
Post-COVID-19 Impairment of the Senses of Smell, Taste, Hearing, and Balance

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Smell Test
2.3. Taste Test
2.4. Pure Tone Audiometry (PTA) and Speech Audiometry
2.5. Video Head Impulse Test (vHIT)
2.6. Subjective Visual Vertical (SVV) Test and Vestibular Evoked Myogenic Potentials (VEMPs)
2.7. Questionnaires
2.8. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Presence and Duration of Sensory Dysfunction after COVID-19
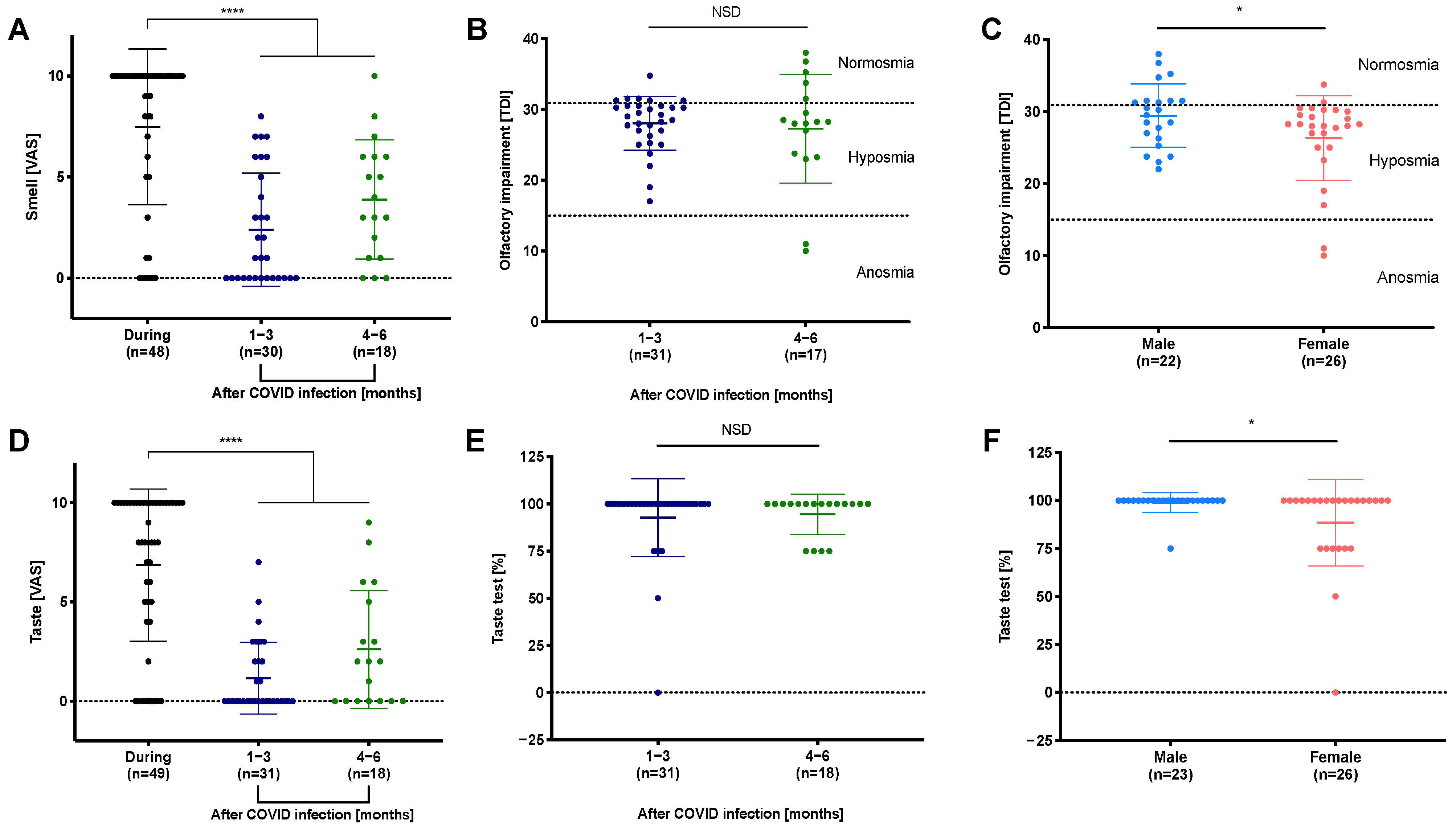
3.3. Reduced Perception of Smell and Taste during and after COVID-19
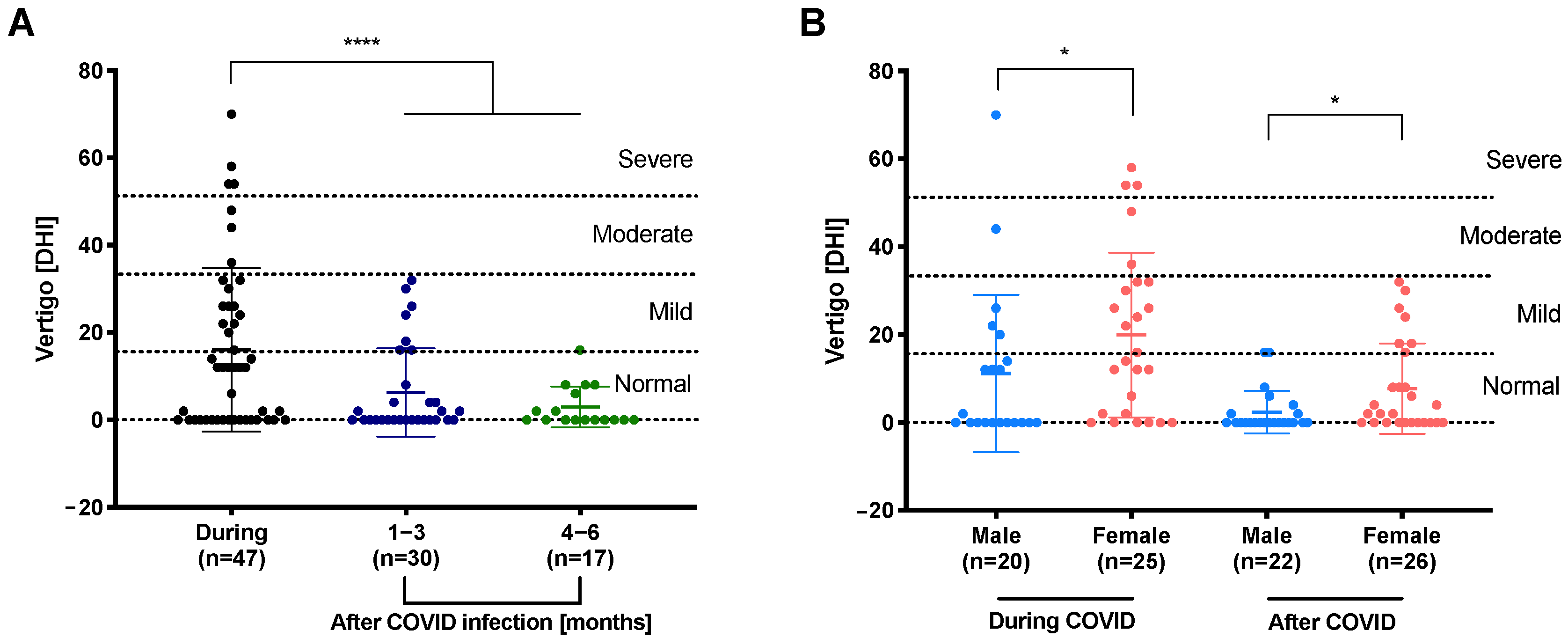
3.4. Decreased Dizziness during First Months of Follow-Up
3.5. Vestibular and Auditory Functions Rarely Affected after COVID-19
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Kim, G.U.; Kim, M.J.; Ra, S.H.; Lee, J.; Bae, S.; Jung, J.; Kim, S.H. Clinical characteristics of asymptomatic and symptomatic patients with mild COVID-19. Clin. Microbiol. Infect. 2020, 26, 948.e1–948.e3. [Google Scholar] [CrossRef]
- Iadecola, C.; Anrather, J.; Kamel, H. Effects of COVID-19 on the Nervous System. Cell 2020, 183, 16–27. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.U.; Hanif, M.; Ali, M.J.; Haider, M.A.; Kherani, D.; Memon, G.M.; Karim, A.H.; Sattar, A. Neurological Manifestations of COVID-19 (SARS-CoV-2): A Review. Front. Neurol. 2020, 11, 518. [Google Scholar] [CrossRef]
- Simon, O.J.; Timmermann, L. COVID-19: A neurological point-of-view. Dtsch. Med. Wochenschr. 2020, 145, 1074–1079. [Google Scholar] [CrossRef]
- Saniasiaya, J.; Kulasegarah, J. Dizziness and COVID-19. Ear Nose Throat J. 2021, 100, 29–30. [Google Scholar] [CrossRef]
- Adour, K.K.; Bell, D.N.; Hilsinger, R.L. Herpes simplex virus in idiopathic facial paralysis (Bell palsy). JAMA 1975, 233, 527–530. [Google Scholar] [CrossRef]
- Wu, Y.; Xu, X.; Chen, Z.; Duan, J.; Hashimoto, K.; Yang, L.; Liu, C.; Yang, C. Nervous system involvement after infection with COVID-19 and other coronaviruses. Brain Behav. Immun. 2020, 87, 18–22. [Google Scholar] [CrossRef]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ sticks’: Olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Hoth, S. The Freiburg speech intelligibility test: A pillar of speech audiometry in German-speaking countries. HNO 2016, 64, 540. [Google Scholar] [CrossRef] [PubMed]
- MacDougall, H.G.; Weber, K.P.; McGarvie, L.A.; Halmagyi, G.M.; Curthoys, I.S. The video head impulse test: Diagnostic accuracy in peripheral vestibulopathy. Neurology 2009, 73, 1134–1141. [Google Scholar] [CrossRef] [Green Version]
