
Feline Morbillivirus in Southern Italy: Epidemiology, Clinico-Pathological Features and Phylogenetic Analysis in Cats

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Power and Sample Size
2.2. Study Sites, Cat Enrollment and Sampling Procedures
2.3. Clinicopathological Evaluation
2.4. Clinical Groups
2.5. Molecular Detection of FeMV RNA and Other Relevant Feline Pathogens in Cats
2.6. Indirect Immunofluorescence Assay for Anti-FeMV Antibodies and Enzyme-Linked Immunosorbent Assay for Anti-FIV Antibodies Detections
2.7. Histopathological Examination
2.8. Sequencing and Phylogenetic Characterization
2.9. Statistical Analysis
3. Results
3.1. Cat Population Demographic and Clinical Data
3.2. FeMV RNA and Anti-FeMV Antibodies Were Detected
3.3. FeMV Detection Was Related with Some Investigated Variables
3.4. FeMV Infection Was Associated with Retroviral Infections
3.5. FeMV Patterns Based on Molecular and Serological Data Were Associated with Some Investigated Variables
3.6. Older Age Was a Risk Factor for FeMV Infection and Seropositivity to FeMV Was Associated with CKD
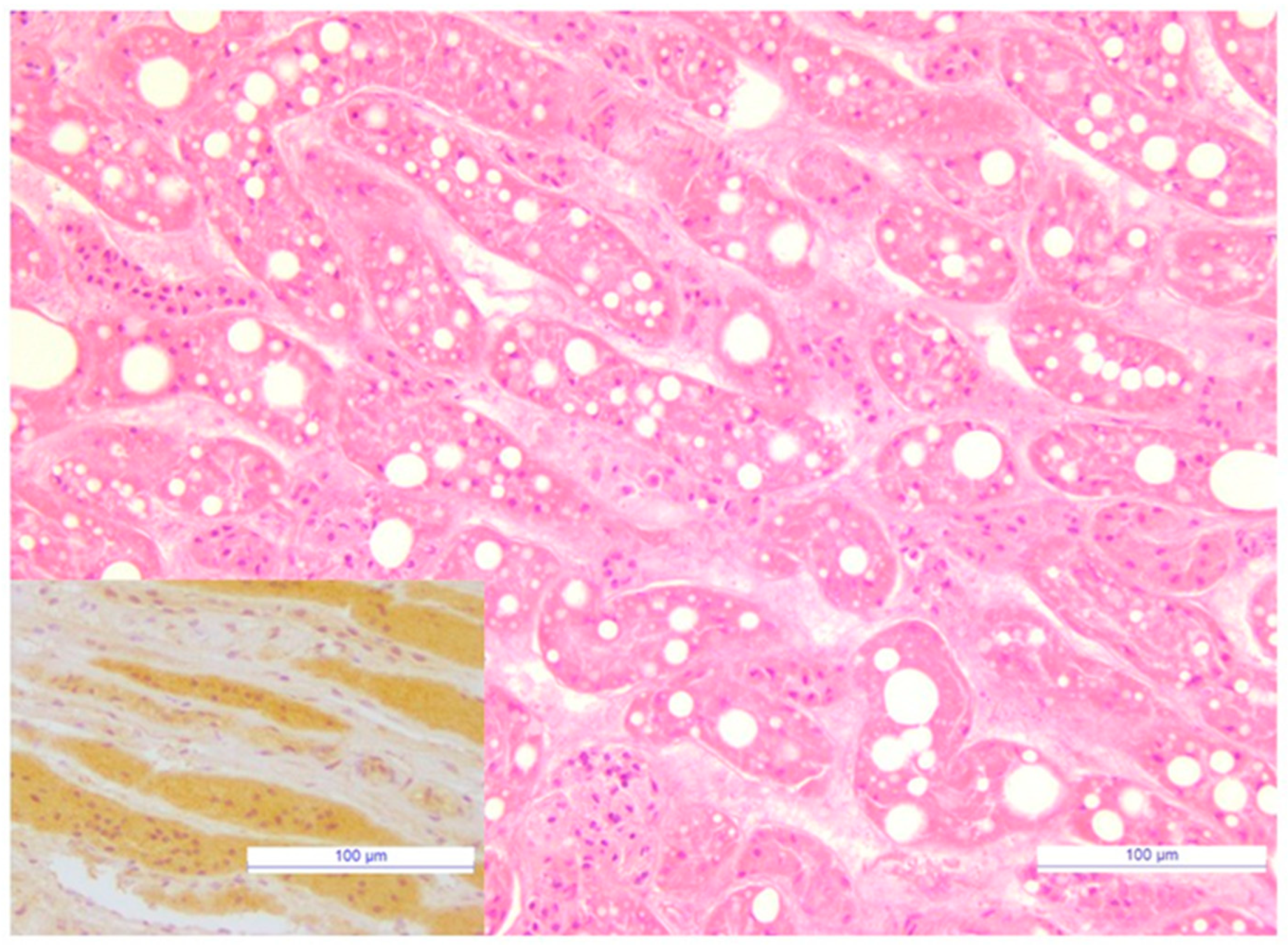
3.7. Immunoreactivity to FeMV Was Observed in Renal Tubules
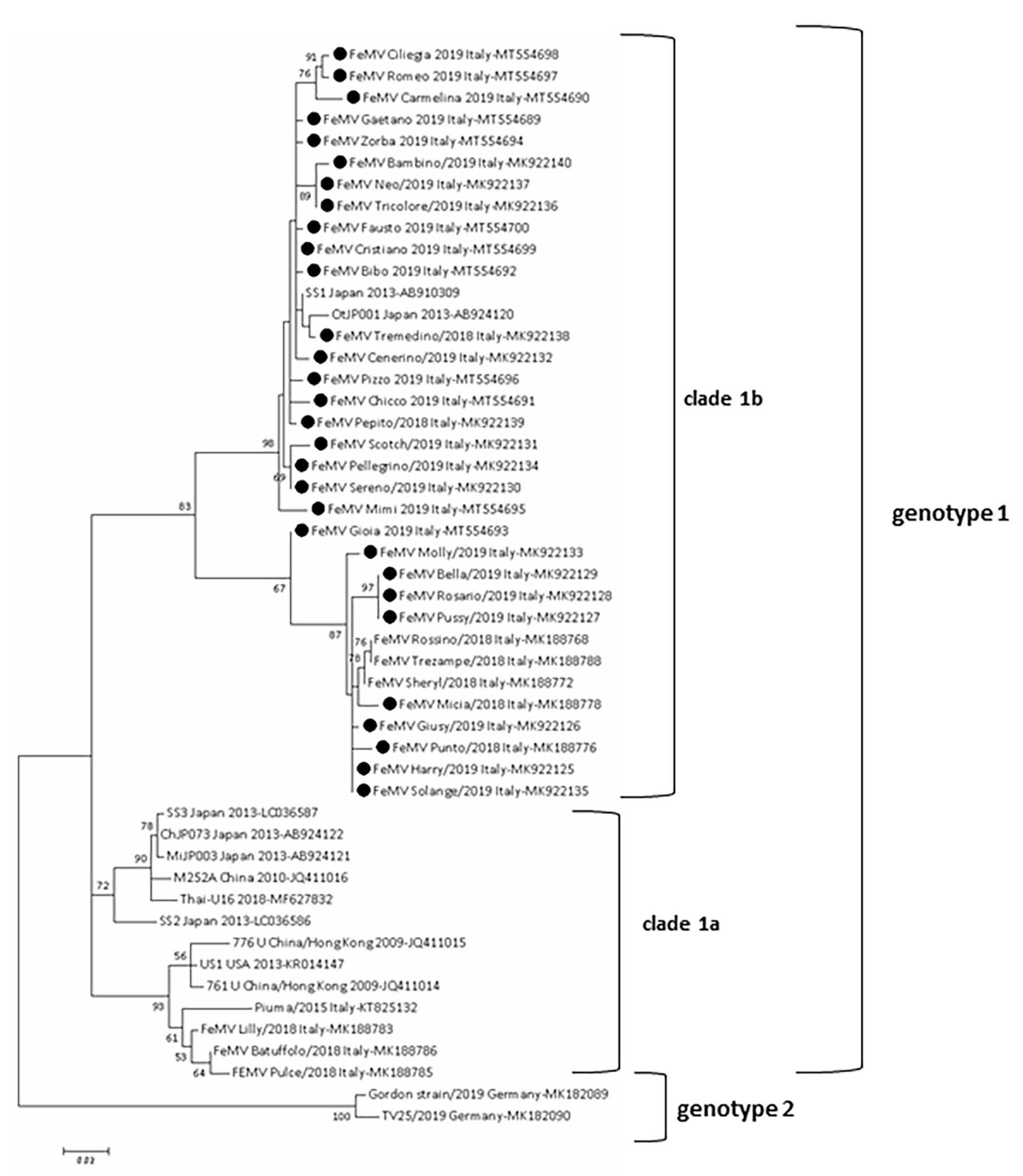
3.8. FeMV Genotype 1 Was Sequenced
3.9. Data about FeMV Viremia, Urinary Shedding, Seroreactivity and CKD in Followed Up Cats
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Vries, R.D.; Duprex, W.P.; de Swart, R.L. Morbillivirus infections: An introduction. Viruses 2015, 7, 699–706. [Google Scholar] [CrossRef] [Green Version]
- Park, E.S.; Suzuki, M.; Kimura, M.; Mizutani, H.; Saito, R.; Kubota, N.; Hasuike, Y.; Okajima, J.; Kasai, H.; Sato, Y.; et al. Epidemiological and pathological study of feline morbillivirus infection in domestic cats in Japan. BMC Vet. Res. 2016, 12, 228. [Google Scholar] [CrossRef] [Green Version]
- Woo, P.C.; Lau, S.K.; Wong, B.H.; Fan, R.Y.; Wong, A.Y.; Zhang, A.J.; Wu, Y.; Choi, G.K.; Li, K.S.; Hui, J.; et al. Feline morbillivirus, a previously undescribed paramyxovirus associated with tubulointerstitial nephritis in domestic cats. Proc. Natl. Acad. Sci. USA 2012, 109, 5435–5440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afonso, C.L.; Amarasinghe, G.K.; Banyai, K.; Bào, Y.; Basler, C.F.; Bavari, S.; Bejerman, N.; Blasdell, K.R.; Briand, F.; Briese, T.; et al. Taxonomy of the order Mononegavirales: Update 2016. Arch. Virol. 2016, 161, 2351–2360. [Google Scholar] [CrossRef]
- Chaiyasak, S.; Piewbang, C.; Rungsipipat, A.; Techangamsuwan, S. Molecular epidemiology and genome analysis of feline morbillivirus in household and shelter cats in Thailand. BMC Vet. Res. 2020, 16, 240. [Google Scholar] [CrossRef] [PubMed]
- Mohd Isa, N.H.; Selvarajah, G.T.; Khor, K.H.; Tan, S.W.; Manoraj, H.; Omar, N.H.; Omar, A.R.; Mustaffa-Kamal, F. Molecular detection and characterisation of feline morbillivirus in domestic cats in Malaysia. Vet. Microbiol. 2019, 236, 108382. [Google Scholar] [CrossRef] [PubMed]
- Ou, J.; Ye, S.; Xu, H.; Zhao, J.; Ren, Z.; Lu, G.; Li, S. First report of feline morbillivirus in mainland China. Arch. Virol. 2020, 165, 1837–1841. [Google Scholar] [CrossRef] [PubMed]
- Furuya, T.; Sassa, Y.; Omatsu, T.; Nagai, M.; Fukushima, R.; Shibutani, M.; Yamaguchi, T.; Uematsu, Y.; Shirota, K.; Mizutani, T. Existence of feline morbillivirus infection in Japanese cat populations. Arch. Virol. 2014, 159, 371–373. [Google Scholar] [CrossRef]
