environmental Cleaning in Non-Healthcare Facilities Exposed to SARS-CoV-2; European Center for Disease Prevention and Control: Solna, Sweden, 2020.
- Paules, C.; Marston, H.; Fauci, A. Coronavirus Infections—More Than Just the Common Cold. JAMA 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- V’kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2020. [Google Scholar] [CrossRef]
- Marinella, M. Indomethacin and resveratrol as potential treatment adjuncts for SARS-CoV-2/COVID-19. Int. J. Clin. Pract. 2020, 74, e13535. [Google Scholar] [CrossRef]
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.; Chen, S.; Jin, H.; Tan, K.; Wang, D.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Military Med. Res. 2020, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Valle, D.M.; Kim-Schulze, S.; Huang, H.H.; Beckmann, N.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nat. Med. 2020, 26, 1636–1643. [Google Scholar] [CrossRef] [PubMed]
- Dauby, N.; Bottieau, E. The unfinished story of hydroxychloroquine in COVID-19: The right anti-inflammatory dose at the right moment? Int. J. Infect. Dis 2021, 103, 1–2. [Google Scholar] [CrossRef]
- Tanacan, A.; Yazihan, N.; Erol, S.; Anuk, A.; Yetiskin, F.; Biriken, D.; Ozgu-Erdinc, A.; Keskin, H.; Tekin, O.; Sahin, D. The impact of COVID-19 infection on the cytokine profile of pregnant women: A prospective case-control study. Cytokine 2021, 140, 155431. [Google Scholar] [CrossRef]
- Karki, R.; Karki, R.; Sharma, B.; Tuladhar, S.; Williams, E.; Zalduondo, L.; Samir, P.; Zheng, M.; Sundaram, B.; Banoth, B.; et al. Synergism of TNF-a and IFN-g Triggers Inflammatory Cell Death, Tissue Damage, and Mortality in SARSCoV-2 Infection and Cytokine Shock Syndromes. Cell 2021, 184, 149–168. [Google Scholar] [CrossRef] [PubMed]
- Hojyo, S.; Hojyo, S.; Uchida, M.; Tanaka, K.; Hasebe, R.; Tanaka, Y.; Murakami, M.; Hirano, T. How COVID-19 induces cytokine storm with high mortality. Inflamm. Regen. 2020, 40, 37. [Google Scholar] [CrossRef]
- Mustafa, M.; Abdelmoneim, A.; Mahmoud, E.; Makhawi, A. Cytokine storm in COVID-19 patients, its impact on organs and potential treatment by QTY code-designed detergent-free chemokine receptors. Mediators Inflam. 2020, 2020, 8198963. [Google Scholar] [CrossRef] [PubMed]
- Abdulkhaleq, L.A.; Assi, M.A.; Abdullah, R.; Zamri-Saad, M.; Taufiq-Yap, Y.H.; Hezmee, M.N.M. The crucial roles of inflammatory mediators in inflammation: A review. Vet. World 2020, 11, 627–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEvoy, N.; McElvaney, O.; Carroll, T.; Murphy, M.; Dunlea, D.; Choileain, O.; Clarke, J.; O’Connor, E.; Hogan, G.; Ryan, D.; et al. Characterization of the inflammatory response to severe COVID-19 illness. Am. J. Respir. Crit. Care Med. 2020, 202, 812–821. [Google Scholar]
- Li, A.; Garcia-Bengochea, Y.; Stechel, R.; Azari, B. Management of COVID-19 myopericarditis with reversal of cardiac dysfunction after blunting of cytokine storm: A case report. Eur. Heart J. Case Rep. 2020, 4, 1–6. [Google Scholar] [CrossRef]
- Food and Drug Administration (FDA). Guidance for Industry. Antiviral Product Development—Conducting and Submitting Virology Studies to the Agency; U.S. Department of Health and Human Services, FDA, Center for Drug Evaluation and Research (CDER): Silver Spring, MA, USA, 2006. [Google Scholar]
- St John, A.L.; Rathore, A.P.S.; Raghavan, B.; Ng, M.L.; Abraham, S.N. Contributions of mast cells and vasoactive products, leukotrienes and chymase, to dengue virus-induced vascular leakage. eLife 2013, 2, e00481. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Fontela, C. Animal models for COVID-19. Nature 2020, 586, 509–515. [Google Scholar] [CrossRef]
- Disodium cromoglycate. Lancet 1972, 2, 1299.