- Böhmer, A.; Mast, F. Assessing otolith function by the subjective visual vertical. Ann. N. Y. Acad. Sci. 1999, 871, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Birk, R.; Dietz, M.; Sommer, J.U.; Stuck, B.A.; Hörmann, K.; Rotter, N.; Maurer, J.T.; Kramer, B.; Hülse, R.; Schell, A. Nightly Hypoxia Does Not Seem to Lead to Otolith Dysfunction in Patients with Obstructive Sleep Apnea. Ear Nose Throat J. 2020, 100, 667–672. [Google Scholar] [CrossRef]
- Jacobson, G.P.; Newman, C.W. The development of the dizziness handicap inventory. Arch. Otolaryngol. Head Neck Surg. 1990, 116, 424–427. [Google Scholar] [CrossRef]
- Moein, S.T.; Hashemian, S.M.; Tabarsi, P.; Doty, R.L. Prevalence and reversibility of smell dysfunction measured psychophysically in a cohort of COVID-19 patients. Int. Forum Allergy Rhinol. 2020, 10, 1127–1135. [Google Scholar] [CrossRef]
- Niklassen, A.S.; Draf, J.; Huart, C.; Hintschich, C.; Bocksberger, S.; Trecca, E.M.C.; Klimek, L.; Le Bon, S.D.; Altundag, A.; Hummel, T. COVID-19: Recovery from Chemosensory Dysfunction. A Multicentre study on Smell and Taste. Laryngoscope 2021, 131, 109–1100. [Google Scholar] [CrossRef]
- Konstantinidis, I.; Delides, A.; Tsakiropoulou, E.; Maragoudakis, P.; Sapounas, S.; Tsiodras, S. Short-Term Follow-Up of Self-Isolated COVID-19 Patients with Smell and Taste Dysfunction in Greece: Two Phenotypes of Recovery. ORL J. Otorhinolaryngol. Relat. Spec. 2020, 82, 295–303. [Google Scholar] [CrossRef]
- Printza, A.; Katotomichelakis, M.; Valsamidis, K.; Metallidis, S.; Panagopoulos, P.; Panopoulou, M.; Petrakis, V.; Constantinidis, J. Smell and Taste Loss Recovery Time in COVID-19 Patients and Disease Severity. J. Clin. Med. 2021, 10, 966. [Google Scholar] [CrossRef]
- Speth, M.M.; Singer-Cornelius, T.; Oberle, M.; Gengler, I.; Brockmeier, S.J.; Sedaghat, A.R. Time scale for resolution of olfactory dysfunction in COVID-19. Rhinology 2020, 58, 404–405. [Google Scholar] [CrossRef] [PubMed]
- Singer-Cornelius, T.; Cornelius, J.; Oberle, M.; Metternich, F.U.; Brockmeier, S.J. Objective gustatory and olfactory dysfunction in COVID-19 patients: A prospective cross-sectional study. Eur. Arch. Otorhinolaryngol. 2021, 278, 3325–3332. [Google Scholar] [CrossRef] [PubMed]
- Bryche, B.; St Albin, A.; Murri, S.; Lacote, S.; Pulido, C.; Ar Gouilh, M.; Lesellier, S.; Servat, A.; Wasniewski, M.; Picard-Meyer, E.; et al. Massive transient damage of the olfactory epithelium associated with infection of sustentacular cells by SARS-CoV-2 in golden Syrian hamsters. Brain Behav. Immun. 2020, 89, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Beidler, L.M.; Smallman, R.L. Renewal of cells within taste buds. J. Cell Biol. 1965, 27, 263–272. [Google Scholar] [CrossRef]