- Sakaguchi, S.; Nakagawa, S.; Yoshikawa, R.; Kuwahara, C.; Hagiwara, H.; Asai, K.I.; Kawakami, K.; Yamamoto, Y.; Ogawa, M.; Miyazawa, T. Genetic diversity of feline morbilliviruses isolated in Japan. J. Gen. Virol. 2014, 95, 1464–1468. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, A.; Di Tommaso, M.; Di Felice, E.; Zaccaria, G.; Luciani, A.; Marcacci, M.; Aste, G.; Boari, A.; Savini, G. First report of feline morbillivirus in Europe. Vet. Ital. 2015, 51, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, A.; de Luca, E.; Crisi, P.E.; Febo, E.; Di Tommaso, M.; Malatesta, D.; Zaccaria, G.; Marcacci, M.; Di Francesco, G.; Di Domenico, M.; et al. Feline morbillivirus in domestic cats in Italy: Epidemiological and pathological aspects. In Proceedings of the International Symposium of the Word Association of Veterinary Laboratory Diagnosticans, Sorrento, Italy, 7–10 June 2017; pp. 87–88. [Google Scholar]
- Sieg, M.; Heenemann, K.; Rückner, A.; Burgener, I.; Oechtering, G.; Vahlenkamp, T.W. Discovery of new feline paramyxoviruses in domestic cats with chronic kidney disease. Virus Genes 2015, 51, 294–297. [Google Scholar] [CrossRef]
- Sharp, C.R.; Nambulli, S.; Acciardo, A.S.; Rennick, L.J.; Drexler, J.F.; Rima, B.K.; Williams, T.; Duprex, W.P. Chronic infection of domestic cats with feline morbillivirus, United States. Emerg. Infect. Dis. 2016, 22, 760–762. [Google Scholar] [CrossRef] [Green Version]
- Darold, G.M.; Alfieri, A.A.; Muraro, L.S.; Amude, A.M.; Zanatta, R.; Yamauchi, K.C.; Alfieri, A.F.; Lunardi, M. First report of feline morbillivirus in South America. Arch. Virol. 2017, 162, 469–475. [Google Scholar] [CrossRef]
- De Luca, E.; Crisi, P.E.; Febo, E.; di Tommaso, M.; Malatesta, D.; Zaccaria, G.; Marcacci, M.; di Francesco, G.; di Domenico, M.; Giovannini, A.; et al. Feline morbillivirus infection in domestic cats in Italy: Epidemiological and pathological aspects. In Proceedings of the European College of Veterinary Internal Medicine Companion Animal Congress, St Julian’s, Malta, 14–16 September 2017. [Google Scholar]
- Yilmaz, H.; Tekelioglu, B.K.; Gurel, A.; Bamac, O.E.; Ozturk, G.Y.; Cizmecigil, U.Y.; Altan, E.; Aydin, O.; Yilmaz, A.; Berriatua, E.; et al. Frequency, clinicopathological features and phylogenetic analysis of feline morbillivirus in cats in Istanbul, Turkey. J. Feline Med. Surg. 2017, 19, 1206–1214. [Google Scholar] [CrossRef]
- Donato, G.; de Luca, E.; Pizzurro, F.; Masucci, M.; Lorusso, A.; Pennisi, M.G. Morbillivirus RNA and antibody prevalence in cats with renal disease investigated by measuring serum SDMA. In Proceedings of the ISFM European Feline Congress, Sorrento, Italy, 27 June–1 July 2018; p. 849. [Google Scholar]
- McCallum, K.E.; Stubbs, S.; Hope, N.; Mickleburgh, I.; Dight, D.; Tiley, L.; Williams, T.L. Detection and seroprevalence of morbillivirus and other paramyxoviruses in geriatric cats with and without evidence of azotemic chronic kidney disease. J. Vet. Intern. Med. 2018, 32, 1100–1108. [Google Scholar] [CrossRef]
- Sutummaporn, K.; Suzuki, K.; Machida, N.; Mizutani, T.; Park, E.S.; Morikawa, S.; Furuya, T. Association of feline morbillivirus infection with defined pathological changes in cat kidney tissues. Vet. Microbiol. 2019, 228, 12–19. [Google Scholar] [CrossRef]
- Stranieri, A.; Lauzi, S.; Dallari, A.; Gelain, M.E.; Bonsembiante, F.; Ferro, S.; Paltrinieri, S. Feline morbillivirus in Northern Italy: Prevalence in urine and kidneys with and without renal disease. Vet. Microbiol. 2019, 233, 133–139. [Google Scholar] [CrossRef]
- Muratore, E.; Cerutti, F.; Colombino, E.; Biasibetti, E.; Caruso, C.; Brovida, C.; Cavana, P.; Poncino, L.; Caputo, M.P.; Peletto, S.; et al. Feline morbillivirus in northwestern Italy: First detection of genotype 1-B. J. Feline Med. Surg. 2020, 3, 1098612X20969360. [Google Scholar] [CrossRef]
