
Characterizing Risk Factors for Hospitalization and Clinical Characteristics in a Cohort of COVID-19 Patients Enrolled in the GENCOV Study
 , , , and add
Show full author list
, , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participant Recruitment
2.2. Patient Data Collection by Intake Surveys
2.3. Collection of Viral Lineage Data
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics and Associations with Hospitalization
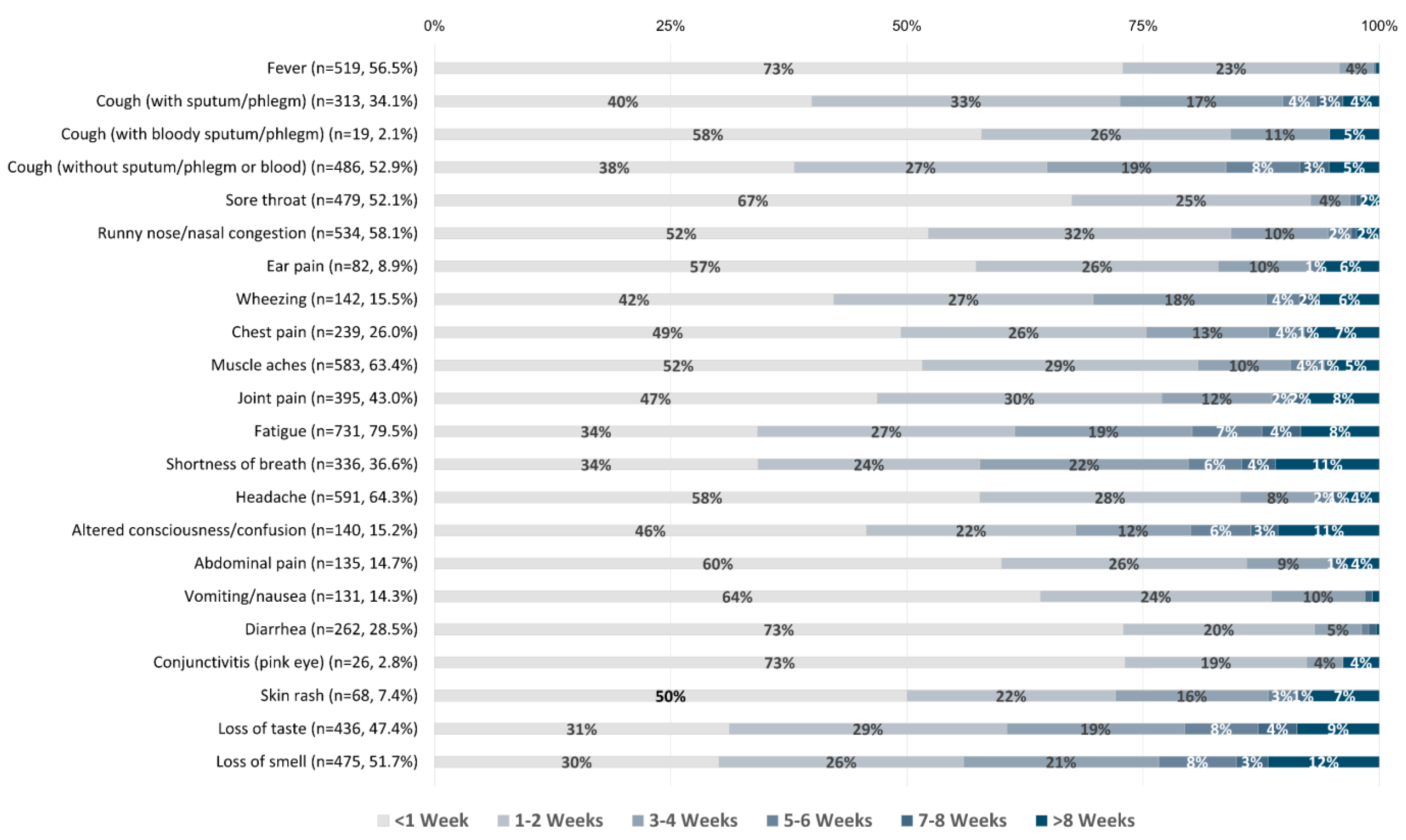
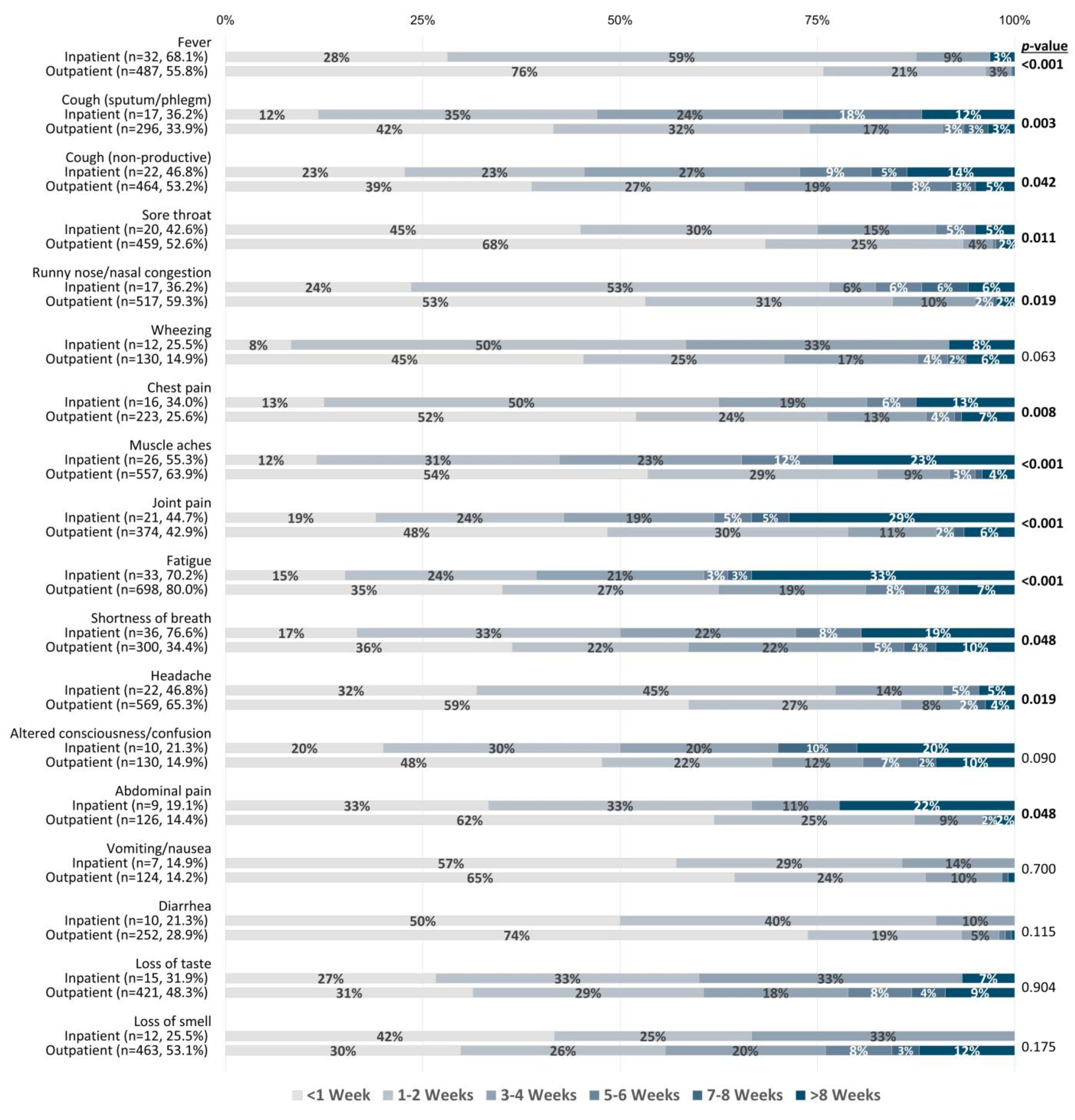
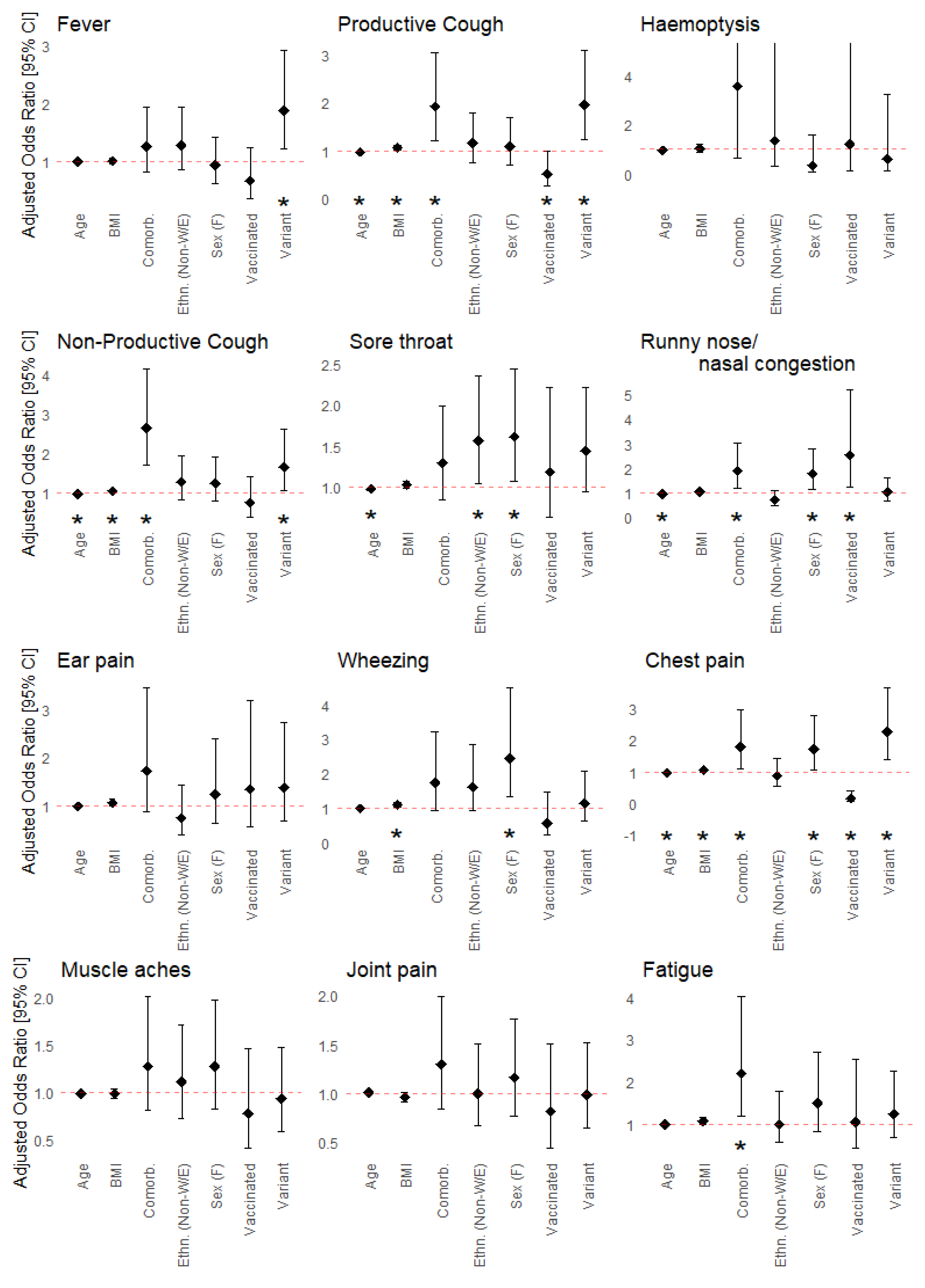
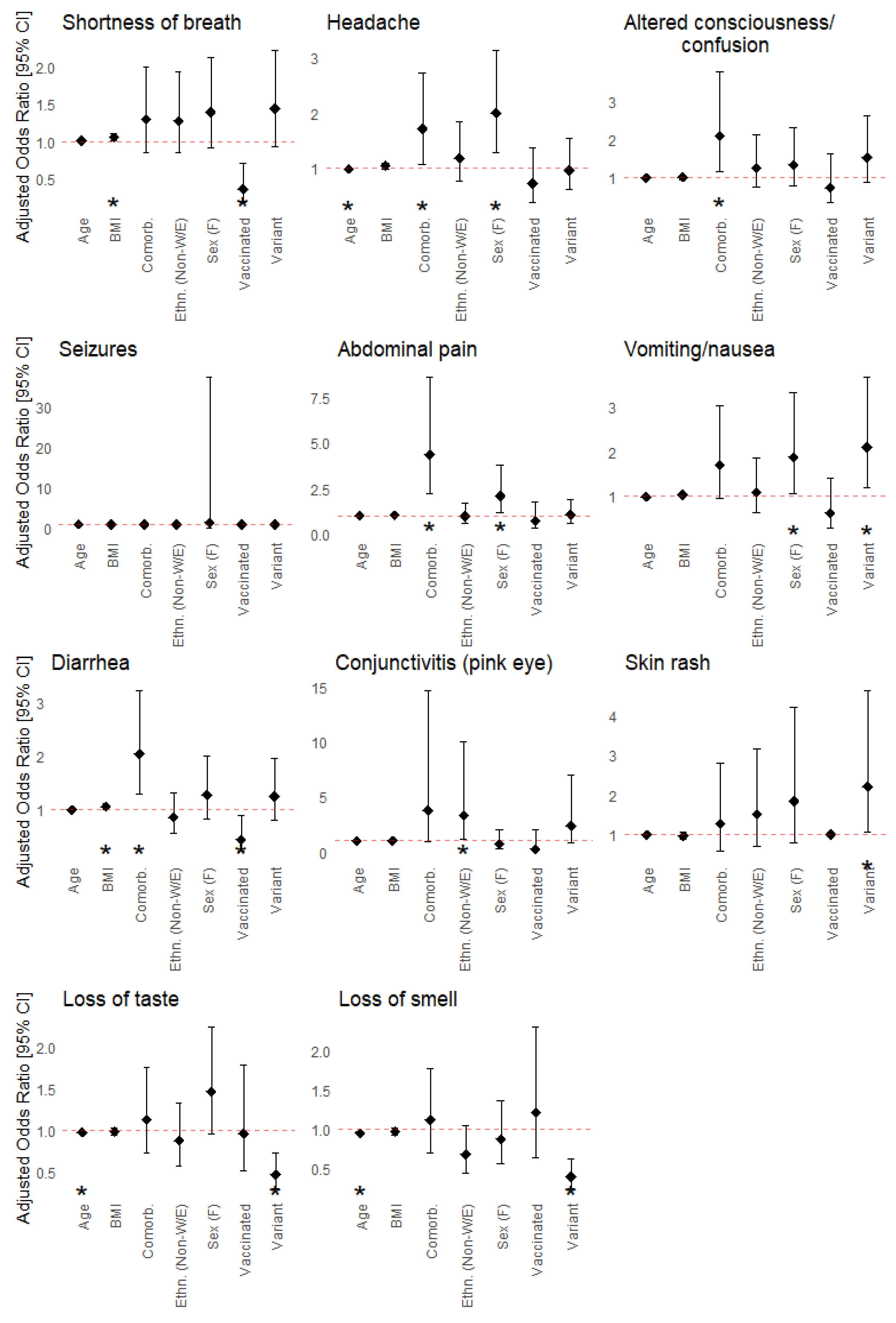
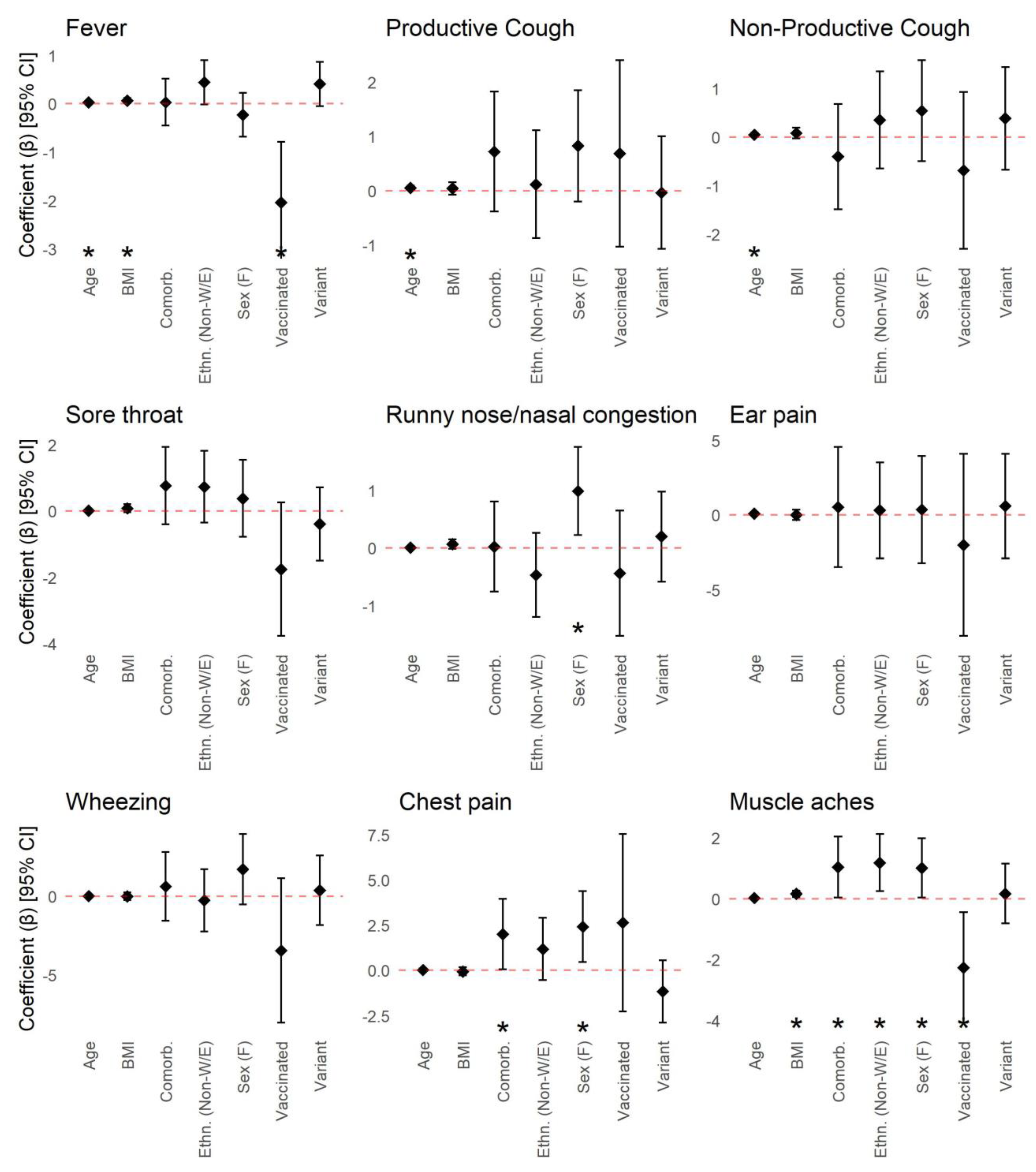
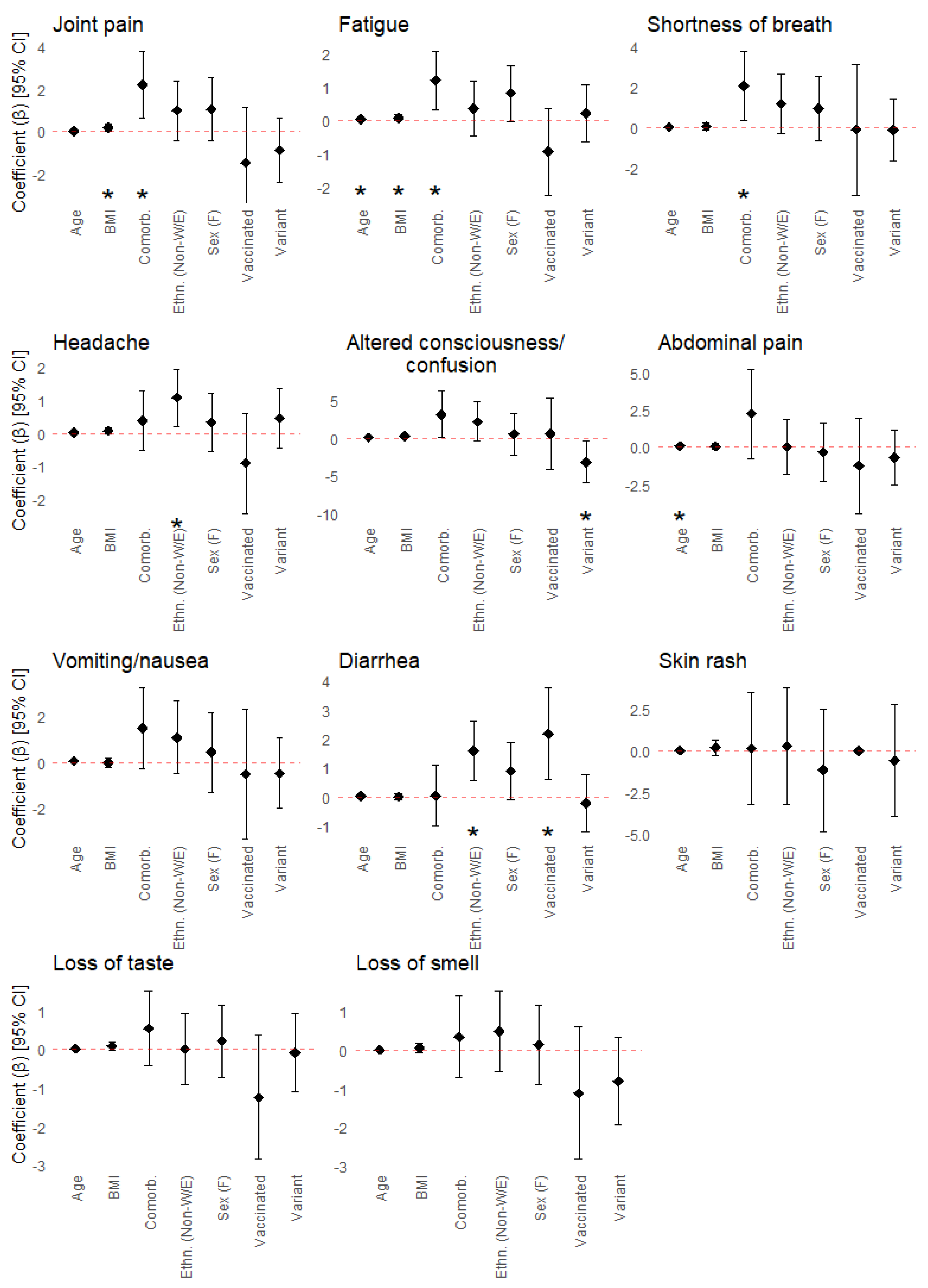
3.2. COVID-19 Symptom Prevalence, Duration, and Associations with Patient Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Condition Category/Subcategory | Specific Conditions Listed |
|---|---|
| Hypertension | Hypertension |
| Endocrine Conditions | Thyroid disease, hypothyroidism, polycystic ovary syndrome (PCOS), adrenal hemorrhage, hyperthyroidism, postpartum thyroiditis hypoglycemia, pituitary adenoma |
| Type 2 Diabetes | Type 2 diabetes |
| Type 1 Diabetes | Type 1 diabetes |
| Endocrine Cancer | Thyroid cancer, papillary carcinoma |
| Endocrine Autoimmune Disorders | Autoimmune thyroiditis, Hashimoto’s disease, Graves disease |
| Gestational Diabetes | Gestational diabetes |
| Maturity-Onset Diabetes of the Young | Maturity-onset diabetes of the young |
| Pre-Diabetes | Pre-diabetes |
| Cardiovascular Conditions | Heart murmur, cardiovascular heart disease (atherosclerosis, peripheral vascular disease, stroke), right bundle branch block, heart defect (partition heart defect, patent ductus arteriosus ligation), atrial fibrillation, valvular disease (mitral valve prolapse, MV or aortic regurgitation), patent foramen ovale, tachycardia (SVT, VT), hypertrophy, arrhythmia (sick sinus syndrome, pacemaker Tx, AVNRT inappropriate sinus tachycardia, Mobitz type I AV block), pericarditis, heart failure, myocardial infarction/ischemia, postural tachycardia syndrome, pericarditis (idiopathic, undetermined cause), small aortic dilation, hypotension (orthostatic, unspecified), congenital heart murmur |
| Other Conditions | Alopecia (type not specified), pituitary cyst, pseudocholinesterase deficiency, lymphedema, lichen simplex chronicus |
| Sleep Disorders | Sleep apnea, sleep paralysis, insomnia, parasomnia restless leg syndrome |
| Muscle/Joint Conditions | Gout, arthritis (unspecified, osteoarthritis), joint pain/tendonitis, carpal tunnel, tendinosis, chondromalacia, history of hip replacements, knee replacement, degenerative disc disease/nerve damage, herniated disc |
| Gynecological/Urological Conditions | Endometriosis, ovarian cysts, hysterectomy, endometrioma cyst, adenomyosis, overactive bladder, fertility issues, atypical cells in cervix, uterine fibroid, dysmenorrhea, vesicoureteral reflux, benign prostatic hyperplasia |
| Dermatological Conditions | Eczema, hidradenitis suppurativa, keloids, plantar fasciitis, dermatitis, rosacea |
| Bone Conditions | Osteopenia, osteoporosis, scoliosis, ORIF surgery, brachymetatarsia, osteophytes, congenital hip dysplasia, congenital fused vertebrae |
| Ophthalmologic Conditions | Glaucoma, detached retina, macular degeneration, chorioretinopathy, posterior vitreous detachment, blindness, iritis, styes, blepharospasm |
| Cancer | Cancer (unspecified), uterine, breast, prostate, ductal carcinoma, skin, breast, bladder, testicular, adenocarcinoma |
| Lipid Conditions | Lipid disorders, dyslipidemia, hypercholesterolemia, elevated triglycerides |
| Hepatic Conditions | Fatty liver, cirrhosis, non-alcoholic fatty liver disease, fibrosis, liver hemangioma, hyperbilirubinemia, hepatomegaly, non-viral hepatitis |
| Viral Hepatitis | Hepatitis A, hepatitis B, hepatitis C |
| Blood Conditions | Factor v leiden and protein c deficiency, thrombophilia, Raynaud’s syndrome, popliteal aneurysm, abdominal aneurysm |
| Iron Disorders | Hemochromatosis, iron deficiency/anemia |