- Graziadei, P.P.; Levine, R.R.; Monti Graziadei, G.A. Plasticity of connections of the olfactory sensory neuron: Regeneration into the forebrain following bulbectomy in the neonatal mouse. Neuroscience 1979, 4, 713–727. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hahner, A.; Hummel, T. Updated Sniffin’ Sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Otorhinolaryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [Green Version]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. EClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Martin-Guerrero, J.D.; Pellicer-Valero, O.J.; Navarro-Pardo, E.; Gomez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalon, J.A.; Cigaran-Mendez, M.; Hernandez-Barrera, V.; Arendt-Nielsen, L. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J. Clin. Med. 2022, 11, 413. [Google Scholar] [CrossRef]
- Ortona, E.; Buonsenso, D.; Carfi, A.; Malorni, W.; Long Covid Kids study, g. Long COVID: An estrogen-associated autoimmune disease? Cell Death Discov. 2021, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 57. [Google Scholar] [CrossRef] [PubMed]
- Hannum, M.E.; Ramirez, V.A.; Lipson, S.J.; Herriman, R.D.; Toskala, A.K.; Lin, C.; Joseph, P.V.; Reed, D.R. Objective Sensory Testing Methods Reveal a Higher Prevalence of Olfactory Loss in COVID-19-Positive Patients Compared to Subjective Methods: A Systematic Review and Meta-Analysis. Chem. Senses 2020, 45, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Pierron, D.; Pereda-Loth, V.; Mantel, M.; Moranges, M.; Bignon, E.; Alva, O.; Kabous, J.; Heiske, M.; Pacalon, J.; David, R.; et al. Smell and taste changes are early indicators of the COVID-19 pandemic and political decision effectiveness. Nat. Commun. 2020, 11, 5152. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, A.S.; Joshi, S.V.; Naik, S.; Sangle, S.; Abraham, N.M. Quantitative assessment of olfactory dysfunction accurately detects asymptomatic COVID-19 carriers. EClinicalMedicine 2020, 28, 100575. [Google Scholar] [CrossRef] [PubMed]
- Hülse, R.; Biesdorf, A.; Hörmann, K.; Stuck, B.; Erhart, M.; Hülse, M.; Wenzel, A. Peripheral Vestibular Disorders: An Epidemiologic Survey in 70 Million Individuals. Otol. Neurotol. 2019, 40, 88–95. [Google Scholar] [CrossRef]
- Neuhauser, H.; Von Brevern, M.; Radtke, A.; Lezius, F.; Feldmann, M.; Ziese, T.; Lempert, T. Epidemiology of vestibular vertigo A neurotologic survey of the general population. Neurology 2005, 65, 898–904. [Google Scholar] [CrossRef]
