Mucoadhesive Poloxamer-Based Hydrogels for the Release of HP-β-CD-Complexed Dexamethasone in the Treatment of Buccal Diseases

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Preparation of Hydrogels
2.2.2. Phase Solubility Diagrams and Apparent Solubility Determination
2.2.3. Rheological Characterization of Formulations
Flow Rheometry Studies
Oscillatory Rheometry Studies and Determination of Gelation Transition Temperature
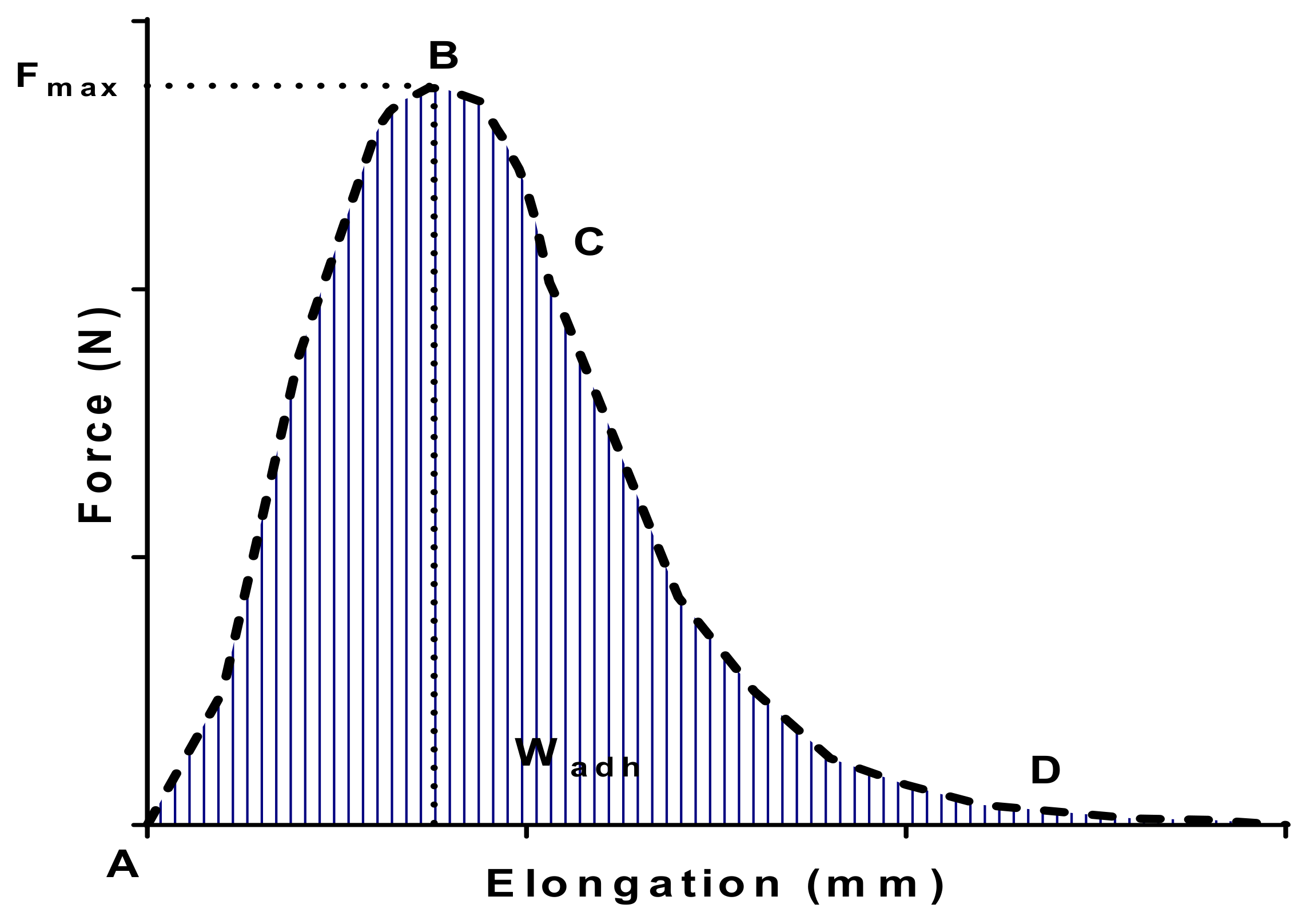
2.2.4. Measurement of the Adhesive and Mucoadhesive Forces
2.2.5. Flow-Through USP-4 Apparatus In Vitro Drug Release
2.2.6. Statistical Analysis
3. Results and Discussion
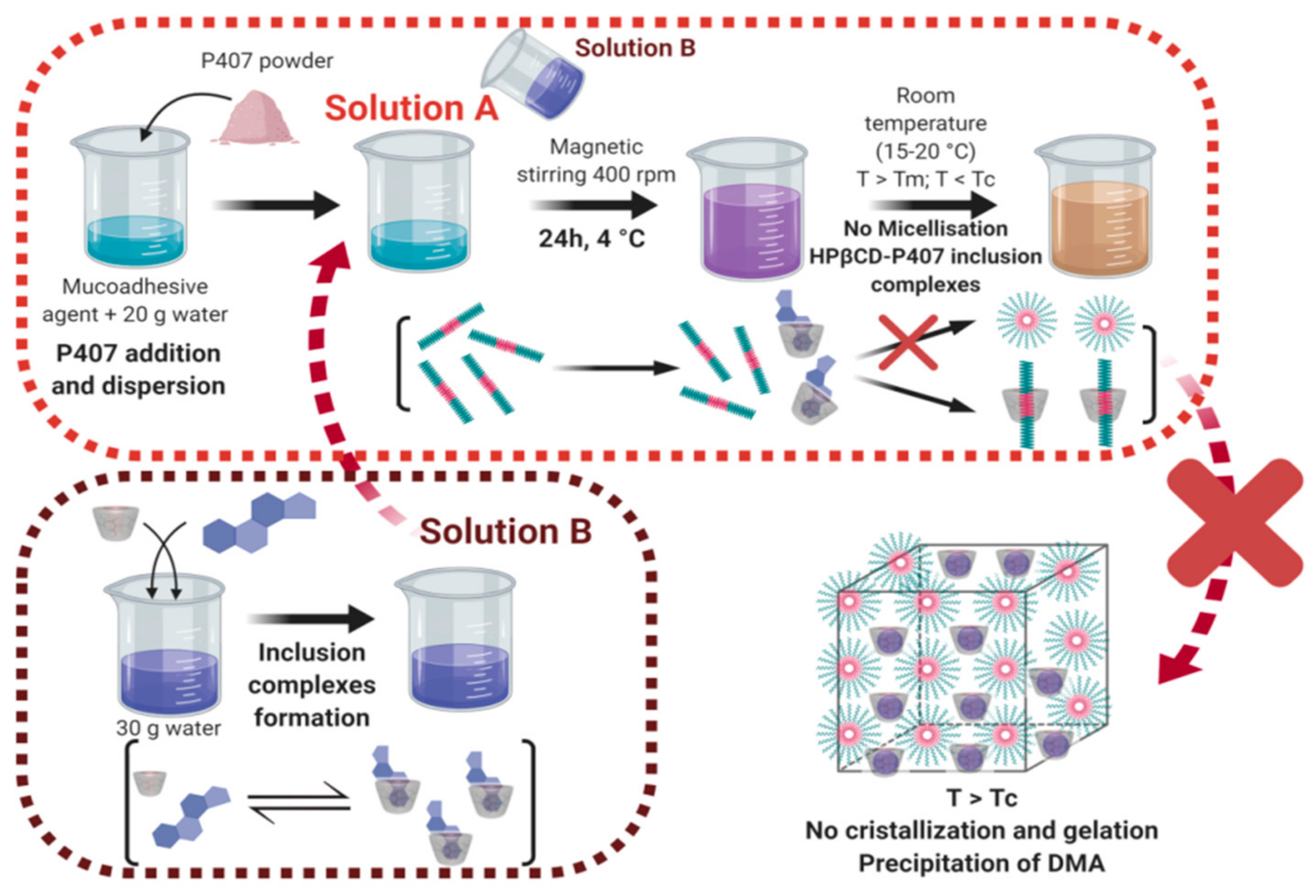
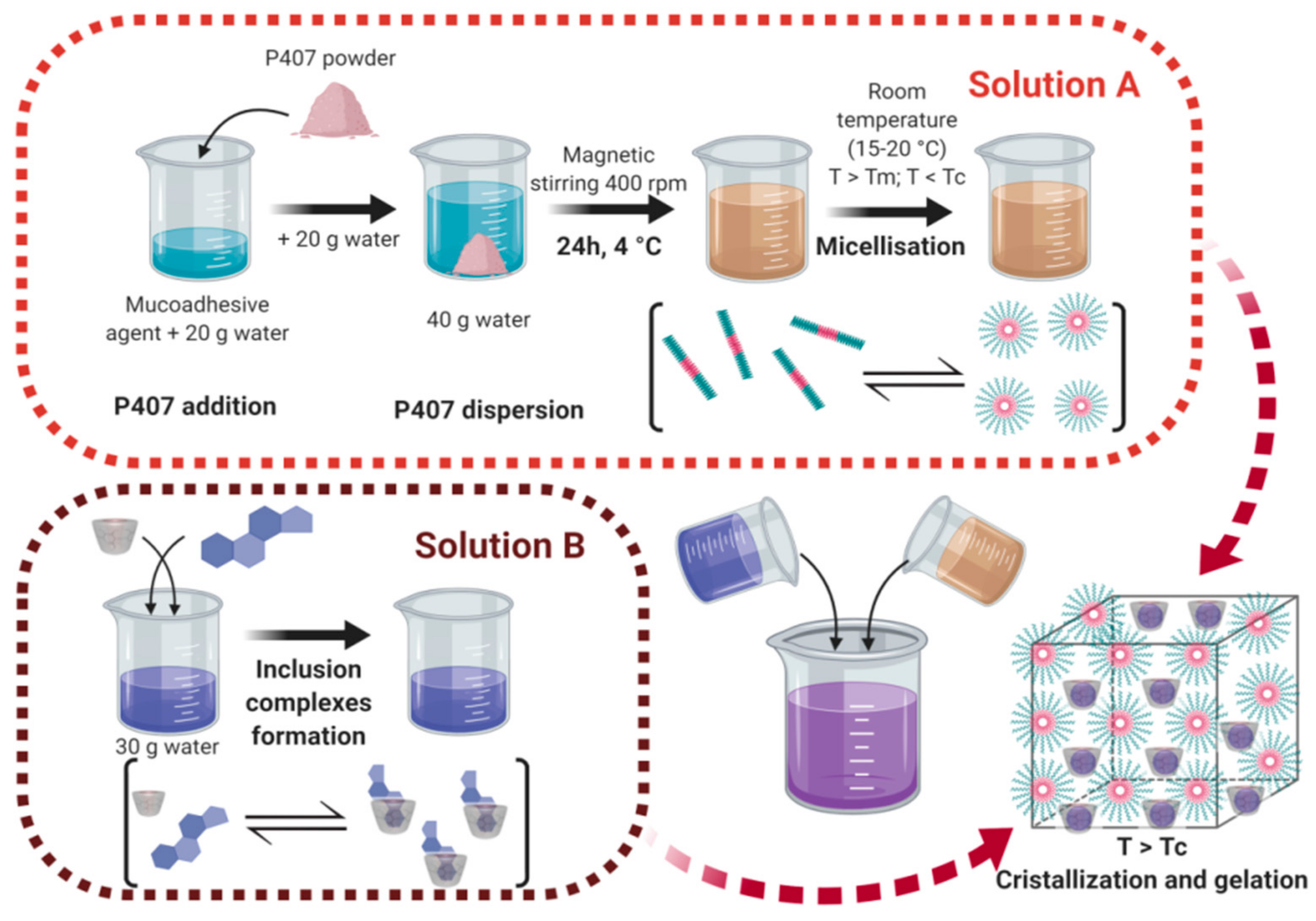
3.1. Influence of the Hydrogel Preparation Approach on the Physicochemical Behavior of Hydrogels
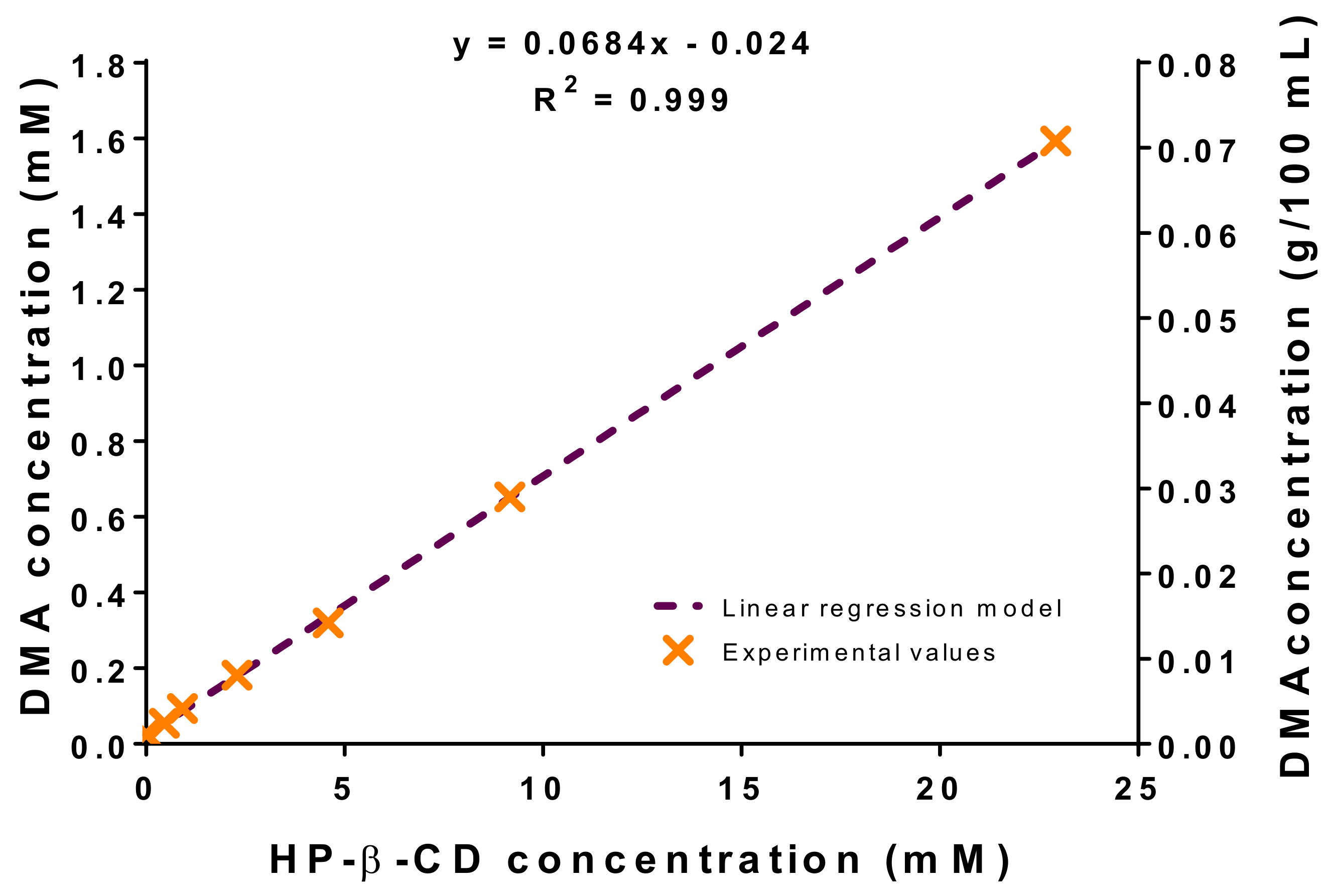
3.2. Phase Solubility Diagrams and Apparent Solubility Determination
3.3. Rheological Studies
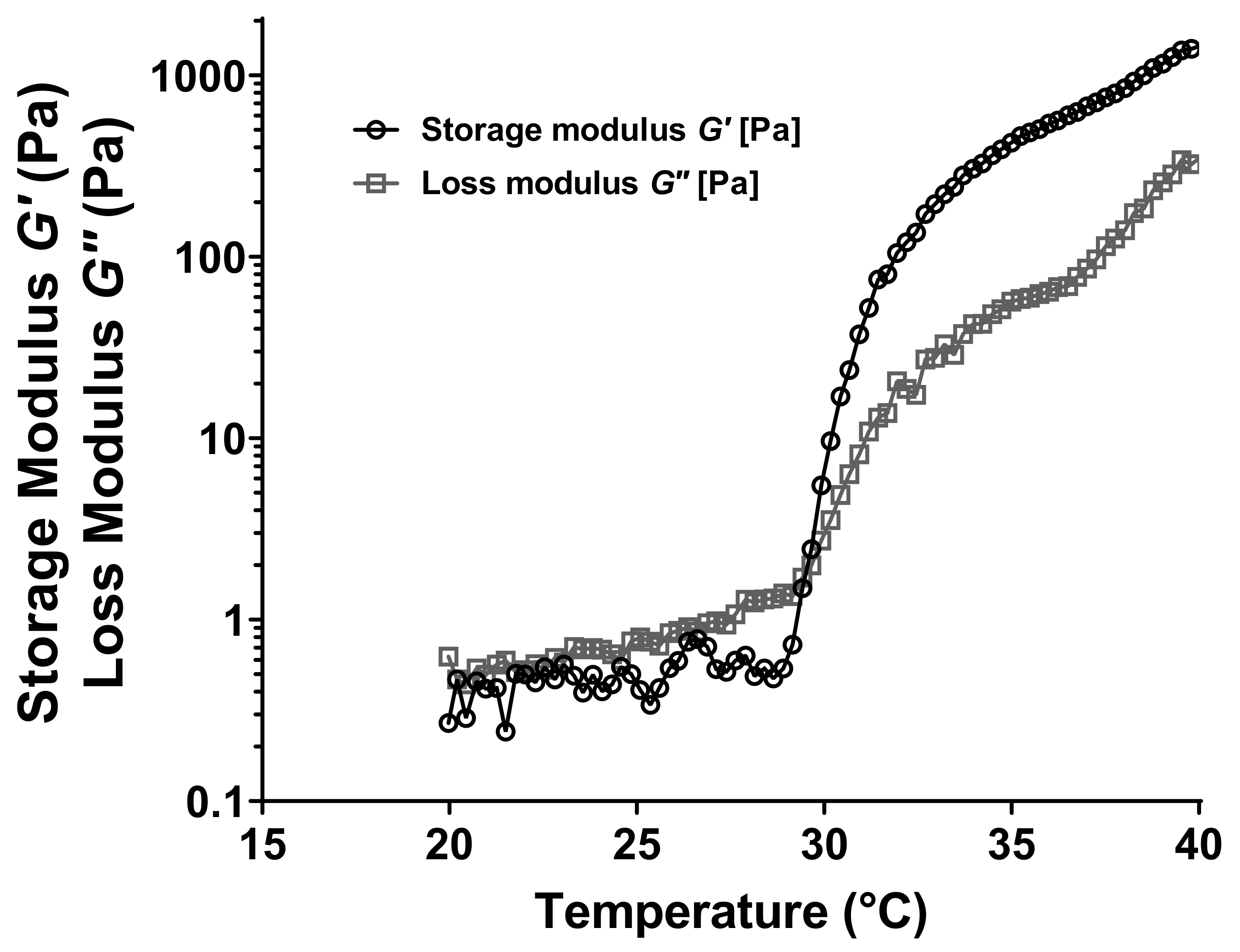
3.3.1. Oscillatory Rheometry Studies
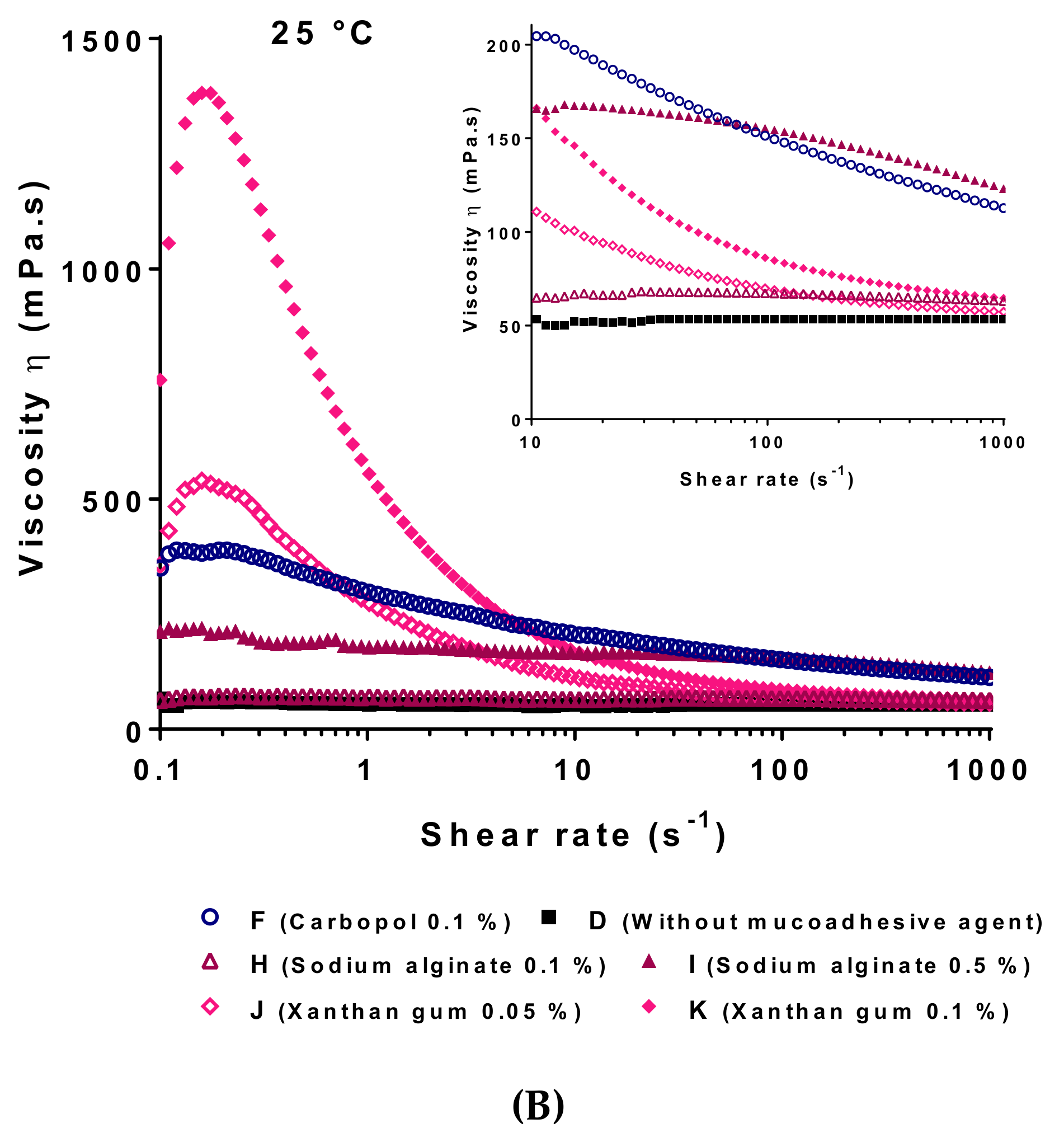
3.3.2. Flow Rheometry Studies
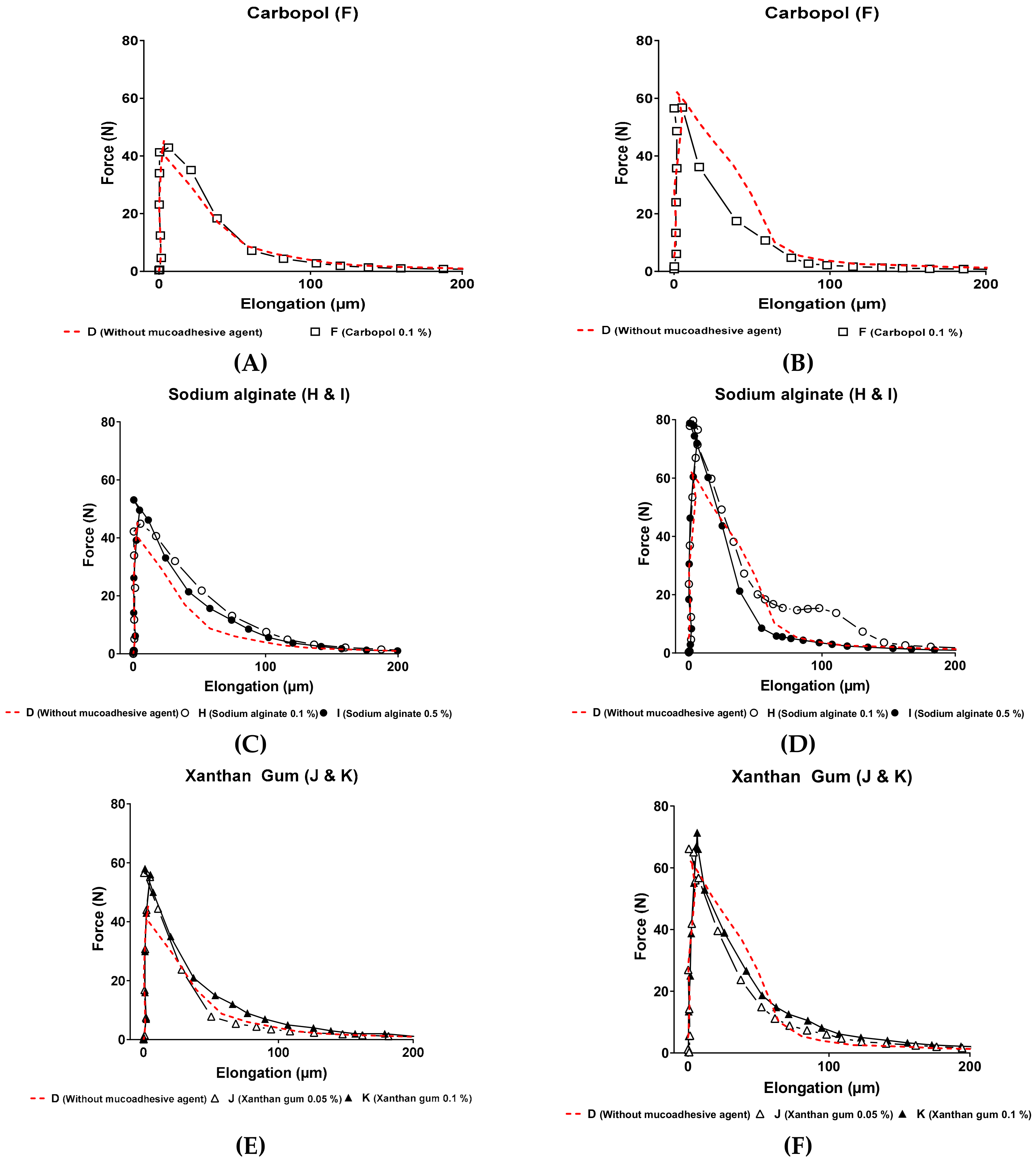
3.4. Measurement of the Adhesive and Mucoadhesive Forces
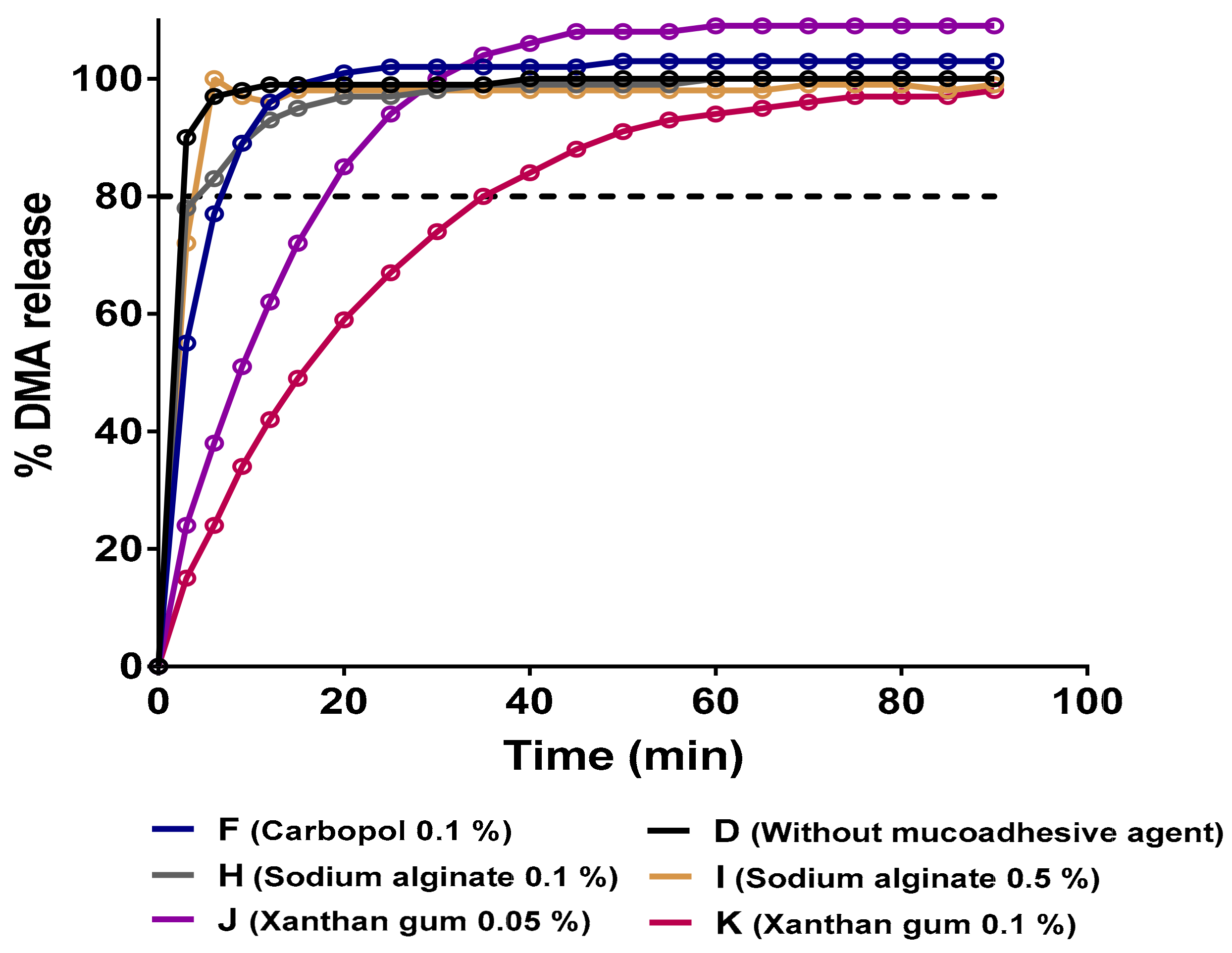
3.5. Flow-Through USP-4 Apparatus In Vitro Drug Release
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boorghani, M.; Gholizadeh, N.; Zenouz, A.T.; Vatankhah, M.; Mehdipour, M. Oral lichen planus: Clinical features, etiology, treatment and management; a review of literature. J. Dental Res. Dental Clin. Dental Prosp. 2010, 4, 3. [Google Scholar] [CrossRef]
- Gupta, S.; Jawanda, M.K. Oral lichen planus: An update on etiology, pathogenesis, clinical presentation, diagnosis and management. Indian J. Dermatol. 2015, 60, 222. [Google Scholar] [CrossRef] [PubMed]
- Baek, K.; Choi, Y. The microbiology of oral lichen planus: Is microbial infection the cause of oral lichen planus? Mol. Oral Microbiol. 2018, 33, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, N.; Scully, C.; Eveson, J.; Cunningham, S.; Porter, S. Oral cancer development in patients with oral lichen planus. J. Oral Pathol. Med. 1993, 22, 421–424. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, J. Oral lichen planus: I. A clinical evaluation of 115 cases. Oral Surg. Oral Med. Oral Pathol. 1968, 25, 31–42. [Google Scholar] [CrossRef]
- Scully, C.; El-Kom, M. Lichen planus: Review and update on pathogenesis. J. Oral Pathol. Med. 1985, 14, 431–458. [Google Scholar] [CrossRef]
- McGrath, C.; Hegarty, A.M.; Hodgson, T.A.; Porter, S.R. Patient-Centred outcome measures for oral mucosal disease are sensitive to treatment. Int. J. Oral Maxillofac. Surg. 2003, 32, 334–336. [Google Scholar] [CrossRef]
- Lozada, F.; Silverman, S. Topically applied fluocinonide in an adhesive base in the treatment of oral vesiculoerosive diseases. Arch. Dermatol. 1980, 116, 898–901. [Google Scholar] [CrossRef]
- Holbrook, W.P.; Kristmundsdóttir, T.; Loftsson, T. Aqueous hydrocortisone mouthwash solution: Clinical evaluation. Acta Odontol. Scand. 1998, 56, 157–160. [Google Scholar] [CrossRef]
- Hegarty, A.M.; Hodgson, T.A.; Lewsey, J.D.; Porter, S.R. Fluticasone propionate spray and betamethasone sodium phosphate mouthrinse: A randomized crossover study for the treatment of symptomatic oral lichen planus. J. Am. Acad. Dermatol. 2002, 47, 271–279. [Google Scholar] [CrossRef]