| Blood Cancer | Non-Hodgkin’s lymphoma, polycythemia rubra vera |
| Blood Autoimmune Disorders | Immune thrombocytopenia |
| Gastrointestinal Conditions | Irritable bowel syndrome (IBS), gastroesophageal reflux disease (GERD), chronic gastritis, acid reflux/heartburn, diverticulitis, hiatal hernia, bowel resection, Schatzki’s ring, esophageal dysmotility, eosinophilic esophagitis, Helicobacter pylori (H. pylori) infection, dysmotility (achalasia), peptic ulcer disease, familial adenomatous polyposis, lactose intolerance, umbilical hernia, gall stones, cholecystectomy |
| Gastrointestinal Autoimmune Disorders | Colitis, inflammatory bowel disease (Crohn’s and ulcerative colitis), celiac disease |
| Gastrointestinal Cancer | Esophageal cancer, appendix cancer, colon cancer, rectal cancer, gastric cancer |
| Pulmonary Conditions | Asthma, bronchitis, pulmonary fibrosis, pneumonia, pneumothorax, COPD, pulmonary tuberculosis |
| Autoimmune Conditions | Vasculitis, dermatomyositis, lechen planus, rheumatoid arthritis, psoriatic arthritis, multiple sclerosis, psoriasis, alopecia areata, ankylosing spondylitis, hidradenitis suppurativa, Henoch–Schönlein purpura, cold urticaria (autoimmune), interstitial cystitis, lupus, Sjogren’s syndrome |
| Neurologic/Psychiatric Conditions | Childhood epilepsy, hydrocephalus, fibromyalgia, neuropathy, depression, anxiety, chronic fatigue syndrome, post-concussion syndrome, epilepsy, brain aneurysm, dementia/memory loss, PTSD, eating disorder, bipolar disorder, head trauma (from motor vehicle accident), concussion, ADHD, OCD, cerebral palsy, chronic headache (unspecified, migraines), sciatica, vertigo |
| Neurological Autoimmune Disorders | Multiple sclerosis |
| Renal Conditions | Kidney stones, proteinuria, Cacchi–Ricci disease (medullary sponge kidney), kidney dysplasia, UPJ obstruction, duplex kidney, megaureter, grade 4 reflux, pyelonephritis, kidney failure |
| Renal Cancer | Renal liposarcoma |
| Renal Autoimmune Disorders | Nephrotic syndrome (autoimmune), lupus nephritis |
| Non-SARS-CoV-2 Viral Infections | Herpes simplex virus, HIV, Epstein–Barr virus, HPV |
| Hereditary Genetic Conditions | Leber hereditary optic neuropathy, hemachromatosis, lamellar ichthyosis, Alpha-1 antitrypsin deficiency, PMS2 mutation (Lynch syndrome), familial tremor |
| Hereditary Blood Disorders | Von Willibrand disease, sickle cell anemia, hereditary hemorrhagic telangiectasia, thalassemia |
| Hereditary Lipid Disorders | Tay Sachs |
| n (%) | |
|---|---|
| Ethnicity | 966 |
| White/European | 532 (55.1) |
| Middle Eastern | 95 (9.8) |
| Asian—South | 75 (7.8) |
| Ashkenazi Jewish | 74 (7.7) |
| Latin American | 56 (5.8) |
| Asian—East | 55 (5.7) |
| Asian—Southeast | 40 (4.1) |
| Other | 37 (3.8) |
| Black—Caribbean | 18 (1.9) |
| Black—North American | 9 (<1.0) |
| Black—African | 8 (<1.0) |
| Indigenous | 5 (<1.0) |
| Did not specify | 26 (2.7) |
| Viral Variants | 966 |
| Wild-type | 277 (28.7) |
| Alpha | 201 (20.8) |
| Omicron | 69 (7.1) |
| Delta | 64 (6.6) |
| Gamma | 11 (1.1) |
| Zeta | 3 (<1.0) |
| Beta | 2 (<1.0) |
| Beta/Gamma (Undetermined) | 2 (<1.0) |
| Delta/Omicron (Undetermined) | 1 (<1.0) |
| Unknown | 336 (34.8) |
| n (%) | |
|---|---|
| Total Number of Vaccinated Participants | 244 |
| Median Time of Most Recent Vaccination Before Infection [IQR] | 85 days [24–172 days] |
| Received One Vaccine Dose Before Infection | 79 |
| Median Time of Most Recent Vaccination Before Infection [IQR] | 17 days [7–48.5 days] |
| Pfizer-BioNTech | 50 (63.3%) |
| Moderna | 11 (13.9%) |
| AstraZeneca | 16 (20.3%) |
| Janssen | 1 (1.3%) |
| Unknown | 1 (1.3%) |
| Received Two Vaccine Doses Before Infection | 110 |
| Median Time of Most Recent Vaccination Before Infection [IQR] | 169 days [104–184 days] |
| Pfizer-BioNTech/Pfizer-BioNTech | 58 (52.7%) |
| Pfizer-BioNTech/Moderna | 18 (16.4%) |
| Moderna/Pfizer | 1 (0.9%) |
| Moderna/Moderna | 19 (17.3%) |
| AstraZeneca/Pfizer | 4 (3.6%) |
| AstraZeneca/Moderna | 1 (0.9%) |
| AstraZeneca/AstraZeneca | 6 (5.5%) |
| Unknown | 3 (2.7%) |