- Bisdorff, A.; Bosser, G.; Gueguen, R.; Perrin, P. The epidemiology of vertigo, dizziness, and unsteadiness and its links to co-morbidities. Front. Neurol. 2013, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Navari, E.; Cerchiai, N.; Casani, A.P. Assessment of vestibulo-ocular reflex gain and catch-up saccades during vestibular rehabilitation. Otol. Neurotol. 2018, 39, e1111–e1117. [Google Scholar] [CrossRef]
- Chern, A.; Famuyide, A.O.; Moonis, G.; Lalwani, A.K. Bilateral Sudden Sensorineural Hearing Loss and Intralabyrinthine Hemorrhage in a Patient With COVID-19. Otol. Neurotol. 2021, 42, e10. [Google Scholar] [CrossRef]
- Koumpa, F.S.; Forde, C.T.; Manjaly, J.G. Sudden irreversible hearing loss post COVID-19. BMJ Case Rep. 2020, 13, e238419. [Google Scholar] [CrossRef] [PubMed]
- Malayala, S.V.; Raza, A. A case of COVID-19-induced vestibular neuritis. Cureus 2020, 12, e8918. [Google Scholar] [CrossRef] [PubMed]
- Jha, N.K.; Ojha, S.; Jha, S.K.; Dureja, H.; Singh, S.K.; Shukla, S.D.; Chellappan, D.K.; Gupta, G.; Bhardwaj, S.; Kumar, N.; et al. Evidence of Coronavirus (CoV) Pathogenesis and Emerging Pathogen SARS-CoV-2 in the Nervous System: A Review on Neurological Impairments and Manifestations. J. Mol. Neurosci. 2021, 71, 2192–2209. [Google Scholar] [CrossRef] [PubMed]
- Furman, J.M.; Jacob, R.G. A clinical taxonomy of dizziness and anxiety in the otoneurological setting. J. Anxiety Disord. 2001, 15, 9–26. [Google Scholar] [CrossRef]
- Elibol, E. Otolaryngological symptoms in COVID-19. Eur. Arch. Otorhinolaryngol. 2021, 278, 1233–1236. [Google Scholar] [CrossRef]
- Viola, P.; Ralli, M.; Pisani, D.; Malanga, D.; Sculco, D.; Messina, L.; Laria, C.; Aragona, T.; Leopardi, G.; Ursini, F.; et al. Tinnitus and equilibrium disorders in COVID-19 patients: Preliminary results. Eur. Arch. Otorhinolaryngol. 2021, 278, 3725–3730. [Google Scholar] [CrossRef]
- Jafari, Z.; Kolb, B.E.; Mohajerani, M.H. Hearing Loss, Tinnitus, and Dizziness in COVID-19: A Systematic Review and Meta-Analysis. Can. J. Neurol. Sci. 2021, 49, 184–195. [Google Scholar] [CrossRef]
- Beukes, E.W.; Baguley, D.M.; Jacquemin, L.; Lourenco, M.; Allen, P.M.; Onozuka, J.; Stockdale, D.; Kaldo, V.; Andersson, G.; Manchaiah, V. Changes in Tinnitus Experiences During the COVID-19 Pandemic. Front. Public Health 2020, 8, 592878. [Google Scholar] [CrossRef]