- Balbo, L.C.; Fritzen, J.T.T.; Lorenzetti, E.; Medeiros, T.N.S.; Jardim, A.M.; Alfieri, A.A.; Alfieri, A.F. Molecular characterization of Feline paramyxovirus and Feline morbillivirus in cats from Brazil. Braz. J. Microbiol. 2021, 52, 961–965. [Google Scholar] [CrossRef]
- Busch, J.; Sacristán, I.; Cevidanes, A.; Millán, J.; Vahlenkamp, T.W.; Napolitano, C.; Sieg, M. High seroprevalence of feline morbilliviruses in free-roaming domestic cats in Chile. Arch. Virol. 2021, 166, 281–285. [Google Scholar] [CrossRef]
- Park, E.S.; Suzuki, M.; Kimura, M.; Maruyama, K.; Mizutani, H.; Saito, R.; Kubota, N.; Furuya, T.; Mizutani, T.; Imaoka, K.; et al. Identification of a natural recombination in the F and H genes of feline Morbillivirus. Virology 2014, 468–470, 524–531. [Google Scholar] [CrossRef] [Green Version]
- Furuya, T.; Wachi, A.; Sassa, Y.; Omatsu, T.; Nagai, M.; Fukushima, R.; Shibutani, M.; Yamaguchi, T.; Uematsu, Y.; Shirota, K.; et al. Quantitative PCR detection of feline morbillivirus in cat urine samples. J. Vet. Med. Sci. 2016, 77, 1701–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Luca, E.; Crisi, P.E.; Marcacci, M.; Malatesta, D.; Di Sabatino, D.; Cito, F.; D’Alterio, N.; Puglia, I.; Berjaoui, S.; Colaianni, M.L.; et al. Epidemiology, pathological aspects and genome heterogeneity of feline morbillivirus in Italy. Vet. Microbiol. 2020, 240, 108484. [Google Scholar] [CrossRef] [PubMed]
- Sparkes, A.H.; Caney, S.; Chalhoub, S.; Elliott, J.; Finch, N.; Gajanayake, I.; Langston, C.; Lefebvre, H.P.; White, J.; Quimby, J. ISFM Consensus guidelines on the diagnosis and management of feline chronic kidney disease. J. Feline Med. Surg. 2016, 18, 219–239. [Google Scholar] [CrossRef] [PubMed]
- Marino, C.L.; Lascelles, B.D.; Vaden, S.L.; Gruen, M.E.; Marks, S.L. Prevalence and classification of chronic kidney disease in cats randomly selected from four age groups and in cats recruited for degenerative joint disease studies. J. Feline Med. Surg. 2014, 16, 465–472. [Google Scholar] [CrossRef] [Green Version]
- Beatty, J.A.; Sharp, W.P.; Duprex, W.P.; Munday, J.S. Novel feline virus. Emerging significance of gammaherpesvirus and morbillivirus infection. J. Feline Med. Surg. 2019, 21, 5–11. [Google Scholar] [CrossRef]
- Paepe, D. Early recognition of feline chronic kideny disease. Eur. J. Companion Anim. Pract. 2015, 25, 61–77. [Google Scholar]
- Darold, G.M.; Alfieri, A.A.; Araújo, J.P.; da Cruz, T.F.; Bertti, K.M.L.B.; da Silva, G.C.P.; Amude, A.M.; Muraro, L.S.; Lavorente, F.L.P.; Lunardi, M. High genetic diversity of paramyxoviruses infecting domestic cats in Western Brazil. Transbound. Emerg. Dis. 2020. [Google Scholar] [CrossRef]
- De Luca, E.; Sautto, G.A.; Crisi, P.E.; Lorusso, A. Feline morbillivirus infection in domestic cats: What have we learned so far? Viruses 2021, 13, 683. [Google Scholar] [CrossRef]
- Courcier, E.A.; O’Higgins, R.; Mellor, D.J.; Yam, P.S. Prevalence and risk factors for feline obesity in a first opinion practice in Glasgow, Scotland. J. Feline Med. Surg. 2010, 12, 746–753. [Google Scholar] [CrossRef]
- World Small Animal Veterinary Association. Muscle Condition Score. Available online: https://wsava.org/wp-content/uploads/2020/01/Muscle-Condition-Score-Chart-for-Cats.pdf (accessed on 2 July 2021).
- Piaton, E.; Fabre, M.; Goubin-Versini, I.; Bretz-Grenier, M.F.; Courtade-Saïdi, M.; Vincent, S.; Belleannée, G.; Thivolet, F.; Boutonnat, J.; Debaque, H.; et al. Guidelines for May-Grünwald-Giemsa staining in haematology and non-gynaecological cytopathology: Recommendations of the French Society of Clinical Cytology (SFCC) and of the French Association for Quality Assurance in Anatomic and Cytologic Pathology (AFAQAP). Cytopathology 2016, 27, 359–368. [Google Scholar] [CrossRef]