| Received Three Vaccine Doses Before Infection | 55 |
| Median Time of Most Recent Vaccination Before Infection [IQR] | 56 days [24 –104 days] |
| Pfizer-BioNTech/Pfizer-BioNTech/Pfizer-BioNTech | 39 (70.9%) |
| Pfizer-BioNTech/Moderna/Pfizer-BioNTech | 3 (5.5%) |
| Pfizer-BioNTech/Pfizer-BioNTech/Moderna | 5 (9.1%) |
| Moderna/Moderna/Pfizer | 1 (1.8%) |
| Moderna/Moderna/Moderna | 4 (7.3%) |
| AstraZeneca/Moderna/Pfizer-BioNTech | 1 (1.8%) |
| AstraZeneca/Moderna/Moderna | 1 (1.8%) |
| Unknown | 1 (1.8%) |

References
- Macera, M.; De Angelis, G.; Sagnelli, C.; Coppola, N.; Vanvitelli COVID-19 Group. Clinical Presentation of COVID-19: Case Series and Review of the Literature. Int. J. Environ. Res. Public Health 2020, 17, 5062. [Google Scholar] [CrossRef] [PubMed]
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk Factors for Severe Disease and Death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Xu, S.; Yu, M.; Wang, K.; Tao, Y.; Zhou, Y.; Shi, J.; Zhou, M.; Wu, B.; Yang, Z.; et al. Risk Factors for Severity and Mortality in Adult COVID-19 Inpatients in Wuhan. J. Allergy Clin. Immunol. 2020, 146, 110–118. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK Patients in Hospital with COVID-19 Using the ISARIC WHO Clinical Characterisation Protocol: Prospective Observational Cohort Study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Ahmed, Z.; Younas, S. COVID-19 and Comorbidities: Deleterious Impact on Infected Patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef]
- Gou, Y.; Ping, K.; Lei, M.; Yu, C.; Tao, Y.; Hu, C.; Tao, Z.; Zou, Z.; Jiang, W.; Li, S.; et al. Initial Clinical Characteristics of 146 Patients with COVID-19 Reported in Guizhou Province, China: A Survival Analysis. J. Infect. Dev. Ctries. 2022, 16, 32–40. [Google Scholar] [CrossRef]
- Hu, J.; Wang, Y. The Clinical Characteristics and Risk Factors of Severe COVID-19. Gerontology 2021, 67, 255–266. [Google Scholar] [CrossRef]
- Gao, Y.; Ding, M.; Dong, X.; Zhang, J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.; Fu, W.; Li, W.; et al. Risk Factors for Severe and Critically Ill COVID-19 Patients: A Review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of Comorbidities and Its Effects in Patients Infected with SARS-CoV-2: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef]
- Fang, X.; Li, S.; Yu, H.; Wang, P.; Zhang, Y.; Chen, Z.; Li, Y.; Cheng, L.; Li, W.; Jia, H.; et al. Epidemiological, Comorbidity Factors with Severity and Prognosis of COVID-19: A Systematic Review and Meta-Analysis. Aging 2020, 12, 12493–12503. [Google Scholar] [CrossRef]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The Prevalence of Symptoms in 24,410 Adults Infected by the Novel Coronavirus (SARS-CoV-2; COVID-19): A Systematic Review and Meta-Analysis of 148 Studies from 9 Countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- Talukder, A.; Razu, S.R.; Alif, S.M.; Rahman, M.A.; Islam, S.M.S. Association Between Symptoms and Severity of Disease in Hospitalised Novel Coronavirus (COVID-19) Patients: A Systematic Review and Meta-Analysis. JMDH 2022, 15, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Zheng, B.; Daines, L.; Sheikh, A. Long-Term Sequelae of COVID-19: A Systematic Review and Meta-Analysis of One-Year Follow-Up Studies on Post-COVID Symptoms. Pathogens 2022, 11, 269. [Google Scholar] [CrossRef] [PubMed]
- Wu, D.C.; Jha, P.; Lam, T.; Brown, P.; Gelband, H.; Nagelkerke, N.; Birnboim, H.C.; Reid, A.; on behalf of the Action to Beat Coronavirus in Canada/Action pour Battre le Coronavirus (Ab-C) Study Group. Predictors of Self-Reported Symptoms and Testing for COVID-19 in Canada Using a Nationally Representative Survey. PLoS ONE 2020, 15, e0240778. [Google Scholar] [CrossRef]
- Taher, J.; Mighton, C.; Chowdhary, S.; Casalino, S.; Frangione, E.; Arnoldo, S.; Bearss, E.; Binnie, A.; Bombard, Y.; Borgundvaag, B.; et al. Implementation of Serological and Molecular Tools to Inform COVID-19 Patient Management: Protocol for the GENCOV Prospective Cohort Study. BMJ Open 2021, 11, e052842. [Google Scholar] [CrossRef]