- Freni, F.; Meduri, A.; Gazia, F.; Nicastro, V.; Galletti, C.; Aragona, P.; Galletti, C.; Galletti, B.; Galletti, F. Symptomatology in head and neck district in coronavirus disease (COVID-19): A possible neuroinvasive action of SARS-CoV-2. Am. J. Otolaryngol. 2020, 41, 102612. [Google Scholar] [CrossRef]
- Alves de Sousa, F.; Pinto Costa, R.; Xara, S.; Nobrega Pinto, A.; Almeida, E.S.C. SARS-CoV-2 and hearing: An audiometric analysis of COVID-19 hospitalized patients. J. Otol. 2021, 16, 158–164. [Google Scholar] [CrossRef]
- Sia, S.F.; Yan, L.M.; Chin, A.W.H.; Fung, K.; Choy, K.T.; Wong, A.Y.L.; Kaewpreedee, P.; Perera, R.; Poon, L.L.M.; Nicholls, J.M.; et al. Pathogenesis and transmission of SARS-CoV-2 in golden hamsters. Nature 2020, 583, 834–838. [Google Scholar] [CrossRef] [PubMed]
- Delmas, B.; Laude, H. Assembly of coronavirus spike protein into trimers and its role in epitope expression. J. Virol 1990, 64, 5367–5375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsuyama, S.; Nagata, N.; Shirato, K.; Kawase, M.; Takeda, M.; Taguchi, F. Efficient activation of the severe acute respiratory syndrome coronavirus spike protein by the transmembrane protease TMPRSS2. J. Virol 2010, 84, 12658–12664. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, C.G.K.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhou, M.; Brand, J.; Huang, L. Inflammation and taste disorders: Mechanisms in taste buds. Ann. N. Y. Acad. Sci. 2009, 1170, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brunink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2020, 24, 168–175. [Google Scholar] [CrossRef]
- Benghanem, S.; Mazeraud, A.; Azabou, E.; Chhor, V.; Shinotsuka, C.R.; Claassen, J.; Rohaut, B.; Sharshar, T. Brainstem dysfunction in critically ill patients. Crit. Care 2020, 24, 5. [Google Scholar] [CrossRef] [Green Version]
- Nouchi, A.; Chastang, J.; Miyara, M.; Lejeune, J.; Soares, A.; Ibanez, G.; Saadoun, D.; Morelot-Panzini, C.; Similowski, T.; Amoura, Z.; et al. Prevalence of hyposmia and hypogeusia in 390 COVID-19 hospitalized patients and outpatients: A cross-sectional study. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 691–697. [Google Scholar] [CrossRef]
- Brandal, L.T.; MacDonald, E.; Veneti, L.; Ravlo, T.; Lange, H.; Naseer, U.; Feruglio, S.; Bragstad, K.; Hungnes, O.; Odeskaug, L.E.; et al. Outbreak caused by the SARS-CoV-2 Omicron variant in Norway, November to December 2021. Euro Surveill. 2021, 26, 2101147. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: Runny nose, headache, and fatigue are commonest symptoms of omicron, early data show. BMJ 2021, 375, n3103. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | N (%) |