- Theoharides, T.C.; Sieghart, W.; Greengard, P.; Douglas, W.W. Antiallergic drug cromolyn may inhibit histamine secretion by regulating phosphorylation of a mast cell protein. Science 1980, 207, 80–82. [Google Scholar] [CrossRef]
- McClean, S.P.; Arreaza, E.E.; Lett-Brown, M.A.; Grant, J.A. Refractory cholinergic urticaria successfully treated with ketotifen. J. Allergy Clin. Immunol. 1989, 83, 738–741. [Google Scholar] [CrossRef]
- Pauwels, R.; Balzarini, J.; Baba, M.; Snoeck, R.; Schols, D.; Herdewijn, P.; Desmyter, J.; De Clercq, E. Rapid and automated tetrazoliμM-based colorimetric assay for the detection of anti-HIV compounds. J. Virol. Methods 1988, 20, 309–321. [Google Scholar] [CrossRef]
- Reed, L.J.; Muench, H. A simple method of estimating fifty percent endpoints. Am. J. Hyg. 1938, 27, 493–497. [Google Scholar]
- Lejal, N.; Tarus, B.; Bouguyon, E.; Chenavas, S.; Bertho, N.; Delmas, B.; Ruigrok, R.W.H.; Di Primo, C.; Slama-Schwok, A. structure-based discovery of the novel antiviral properties of naproxen against the nucleoprotein of influenza A virus. Antimicrob. Agents Chemother. 2013, 57, 2231–2241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, W.; Fan, W.; Zhang, S.; Jiao, P.; Shang, Y.; Cui, L.; Mahesutihan, M.; Li, J.; Wang, D.; Fu Gao, G.; et al. Naproxen exhibits broad anti-influenza virus activity in mice by impeding viral nucleoprotein nuclear export. Cell Rep. 2019, 27, 1875–1885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amici, C.; Di Caro, A.; Ciucci, A.; Chiappa, L.; Castilletti, C.; Martella, V.; Decaro, N.; Buonavoglia, C.; Capobianchi, M.R.; Santoro, M.G. Indomethacin has a potent antiviral activity against SARS coronavirus. Antivir Ther. 2006, 11, 1021–1030. [Google Scholar]
- Gomeni, R.; Xu, T.; Gao, X.; Bressolle-Gomeni, F. Model based approach for estimating the dosage regimen of indomethacin a potential antiviral treatment of patients infected with SARS CoV-2. J. Pharmacokin. Pharmacodyn. 2020, 47, 189–198. [Google Scholar] [CrossRef]
- Terracciano, R.; Preianò, M.; Fregola, A.; Pelaia, C.; Montalcini, T.; Savino, R. Mapping the SARS-CoV-2–host protein–protein interactome by affinity purification mass spectrometry and proximity-dependent biotin labeling: A rational and straightforward route to discover host-directed anti-SARS-CoV-2 therapeutics. Int. J. Mol. Sci. 2021, 22, 532. [Google Scholar] [CrossRef]