- Brown, K.A.; Gubbay, J.; Hopkins, J.; Patel, S.; Buchan, S.A.; Daneman, N.; Goneau, L.W. S-Gene Target Failure as a Marker of Variant B.1.1.7 among SARS-CoV-2 Isolates in the Greater Toronto Area, December 2020 to March 2021. JAMA 2021, 325, 2115. [Google Scholar] [CrossRef]
- Public Health Ontario. Phylogenetic Analysis of SARS-CoV-2 in Ontario. Available online: https://nextstrain.publichealthontario.ca/ncov/ (accessed on 14 June 2023).
- Hadfield, J.; Megill, C.; Bell, S.M.; Huddleston, J.; Potter, B.; Callender, C.; Sagulenko, P.; Bedford, T.; Neher, R.A. Nextstrain: Real-Time Tracking of Pathogen Evolution. Bioinformatics 2018, 34, 4121–4123. [Google Scholar] [CrossRef]
- Li, J.; Huang, D.Q.; Zou, B.; Yang, H.; Hui, W.Z.; Rui, F.; Yee, N.T.S.; Liu, C.; Nerurkar, S.N.; Kai, J.C.Y.; et al. Epidemiology of COVID-19: A Systematic Review and Meta-analysis of Clinical Characteristics, Risk Factors, and Outcomes. J. Med. Virol. 2021, 93, 1449–1458. [Google Scholar] [CrossRef]
- Lhendup, K.; Tsheten, T.; Rinzin, T.; Wangdi, K. Risk Factors of Symptomatic COVID-19 in Samtse District, Bhutan. Front. Public Health 2022, 10, 857084. [Google Scholar] [CrossRef]
- Davies, N.G.; Klepac, P.; Liu, Y.; Prem, K.; Jit, M.; CMMID COVID-19 Working Group; Pearson, C.A.B.; Quilty, B.J.; Kucharski, A.J.; Gibbs, H.; et al. Age-Dependent Effects in the Transmission and Control of COVID-19 Epidemics. Nat. Med. 2020, 26, 1205–1211. [Google Scholar] [CrossRef]
- Cheng, W.A.; Turner, L.; Marentes Ruiz, C.J.; Tanaka, M.L.; Congrave-Wilson, Z.; Lee, Y.; Jumarang, J.; Perez, S.; Peralta, A.; Pannaraj, P.S. Clinical Manifestations of COVID-19 Differ by Age and Obesity Status. Influenza Resp. Viruses 2022, 16, 255–264. [Google Scholar] [CrossRef]
- McCarty, T.R.; Hathorn, K.E.; Redd, W.D.; Rodriguez, N.J.; Zhou, J.C.; Bazarbashi, A.N.; Njie, C.; Wong, D.; Trinh, Q.-D.; Shen, L.; et al. How Do Presenting Symptoms and Outcomes Differ by Race/Ethnicity Among Hospitalized Patients with Coronavirus Disease 2019 Infection? Experience in Massachusetts. Clin. Infect. Dis. 2021, 73, e4131–e4138. [Google Scholar] [CrossRef] [PubMed]
- Schulze, H.; Bayer, W. Changes in Symptoms Experienced by SARS-CoV-2-Infected Individuals—From the First Wave to the Omicron Variant. Front. Virol. 2022, 2, 880707. [Google Scholar] [CrossRef]
- Rotshild, V.; Hirsh-Raccah, B.; Miskin, I.; Muszkat, M.; Matok, I. Comparing the Clinical Efficacy of COVID-19 Vaccines: A Systematic Review and Network Meta-Analysis. Sci. Rep. 2021, 11, 22777. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Zhou, M.; Liu, Y.; Guo, T.; Ou, C.; Yang, L.; Li, Y.; Li, D.; Hu, X.; Shuai, L.; et al. Characteristics of Asymptomatic COVID-19 Infection and Progression: A Multicenter, Retrospective Study. Virulence 2020, 11, 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R.; et al. Ethnicity and Clinical Outcomes in COVID-19: A Systematic Review and Meta-Analysis. eClinicalMedicine 2020, 29–30, 100630. [Google Scholar] [CrossRef] [PubMed]
- Magesh, S.; John, D.; Li, W.T.; Li, Y.; Mattingly-app, A.; Jain, S.; Chang, E.Y.; Ongkeko, W.M. Disparities in COVID-19 Outcomes by Race, Ethnicity, and Socioeconomic Status: A Systematic Review and Meta-Analysis. JAMA Netw. Open 2021, 4, e2134147. [Google Scholar] [CrossRef]
- Twohig, K.A.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, M.A.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital Admission and Emergency Care Attendance Risk for SARS-CoV-2 Delta (B.1.617.2) Compared with Alpha (B.1.1.7) Variants of Concern: A Cohort Study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef]
- Lin, L.; Liu, Y.; Tang, X.; He, D. The Disease Severity and Clinical Outcomes of the SARS-CoV-2 Variants of Concern. Front. Public Health 2021, 9, 775224. [Google Scholar] [CrossRef]
- Buchan, S.A.; Chung, H.; Brown, K.A.; Austin, P.C.; Fell, D.B.; Gubbay, J.B.; Nasreen, S.; Schwartz, K.L.; Sundaram, M.E.; Tadrous, M.; et al. Estimated Effectiveness of COVID-19 Vaccines Against Omicron or Delta Symptomatic Infection and Severe Outcomes. JAMA Netw. Open 2022, 5, e2232760. [Google Scholar] [CrossRef]