|---|---|
| Age | |
| 20–40 years | 22 (44) |
| 41–76 years | 28 (56) |
| Mean ± SD | 45 ± 15.44 |
| Gender | |
| Male | 23 (46) |
| Female | 27 (54) |
| Location | |
| Outpatient | 44 (88) |
| Inpatient | 3 (6) |
| Intensive care | 2 (4) |
| No data | 1 (2) |
| Duration of disease | |
| 1–7 days | 4 (8) |
| 8–14 days | 21 (42) |
| 15–30 days | 17 (34) |
| 30–60 days | 6 (12) |
| No data | 2 (4) |
| Mean ± SD | 18.54 ± 11.01 |
| Follow up after COVID-19 | |
| 1–3 months | 32 (64) |
| 4–6 months | 18 (36) |
| Mean (days) ± SD | 69.12 ± 41.61 |
| Smoker | |
| Yes | 1 (2) |
| No | 49 (98) |
| Alcohol consumption | |
| Yes | 17 (34) |
| No | 32 (64) |
| No data | 1 (2) |
| Medical history | |
| Hypertension | 10 (20) |
| Atrial Fibrillation | 2 (4) |
| Depression | 3 (6) |
| Asthma | 4 (8) |
| Thyroid dysfunction | 8 (16) |
| Medication | |
| Hypertensive medication | 11 |
| Antilipemic medication | 4 |
| Antidepressant medication | 5 |
| Asthma medication | 3 |
| Analgesics | 3 |
| Others | 21 |
| Olfactory N (%) | Gustatory N (%) | Hearing N (%) | Vestibular N (%) | |
|---|---|---|---|---|
| Presence of symptoms | ||||
| None Before COVID-19 | 8 (16) 3 (6) | 8 (16) 0 (0) | 34 (68) 8 (16) | 23 (46) 3 (6) |
| COVID19-associated symptoms: | ||||
| Only during COVID-19 | 15 (30) | 21 (42) | 3 (6) | 15 (30) |
| During and after | 21 (42) | 19 (38) | 1 (2) | 5 (10) |
| Only after | 2 (4) | 1 (2) | 0 (0) | 4 (8) |
| No data | 1 (2) | 1 (2) | 4 (8) | 0 (0) |
| Total | 50 (100) | 50 (100) | 50 (100) | 50 (100) |
| Initial begin of COVID-19 associated symptoms | ||||
| With onset of COVID-19 | 9 (18) | 10 (20) | 1 (2) | 8 (16) |
| 1–7 days after onset | 20 (40) | 24 (48) | 4 (2) | 13 (26) |
| 8–14 days after onset | 5 (10) | 4 (8) | 0 (0) | 2 (4) |
| 15–21 days after onset | 0 (0) | 0 (0) | 0 (0) | 1 (4) |
| 31 days after onset | 1 (2) | 0 (0) | ||
| No data | 15 (30) | 12 (24) | 45 (90) | 26 (52) |
| Total | 50 (100) | 50 (100) | 50 (100) | 50 (100) |
| Mean ± SD | 4.86 ± 5.68 | 3.74 ± 3.29 | 3.2 ± 3.49 | 2.96 ± 4.59 |
| Duration of disease | ||||
| 1–7 days | 9 (18) | 11 (22) | 1 (2) | 14 (28) |
| 8–14 days | 7 (14) | 10 (20) | 1 (2) | 2 (4) |
| 15–21 days | 4 (8) | 6 (12) | 1 (2) | 1 (5) |
| 22–120 days | 5 (12) | 7 (14) | 0 (0) | 4 (8) |
| No data | 25 (50) | 16 (32) | 47 (94) | 29 (58) |
| Total | 50 (100) | 50 (100) | 50 (100) | 50 (100) |
| Mean ± SD | 19.92 ± 27.37 | 16.53 ± 20.4 | 11.33 ± 9.07 | 11.67 ± 14.73 |
| Olfactory Test | Gustatory Test | ||
| Sniffing sticks | Taste test | ||
| Threshold | 3.03 ± 2.73 | Normal taste (100%) | 40 (80) |