- International Renal Interest Society. IRIS 2019 Staging of CKD. Available online: http://www.iris-kidney.com/guidelines/staging.html (accessed on 12 December 2019).
- De Luca, E.; Crisi, P.E.; Di Domenico, M.; Malatesta, D.; Vincifori, G.; Di Tommaso, M.; Di Guardo, G.; Di Francesco, G.; Petrini, A.; Savini, G.; et al. A real-time RT-PCR assay for molecular identification and quantitation of feline morbillivirus RNA from biological specimens. J. Virol. Methods 2018, 258, 24–28. [Google Scholar] [CrossRef]
- Decaro, N.; Desario, C.; Miccolupo, A.; Campolo, M.; Parisi, A.; Martella, V.; Amorisco, F.; Lucente, M.S.; Lavazza, A.; Buonavoglia, C. Genetic analysis of feline panleukopenia viruses from cats with gastroenteritis. J. Gen. Virol. 2008, 89, 2290–2298. [Google Scholar] [CrossRef]
- Katoh, K.; Standley, D.M. MAFFT multiple sequence alignment software version 7: Improvements in performance and usability. Mol. Biol. Evol. 2013, 30, 772–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamura, K.; Nei, M. Estimation of the number of nucleotide substitutions in the control region of mitochondrial DNA in humans and chimpanzees. Mol. Biol. Evol. 1993, 10, 512–526. [Google Scholar] [CrossRef]
- Kumar, S.; Stecher, G.; Tamura, K. MEGA7: Molecular evolutionary genetics analysis version 7.0 for bigger datasets. Mol. Biol. Evol. 2016, 33, 1870–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marcacci, M.; de Luca, E.; Zaccaria, G.; Di Tommaso, M.; Mangone, I.; Aste, G.; Savini, G.; Boari, A.; Lorusso, A. Genome characterization of feline morbillivirus from Italy. J. Virol. Methods 2016, 234, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Donato, G.; de Luca, E.; Crisi, P.E.; Pizzurro, F.; Masucci, M.; Marcacci, M.; Cito, F.; Di Sabatino, D.; Boari, A.; D’Alterio, N.; et al. Isolation and genome sequences of two Feline Morbillivirus genotype 1 strains from Italy. Vet. Ital. 2019, 55, 179–182. [Google Scholar] [CrossRef] [PubMed]
- Busch, J.; Heilmann, R.M.; Vahlenkamp, T.W.; Sieg, M. Seroprevalence of infection with feline morbilliviruses is associated with FLUTD and increased blood creatinine concentrations in domestic cats. Viruses 2021, 13, 578. [Google Scholar] [CrossRef] [PubMed]
- Hosie, M.J.; Addie, D.; Belák, S.; Boucraut-Baralon, C.; Egberink, H.; Frymus, T.; Gruffydd-Jones, T.; Hartmann, K.; Lloret, A.; Lutz, H.; et al. Feline immunodeficiency. ABCD guidelines on prevention and management. J. Feline Med. Surg. 2009, 11, 57584. [Google Scholar] [CrossRef] [PubMed]
- Sieg, M.; Busch, J.; Eschke, M.; Böttcher, D.; Heenemann, K.; Vahlenkamp, A.; Reinert, A.; Seeger, J.; Heilmann, R.; Scheffler, K.; et al. A new genotype of feline morbillivirus infects primary cells of the lung, kidney, brain and peripheral blood. Viruses 2019, 11, 146. [Google Scholar] [CrossRef] [Green Version]
- Koide, R.; Sakaguchi, S.; Miyazawa, T. Basic biological characterization of feline morbillivirus. J. Vet. Med. Sci. 2015, 77, 565–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, E.J.; Ortega, V.; Aguilar, H.C. Feline morbillivirus, a new paramyxovirus possibly associated with feline kidney disease. Viruses 2020, 12, 501. [Google Scholar] [CrossRef]
- Crisi, P.E.; Dondi, F.; de Luca, E.; Di Tommaso, M.; Vasylyeva, K.; Ferlizza, E.; Savini, G.; Luciani, A.; Malatesta, D.; Lorusso, A.; et al. Early renal involvement in cats with natural feline morbillivirus infection. Animals 2020, 10, 828. [Google Scholar] [CrossRef]