- Moghadas, S.M.; Vilches, T.N.; Zhang, K.; Wells, C.R.; Shoukat, A.; Singer, B.H.; Meyers, L.A.; Neuzil, K.M.; Langley, J.M.; Fitzpatrick, M.C.; et al. The Impact of Vaccination on Coronavirus Disease 2019 (COVID-19) Outbreaks in the United States. Clin. Infect. Dis. 2021, 73, 2257–2264. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Vega, M.F.; Salinas-Escudero, G.; García-Peña, C.; Gutiérrez-Robledo, L.M.; Parra-Rodríguez, L. Early Estimation of the Risk Factors for Hospitalization and Mortality by COVID-19 in Mexico. PLoS ONE 2020, 15, e0238905. [Google Scholar] [CrossRef] [PubMed]
- Alwani, M.; Yassin, A.; Al-Zoubi, R.M.; Aboumarzouk, O.M.; Nettleship, J.; Kelly, D.; Al-Qudimat, A.R.; Shabsigh, R. Sex-based Differences in Severity and Mortality in COVID-19. Rev. Med. Virol. 2021, 31, e2223. [Google Scholar] [CrossRef]
- Danielsen, A.C.; Lee, K.M.; Boulicault, M.; Rushovich, T.; Gompers, A.; Tarrant, A.; Reiches, M.; Shattuck-Heidorn, H.; Miratrix, L.W.; Richardson, S.S. Sex Disparities in COVID-19 Outcomes in the United States: Quantifying and Contextualizing Variation. Soc. Sci. Med. 2022, 294, 114716. [Google Scholar] [CrossRef] [PubMed]
- Sharma, J.; Rajput, R.; Bhatia, M.; Arora, P.; Sood, V. Clinical Predictors of COVID-19 Severity and Mortality: A Perspective. Front. Cell. Infect. Microbiol. 2021, 11, 674277. [Google Scholar] [CrossRef]
- Zhabokritsky, A.; Daneman, N.; MacPhee, S.; Estrada-Codecido, J.; Santoro, A.; Kit Chan, A.; Wai-Hei Lam, P.; Simor, A.; Allen Leis, J.; Mubareka, S.; et al. Association between Initial Symptoms and Subsequent Hospitalization in Outpatients with COVID-19: A Cohort Study. Off. J. Assoc. Med. Microbiol. Infect. Dis. Can. 2021, 6, 259–268. [Google Scholar] [CrossRef]
- Purja, S.; Shin, H.; Lee, J.-Y.; Kim, E. Is Loss of Smell an Early Predictor of COVID-19 Severity: A Systematic Review and Meta-Analysis. Arch. Pharm. Res. 2021, 44, 725–740. [Google Scholar] [CrossRef]
- Patel, J.R.; Amick, B.C.; Vyas, K.S.; Bircan, E.; Boothe, D.; Nembhard, W.N. Racial Disparities in Symptomatology and Outcomes of COVID-19 among Adults of Arkansas. Prev. Med. Rep. 2022, 28, 101840. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and Risk Factors for Long COVID in Non-Hospitalized Adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and Predictors of Long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef]
- Office of the Premier. Ontario Moving to Phase Two of COVID-19 Vaccine Distribution Plan. Available online: https://news.ontario.ca/en/release/61009/ontario-moving-to-phase-two-of-covid-19-vaccine-distribution-plan (accessed on 8 February 2023).
- Lăzăroiu, G.; Mihăilă, R.; Braniște, L. The Language of COVID-19 Vaccine Hesitancy and Public Health Misinformation: Distrust, Unwillingness, and Uncertainty. Rev. Contemp. Philos. 2021, 20, 117. [Google Scholar] [CrossRef]
- Wells, R.; Vochozka, M.; Vojtech, S. Hesitancy towards Receiving a COVID-19 Vaccine: Concerns about Side Effects and Safety, Mistrust in Government and Health Authorities, and Perceived Susceptibility and Severity of the Virus. Rev. Contemp. Philos. 2021, 20, 163. [Google Scholar] [CrossRef]
- Lăzăroiu, G.; Mihăilă, R.; Braniște, L. The Language of Misinformation Literacy: COVID-19 Vaccine Hesitancy Attitudes, Behaviors, and Perceptions. Linguist. Philos. Investig. 2021, 20, 85. [Google Scholar] [CrossRef]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]






| No. of Observations (%) | |||||||
|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | ||||||
| Characteristics | Total (n = 966) | Inpatient (n = 54) | Outpatient (n = 912) | p (OR) | OR [95%CI] | p (aOR) | aOR [95%CI] |
| Sex | |||||||
| Male | 417 (43.2) | 28 (51.8) | 389 (42.6) | 0.187 | 0.69 [0.40–1.20] | 0.977 | 1.01 [0.47–2.18] |
| Female | 549 (56.8) | 26 (48.2) | 523 (57.4) | ||||
| Age (Median [IQR]) | 43 [32–55] | 56 [46–65] | 42 [31–54] | <0.001 | 1.07 [1.05–1.09] | 0.007 | 1.05 [1.01–1.08] |
