
Immune Response 5–7 Months after Vaccination against SARS-CoV-2 in Elderly Nursing Home Residents in the Czech Republic: Comparison of Three Vaccines

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Samples
2.2. Evaluation of Humoral Immunity
2.3. Evaluation of Cellular Immunity
2.4. Statistical Analysis
3. Results
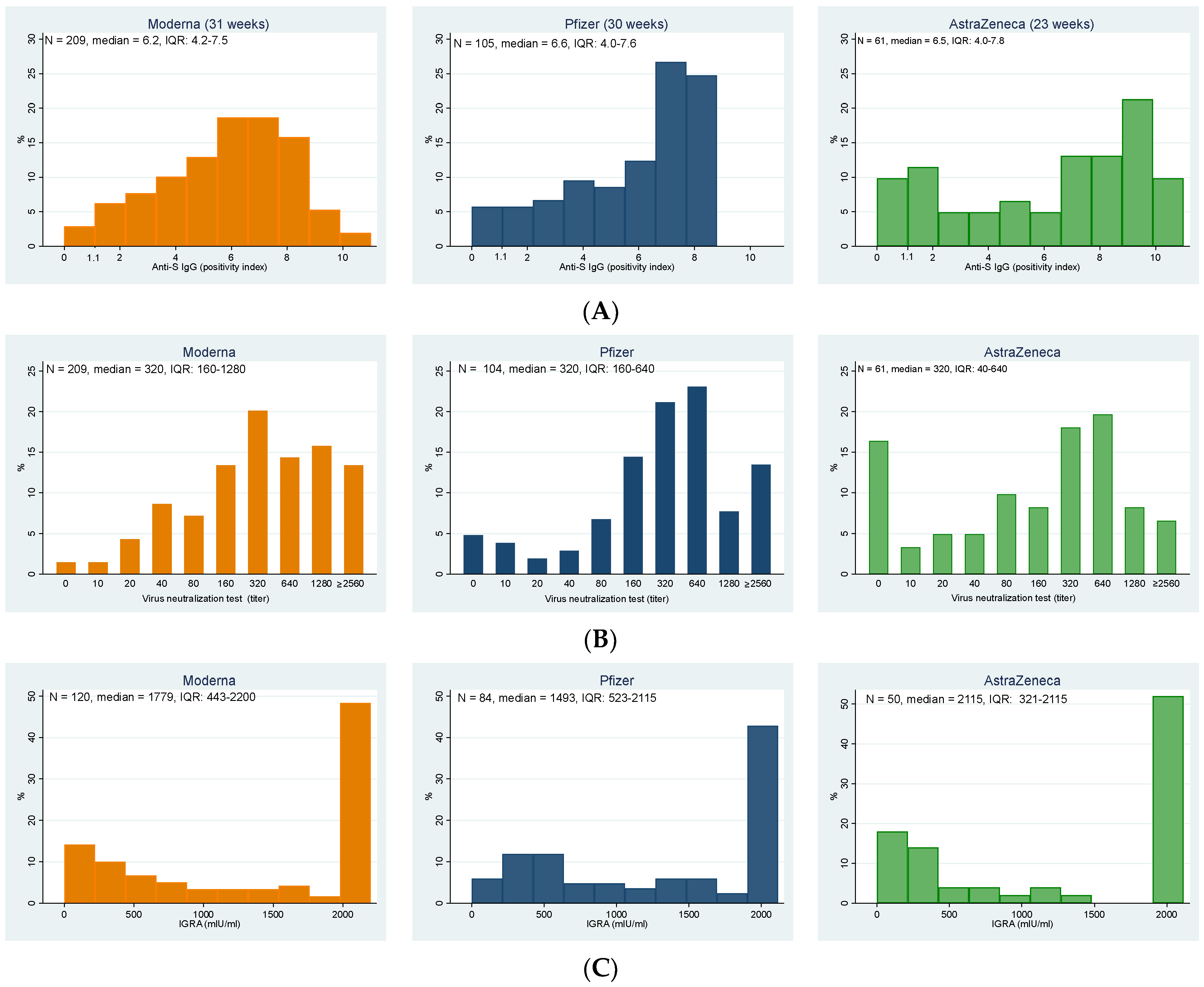
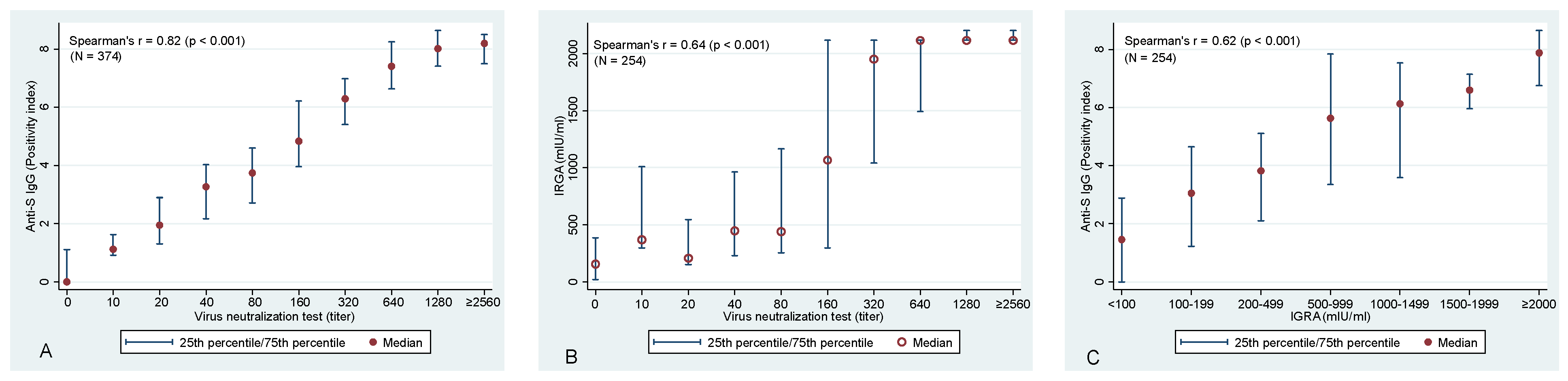
3.1. Humoral Immunity
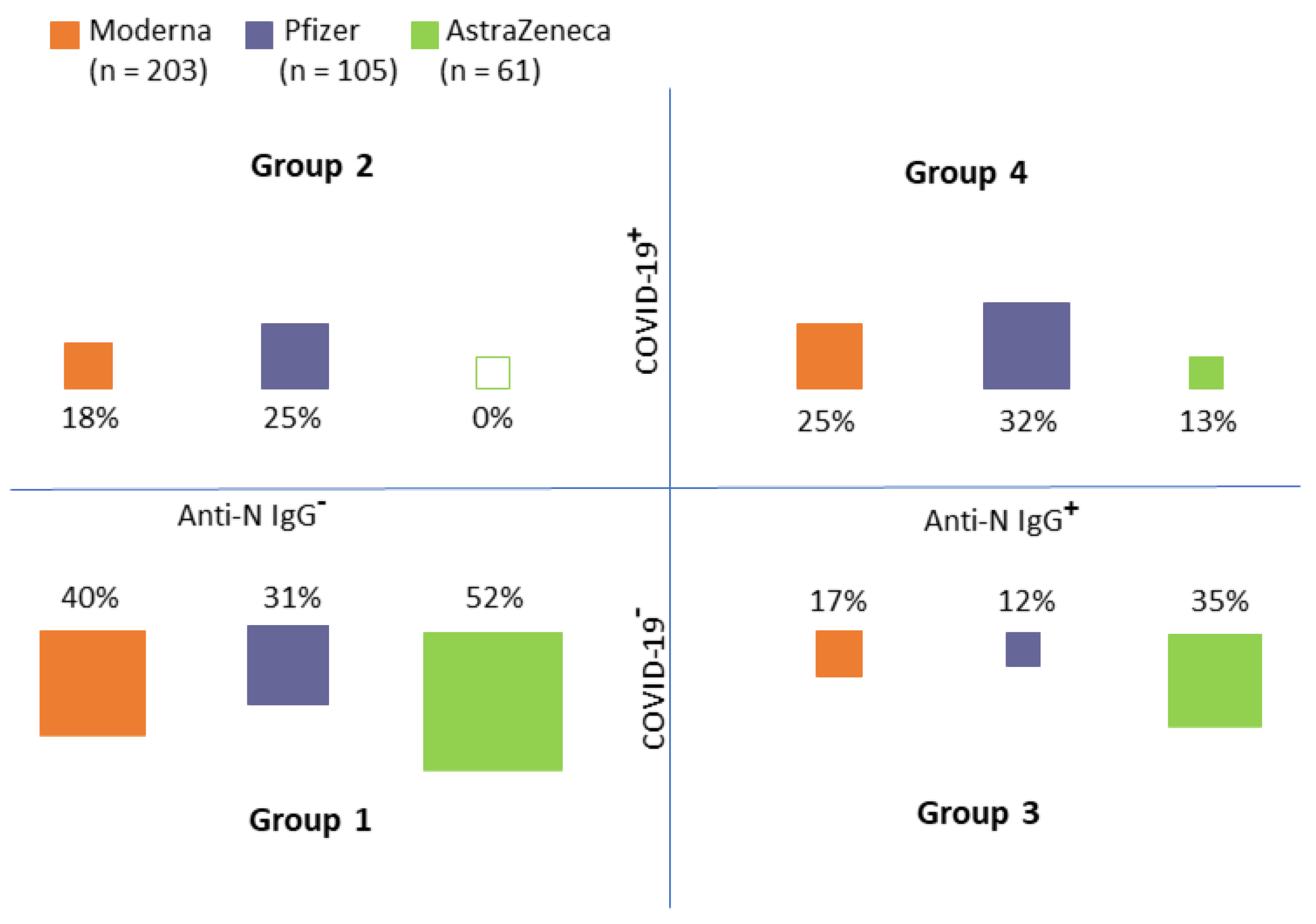
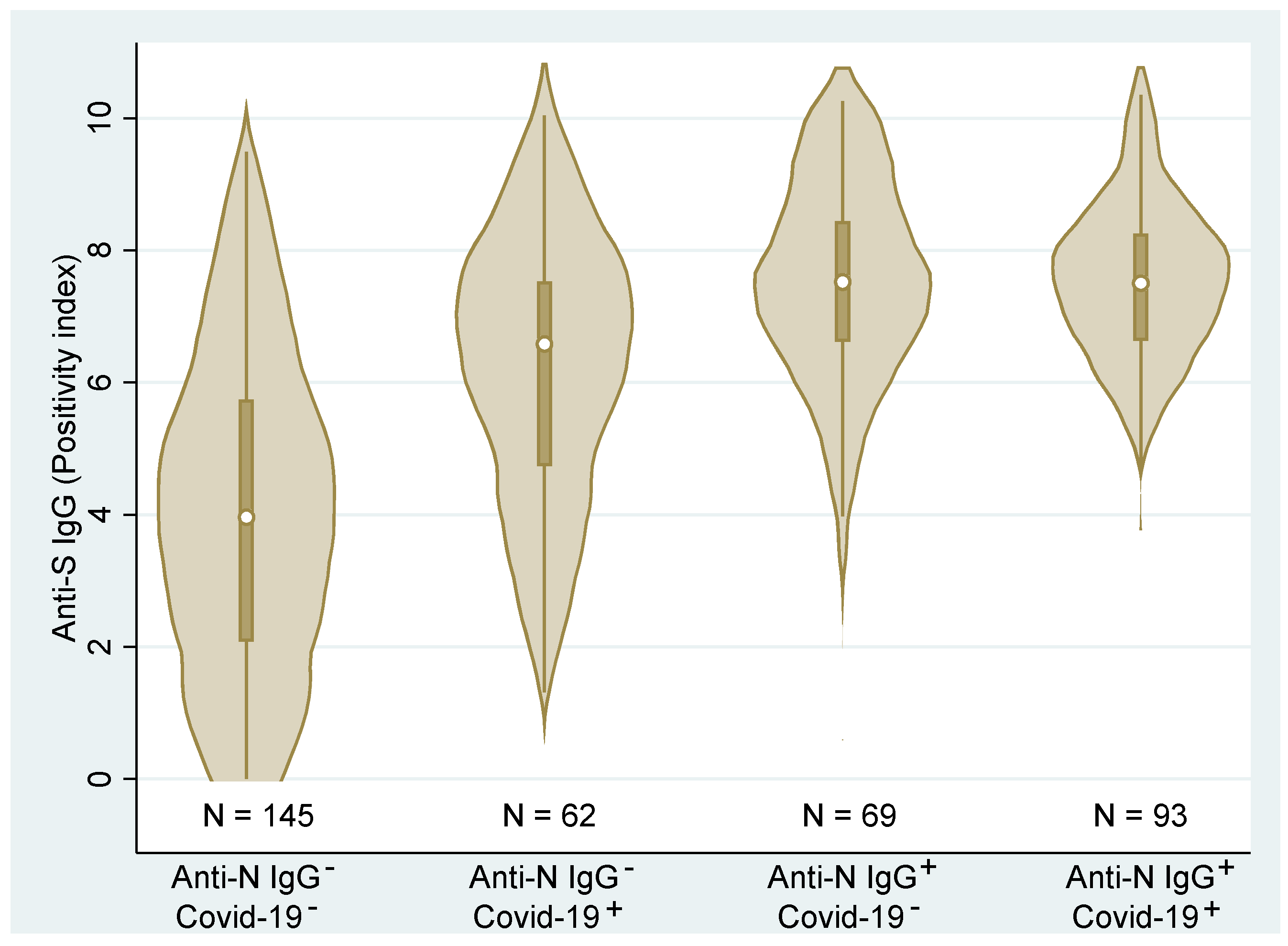
3.2. Immune Response in Association with the Personal History of COVID-19
- Group 1: No COVID-19 record in personal history/no anti-N IgG
- Group 2: COVID-19 record in personal history/no anti-N IgG
- Group 3: No COVID-19 record in personal history/anti-N IgG positive
- Group 4: COVID-19 record in personal history/anti-N IgG positive
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldberg, Y.; Mandel, M.; Bar-On, Y.M.; Bodenheimer, O.; Freedman, L.; Ash, N.; Alroy-Preis, S.; Huppert, A.; Milo, R. Protection and waning of natural and hybrid COVID-19 immunity. Medrxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Havervall, S.; Ng, H.; Jernbom Falk, A.; Greilert-Norin, N.; Månberg, A.; Marking, U.; Laurén, I.; Gabrielsson, L.; Salomonsson, A.