- Jepson, R.E.; Syme, H.M.; Vallance, C.; Elliott, J. Plasma asymmetric dimethylarginine, symmetric dimethylarginine, l-arginine, and nitrite/nitrate concentrations in cats with chronic kidney disease and hypertension. J. Vet. Intern. Med. 2008, 22, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Hall, J.A.; Yerramilli, M.; Obare, E.; Yerramilli, M.; Jewell, D.E. Comparison of serum concentrations of symmetric dimethylarginine and creatinine as kidney function biomarkers in cats with chronic kidney disease. J. Vet. Intern. Med. 2014, 28, 1676–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Signalment and History | Physical Examination | CBC and Renal Profile Parameters [Reference Values] | Abnormality |
|---|---|---|---|
| Sex Male/Female Age group (months) Junior (6–24) Adult (25–96) Senior (>96) Breed Domestic shorthair (DSH) Domestic longhair (DLH) Pure Breed Lifestyle and origin Outoor Indoor Single-cat household Multi-cat household Rescue Cattery Foundling cat ^ Not-foundling cat Environment Urban (area with a high population density) Suburban (sites near outskirts of urban areas) Rural (area with a low population density and small settlements) | Body condition score (BCS) Muscle condition score (MCS) Lymph node enlargement Upper respiratory tract signs Lower respiratory tract signs Gastrointestinal signs Skin lesions Ocular lesions Oral lesions | Hemoglobin (Hb) [8.82–17.82 g/dL] Neutrophils [2.07–11.32 K/µL] Lymphocytes [0.83–7.57 K/µL] Monocytes [0.05–0.74 K/µL] Eosinophils [0.15–1.73 K/µL] Basophils [0.01–0.29 K/µL] Thrombocytes [136–660 K/µL] Symmetric Dimethylarginine (SDMA) [≤ 14 μg/dL] Serum Creatinine (sCr) [0.8–2.4 mg/dL] Blood Urea Nitrogen (BUN) [16–36 mg/dL] Phosphorus (PHOS) [3.1–7.5 mg/dL] Urine Specific Gravity (USG) [>1035] Urine Protein to Creatinine Ratio (UPC) [>0.4] Total Thyroxine (tT4) [1–3 µg/dL] | Anemia Neutrophilia/Neutropenia Lymphocytosis/Lymphopenia Monocytosis Eosinophilia/Eosinopenia Basophilia Thrombocytosis/Thrombocytopenia Increased SDMA Increased sCr Increased BUN/Decreased BUN Increased PHOS USG < 1035 Proteinuria * Increased tT4 |
| Signalment and History | Enrolled Cats | u+ | b+ | u+ and/or b+ | Ab+ | Ab+ and/or RNA+ |
|---|---|---|---|---|---|---|
| Sex | ||||||
| Male | 110 (49.3) | 21/107 (19.6) | 4/106 (3.8) | 22/103 (21.4) | 16/95 (16.8) | 30/92 (32.6) |
| Female | 113 (50.7) | 15/110 (13.6) | 1/105 (0.9) | 16/102 (15.7) | 12/98 (12.2) | 26/92 (28.3) |
| Age group | ||||||
| Junior | 91 (40.8) | 9/88 (10.22) | 2/90 (2.2) | 10/87 (11.5) | 9/84 (10.7) | 18/81 (22.2) |
| Adult | 79 (35.4) | 16/77 (20.8) | 2/72 (2.8) | 16/70 (22.9) | 9/64 (14) | 21/61 (34.4) |
| Senior | 53 (23.8) | 11/52 (21.2) | 1/49(2) | 12/48 (25) | 10/45 (22.2) | 17/42 (40.5) |
| Breed | ||||||
| DSH | 188 (84.3) | 33/182 (18.1) | 5/179 (2.8) | 35/173 (20.2) | 25/164 (15.2) | 52/156 (33.3) |
| DLH | 23 (10.3) | 3/23 (13) | 0 | 3/20 (15) | 3/19 (15.8) | 4/18 (22.2) |
| Pure Breed | 12 (5.4) | 0 | 0 | 0 | 0 | 0 |
| Maine Coon | 9 | 0 | 0 | 0 | 0 | 0 |
| Persian | 1 | 0 | 0 | 0 | 0 | 0 |
| Brithish Shorthair | 1 | 0 | 0 | 0 | 0 | 0 |
| Ragdoll | 1 | 0 | 0 | 0 | 0 | 0 |
| Lifestyle and origin | ||||||
| Outoor | 115 (51.6) | 21/111 (18.9) | 3/111 (2.7) | 23/107 (21.5) | 19/103 (18.5) | 35/97 (36) |
| Indoor | 108 (48.4) | 15/106 (14.2) | 2/100 (2) | 15/98 (15.3) | 9/90 (10) | 21/87 (24.1) |
| Single-cat household | 32 (29.6) | 8/32 (25) | 1/28 (3.6) | 7/28 (25) | 0 | 7/24 (29.2) |
| Multi-cat household | 35 (32.4) | 1/35 (2.9) | 0 | 1/35 (2.9) | 1/30 (3.3) | 2/30 (6.7) |
| Rescue Cattery | 41 (38) | 6/39 (15.4) | 1/37 (2.7) | 7/35 (20) | 8/36 (22.2) | 12/33 (36.4) |
| Foundling cat | 57 (52.8) | 9/55 (16.4) | 1/53 (1.9) | 10/51 (19.6) | 8/52 (15.4) | 15/49 (30.6) |
| Not-foundling cat | 51 (47.2) | 6/51 (11.8) | 1/47 (2.1) | 5/47 (10.6) | 1/38 (2.6) | 6/38 (15.8) |
| Environment | ||||||
| Urban | 148 (66.4) | 21/145 (14.5) | 3/143 (2.1) | 21/140 (15) | 16/129 (12.4) | 33/126 (26.2) |