- Mostafa, A.; Kandeil, A.; Elshaier, Y.; Kutkat, O.; Moatasim, Y.; Rashad, A.; Shehata, M.; Gomaa, M.; Mahrous, N.; Mahmoud, S.; et al. FDA-Approved drugs with potent In vitro antiviral activity against Severe Acute Respiratory Syndrome Coronavirus 2. Pharmaceuticals 2020, 13, 443. [Google Scholar] [CrossRef]
- Baradaran, H.; Hamishehkar, H.; Rezaee, H. NSAIDs and COVID-19: A new challenging area. Pharm. Sci. 2020, 26, S49–S51. [Google Scholar] [CrossRef]
- Hung, I.F.N.; To, K.K.W.; Chan, J.F.W.; Cheng, V.C.C.; Liu, K.S.H.; Tam, A.; Chan, T.-C.; Zhang, A.J.; Li, P.; Wong, T.-L.; et al. Efficacy of clarithromycin-naproxen-oseltamivir combination in the treatment of patients hospitalized for influenza A (H3N2) infection: An open-label randomized, controlled, phase IIb/III trial. Chest 2017, 151, 1069–1080. [Google Scholar] [CrossRef]
- Hanly, P.J.; Roberts, D.; Dobson, K.; Light, R.B. Effects of indomethacin on arterial oxygenation in critically ill patients with severe distress syndrome. Lancet 1987, 1, 351–354. [Google Scholar] [CrossRef]
- Steinberg, S.M.; Rodriguez, J.L.; Bitzer, L.G.; Rhee, J.W.; Kelley, K.A.; Flint, L.M. Indomethacin treatment of human adult respiratory distress syndrome. Circ. Shock 1990, 30, 375–384. [Google Scholar]
- Sacerdote, P.; Carrabba, M.; Galante, A.; Pisati, R.; Manfredi, B.; Panerai, A.E. Plasma and synovial fluid interleukin-1, interleukin-6 and substance P concentrations in rheumatoid arthritis patients: Effect of the nonsteroidal anti-inflammatory drugs indomethacin, diclofenac and naproxen. Inflamm. Res. 1995, 44, 486–490. [Google Scholar] [CrossRef]
- Bour, A.M.; Westendorp, R.G.; Laterveer, J.C.; Bollen, E.L.; Remarque, E.J. Interaction of indomethacin with cytokine production in whole blood. Potential mechanism for a brain-protective effect. Exp. Gerontol. 2000, 35, 1017–1024. [Google Scholar] [CrossRef]
- Wu, R.; Wang, L.; Kuo, H.; Shannar, A.; Peter, R.; Chou, P.; Li, S.; Hudlikar, R.; Liu, X.; Liu, Z.; et al. An update on current therapeutic drugs treating COVID-19. Curr. Pharmacol. Rep. 2020, 6, 56–70. [Google Scholar] [CrossRef] [PubMed]
- Al-Horani, R.; Kar, S. Potential anti-SARS-CoV-2 therapeutics that target the post-entry stages of the viral life cycle: A comprehensive review. Viruses 2020, 12, 1092. [Google Scholar] [CrossRef]