-C.; Aguilera, K.; et al. Robust humoral and cellular immune responses and low risk for reinfection at least 8 months following asymptomatic to mild COVID-19. J. Intern. Med. 2022, 291, 72–80. [Google Scholar] [CrossRef]
- León, T.M.; Dorabawila, V.; Nelson, L.; Lutterloh, E.; Bauer, U.E.; Backenson, B.; Bassett, M.T.; Henry, H.; Bregman, B.; Midgley, C.M.; et al. COVID-19 Cases and Hospitalizations by COVID-19 Vaccination Status and Previous COVID-19 Diagnosis—California and New York, May–November 2021. Morb. Mortal. Wkly. Rep. 2022, 71, 125–131. [Google Scholar] [CrossRef]
- Blain, H.; Tuaillon, E.; Gamon, L.; Pisoni, A.; Miot, S.; Rolland, Y.; Picot, M.-C.; Bousquet, J. Antibody response after one and two jabs of the BNT162b2 vaccine in nursing home residents: The CONsort-19 study. Allergy 2022, 77, 271–281. [Google Scholar] [CrossRef]
- Hartley, G.E.; Edwards, E.S.J.; Aui, P.M.; Varese, N.; Stojanovic, S.; McMahon, J.; Peleg, A.Y.; Boo, I.; Drummer, H.E.; Hogarth, P.M.; et al. Rapid generation of durable B cell memory to SARS-CoV-2 spike and nucleocapsid proteins in COVID-19 and convalescence. Sci. Immunol. 2020, 5, eabf8891. [Google Scholar] [CrossRef]
- Figueiredo-Campos, P.; Blankenhaus, B.; Mota, C.; Gomes, A.; Serrano, M.; Ariotti, S.; Costa, C.; Nunes-Cabaço, H.; Mendes, A.M.; Gaspar, P.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies in COVID-19 patients and healthy volunteers up to 6 months post disease onset. Eur. J. Immunol. 2020, 50, 2025–2040. [Google Scholar] [CrossRef]
- Post, N.; Eddy, D.; Huntley, C.; van Schalkwyk, M.C.I.; Shrotri, M.; Leeman, D.; Rigby, S.; Williams, S.V.; Bermingham, W.H.; Kellam, P.; et al. Antibody response to SARS-CoV-2 infection in humans: A systematic review. PLoS ONE 2020, 15, e0244126. [Google Scholar] [CrossRef]
- Geisen, U.M.; Sümbül, M.; Tran, F.; Berner, D.K.; Reid, H.M.; Vullriede, L.; Ciripoi, M.; Longardt, A.C.; Hoff, P.; Morrison, P.J.; et al. Humoral protection to SARS-CoV2 declines faster in patients on TNF alpha blocking therapies. RMD Open 2021, 7, e002008. [Google Scholar] [CrossRef]