- Aguirre, J.; Bagan, J.; Rodriguez, C.; Jimenez, Y.; Martínez-Conde, R.; Díaz de Rojas, F.; Ponte, A. Efficacy of mometasone furoate microemulsion in the treatment of erosive-ulcerative oral lichen planus: Pilot study. J. Oral Pathol. Med. 2004, 33, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Arduino, P.; Carrozzo, M.; Gandolfo, S.; Argiolas, M.; Bertolusso, G.; Conrotto, D.; Pentenero, M.; Broccoletti, R. Course of oral lichen planus: A retrospective study of 808 northern Italian patients. Oral Dis. 2009, 15, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Moles, M.A.; Morales, P.; Rodriguez-Archilla, A.; Isabel, I.R.-A.; Gonzalez-Moles, S. Treatment of severe chronic oral erosive lesions with clobetasol propionate in aqueous solution. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2002, 93, 264–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muzio, L.L.; Della Valle, A.; Mignogna, M.D.; Pannone, G.; Bucci, P.; Bucci, E.; Sciubba, J. The treatment of oral aphthous ulceration or erosive lichen planus with topical clobetasol propionate in three preparations: A clinical and pilot study on 54 patients. J. Oral Pathol. Med. 2001, 30, 611–617. [Google Scholar] [CrossRef]
- Sardella, A.; Demarosi, F.; Oltolina, A.; Rimondini, L.; Carrassi, A. Efficacy of topical mesalazine compared with clobetasol propionate in treatment of symptomatic oral lichen planus. Oral Dis. 1998, 4, 255–259. [Google Scholar] [CrossRef]
- Ungphaiboon, S.; Nittayananta, W.; Vuddhakul, V.; Maneenuan, D.; Kietthubthew, S.; Wongpoowarak, W. Phadoongsombat, N. Formulation and efficacy of triamcinolone acetonide mouthwash for treating oral lichen planus. Am. J. Health Syst. Pharm. 2005, 62, 485–491. [Google Scholar] [CrossRef]
- González-Moles, M.A.; Scully, C. Vesiculo-Erosive Oral Mucosal Disease—Management with Topical Corticosteroids: (1) Fundamental Principles and Specific Agents Available. J. Dent. Res. 2005, 84, 294–301. [Google Scholar] [CrossRef]
- Zakrzewska, J.; Chan, E.; Thornhill, M. A systematic review of placebo-controlled randomized clinical trials of treatments used in oral lichen planus. Br. J. Dermatol. 2005, 153, 336–341. [Google Scholar] [CrossRef]
- Silverman, S.; Gorsky, M.; Lozada-Nur, F.; Giannotti, K. A prospective study of findings and management in 214 patients with oral lichen planus. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 665–670. [Google Scholar] [CrossRef]
- Thongprasom, K.; Dhanuthai, K. Steriods in the treatment of lichen planus: A review. J. Oral Sci. 2008, 50, 377–385. [Google Scholar] [CrossRef] [Green Version]
- Zegarelli, D. Ulcerative and erosive lichen planus. Treated by modified topical steroid and injection steroid therapy. N. Y. State Dent. J. 1987, 53, 23–24. [Google Scholar] [PubMed]
- Sankar, V.; Hearnden, V.; Hull, K.; Juras, D.V.; Greenberg, M.; Kerr, A.; Lockhart, P.; Patton, L.; Porter, S.; Thornhill, M. Local drug delivery for oral mucosal diseases: Challenges and opportunities: Local drug delivery for oral mucosal diseases. Oral Dis. 2011, 1, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Poddar, S. Development and characterization of mucoadhesive buccal patches of salbutamol sulphate. Curr. Drug Deliv. 2009, 6, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Salamat-Miller, N.; Chittchang, M.; Johnston, T.P. The use of mucoadhesive polymers in buccal drug delivery. Adv. Drug Deliv. Rev. 2005, 57, 1666–1691. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Tiwary, A.; Kaur, G. Investigations on interpolymer complexes of cationic guar gum and xanthan gum for formulation of bioadhesive films. Res. Pharm. Sci. 2010, 5, 79–87. [Google Scholar] [PubMed]
- Smart, J.D. Buccal drug delivery. Expert opin. Drug Deliv. 2005, 2, 507–517. [Google Scholar] [CrossRef]