| <65 | 882 (91.3) | 38 (70.4) | 844 (92.5) | ||||
| ≥65 | 84 (8.7) | 16 (29.6) | 68 (7.5) | ||||
| Ethnicity | |||||||
| White/European | 484 (50.1) | 15 (27.8) | 469 (51.4) | 0.002 | 2.75 [1.47–5.14] | 0.014 | 2.72 [1.22–6.05] |
| Non-White/European | 408 (42.2) | 33 (61.1) | 375 (41.1) | ||||
| Mixed Ethnicity | 48 (5.0) | 1 (1.8) | 47 (5.2) | ||||
| Unknown | 26 (2.7) | 5 (9.3) | 21 (2.3) | ||||
| BMI (Median [IQR]) | 25.9 [22.9–29.1] | 30.2 [26.6–34.6] | 25.8 [22.8–28.7] | <0.001 | 1.18 [1.12–1.24] | <0.001 | 1.17 [1.10–1.24] |
| <25 kg/m2 | 303 (31.4) | 4 (7.4) | 299 (32.8) | ||||
| ≥25 kg/m2 | 419 (43.4) | 35 (64.8) | 384 (42.1) | ||||
| Unknown | 244 (25.2) | 15 (27.8) | 229 (25.1) | ||||
| Viral Variants | |||||||
| Wild-Type | 277 (28.7) | 7 (13.0) | 270 (29.6) | 0.045 | 2.44 [1.02–5.83] | 0.012 | 5.43 [1.45–20.34] |
| Variant | 353 (36.5) | 21 (38.9) | 332 (36.4) | ||||
| Unknown | 336 (34.8) | 26 (48.1) | 310 (34.0) | ||||
| Vaccination Status (at COVID-19 positivity date) | |||||||
| Unvaccinated | 668 (69.1) | 44 (81.5) | 624 (68.4) | 0.003 | 0.12 [0.03–0.49] | N/A | N/A |
| Vaccinated (Any dose) | 244 (25.3) | 2 (3.7) | 242 (26.5) | ||||
| Unknown | 54 (5.6) | 8 (14.8) | 46 (5.1) | ||||
| Underlying Health Conditions | |||||||
| None | 414 (42.9) | 18 (33.3) | 396 (43.4) | 0.148 | 1.53 [0.86–2.74] | N/A | N/A |
| Any (≥1) | 552 (57.1) | 36 (66.7) | 516 (56.6) | ||||
| History of Smoking | |||||||
| Yes | 357 (37.0) | 16 (29.6) | 341 (37.4) | 0.565 | 0.83 [0.45–1.55] | 0.745 | 1.14 [0.52–2.52] |
| No | 582 (60.2) | 31 (57.4) | 551 (60.4) | ||||
| Unknown | 27 (2.8) | 7 (13.0) | 20 (2.2) | ||||
| No. of Observations (%) | |||||||
|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | ||||||
| Health Condition | Inpatient (n = 54) | Outpatient (n = 912) | Total (n = 966) | p (OR) | OR [95%CI] | p (aOR) | aOR [95%CI] |
| Hypertension | |||||||
| Yes | 22 (40.7) | 101 (11.1) | 123 (12.7) | <0.001 | 6.56 [3.58–12.01] | 0.015 | 2.78 [1.22–6.34] |
| No | 26 (48.1) | 783 (85.9) | 809 (83.7) | ||||
| Unknown | 6 (11.1) | 28 (3.1) | 34 (3.5) | ||||
| Endocrine Conditions | |||||||
| Yes | 17 (31.5) | 100 (11.0) | 117 (12.1) | <0.001 | 4.20 [2.25–7.83] | 0.343 | 1.91 [0.50–7.32] |
| Diabetes (Any) | 13 (24.1) | 48 (5.3) | 61 (6.3) | <0.001 | 6.37 [3.17–12.80] | 0.677 | 0.79 [0.26–2.41] |
| Type 2 Diabetes | 13 (24.1) | 45 (4.9) | 58 (6.0) | ||||
| Type 1 Diabetes | 1 (1.9) | 5 (0.5) | 6 (0.6) | ||||
| Endocrine Cancer | 1 (1.9) | 5 (0.5) | 6 (0.6) | ||||
| Endocrine Autoimmune Disorders | 0 (0.0) | 10 (1.1) | 10 (1.0) | ||||
| Gestational Diabetes | 0 (0.0) | 2 (0.2) | 2 (0.2) | ||||
| Maturity-Onset Diabetes of the Young | 0 (0.0) | 2 (0.2) | 2 (0.2) | ||||
| Pre-Diabetes | 0 (0.0) | 2 (0.2) | 2 (0.2) | ||||
| No | 32 (59.3) | 790 (86.6) | 822 (85.1) | ||||
| Unknown | 5 (9.3) | 22 (2.4) | 27 (2.8) | ||||
| Cardiovascular Conditions | |||||||
| Yes | 11 (20.4) | 72 (7.9) | 83 (8.6) | <0.001 | 3.55 [1.73–7.29] | 0.787 | 1.16 [0.39–3.44] |
| No | 35 (64.8) | 814 (89.3) | 849 (87.9) | ||||
| Unknown | 8 (14.8) | 26 (2.9) | 34 (3.5) | ||||
| Cancer | |||||||
| Yes | 9 (16.7) | 47 (5.2) | 56 (5.8) | <0.001 | 4.14 [1.89–9.05] | 0.523 | 1.46 [0.46–4.66] |
| No | 39 (72.2) | 843 (92.4) | 882 (91.3) | ||||
| Unknown | 6 (11.1) | 22 (2.4) | 28 (2.9) | ||||
| Lipid Conditions | |||||||
| Yes | 7 (13.0) | 43 (4.7) | 50 (5.2) | 0.006 | 3.32 [1.41–7.82] | 0.503 | 1.49 [0.47–4.74] |
| No | 41 (75.9) | 835 (91.6) | 876 (90.7) | ||||
| Unknown | 6 (11.1) | 34 (3.7) | 40 (4.1) | ||||
| Hepatic Conditions | |||||||
| Yes | 6 (11.1) | 35 (3.8) | 41 (4.2) | 0.009 | 3.41 [1.36–8.54] | 0.259 | 2.03 [0.59–6.93] |
| Viral Hepatitis | 1 (1.9) | 8 (0.9) | 9 (0.9) | ||||
| No | 43 (79.6) | 855 (93.8) | 898 (93.0) | ||||
| Unknown | 5 (9.3) | 22 (2.4) | 27 (2.8) | ||||
| Blood Conditions | |||||||
| Yes | 5 (9.3) | 91 (10.0) | 96 (9.9) | 0.927 | 1.05 [0.40–2.71] | 0.471 | 0.53 [0.09–2.97] |
| Iron Disorders | 4 (7.4) | 69 (7.6) | 73 (7.6) | ||||
| Blood Cancer | 0 (0.0) | 6 (0.7) | 6 (0.6) | ||||
| Blood Autoimmune Disorders | 0 (0.0) | 3 (0.3) | 3 (0.3) | ||||