- Robb, C.; Goepp, M.; Rossi, A.; Yao, C. Non-steroidal anti-inflammatory drugs, prostaglandins, and COVID-19. Br. J. Pharmacol. 2020, 177, 4899–4920. [Google Scholar] [CrossRef]
- Dilly, S.; Fotso, A.; Lejal, N.; Zedda, G.; Chebbo, M.; Rahman, F.; Companys, S.; Bertrand, H.; Vidic, J.; Noiray, M.; et al. From Naproxen Repurposing to Naproxen Analogues and Their Antiviral Activity against Influenza A Virus. J. Med. Chem. 2018, 61, 7202–7217. [Google Scholar] [CrossRef] [PubMed]
- Enkirch, T.; Sauber, S.; Anderson, D.E.; Gan, E.S.; Kenanov, D.; Maurer-Stroh, S.; von Messling, V. Identification and in vivo efficacy assessment of approved orally bioavailable human host protein-targeting drugs with broad anti-influenza A activity. Front Immunol. 2019, 10, 1097. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.; Jin, Y.; Han, D.; Zhang, G.; Cao, S.; Xie, J.; Xue, J.; Li, Y.; Meng, D.; Fan, X.; et al. Mast cell-induced lung injury in mice infected with H5N1 influenza virus. J. Virol. 2012, 86, 3347–3356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eliakim, R.; Karmeli, F.; Rachmilewitz, D. Ketotifen-old drug, new indication: Reduction of gastric mucosal injury. Scand J. Gastroenterol. 1993, 28, 202–204. [Google Scholar] [CrossRef] [PubMed]
- Narendranathan, M.; Chitra, P.; Kurien, M.; Philip, J. Ketotifen in prevention of indomethacin-induced gastropathy. Indian J. Gastroenterol. 1999, 18, 76–77. [Google Scholar] [PubMed]
- Terrier, O.; Dilly, S.; Pizzorno, A.; Henri, J.; Berenbaum, F.; Lina, B.; Fève, B.; Adnet, F.; Sabbah, M.; Rosa-Calatrava, M.; et al. Broad-spectrum antiviral activity of naproxen: From influenza A to SARS-CoV-2 coronavirus. BioRxiv 2020. [Google Scholar] [CrossRef]
- Xu, T.; Gao, X.; Wu, Z.; Selinger, D.W.; Zhou, Z. Indomethacin has a potent antiviral activity against SARS CoV-2 in vitro and canine coronavirus in vivo. BioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Compound | EC50 (μM) | CC50 (μM) |
|---|---|---|
| Ketotifen | >138.6 | 138.6 |
| Naproxen | >400 | >400 |
| Indomethacin | >400 | >400 |
| Remdesivir | 2.9 | NT |
| Concentration Naproxen (μM) | |||||||
|---|---|---|---|---|---|---|---|
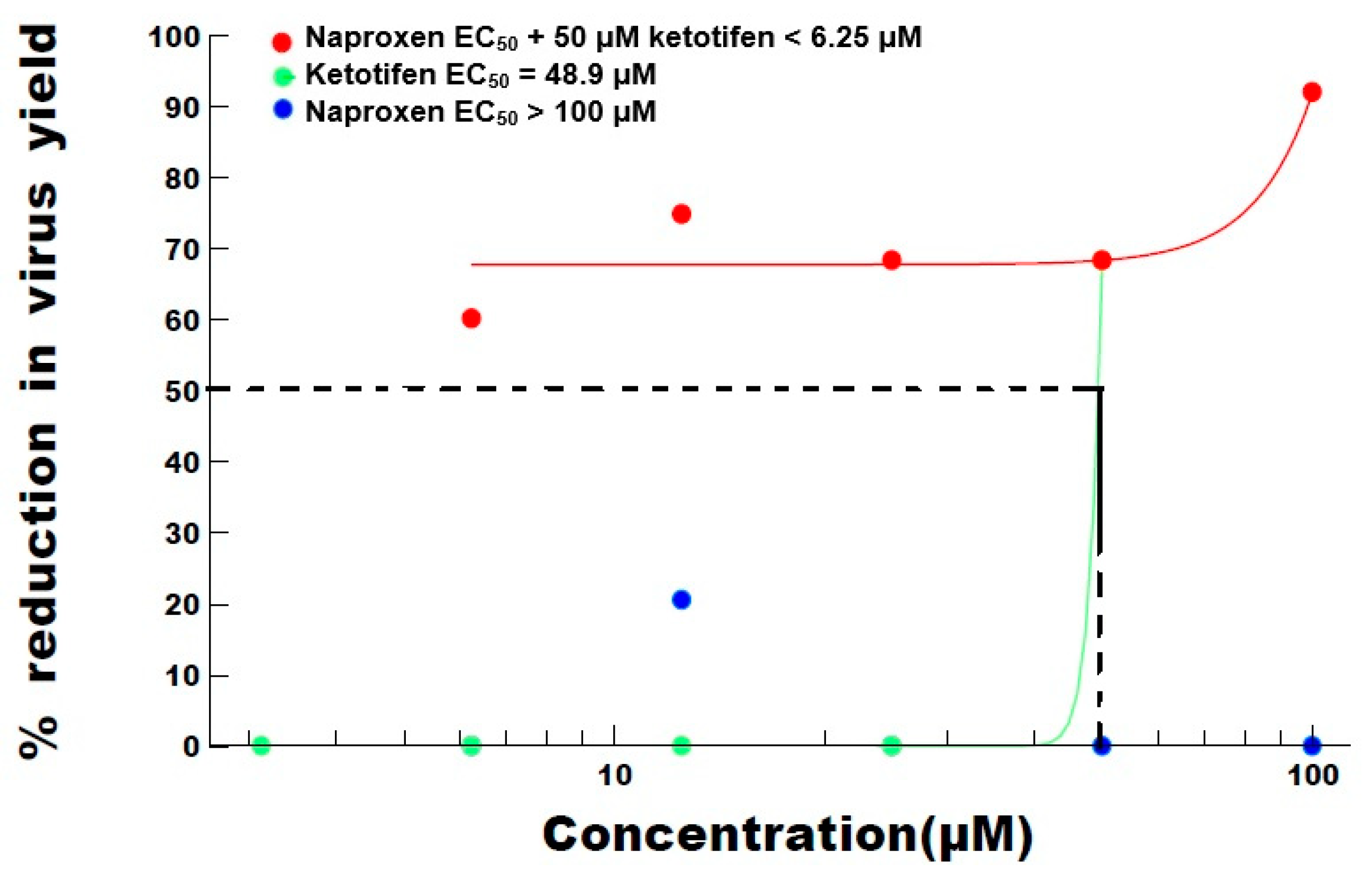
| Treatment | EC50 | 100 | 50 | 25 | 12.5 | 6.25 | 3125 |