- Sun, B.; Wang, W.; He, Z.; Zhang, M.; Kong, F.; Sain, M. Biopolymer Substrates in Buccal Drug Delivery: Current Status and Future Trend. Curr. Med. Chem. 2020, 27, 1661–1669. [Google Scholar] [CrossRef]
- Vasantha, P.V.; Puratchikody, A.; Mathew, S.T.; Balaraman, A.K. Development and characterization of Eudragit based mucoadhesive buccal patches of salbutamol sulfate. Saudi Pharm. J. 2011, 19, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Zeng, N.; Dumortier, G.; Maury, M.; Mignet, N.; Boudy, V. Influence of additives on a thermosensitive hydrogel for buccal delivery of salbutamol: Relation between micellization, gelation, mechanic and release properties. Int. J. Pharm. 2014, 467, 70–83. [Google Scholar] [CrossRef]
- Zeng, N.; Seguin, J.; Destruel, P.-L.; Dumortier, G.; Maury, M.; Dhotel, H.; Bessodes, M.; Scherman, D.; Mignet, N.; Boudy, V. Cyanine derivative as a suitable marker for thermosensitive in situ gelling delivery systems: In vitro and in vivo validation of a sustained buccal drug delivery. Int. J. Pharm. 2017, 534, 128–135. [Google Scholar] [CrossRef]
- Yu, S.; Zhang, X.; Tan, G.; Tian, L.; Liu, D.; Liu, Y.; Yang, X.; Pan, W. A novel pH-induced thermosensitive hydrogel composed of carboxymethyl chitosan and poloxamer cross-linked by glutaraldehyde for ophthalmic drug delivery. Carbohydr. Polym. 2017, 155, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Zeng, N.; Mignet, N.; Dumortier, G.; Olivier, E.; Seguin, J.; Maury, M.; Scherman, D.; Rat, P.; Boudy, V. Poloxamer bioadhesive hydrogel for buccal drug delivery: Cytotoxicity and trans-epithelial permeability evaluations using TR146 human buccal epithelial cell line. Int. J. Pharm. 2015, 495, 1028–1037. [Google Scholar] [CrossRef] [PubMed]
- Al Sabbagh, C.; Seguin, J.; Agapova, E.; Kramerich, D.; Boudy, V.; Mignet, N. Thermosensitive hydrogels for local delivery of 5-fluorouracil as neoadjuvant or adjuvant therapy in colorectal cancer. Eur. J. Pharm. Biopharm. 2020, 157, 154–164. [Google Scholar] [CrossRef]
- Hoare, T.R.; Kohane, D.S. Hydrogels in drug delivery: Progress and challenges. Polymer 2008, 49, 1993–2007. [Google Scholar] [CrossRef] [Green Version]
- Peppas, N.; Bures, P.; Leobandung, W.; Ichikawa, H. Hydrogels in pharmaceutical formulations. Eur. J. Pharm. Biopharm. 2000, 50, 27–46. [Google Scholar] [CrossRef]
- Koffi, A.A.; Agnely, F.; Ponchel, G.; Grossiord, J.L. Modulation of the rheological and mucoadhesive properties of thermosensitive poloxamer-based hydrogels intended for the rectal administration of quinine. Eur. J. Pharm. Sci. 2006, 27, 328–335. [Google Scholar] [CrossRef]
- Singh, V.; Khullar, P.; Dave, P.N.; Kaur, N. Micelles, mixed micelles, and applications of polyoxypropylene (PPO)-polyoxyethylene (PEO)-polyoxypropylene (PPO) triblock polymers. Int. J. Ind. Chem. 2013, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Sandri, G.; Cristina Bonferoni, M.; Ferrari, F.; Rossi, S.; Del Fante, C.; Perotti, C.; Gallanti, A.; Caramella, C. An in situ gelling buccal spray containing platelet lysate for the treatment of oral mucositis. Curr. Drug Discov. Technol. 2011, 8, 277–285. [Google Scholar] [CrossRef]
- Dumortier, G.; Grossiord, J.L.; Agnely, F.; Chaumeil, J.C. A Review of Poloxamer 407 Pharmaceutical and Pharmacological Characteristics. Pharm. Res. 2006, 23, 2709–2728. [Google Scholar] [CrossRef]
- Bochot, A.; Fattal, E.; Gulik, A.; Couarraze, G.; Couvreur, P. Liposomes dispersed within a thermosensitive gel: A new dosage form for ocular delivery of oligonucleotides. Pharm. Res. 1998, 15, 1364–1369. [Google Scholar] [CrossRef]