| Suburban | 61 (27.4) | 11/59 (18.7) | 2/55 (3.6) | 13/53 (24.5) | 11/53 (20.8) | 18/49 (36.7) |
| Rural | 14 (6.3) | 4/13 (30.8) | 0 | 4/12 (33.3) | 1/11 (9.1) | 5/9 (55.6) |
| TOTAL | 223 | 36/223 (16.1) | 5/211 (2.4) | 38/205 (18.5) | 28/193 (14.5) | 56/184 (30.4) |
| Variable | Enrolled Cats | u+ | b+ | u+ and/or b+ | Ab+ | Ab+ and/or RNA+ |
|---|---|---|---|---|---|---|
| Body Condition Score | 40/223 (17.9) | |||||
| n (%) | 5/36 (13.9) | 0/5 | 5/38 (13.2) | 9/28 (32.1) | 13/56 (23.2) | |
| rs | 0.046 | 0.073 | 0.055 | −0.165 | −0.124 | |
| p | 0.492 | 0.291 | 0.432 | 0.022 * | 0.094 | |
| Muscle Condition Score | 50/216 (23.1) | |||||
| n (%) | 8/35 (22.9) | 0/5 | 8/37 (21.6) | 8/26 (30.8) | 15/53 (28.3) | |
| rs | 0.003 | 0.086 | 0.014 | −0.083 | −0.106 | |
| p | 0.965 | 0.216 | 0.840 | 0.254 | 0.157 | |
| Lymph node enlargement | 64/216 (29.6) | |||||
| n (%) | 11/36 (30.6) | 0/5 | 11/38 (28.9) | 10/28 (35.7) | 17/56 (30.4) | |
| rs | 0.009 | −0.103 | −0.015 | 0.041 | −0.017 | |
| p | 0.895 | 0.135 | 0.831 | 0.570 | 0.823 | |
| Upper respiratory tract signs | 18/216 (8.3) | |||||
| n (%) | 6/36 (16.7) | 2/5 (40) | 8/38 (21) | 4/28 (14.3) | 9/56 (16.1) | |
| rs | 0.135 | 0.183 | 0.220 | 0.080 | 0.173 | |
| p | 0.048 * | 0.008 * | 0.002 * | 0.271 | 0.019 * | |
| Lower respiratory tract signs | 3/216 (1.4) | |||||
| n (%) | 0/36 | 1/5 (20) | 1/38 (2.6) | 1/28 (3.6) | 1/56 (1.8) | |
| rs | −0.053 | 0.244 | 0.046 | 0.067 | 0.008 | |
| p | 0.438 | 0.000 * | 0.512 | 0.353 | 0.913 | |
| Gastrointestinal signs | 19/216 (8.8) | |||||
| n (%) | 6/36 (16.7) | 2/5 (40) | 6/38 (15.8) | 6/28 (21.4) | 10/56 (17.9) | |
| rs | 0.124 | 0.175 | 0.118 | 0.183 | 0.215 | |
| p | 0.068 | 0.011 * | 0.094 | 0.011 * | 0.003 * | |
| Skin lesions | 44/216 (20.4) | |||||
| n (%) | 11/36 (30.6) | 2/5 (40) | 12/38 (31.6) | 10/28 (35.7) | 17/56 (30.4) | |
| rs | 0.113 | 0.076 | 0.130 | 0.152 | 0.159 | |
| p | 0.097 | 0.276 | 0.064 | 0.034 * | 0.032 * | |
| Ocular lesions | 22/216 (10.2) | |||||
| n (%) | 7/36 (19.4) | 1/5 (20) | 8/38 (21) | 4/28 (14.3) | 9/56 (16.1) | |
| rs | 0.138 | 0.052 | 0.169 | 0.061 | 0.125 | |
| p | 0.043 * | 0.453 | 0.015 * | 0.396 | 0.091 | |
| Oral lesions | 46/216 (21.3) | |||||
| n (%) | 10/36 (27.8) | 2/5 (40) | 11/38 (28.9) | 12/28 (42.9) | 18/56 (32.1) | |
| rs | 0.071 | 0.073 | 0.099 | 0.204 | 0.177 | |
| p | 0.300 | 0.292 | 0.159 | 0.004 * | 0.016 * |
| Parameter and Abnormalities | Enrolled Cats | u+ | b+ | u+ and/or b+ | Ab+ | Ab+ and/or RNA+ |
|---|---|---|---|---|---|---|
| Hb | ||||||
| Anemia | 41/223 (18.4) | 9/36 (25) | 1/5 (20) | 9/38 (23.7) | 9/28 (32.1) | 16/56 (28.6) |
| Neutrophils | ||||||
| Neutrophilia | 42/194 (21.6) | 11/31 (35.4) | 2/5 (40) | 11/33 (33.3) | 11/28 (39.3) | 19/51 (37.2) |
| Neutropenia | 8/194 (4.1) | 0/31 | 0/5 | 0/33 | 0/28 | 0/51 |
| Lymphocytes | ||||||
| Lymphocytosis | 6/194 (3.1) | 0/31 | 1/4 (25) | 1/33 (3) | 0/28 | 1/51 (1.9) |
| Lymphopenia | 17/194 (8.8) | 4/31 (12.9) | 1/4 (25) | 4/33 (12.1) | 1/28 (3.6) | 4/51 (7.8) |
| Monocytes | ||||||
| Monocytosis | 34/194 (17.5) | 9/31 (29) | 1/5 (20) | 11/33 (33.3) | 7/28 (25) | 16/51 (31.4) |
| Eosinophils | ||||||
| Eosinophilia | 10/194 (5.1) | 1/31 (3.2) | 0/5 | 1/33 (3) | 2/28 (7.1) | 2/51 (3.9) |
| Eosinopenia | 20/194 (10.3) | 4/31 (12.9) | 2/5 (40) | 5/33 (15.2) | 2/28 (7.1) | 6/51 (11.8) |
| Basophils | ||||||
| Basophilia | 1/194 (0.5) | 1/31 (3.2) | 0/5 | 1/33 (3) | 1/28 (3.6) | 1/51 (1.9) |
| Thrombocytes | ||||||
| Thrombocytosis | 7/199 (3.5) | 3/32 (9.4) | 0/5 | 3/34 (8.8) | 4/28 (14.3) | 7/52 (13.5) |
| Thrombocytopenia | 23/199 (11.6) | 2/32 (6.2) | 0/5 | 2/34 (5.9) | 2/28 (7.1) | 3/52 (5.8) |