- Irsara, C.; Egger, A.E.; Prokop, W.; Nairz, M.; Loacker, L.; Sahanic, S.; Pizzini, A.; Sonnweber, T.; Holzer, B.; Mayer, W.; et al. Clinical validation of the Siemens quantitative SARS-CoV-2 spike IgG assay (sCOVG) reveals improved sensitivity and a good correlation with virus neutralization titers. Clin. Chem. Lab. Med. (CCLM) 2021, 59, 1453–1462. [Google Scholar] [CrossRef]
- Mendrone-Junior, A.; Dinardo, C.L.; Ferreira, S.C.; Nishya, A.; Salles, N.A.; de Almeida Neto, C.; Hamasaki, D.T.; Facincani, T.; de Oliveira Alves, L.B.; Machado, R.R.G.; et al. Correlation between SARS-CoV-2 antibody screening by immunoassay and neutralizing antibody testing. Transfusion 2021, 61, 1181–1190. [Google Scholar] [CrossRef]
- Toor, S.M.; Saleh, R.; Sasidharan Nair, V.; Taha, R.Z.; Elkord, E. T-cell responses and therapies against SARS-CoV-2 infection. Immunology 2021, 162, 30–43. [Google Scholar] [CrossRef]
- Murugesan, K.; Jagannathan, P.; Pham, T.D.; Pandey, S.; Bonilla, H.F.; Jacobson, K.; Parsonnet, J.; Andrews, J.R.; Weiskopf, D.; Sette, A.; et al. Interferon-γ Release Assay for Accurate Detection of Severe Acute Respiratory Syndrome Coronavirus 2 T-Cell Response. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 73, e3130–e3132. [Google Scholar] [CrossRef]