- Henry, R. Burn wound coverings and the use of poloxamer preparations. Crit. Rev. Biocompat. 1989, 5, 207–220. [Google Scholar]
- Morikawa, K.; Okada, F.; Hosokawa, M.; Kobayashi, H. Enhancement of therapeutic effects of recombinant interleukin 2 on a transplantable rat fibrosarcoma by the use of a sustained release vehicle, pluronic gel. Cancer Res. 1987, 47, 37–41. [Google Scholar] [PubMed]
- Tomida, H.; Shinohara, M.; Kuwada, N.; Kiryu, S. In vitro release characteristics of diclofenac and hydrocortisone from Pluronic F-127 gels. Acta Pharm. Suec. 1987, 24, 263–272. [Google Scholar] [PubMed]
- Chen, C.-C.; Fang, C.-L.; Al-Suwayeh, S.A.; Leu, Y.-L.; Fang, J.-Y. Transdermal delivery of selegiline from alginate—Pluronic composite thermogels. Int. J. Pharm. 2011, 415, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.-H.; Leu, Y.-L.; Hu, J.-W.; Fang, J.-Y. Physicochemical characterization and drug release of thermosensitive hydrogels composed of a hyaluronic acid/pluronic f127 graft. Chem. Pharm. Bull. 2009, 57, 453–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fefelova, N.A.; Nurkeeva, Z.S.; Mun, G.A.; Khutoryanskiy, V.V. Mucoadhesive interactions of amphiphilic cationic copolymers based on [2-(methacryloyloxy)ethyl]trimethylammonium chloride. Int. J. Pharm. 2007, 339, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Heemstra, L.B.; Finnin, B.C.; Nicolazzo, J.A. The Buccal Mucosa as an Alternative Route for the Systemic Delivery of Risperidone. J. Pharm. Sci. 2010, 99, 4584–4592. [Google Scholar] [CrossRef]
- Russo, E.; Selmin, F.; Baldassari, S.; Gennari, C.G.M.; Caviglioli, G.; Cilurzo, F.; Minghetti, P.; Parodi, B. A focus on mucoadhesive polymers and their application in buccal dosage forms. J. Drug Deliv. Sci. Technol. 2016, 32, 113–125. [Google Scholar] [CrossRef]
- Remuñán-López, C.; Portero, A.; Vila-Jato, J.L.; Alonso, M.J. Design and evaluation of chitosan/ethylcellulose mucoadhesive bilayered devices for buccal drug delivery. J. Control. Release 1998, 55, 143–152. [Google Scholar] [CrossRef]
- Westhaus, E.; Messersmith, P.B. Triggered release of calcium from lipid vesicles: A bioinspired strategy for rapid gelation of polysaccharide and protein hydrogels. Biomaterials 2001, 22, 453–462. [Google Scholar] [CrossRef]
- Menchicchi, B.; Fuenzalida, J.P.; Hensel, A.; Swamy, M.J.; David, L.; Rochas, C.; Goycoolea, F.M. Biophysical Analysis of the Molecular Interactions between Polysaccharides and Mucin. Biomacromolecules 2015, 16, 924–935. [Google Scholar] [CrossRef] [PubMed]
- Roy, S.; Pal, K.; Anis, A.; Pramanik, K.; Prabhakar, B. Polymers in Mucoadhesive Drug-Delivery Systems: A Brief Note. Des. Monomers Polym. 2009, 12, 483–495. [Google Scholar] [CrossRef] [Green Version]
- Mughal, M.A.; Iqbal, Z.; Neau, S.H. Guar Gum, Xanthan Gum, and HPMC Can Define Release Mechanisms and Sustain Release of Propranolol Hydrochloride. AAPS PharmSciTech 2011, 12, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varshosaz, J.; Tavakoli, N.; Kheirolahi, F. Use of hydrophilic natural gums in formulation of sustained-release matrix tablets of tramadol hydrochloride. AAPS PharmSciTech 2006, 7, E168–E174. [Google Scholar] [CrossRef]
- Verhoeven, E.; Vervaet, C.; Remon, J.P. Xanthan gum to tailor drug release of sustained-release ethylcellulose mini-matrices prepared via hot-melt extrusion: In vitro and in vivo evaluation. Eur. J. Pharm. Biopharma. 2006, 63, 320–330. [Google Scholar] [CrossRef]
- Setterfield, J.; Black, M.; Challacombe, S. The management of oral lichen planus: Clinical dermatology—Review article. Clin. Exp. Dermatol. 2000, 25, 176–182. [Google Scholar] [CrossRef]