| SDMA | ||||||
| Increased SDMA | 64/197 (32.5) | 9/35 (25.7) | 2/5 (40) | 10/38 (26.3) | 13/26 (50) | 19/54 (35.2) |
| sCr | ||||||
| Increased sCr | 18/205 (8.8) | 2/36 (5.6) | 1/5 (20) | 2/38 (5.3) | 5/27 (18.5) | 6/55 (10.9) |
| BUN | ||||||
| Increased BUN | 27/177 (15.2) | 5/33 (15.2) | 2/4 (50) | 5/34 (14.7) | 6/23 (26.1) | 10/50 (20) |
| Decreased BUN | 12/177 (6.8) | 2/33 (6.1) | 2/4 (50) | 2/34 (5.9) | 1/23 (4.3) | 3/50 (6) |
| PHOS | ||||||
| Increased PHOS | 47/140 (33.6) | 5/22 (22.7) | 0/2 | 5/23 (21.7) | 2/18 (11.1) | 7/38 (18.4) |
| USG | ||||||
| USG < 1035 | 56/208 (26.9) | 11/36 (30.6) | 3/4 (75) | 12/37 (32.4) | 8/26 (30.8) | 17/54 (31.5) |
| UPC | ||||||
| BP | 19/159 (11.9) | 3/30 (10) | 0/4 | 3/31 (9.7) | 2/16 (12.5) | 3/39 (7.7) |
| P | 21/159 (13.2) | 5/30 (16.7) | 2/4 (50) | 5/31 (16.1) | 3/16 (18.7) | 6/39 (15.3) |
| tT4 | ||||||
| Increased tT4 | 10/38 (26.3) | 1/11 (9.1) | 0/1 | 1/12 (8.3) | 2/7 (28.6) | 3/14 (21.4) |
| Variable | u+ | b+ | u+ and/or b+ | Ab+ | Ab+ and/or RNA+ |
|---|---|---|---|---|---|
| Anemia | |||||
| rs | 0.075 | 0.006 | 0.063 | 0.136 | 0.172 |
| p | 0.265 | 0.930 | 0.368 | 0.060 | 0.020 * |
| Neutrophilia | |||||
| rs | 0.163 | 0.080 | 0.164 | 0.191 | 0.274 |
| p | 0.023 * | 0.271 | 0.025 * | 0.012 * | 0.000 * |
| Monocytosis | |||||
| rs | 0.132 | 0.266 | 0.198 | 0.060 | 0.207 |
| p | 0.067 | 0.000 * | 0.007 * | 0.429 | 0.007 * |
| Eosinopenia | |||||
| rs | −0.050 | −0.151 | −0.090 | 0.069 | −0.032 |
| p | 0.485 | 0.037 * | 0.222 | 0.367 | 0.682 |
| Basophilia | |||||
| rs | 0.165 | −0.12 | 0.158 | 0.174 | 0.117 |
| p | 0.021 * | 0.870 | 0.031 * | 0.022 * | 0.130 |
| Thrombocytosis | |||||
| rs | 0.126 | 0.037 | 0.129 | 0.160 | 0.249 |
| p | 0.077 | 0.610 | 0.075 | 0.032 * | 0.001 * |
| sCr | |||||
| rs | −0.053 | 0.071 | −0.044 | 0.145 | 0.077 |
| p | 0.454 | 0.319 | 0.539 | 0.049 * | 0.308 |
| USG | |||||
| rs | −0.037 | −0.165 | −0.084 | −0.038 | −0.087 |
| p | 0.591 | 0.020 * | 0.240 | 0.609 | 0.247 |
| Clinical Group | n | u+ | b+ | u+ and/or b+ | Ab+ | Ab+ and/or RNA+ |
|---|---|---|---|---|---|---|
| Healthy | 12 | 1 | 0 | 1 | 1 | 2 |
| Unhealthy without CKD | 92 | 20 | 1 | 20 | 8 | 23 |
| CKD | 88 | 15 | 3 | 16 | 15 | 27 |
| Virus and Sample | n | Positive (%) |
|---|---|---|
| FIV | ||
| Serum | 209 | 27 (12.9) |
| EDTA blood | 211 | 21 (10) |
| FeLV | ||
| EDTA blood | 211 | 3 (1.4) |
| FCoV | ||
| EDTA blood | 174 | 33 (19) |
| FPV | ||
| EDTA blood | 105 | 8 (7.6) |
| Variable | FeMV and FIV | FeMV and FCoV |
|---|---|---|
| Age | ||
| rs | 0.396 | 0.000 |
| p | 0.003 * | 1.000 |
| Enlarged Lymph nodes | ||
| rs | 0.412 | −0.065 |
| p | 0.002 * | 0.651 |
| BCS | ||
| rs | −0.331 | −0.239 |
| p | 0.013 * | 0.095 |
| MCS | ||
| rs | −0.161 | −0.324 |
| p | 0.251 | 0.026 * |
| Thrombocytosis | ||
| rs | 0.011 | 0.329 |
| p | 0.936 | 0.024 * |
| qPCRFeMV u and/or b | Ab | n |
|---|---|---|
| Positive | Positive | 8 |
| Positive | Negative | 28 |
| Negative | Positive | 20 |
| Negative | Negative | 128 |
| qPCRFeMV u and/or b | Ab | Variable | p | OR | 95% CI |
|---|---|---|---|---|---|
| Positive | Positive | Oral lesions | 0.0377 | 5.095 | 1.371–18.32 |
| FIV RNA+ | 0.0134 | 10.37 | 2.286–57.91 | ||
| Positive | Negative | Single-cat household | 0.017 | 11.53 | 1.672–133.6 |
| Neutrophilia | 0.04 | 2.949 | 1.048–8.073 | ||
| Monocytosis | 0.007 | 4.058 | 1.552–11.15 | ||
| Negative | Positive | Low BCS | 0.0071 | 4.353 | 148–11.19 |
| Oral lesions | 0.0288 | 3.397 | 1.96–9.656 | ||
| Gastrointestinal signs | 0.0303 | 5.083 | 1.467–17.52 | ||
| Anemia | 0.0094 | 4.074 | 1.399–10.56 | ||
| Neutrophilia | 0.0048 | 4.524 | 1.651–11.74 |