- Mehta, H.B.; Li, S.; Goodwin, J.S. Risk Factors Associated with SARS-CoV-2 Infections, Hospitalization, and Mortality among US Nursing Home Residents. JAMA Netw Open 2021, 4, e216315. [Google Scholar] [CrossRef]
- Collier, D.A.; Ferreira, I.A.T.M.; Kotagiri, P.; Datir, R.P.; Lim, E.Y.; Touizer, E.; Meng, B.; Abdullahi, A.; Baker, S.; Dougan, G.; et al. Age-related immune response heterogeneity to SARS-CoV-2 vaccine BNT162b2. Nature 2021, 596, 417–422. [Google Scholar] [CrossRef]
- Witkowski, W.; Gerlo, S.; De Smet, E.; Wejda, M.; Acar, D.; Callens, S.; Heytens, S.; Padalko, E.; Vercruysse, H.; Cools, P.; et al. Humoral and Cellular Responses to COVID-19 Vaccination Indicate the Need for Post-Vaccination Testing in Frail Population. Vaccines 2022, 10, 260. [Google Scholar] [CrossRef]
- Mravčík, V.; Husa, P.; Kumpanová Valachovičová, S.; Vobořil, J. Pokles hladiny neutralizačních protilátek po očkování proti SARS-CoV-2 u seniorů: Výsledky observační studie v Jihomoravském kraji. Epidemiol. Mikrobiol. Imunol. 2022, in press.