| No | 42 (77.8) | 799 (87.6) | 841 (87.1) | ||||
| Unknown | 7 (13.0) | 22 (2.4) | 29 (3.0) | ||||
| Gastrointestinal Conditions | |||||||
| Yes | 5 (9.3) | 137 (15.0) | 142 (14.7) | 0.326 | 0.62 [0.24–1.60] | 0.837 | 0.89 [0.31–2.59] |
| Gastrointestinal Autoimmune Disorders | 1 (1.9) | 17 (1.9) | 18 (1.9) | ||||
| Gastrointestinal Cancer | 1 (1.9) | 9 (1.0) | 10 (1.0) | ||||
| No | 44 (81.5) | 752 (82.5) | 796 (82.4) | ||||
| Unknown | 5 (9.3) | 23 (2.5) | 28 (2.9) | ||||
| Pulmonary Conditions | |||||||
| Yes | 4 (7.4) | 91 (10.0) | 95 (9.8) | 0.762 | 0.85 [0.30–2.43] | 0.883 | 1.10 [0.32–3.81] |
| No | 41 (75.9) | 793 (87.0) | 834 (86.3) | ||||
| Unknown | 9 (16.7) | 28 (3.1) | 37 (3.8) | ||||
| Autoimmune Conditions | |||||||
| Yes | 4 (7.4) | 60 (6.6) | 64 (6.6) | 0.706 | 1.23 [0.43–3.52] | 0.264 | 2.15 [0.56–8.23] |
| No | 45 (83.3) | 827 (90.7) | 872 (90.3) | ||||
| Unknown | 5 (9.3) | 25 (2.7) | 30 (3.1) | ||||
| Neurologic/Psychiatric Conditions | |||||||
| Yes | 3 (5.6) | 64 (7.0) | 67 (6.9) | 0.853 | 0.89 [0.27–2.96] | 0.834 | 1.18 [0.25–5.66] |
| Neurological Autoimmune Disorders | 1 (1.9) | 0 (0.0) | 1 (0.1) | ||||
| No | 43 (79.6) | 819 (89.8) | 862 (89.2) | ||||
| Unknown | 8 (14.8) | 29 (3.2) | 37 (3.8) | ||||
| Renal Conditions | |||||||
| Yes | 3 (5.6) | 19 (2.1) | 22 (2.3) | 0.085 | 3.00 [0.86–10.52] | N/A | N/A |
| Renal Cancer | 1 (1.9) | 0 (0.0) | 1 (0.1) | ||||
| Renal Autoimmune Disorders | 0 (0.0) | 2 (0.2) | 2 (0.2) | ||||
| No | 46 (85.2) | 875 (95.9) | 921 (95.3) | ||||
| Unknown | 5 (9.3) | 18 (2.0) | 23 (2.4) | ||||
| Non-SARS-CoV-2 Viral Infections | |||||||
| Yes | 1 (1.9) | 33 (3.6) | 34 (3.5) | 0.559 | 0.55 [0.07–4.10] | 0.697 | 0.64 [0.07–6.04] |
| No | 47 (87.0) | 852 (93.4) | 899 (93.1) | ||||
| Unknown | 6 (11.1) | 27 (3.0) | 33 (3.4) | ||||
| Hereditary Genetic Conditions | |||||||
| Yes | 0 (0.0) | 14 (1.5) | 14 (1.4) | N/A | N/A | N/A | N/A |
| Hereditary Blood Disorders | 0 (0.0) | 8 (0.9) | 8 (0.8) | ||||
| Hereditary Lipid Disorders | 0 (0.0) | 1 (0.1) | 1 (0.1) | ||||
| No | 50 (92.6) | 879 (96.4) | 929 (96.2) | ||||
| Unknown | 4 (7.4) | 19 (2.1) | 23 (2.4) | ||||
| Other Conditions | |||||||
| Yes | 13 (24.1) | 91 (10.0) | 104 (10.8) | ||||
| Sleep Disorders | 5 (9.3) | 34 (3.7) | 39 (4.0) | ||||
| Muscle/Joint Conditions | 4 (7.4) | 21 (2.3) | 25 (2.6) | ||||
| Gynecological/Urological Conditions | 4 (7.4) | 14 (1.5) | 18 (1.9) | ||||
| Dermatological Conditions | 1 (1.9) | 12 (1.3) | 13 (1.3) | ||||
| Bone Conditions | 0 (0.0) | 9 (1.0) | 9 (0.9) | ||||
| Ophthalmologic Conditions | 0 (0.0) | 8 (0.9) | 8 (0.8) | ||||
| No | 41 (75.9) | 821 (90.0) | 862 (89.2) | ||||
| COVID-19 Symptoms | Inpatient (n = 54) | Outpatient (n = 912) | Total (n = 966) | p |
|---|---|---|---|---|
| Shortness of breath | ||||
| Yes | 42 (77.8%) | 328 (36.0%) | 370 (38.3%) | <0.001 |
| No | 2 (3.7%) | 510 (55.9%) | 512 (53.0%) | |
| Unknown | 10 (18.5%) | 74 (8.1%) | 84 (8.7%) | |
| Fever | ||||
| Yes | 39 (72.2%) | 512 (56.1%) | 551 (57.0%) | <0.001 |
| No | 4 (7.4%) | 363 (39.8%) | 367 (38.0%) | |
| Unknown | 11 (20.4%) | 37 (4.1%) | 48 (5.0%) | |
| Fatigue | ||||
| Yes | 39 (72.2%) | 734 (80.5%) | 773 (80.0%) | 0.135 |
| No | 3 (5.6%) | 136 (14.9%) | 139 (14.4%) | |
| Unknown | 12 (22.2%) | 42 (4.6%) | 54 (5.6%) | |
| Muscle aches | ||||
| Yes | 30 (55.6%) | 585 (64.1%) | 615 (63.7%) | 0.644 |
| No | 12 (22.2%) | 275 (30.2%) | 287 (29.7%) | |
| Unknown | 12 (22.2%) | 52 (5.7%) | 64 (6.6%) | |
| Non-productive cough | ||||
| Yes | 28 (51.9%) | 493 (54.1%) | 521 (53.9%) | 0.132 |
| No | 12 (22.2%) | 357 (39.1%) | 369 (38.2%) | |
| Unknown | 14 (25.9%) | 62 (6.8%) | 76 (7.9%) | |
| Headache | ||||
| Yes | 28 (51.9%) | 598 (65.6%) | 626 (64.8%) | 0.644 |
| No | 10 (18.5%) | 254 (27.9%) | 264 (27.3%) | |
| Unknown | 16 (29.6%) | 60 (6.6%) | 76 (7.9%) | |
| Joint pain | ||||
| Yes | 23 (42.6%) | 397 (43.5%) | 420 (43.5%) | 0.208 |
| No | 17 (31.5%) | 442 (48.5%) | 459 (47.5%) | |
| Unknown | 14 (25.9%) | 73 (8.0%) | 87 (9.0%) | |