| 0 | 3 d | 7 d | 10 d | 14 d | 21 d | 30 d | 45 d | 60 d | 75 d | 90 d | 120 d | 150 d | 180 d | 210 d | 240 d | 270 d | 300 d | 360 d | 510 d | 570 d | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cat 1. | |||||||||||||||||||||
| IIF assay | |||||||||||||||||||||
| EDTA blood PCR | neg | ||||||||||||||||||||
| Urine PCR | pos | pos | |||||||||||||||||||
| Cat 2. | |||||||||||||||||||||
| IIF assay | pos | neg | |||||||||||||||||||
| EDTA blood PCR | neg | neg | neg | neg | |||||||||||||||||
| Urine PCR | pos | neg | pos | neg | |||||||||||||||||
| Cat 3. | |||||||||||||||||||||
| IIF assay | neg | neg | neg | ||||||||||||||||||
| EDTA blood PCR | neg | neg | neg | ||||||||||||||||||
| Urine PCR | pos | pos | pos | pos | neg | ||||||||||||||||
| Cat. 4 | |||||||||||||||||||||
| IIF assay | neg | pos | |||||||||||||||||||
| EDTA blood PCR | pos | pos | |||||||||||||||||||
| Urine PCR | neg | ||||||||||||||||||||
| Cat 5. | |||||||||||||||||||||
| IIF assay | neg | neg | |||||||||||||||||||
| EDTA blood PCR | neg | ||||||||||||||||||||
| Urine PCR | pos | pos | |||||||||||||||||||
| Cat 6. | |||||||||||||||||||||
| IIF assay | pos | ||||||||||||||||||||
| EDTA blood PCR | neg | neg | |||||||||||||||||||
| Urine PCR | pos | pos | |||||||||||||||||||
| Cat 7. | |||||||||||||||||||||
| IIF assay | pos | pos | |||||||||||||||||||
| EDTA blood PCR | neg | neg | |||||||||||||||||||
| Urine PCR | neg | neg | |||||||||||||||||||
| Cat 8. | |||||||||||||||||||||
| IIF assay | neg | neg | neg | ||||||||||||||||||
| EDTA blood PCR | neg | pos | pos | neg | |||||||||||||||||
| Urine PCR | neg | neg | neg | neg | neg | neg | neg | neg | neg | ||||||||||||
| Cat 9. | |||||||||||||||||||||
| IIF assay | neg | neg | |||||||||||||||||||
| EDTA blood PCR | neg | ||||||||||||||||||||
| Urine PCR | pos | pos | pos | ||||||||||||||||||
| Cat 10. | |||||||||||||||||||||
| IIF assay | pos | pos | neg | ||||||||||||||||||
| EDTA blood PCR | neg | neg | neg | neg | |||||||||||||||||
| Urine PCR | neg | pos | pos | pos | pos | pos | pos | neg | neg | neg | neg | ||||||||||
| Cat 11. | |||||||||||||||||||||
| IIF assay | pos | neg | |||||||||||||||||||
| EDTA blood PCR | neg | neg | |||||||||||||||||||
| Urine PCR | neg | neg | |||||||||||||||||||
| Cat 12. | |||||||||||||||||||||
| IIF assay | pos | ||||||||||||||||||||
| EDTA blood PCR | neg | neg | |||||||||||||||||||
| Urine PCR | pos | pos | |||||||||||||||||||
| Cat 13. | |||||||||||||||||||||
| IIF assay | neg | ||||||||||||||||||||
| EDTA blood PCR | neg | ||||||||||||||||||||
| Urine PCR | pos | pos | pos |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donato, G.; Masucci, M.; De Luca, E.; Alibrandi, A.; De Majo, M.; Berjaoui, S.; Martino, C.; Mangano, C.; Lorusso, A.; Pennisi, M.G. Feline Morbillivirus in Southern Italy: Epidemiology, Clinico-Pathological Features and Phylogenetic Analysis in Cats. Viruses 2021, 13, 1449. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081449
Donato G, Masucci M, De Luca E, Alibrandi A, De Majo M, Berjaoui S, Martino C, Mangano C, Lorusso A, Pennisi MG. Feline Morbillivirus in Southern Italy: Epidemiology, Clinico-Pathological Features and Phylogenetic Analysis in Cats. Viruses. 2021; 13(8):1449. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081449
Chicago/Turabian StyleDonato, Giulia, Marisa Masucci, Eliana De Luca, Angela Alibrandi, Massimo De Majo, Shadia Berjaoui, Camillo Martino, Cyndi Mangano, Alessio Lorusso, and Maria Grazia Pennisi. 2021. "Feline Morbillivirus in Southern Italy: Epidemiology, Clinico-Pathological Features and Phylogenetic Analysis in Cats" Viruses 13, no. 8: 1449. https://0-doi-org.brum.beds.ac.uk/10.3390/v13081449