- Šimánek, V.; Pecen, L.; Krátká, Z.; Fürst, T.; Řezáčková, H.; Topolčan, O.; Fajfrlík, K.; Sedláček, D.; Šín, R.; Pazdiora, P.; et al. Five Commercial Immunoassays for SARS-CoV-2 Antibody Determination and Their Comparison and Correlation with the Virus Neutralization Test. Diagnostics 2021, 11, 593. [Google Scholar] [CrossRef]
- Cohn, B.A.; Cirillo, P.M.; Murphy, C.C.; Krigbaum, N.Y.; Wallace, A.W. SARS-CoV-2 vaccine protection and deaths among US veterans during 2021. Science 2021, 375, 331–336. [Google Scholar] [CrossRef]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E. The impact of SARS-CoV-2 vaccination on Alpha & Delta variant transmission. Medrxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Mazagatos, C.; Monge, S.; Olmedo, C.; Vega, L.; Gallego, P.; Martín-Merino, E.; Sierra, M.J.; Limia, A.; Larrauri, A. Effectiveness of mRNA COVID-19 vaccines in preventing SARS-CoV-2 infections and COVID-19 hospitalisations and deaths in elderly long-term care facility residents, Spain, weeks 53 2020 to 13 2021. Eurosurveillance 2021, 26, 2100452. [Google Scholar] [CrossRef]
- Berec, L.; Šmíd, M.; Přibylová, L.; Májek, O.; Pavlík, T.; Jarkovský, J.; Zajíček, M.; Weiner, J.; Barusová, T.; Trnka, J. Real-life protection provided by vaccination, booster doses and previous infection against COVID-19 infection, hospitalisation or death over time in the Czech Republic: A whole country retrospective view. Medrxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Pierobon, A.; Zotto, A.D.; Antico, A.; De Antoni, M.E.; Vianello, L.; Gennari, M.; Di Caprio, A.; Russo, F.; Brambilla, G.; Saugo, M. Outbreak of SARS-CoV-2 B.1.617.2 (delta) variant in a nursing home 28 weeks after two doses of mRNA anti-COVID-19 vaccines: Evidence of a waning immunity. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2021, 28, 614.e5–614.e7. [Google Scholar] [CrossRef] [PubMed]
- San Segundo, D.; Comins-Boo, A.; Lamadrid-Perojo, P.; Irure-Ventura, J.; Castillo-Otí, J.M.; Wallman, R.; Calvo-Montes, J.; Méndez-Legaza, J.M.; Baamonde-Calzada, C.; Sánchez-Molina, I.; et al. COVID-19 mRNA Based Vaccine Immune-Response Assessment in Nursing Home Residents for Public Health Decision. Vaccines 2021, 9, 1429. [Google Scholar] [CrossRef] [PubMed]
- Homza, M.; Zelena, H.; Janosek, J.; Tomaskova, H.; Jezo, E.; Kloudova, A.; Mrazek, J.; Svagera, Z.; Prymula, R. COVID-19 antigen testing: Better than we know? A test accuracy study. Infect. Dis. 2021, 53, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Pannus, P.; Neven, K.Y.; De Craeye, S.; Heyndrickx, L.; Vande Kerckhove, S.; Georges, D.; Michiels, J.; Francotte, A.; Van Den Bulcke, M.; Zrein, M.; et al. Poor antibody response to BioNTech/Pfizer COVID-19 vaccination in SARS-CoV-2 naïve residents of nursing homes. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, ciab998. [Google Scholar] [CrossRef]