- Thongprasom, K.; Luengvisut, P.; Wongwatanakij, A.; Boonjatturus, C. Clinical evaluation in treatment of oral lichen planus with topical fluocinolone acetonide: A 2-year follow-up. J. Oral Pathol. Med. 2003, 32, 315–322. [Google Scholar] [CrossRef]
- Brewster, M.E.; Loftsson, T. Cyclodextrins as pharmaceutical solubilizers. Adv. Drug Deliv. Rev. 2007, 59, 645–666. [Google Scholar] [CrossRef]
- Siegal, T.; Soti, F.; Biegon, A.; Pop, E.; Brewster, M.E. Effect of a chemical delivery system for dexamethasone (Dex-CDS) on peritumoral edema in an experimental brain tumor model. Pharm. Res. 1997, 14, 672–675. [Google Scholar] [CrossRef]
- Aleem, O.; Kuchekar, B.; Pore, Y.; Late, S. Effect of β-cyclodextrin and hydroxypropyl β-cyclodextrin complexation on physicochemical properties and antimicrobial activity of cefdinir. J. Pharm. Biomed. Anal. 2008, 47, 535–540. [Google Scholar] [CrossRef]
- Bibby, D.C.; Davies, N.M.; Tucker, I.G. Mechanisms by which cyclodextrins modify drug release from polymeric drug delivery systems. Int. J. Pharm. 2000, 197, 1–11. [Google Scholar] [CrossRef]
- Criscuolo, G.R. The genesis of peritumoral vasogenic brain edema and tumor cysts: A hypothetical role for tumor-derived vascular permeability factor. Yale J. Biol. Med. 1993, 66, 277–314. [Google Scholar] [PubMed]
- Brewster, M.; Loftsson, T. The use of chemically modified cyclodextrins in the development of formulations for chemical delivery systems. Pharmazie 2002, 57, 94–101. [Google Scholar]
- Elmotasem, H.; Awad, G.E.A. A stepwise optimization strategy to formulate in situ gelling formulations comprising fluconazole-hydroxypropyl-beta-cyclodextrin complex loaded niosomal vesicles and Eudragit nanoparticles for enhanced antifungal activity and prolonged ocular delivery. Asian J. Pharm. Sci. 2019, 15, 617–636. [Google Scholar] [CrossRef] [PubMed]
- Stella, V.J.; Rao, V.M.; Zannou, E.A.; Zia, V. Mechanisms of drug release from cyclodextrin complexes. Adv. Drug Deliv. Rev. 1999, 36, 3–16. [Google Scholar] [CrossRef]
- Gavriloaia, M.-R.; Budura, E.-A.; Aramã, C.; Nitulescu, M.; Lupuleasa, D. Phase solubility studies and scanning electron microscopy of dexamethasone inclusion complexes with b-cyclodextrin and hydroxypropyl b-cyclodextrin. Studia Univ. Vasile Goldis Seria Stiintele Vietii (Life Sci. Ser.) 2012, 22, 83. [Google Scholar]
- Koffi, A.; Agnely, F.; Besnard, M.; Brou, J.K.; Grossiord, J.; Ponchel, G. In vitro and in vivo characteristics of a thermogelling and bioadhesive delivery system intended for rectal administration of quinine in children. Eur. J. Pharm. Biopharm. 2008, 69, 167–175. [Google Scholar] [CrossRef]
- Kristinsson, J.K.; Fridriksdóttir, H.; Thorisdottir, S.; Sigurdardottir, A.M.; Stefansson, E.; Loftsson, T. Dexamethasone-cyclodextrin-polymer co-complexes in aqueous eye drops. Aqueous humor pharmacokinetics in humans. Invest. Ophthalmol. Vis. Sci. 1996, 37, 1199–1203. [Google Scholar]
- Higuchi, T.; Connors, K. Phase solubility diagram. Adv. Anal. Chem. Instrum. 1965, 4, 117–212. [Google Scholar]
- Carreau, P.J. Rheological equations from molecular network theories. Trans. Soc. Rheol. 1972, 16, 99–127. [Google Scholar] [CrossRef]