| Discrimination | 12.24 ± 2.38 | Hypogeusia (25–75%) | 8 (16) |
| Identification | 12.63 ± 2.57 | Ageusia (0%) | 1 (2) |
| No data | 1 (2) | ||
| TDI score | 27.78 ± 5.37 | Total | 50 (100) |
| Normosmia (≥ 31 pts) | 11 (22) | Retronasal irritation test | |
| Hyposmia (15–31 pts) | 36 (72) | Perceived and identified | 39 (78) |
| Anosmia (≤15 pts) | 2 (4) | Perceived | 8 (16) |
| No data | 1 (2) | No perception | 3 (6) |
| Total | 50 (100) | Total | 50 (100) |
| Audiometric Test | Vestibular Test | ||
| PTA—bone conduction | Video head impulse test | ||
| Normal hearing (0–20 dB) | 36 (72) | (vHIT) | |
| Mild (20–40 dB) | 6 (12) | Normal | 48 (96) |
| Medium (40–60 dB) | 0 (0) | Abnormal | 1 (2) |
| Severe (>60 dB) | 0 (0) | No data | 1 (2) |
| No data/Pre-existing | 8 (16) | Total | 50 (100) |
| Total | 50 (100) | Mean ± SD | 1.03 ± 0.15 |
| Mean ± SD | 11.3 ± 6.7 | ||
| PTA—air conduction | |||
| Normal hearing (0–20 dB) | 27 (54) | ||
| Mild (20–40 dB) | 15 (30) | ||
| Medium (40–60 dB) | 0 (0) | ||
| Severe (>60 dB) | 0 (0) | ||
| No data/Pre-existing | 8 (16) | ||
| Total | 50 (100) | ||
| Mean ± SD | 18.2 ± 8.3 | ||
| Freiburg speech audiogram | |||
| Numbers at 50% | −9.56 ± 13.22 | ||
| No data | 8 (16) | ||
| Monosyllables at 65 dB | 93.91 ± 13.12 | ||
| No data | 10 (20) | ||
| Total | 50 (100) | ||
| Tympanogram | |||
| Normal | 46 (96) | ||
| Abnormal | 3 (6) | ||
| No data | 1 (2) | ||
| Total | 50 (100) | ||
| Stapedius reflex test | |||
| Normal | 22 (44) | ||
| Abnormal | 14 (28) | ||
| No data | 14 (28) | ||
| Total | 50 (100) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ludwig, S.; Schell, A.; Berkemann, M.; Jungbauer, F.; Zaubitzer, L.; Huber, L.; Warken, C.; Held, V.; Kusnik, A.; Teufel, A.; et al. Post-COVID-19 Impairment of the Senses of Smell, Taste, Hearing, and Balance. Viruses 2022, 14, 849. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050849
Ludwig S, Schell A, Berkemann M, Jungbauer F, Zaubitzer L, Huber L, Warken C, Held V, Kusnik A, Teufel A, et al. Post-COVID-19 Impairment of the Senses of Smell, Taste, Hearing, and Balance. Viruses. 2022; 14(5):849. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050849
Chicago/Turabian StyleLudwig, Sonja, Angela Schell, Michelle Berkemann, Frederic Jungbauer, Lena Zaubitzer, Lena Huber, Christian Warken, Valentin Held, Alexander Kusnik, Andreas Teufel, and et al. 2022. "Post-COVID-19 Impairment of the Senses of Smell, Taste, Hearing, and Balance" Viruses 14, no. 5: 849. https://0-doi-org.brum.beds.ac.uk/10.3390/v14050849