- Kontopoulou, K.; Nakas, C.T.; Ainatzoglou, A.; Ifantidou, A.; Ntotsi, P.; Katsioulis, C.; Papazisis, G. Immunogenicity of the BNT162b2 Mrna COVID-19 vaccine in elderly people over 85 years of age in Greece: The GREVAXIMO study. Aging Clin. Exp. Res. 2021, 33, 3385–3389. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Rahman, M.M.; Masum, M.H.U.; Wajed, S.; Talukder, A. A comprehensive review on COVID-19 vaccines: Development, effectiveness, adverse effects, distribution and challenges. Virusdisease 2022, 33, 1–22. [Google Scholar] [CrossRef]
- Gazit, S.; Shlezinger, R.; Perez, G.; Lotan, R.; Peretz, A.; Ben-Tov, A.; Cohen, D.; Muhsen, K.; Chodick, G.; Patalon, T. Comparing SARS-CoV-2 natural immunity to vaccine-induced immunity: Reinfections versus breakthrough infections. Medrxiv Prepr. Serv. Health Sci. 2021. [Google Scholar] [CrossRef]
- Shrestha, N.K.; Burke, P.C.; Nowacki, A.S.; Terpeluk, P.; Gordon, S.M. Necessity of COVID-19 Vaccination in Persons Who Have Already Had COVID-19. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2022, ciac022. [Google Scholar] [CrossRef]
- Kojima, N.; Roshani, A.; Brobeck, M.; Baca, A.; Klausner, J.D. Incidence of SARS-CoV-2 infection among previously infected or vaccinated employees. Int. J. Infect. Dis. 2022, 118, 21–23. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Moderna | Pfizer | AstraZeneca | p-Value * | |
|---|---|---|---|---|---|
| n (%) | 375 (100) | 209 (55.7) | 105 (28.0) | 61 (16.3) | <0.001 |
| Age (mean ± SD) | 80.2 ± 8.45 | 82.5 ± 7.97 | 73.8 ± 6.43 | 83.4 ± 7.22 | <0.001 + |
| Women (%) | 258 (68.8) | 159 (76.1) | 56 (53.3) | 43 (70.5) | <0.001 |
| Men (%) | 117 (29.5) | 50 (23.9) | 49 (46.7) | 18 (29.5) | |
| Vaccination-to-test period—median (IQR), (weeks) | 30 (28–31) | 31 (29–32) | 30 (30–30) | 23 (23–23) | <0.001 |
| N of participants with history of COVID-19 (medical records + N-antibodies) | 224 (59.7) | 122 (58.4) | 73 (69.5) | 29 (47.5) | 0.017 |
| N of participants with history of COVID-19 based on medical records (%) | 155 (41.3) | 87 (41.6) | 60 (57.1) | 8 (13.1) | <0.001 |
| N of participants with history of COVID-19 based on N-antibodies (%) | 162 (43.2) | 86 (41.1) | 47 (44.8) | 29 (47.5) | 0.628 |
| Diabetes (%) | 133 (38.9) | 80 (40.4) | 28 (32.2) | 25 (43.9) | 0.297 |
| Cardiovascular diseases (%) | 226 (66.1) | 141 (71.2) | 32 (36.8) | 53 (93.0) | <0.001 |
| High systolic blood pressure (%) | 246 (71.9) | 145 (73.2) | 54 (62.1) | 47 (82.5) | 0.024 |
| Chronic respiratory diseases (%) | 56 (16.4) | 39 (19.7) | 8 (9.2) | 9 (16.1) | 0.088 |
| Hematooncological disease (%) | 10 (2.9) | 7 (3.5) | 3 (3.5) | 0 (0) | 0.448 ++ |
| Other oncological disease (%) | 31 (9.1) | 17 (8.6) | 7 (8.1) | 7 (12.5) | 0.618 |
| Autoimmune diseases (%) | 20 (5.9) | 14 (7.1) | 6 (6.9) | 0 (0) | 0.124 |