- Tang, J.; Srinivasan, S.; Yuan, W.; Ming, R.; Liu, Y.; Dai, Z.; Noble, C.O.; Hayes, M.E.; Zheng, N.; Jiang, W.; et al. Development of a flow-through USP 4 apparatus drug release assay for the evaluation of amphotericin B liposome. Eur. J. Pharma. Biopharm. 2019, 134, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Yuan, W.; Kuai, R.; Dai, Z.; Yuan, Y.; Zheng, N.; Jiang, W.; Noble, C.; Hayes, M.; Szoka, F.C.; Schwendeman, A. Development of a Flow-Through USP-4 Apparatus Drug Release Assay to Evaluate Doxorubicin Liposomes. AAPS J. 2017, 19, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Ju, H.L.; Liaw, S.-J. On the assessment of similarity of drug dissolution profiles—A simulation study. Drug Inform. J. Drug Inform. Assoc. 1997, 31, 1273–1289. [Google Scholar] [CrossRef]
- Shah, V.P.; Tsong, Y.; Sathe, P.; Liu, J.-P. In vitro dissolution profile comparison—Statistics and analysis of the similarity factor, f2. Pharm. Res. 1998, 15, 889–896. [Google Scholar] [CrossRef]
- Liu, J.-P.; Ma, M.-C.; Chow, S.-C. Statistical Evaluation of Similarity Factor f2 as a Criterion for Assessment of Similarity Between Dissolution Profiles. Drug Inform. J. 1997, 31, 1255–1271. [Google Scholar] [CrossRef]
- Stevens, R.E.; Gray, V.; Dorantes, A.; Gold, L.; Pham, L. Scientific and Regulatory Standards for Assessing Product Performance Using the Similarity Factor, f2. AAPS J. 2015, 17, 301–306. [Google Scholar] [CrossRef] [Green Version]
- Jansook, P.; Pichayakorn, W.; Muankaew, C.; Loftsson, T. Cyclodextrin-Poloxamer aggregates as nanocarriers in eye drop formulations: Dexamethasone and amphotericin B. Drug Dev. Ind. Pharm. 2016, 42, 1446–1454. [Google Scholar] [CrossRef]
- Nogueiras-Nieto, L.; Alvarez-Lorenzo, C.; Sandez-Macho, I.; Concheiro, A.; Otero-Espinar, F.J. Hydrosoluble Cyclodextrin/Poloxamer Polypseudorotaxanes at the Air/Water Interface, in Bulk Solution, and in the Gel State. J. Phys. Chem. B 2009, 113, 2773–2782. [Google Scholar] [CrossRef]
- Wenz, G.; Han, B.-H.; Müller, A. Cyclodextrin rotaxanes and polyrotaxanes. Chem. Rev. 2006, 106, 782–817. [Google Scholar] [CrossRef]
- Kesavan, K.; Kant, S.; Singh, P.N.; Pandit, J.K. Effect of Hydroxypropyl-β-cyclodextrin on the Ocular Bioavailability of Dexamethasone from a pH-Induced Mucoadhesive Hydrogel. Curr. Eye Res. 2011, 36, 918–929. [Google Scholar] [CrossRef]
- Echezarreta-López, M.; Vila-Jato, J.; Torres-Labandeira, J. The Effects of Cyclodextrins on the Incompatibility Dexamethasone-Polymyxin B in Solution; Springer: Berlin/Heidelberg, Germany, 1996; pp. 457–460. [Google Scholar]
- Liu, X.-M.; Lee, H.-T.; Reinhardt, R.A.; Marky, L.A.; Wang, D. Novel biomineral-binding cyclodextrins for controlled drug delivery in the oral cavity. J. Control. Release 2007, 122, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, W.B.; Daranas, A.H. On the Value of c: Can Low Affinity Systems Be Studied by Isothermal Titration Calorimetry? J. Am. Chem. Soc. 2003, 125, 14859–14866. [Google Scholar] [CrossRef] [PubMed]
- Haimhoffer, Á.; Rusznyák, Á.; Réti-Nagy, K.; Vasvári, G.; Váradi, J.; Vecsernyés, M.; Bácskay, I.; Fehér, P.; Ujhelyi, Z.; Fenyvesi, F. Cyclodextrins in Drug Delivery Systems and Their Effects on Biological Barriers. Sci. Pharm. 2019, 87, 33. [Google Scholar] [CrossRef] [Green Version]
- Mazzaferro, S.; Bouchemal, K.; Gallard, J.-F.; Iorga, B.I.; Cheron, M.; Gueutin, C.; Steinmesse, C.; Ponchel, G. Bivalent sequential binding of docetaxel to methyl-β-cyclodextrin. Int. J. Pharm. 2011, 416, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Pradines, B.; Gallard, J.-F.; Iorga, B.I.; Gueutin, C.; Ponchel, G.; Loiseau, P.M.; Bouchemal, K. The unexpected increase of clotrimazole apparent solubility using randomly methylated β-cyclodextrin: Clotrimazole Solubility Increase. J. Mol. Recognit. 2015, 28, 96–102. [Google Scholar] [CrossRef]