| Sore throat | ||||
| Yes | 22 (40.7%) | 483 (53.0%) | 505 (52.3%) | 0.702 |
| No | 19 (35.2%) | 369 (40.5%) | 388 (40.2%) | |
| Unknown | 13 (24.1%) | 60 (6.6%) | 73 (7.6%) | |
| Productive cough | ||||
| Yes | 20 (37.0%) | 315 (34.5%) | 335 (34.7%) | 0.207 |
| No | 22 (40.7%) | 516 (56.6%) | 538 (55.7%) | |
| Unknown | 12 (22.2%) | 81 (8.9%) | 93 (9.6%) | |
| Runny nose/nasal congestion | ||||
| Yes | 20 (37.0%) | 546 (59.9%) | 566 (58.6%) | 0.033 |
| No | 22 (40.7%) | 309 (33.9%) | 331 (34.3%) | |
| Unknown | 12 (22.2%) | 57 (6.3%) | 69 (7.1%) | |
| Chest pain | ||||
| Yes | 20 (37.0%) | 239 (26.2%) | 259 (26.8%) | 0.004 |
| No | 20 (37.0%) | 590 (64.7%) | 610 (63.1%) | |
| Unknown | 14 (25.9%) | 83 (9.1%) | 97 (10.0%) | |
| Wheezing | ||||
| Yes | 15 (27.8%) | 140 (15.4%) | 155 (16.0%) | <0.001 |
| No | 23 (42.6%) | 688 (75.4%) | 711 (73.6%) | |
| Unknown | 16 (29.6%) | 84 (9.2%) | 100 (10.4%) | |
| Loss of taste | ||||
| Yes | 16 (29.6%) | 440 (48.2%) | 456 (47.2%) | 0.142 |
| No | 24 (44.4%) | 408 (44.7%) | 432 (44.7%) | |
| Unknown | 14 (25.9%) | 64 (7.0%) | 78 (8.1%) | |
| Altered consciousness/confusion | ||||
| Yes | 14 (25.9%) | 141 (15.5%) | 155 (16.0%) | 0.001 |
| No | 23 (42.6%) | 691 (75.8%) | 714 (73.9%) | |
| Unknown | 17 (31.5%) | 80 (8.8%) | 97 (10.0%) | |
| Diarrhea | ||||
| Yes | 15 (27.8%) | 260 (28.5%) | 275 (28.5%) | 0.397 |
| No | 25 (46.3%) | 575 (63.0%) | 600 (62.1%) | |
| Unknown | 14 (25.9%) | 77 (8.4%) | 91 (9.4%) | |
| Abdominal pain | ||||
| Yes | 12 (22.2%) | 132 (14.5%) | 144 (14.9%) | 0.015 |
| No | 27 (50.0%) | 698 (76.5%) | 725 (75.1%) | |
| Unknown | 15 (27.8%) | 82 (9.0%) | 97 (10.0%) | |
| Loss of smell | ||||
| Yes | 12 (22.2%) | 485 (53.2%) | 497 (51.4%) | 0.001 |
| No | 28 (51.9%) | 369 (40.5%) | 397 (41.1%) | |
| Unknown | 14 (25.9%) | 58 (6.4%) | 72 (7.5%) | |
| Vomiting/nausea | ||||
| Yes | 11 (20.4%) | 134 (14.7%) | 145 (15.0%) | 0.047 |
| No | 28 (51.9%) | 699 (76.6%) | 727 (75.3%) | |
| Unknown | 15 (27.8%) | 79 (8.7%) | 94 (9.7%) | |
| Skin rash | ||||
| Yes | 5 (9.3%) | 68 (7.5%) | 73 (7.6%) | 0.369 |
| No | 34 (63.0%) | 754 (82.7%) | 788 (81.6%) | |
| Unknown | 15 (27.8%) | 90 (9.9%) | 105 (10.9%) | |
| Cough (with hemoptysis) | ||||
| Yes | 2 (3.7%) | 19 (2.1%) | 21 (2.2%) | 0.245 |
| No | 36 (66.7%) | 782 (85.7%) | 818 (84.7%) | |
| Unknown | 16 (29.6%) | 111 (12.2%) | 127 (13.1%) | |
| Ear pain | ||||
| Yes | 1 (1.9%) | 96 (10.5%) | 97 (10.0%) | 0.112 |
| No | 37 (68.5%) | 731 (80.2%) | 768 (79.5%) | |
| Unknown | 16 (29.6%) | 85 (9.3%) | 101 (10.5%) | |
| Seizures | ||||
| Yes | 1 (1.9%) | 3 (0.3%) | 4 (0.4%) | 0.162 |
| No | 36 (66.7%) | 819 (89.8%) | 855 (88.5%) | |
| Unknown | 17 (31.5%) | 90 (9.9%) | 107 (11.1%) | |
| Conjunctivitis | ||||
| Yes | 0 (0%) | 28 (3.1%) | 28 (2.9%) | 0.630 |
| No | 38 (70.4%) | 793 (87.0%) | 831 (86.0%) | |
| Unknown | 16 (29.6%) | 91 (10.0%) | 107 (11.1%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morgan, G.; Casalino, S.; Chowdhary, S.; Frangione, E.; Fung, C.Y.J.; Haller, S.; Lapadula, E.; Scott, M.; Wolday, D.; Young, J.; et al. Characterizing Risk Factors for Hospitalization and Clinical Characteristics in a Cohort of COVID-19 Patients Enrolled in the GENCOV Study. Viruses 2023, 15, 1764. https://0-doi-org.brum.beds.ac.uk/10.3390/v15081764
Morgan G, Casalino S, Chowdhary S, Frangione E, Fung CYJ, Haller S, Lapadula E, Scott M, Wolday D, Young J, et al. Characterizing Risk Factors for Hospitalization and Clinical Characteristics in a Cohort of COVID-19 Patients Enrolled in the GENCOV Study. Viruses. 2023; 15(8):1764. https://0-doi-org.brum.beds.ac.uk/10.3390/v15081764
Chicago/Turabian StyleMorgan, Gregory, Selina Casalino, Sunakshi Chowdhary, Erika Frangione, Chun Yiu Jordan Fung, Simona Haller, Elisa Lapadula, Mackenzie Scott, Dawit Wolday, Juliet Young, and et al. 2023. "Characterizing Risk Factors for Hospitalization and Clinical Characteristics in a Cohort of COVID-19 Patients Enrolled in the GENCOV Study" Viruses 15, no. 8: 1764. https://0-doi-org.brum.beds.ac.uk/10.3390/v15081764