| Obesity (BMI > 30) (%) | 48 (14.1) | 28 (14.1) | 17 (19.5) | 3 (5.4) | 0.059 |
| Vaccine | Total | ||||
|---|---|---|---|---|---|
| Parameter | Result—n (%) | Spikevax (Moderna) | Comirnaty (Pfizer) | Vaxzevria (AstraZeneca) | |
| Anti-S IgG | Negative | 4 (1.9) | 5 (4.8) | 6 (9.8) | 15 (4.0) |
| Borderline | 2 (1.0) | 1 (1.0) | 0 | 3 (0.8) | |
| Positive | 203 (97.1) | 99 (94.2) | 55 (90.2) | 357 (95.2) | |
| Total | 209 (100) | 105 (100) | 61 (100) | 375 (100) | |
| p-value * | 0.056 | ||||
| VNT | Negative | 3 (1.4) | 5 (4.8) | 10 (16.4) | 18 (4.8) |
| Borderline | 3 (1.4) | 4 (3.9) | 2 (3.3) | 9 (2.4) | |
| Positive | 203 (97.2) | 95 (91.3) | 49 (80.3) | 347 (92.8) | |
| Total | 209 (100) | 104 (100) | 61 (100) | 374 (100) | |
| p-value * | <0.001 | ||||
| IGRA | Negative | 8 (6.7) | 1 (1.2) | 5 (10.0) | 14 (5.5) |
| Borderline | 7 (5.8) | 3 (3.6) | 4 (8.0) | 14 (5.5) | |
| Positive | 105 (87.5) | 80 (95.2) | 41 (82.0) | 226 (89.0) | |
| Total | 120 (100) | 84 (100) | 50 (100) | 254 (100) | |
| p-value * | 0.103 | ||||
| Median (IQR) | ||||
|---|---|---|---|---|
| Group | n | VNT Delta (Titer) | VNT Omicron (Titer) | p-Value * |
| 1: No COVID-19 record in personal history/no anti-N IgG | 10 | 80 (20–80) | 20 (10–40) | 0.016 |
| 2: COVID-19 record in personal history/no anti-N IgG | 10 | 320 (320–640) | 160 (80–320) | 0.059 |
| 3: No COVID-19 record in personal history/anti-N IgG positive | 10 | 1280 (640–2560) | 320 (160–640) | 0.008 |
| 4: COVID-19 record in personal history/anti-N IgG positive | 10 | 640 (320–1280) | 160 (80–320) | 0.002 |
| Total | 40 | 320 (120–1280) | 160 (40–320) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínek, J.; Tomášková, H.; Janošek, J.; Zelená, H.; Kloudová, A.; Mrázek, J.; Ježo, E.; Král, V.; Pohořská, J.; Šturcová, H.; et al. Immune Response 5–7 Months after Vaccination against SARS-CoV-2 in Elderly Nursing Home Residents in the Czech Republic: Comparison of Three Vaccines. Viruses 2022, 14, 1086. https://0-doi-org.brum.beds.ac.uk/10.3390/v14051086
Martínek J, Tomášková H, Janošek J, Zelená H, Kloudová A, Mrázek J, Ježo E, Král V, Pohořská J, Šturcová H, et al. Immune Response 5–7 Months after Vaccination against SARS-CoV-2 in Elderly Nursing Home Residents in the Czech Republic: Comparison of Three Vaccines. Viruses. 2022; 14(5):1086. https://0-doi-org.brum.beds.ac.uk/10.3390/v14051086
Chicago/Turabian StyleMartínek, Jan, Hana Tomášková, Jaroslav Janošek, Hana Zelená, Alena Kloudová, Jakub Mrázek, Eduard Ježo, Vlastimil Král, Jitka Pohořská, Hana Šturcová, and et al. 2022. "Immune Response 5–7 Months after Vaccination against SARS-CoV-2 in Elderly Nursing Home Residents in the Czech Republic: Comparison of Three Vaccines" Viruses 14, no. 5: 1086. https://0-doi-org.brum.beds.ac.uk/10.3390/v14051086