- Mateen, R.; Hoare, T. Carboxymethyl and hydrazide functionalized β-cyclodextrin derivatives: A systematic investigation of complexation behaviours with the model hydrophobic drug dexamethasone. Int. J. Pharm. 2014, 472, 315–326. [Google Scholar] [CrossRef]
- Beig, A.; Agbaria, R.; Dahan, A. Oral Delivery of Lipophilic Drugs: The Tradeoff between Solubility Increase and Permeability Decrease when Using Cyclodextrin-Based Formulations. PLoS ONE 2013, 8, e68237. [Google Scholar] [CrossRef]
- Usayapant, A.; Karara, A.H.; Narurkar, M.M. Effect of 2-hydroxypropyl-β-cyclodextrin on the ocular absorption of dexamethasone and dexamethasone acetate. Pharm. Res. 1991, 8, 1495–1499. [Google Scholar] [CrossRef]
- Castillo, J.; Palomo-Canales, J.; Garcia, J.; Lastres, J.; Bolas, F.; Torrado, J. Preparation and characterization of albendazole β-cyclodextrin complexes. Drug Dev. Ind. Pharm. 1999, 25, 1241–1248. [Google Scholar] [CrossRef]
- Thakur, A.; Kadam, R.S.; Kompella, U.B. Influence of Drug Solubility and Lipophilicity on Transscleral Retinal Delivery of Six Corticosteroids. Drug Metab. Dispos. 2011, 39, 771–781. [Google Scholar] [CrossRef] [Green Version]
- Zoubari, G.; Staufenbiel, S.; Volz, P.; Alexiev, U.; Bodmeier, R. Effect of drug solubility and lipid carrier on drug release from lipid nanoparticles for dermal delivery. Eur. J. Pharm. Biopharm. 2017, 110, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Aka-Any-Grah, A.; Bouchemal, K.; Koffi, A.; Agnely, F.; Zhang, M.; Djabourov, M.; Ponchel, G. Formulation of mucoadhesive vaginal hydrogels insensitive to dilution with vaginal fluids. Eur. J. Pharm. Biopharm. 2010, 76, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.-G.; Lee, M.-K.; Kim, M.-H.; Kim, C.-K. Effect of additives on the physicochemical properties of liquid suppository bases. Int. J. Pharm. 1999, 190, 13–19. [Google Scholar] [CrossRef]
- Ur-Rehman, T.; Tavelin, S.; Gröbner, G. Effect of DMSO on micellization, gelation and drug release profile of Poloxamer 407. Int. J. Pharm. 2010, 394, 92–98. [Google Scholar] [CrossRef] [PubMed]
- Lemdani, K.; Seguin, J.; Lesieur, C.; Al Sabbagh, C.; Doan, B.-T.; Richard, C.; Capron, C.; Malafosse, R.; Boudy, V.; Mignet, N. Mucoadhesive thermosensitive hydrogel for the intra-tumoral delivery of immunomodulatory agents, in vivo evidence of adhesion by means of non-invasive imaging techniques. Int. J. Pharm. 2019, 567, 118421. [Google Scholar] [CrossRef] [PubMed]
- Shama, F.; Sherman, P. Identification of stimuli controlling the sensory evaluation of viscosity II. Oral methods. J. Texture Stud. 1973, 4, 111–118. [Google Scholar] [CrossRef]
- Lejoyeux, F. Evaluation de la Bioadhésion de systemes Matriciels D’acide Polyacrylique: Influence de Paramètres Physicochimiques et Pharmacotechniques. Ph.D. Thesis, University of Paris, Paris, France, 1991. [Google Scholar]
- Ponchel, G.; Touchard, F.; Duchêne, D.; Peppas, N.A. Bioadhesive analysis of controlled-release systems. I. Fracture and interpenetration analysis in poly (acrylic acid)-containing systems. J. Control. Release 1987, 5, 129–141. [Google Scholar] [CrossRef]
- Ritger, P.L.; Peppas, N.A. A simple equation for description of solute release II. Fickian and anomalous release from swellable devices. J. Control. Release 1987, 5, 37–42. [Google Scholar] [CrossRef]
- Ritger, P.L.; Peppas, N.A. A simple equation for description of solute release I. Fickian and non-fickian release from non-swellable devices in the form of slabs, spheres, cylinders or discs. J. Control. Release 1987, 5, 23–36. [Google Scholar] [CrossRef]