| Ketotifen | 48.9 | - | 68 | 0 | 0 | 0 | 0 |
| Naproxen | >100 | 0 | 0 | 0 | 21 | 0 | - |
| Naproxen EC50 + 50 μM ketotifen | <6.25 | 92 | 68 | 68 | 75 | 60 | - |
| Concentration Ketotifen (μM) | ||||||
|---|---|---|---|---|---|---|
| Treatment | EC50 | 50 | 25 | 12.5 | 6.25 | 3125 |
| Ketotifen | 47.1 | 60 | 0 | 0 | 0 | 0 |
| Ketotifen + 100 μM indomethacin | 48.1 | 94 | 0 | 0 | 37 | 0 |
| Ketotifen + 50 μM indomethacin | 46.5 | 97 | 0 | 0 | 0 | 37 |
| Ketotifen + 25 μM indomethacin | 42.2 | 90 | 0 | 0 | 0 | 0 |
| Concentration Indomethacin (μM) | ||||||
|---|---|---|---|---|---|---|
| Treatment | EC50 | 100 | 50 | 25 | 12.5 | 6.25 |
| Indomethacin | 100.1 | 50 | 0 | 0 | - | - |
| Indomethacin + 50 μM ketotifen | <6.25 | 93 | 83 | 79 | 75 | 60 |
| Indomethacin + 25 μM ketotifen | >100 | 0 | 0 | 0 | - | - |
| Indomethacin + 12.5 μM ketotifen | >100 | 0 | 0 | 0 | - | - |
| Indomethacin + 6.25 μM ketotifen | >100 | 37 | 0 | 0 | - | - |
| Indomethacin + 3.125 μM ketotifen | >100 | 0 | 37 | 0 | - | - |
| Concentration (μM) | 100 | 50 | 25 | 12.5 | 6.25 | 3.13 | 1.56 | 0.78 | 0.39 | 0.20 |
|---|---|---|---|---|---|---|---|---|---|---|
| Indomethacin (%) | 143 | 143 | 125 | 124 | 124 | 117 | 111 | 106 | 98 | - |
| Naproxen (%) | 107 | 108 | 107 | 107 | 106 | 112 | 96 | 112 | 108 | - |
| Ketotifen (%) | - | 86 | 104 | 122 | 125 | 121 | 109 | 101 | 103 | 110 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiani, P.; Scholey, A.; Dahl, T.A.; McMann, L.; Iversen, J.M.; Verster, J.C. In Vitro Assessment of the Antiviral Activity of Ketotifen, Indomethacin and Naproxen, Alone and in Combination, against SARS-CoV-2. Viruses 2021, 13, 558. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040558
Kiani P, Scholey A, Dahl TA, McMann L, Iversen JM, Verster JC. In Vitro Assessment of the Antiviral Activity of Ketotifen, Indomethacin and Naproxen, Alone and in Combination, against SARS-CoV-2. Viruses. 2021; 13(4):558. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040558
Chicago/Turabian StyleKiani, Pantea, Andrew Scholey, Thomas A. Dahl, Lauren McMann, Jacqueline M. Iversen, and Joris C. Verster. 2021. "In Vitro Assessment of the Antiviral Activity of Ketotifen, Indomethacin and Naproxen, Alone and in Combination, against SARS-CoV-2" Viruses 13, no. 4: 558. https://0-doi-org.brum.beds.ac.uk/10.3390/v13040558