- Peppas, N.A.; Sahlin, J.J. A simple equation for the description of solute release. III. Coupling of diffusion and relaxation. Int. J. Pharm. 1989, 57, 169–172. [Google Scholar] [CrossRef]
- Kar, R.; Mohapatra, S.; Bhanja, S.; Das, D.; Barik, B. Formulation and in vitro characterization of xanthan gum-based sustained release matrix tables of isosorbide-5-mononitrate. Iranian J. Pharm. Res. 2010, 9, 13. [Google Scholar]
- Talukdar, M.M.; Plaizier-Vercammen, J. Evaluation of xanthan cum as a hydrophilic matrix for controlled-release dosage form preparations. Drug Dev. Ind. Pharm. 1993, 19, 1037–1046. [Google Scholar] [CrossRef]
- Andreopoulos, A.; Tarantili, P. Xanthan gum as a carrier for controlled release of drugs. J. Biomater. Appl. 2001, 16, 34–46. [Google Scholar] [CrossRef] [PubMed]
- Boddeda, B.; Kumari, P.K.; Chowdary, K. Formulation and evaluation of glipizide sustained release tablets. Int J. Pharm. Biomed. Res. 2012, 3, 44–48. [Google Scholar]
- Lu, M.F.; Woodward, L.; Borodkin, S. Xanthan gum and alginate based controlled release theophylline formulations. Drug Dev. Ind. Pharm. 1991, 17, 1987–2004. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P407 (wt%) | P407/H2O Ratio | H2O (wt%) | HP-β-CD (wt%) | DMA (wt%) | MA Agent | MA (wt%) | Use | |
|---|---|---|---|---|---|---|---|---|
| A | 17.00 | 83.00 | 0.205 | 0 | - | - | - | Physicochemical characterization |
| B | 17.00 | 78.13 | 0.218 | 4.87 | - | - | - | Physicochemical characterization |
| C | 16.17 | 78.96 | 0.205 | 4.87 | - | - | - | Physicochemical characterization |
| D | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | - | - | Physicochemical characterization |
| E | 16.16 | 78.87 | 0.205 | 4.87 | 0.10 | - | - | Physicochemical characterization |
| F | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Carbopol 971P | 0.10 | MA in vitro tests and in vitro dissolution profile |
| G | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Carbopol 971P | 0.50 | MA in vitro tests and in vitro dissolution profile |
| H | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Sodium alginate | 0.10 | MA in vitro tests and in vitro dissolution profile |
| I | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Sodium alginate | 0.50 | MA in vitro tests and in vitro dissolution profile |
| J | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Xanthan Gum | 0.05 | MA in vitro tests and in vitro dissolution profile |
| K | 15.21 | 79.82 | 0.191 | 4.87 | 0.10 | Xanthan Gum | 0.10 | MA in vitro tests and in vitro dissolution profile |
| Without DMA | With DMA | |||||
|---|---|---|---|---|---|---|
| A | B | C | D | E | ||
| HP-β-CD (wt%) | 0 | 4.87 | 4.87 | 4.87 | 4.87 | |
| P407 (wt%) | 17 | 17 | 16.17 | 15.21 | 16.16 | |
| H2O (wt%) | 83.00 | 78.13 | 78.96 | 79.82 | 78.87 | |
| P407/H2O ratio | 0.205 | 0.218 | 0.205 | 0.191 | 0.205 | |
| DMA (wt%) | Ø | Ø | Ø | 0.1 | 0.1 | |
| 20 °C | G′ (Pa) | 0.07 ± 0.08 | 0.35 ± 0.56 | 0.02 ± 0.03 | 0.08 ± 0.08 | 0.05 ± 0.08 |
| G″ (Pa) | 0.23 ± 0.03 | 0.26 ± 0.01 | 0.20 ± 0.01 | 0.17 ± 0.06 | 0.31 ± 0.14 | |
| 37 °C | G′ (Pa) | 12139 ± 329 | 10540 ± 291 | 8052 ± 566 | 3787 ± 960 | 9904 ± 641 |
| G″ (Pa) | 1419 ± 987 | 772 ± 282 | 906 ± 27 | 924 ± 111 | 1001 ± 44 | |
| tan δ at 20 °C | 0.32 ± 0.45 | 1.31 ± 2.06 | 0.08 ± 0.14 | 0.36 ± 0.38 | 0.21 ± 0.37 | |
| tan δ at 37 °C | 11.47 ± 6.58 | 14.79 ± 4.69 | 8.89 ± 0.63 | 4.05 ± 0.60 | 9.89 ± 0.45 | |
| Tsol–gel (°C) | 26.4 ± 0.5 | 28.8 ± 0.0 | 29.7 ± 0.6 | 30.2 ± 0.4 | 27.9 ± 0.6 | |
| Without Mucoadhesive | Mucoadhesive Agents | |||||||
|---|---|---|---|---|---|---|---|---|
| D | F | G | H | I | J | K | ||
| Control sample | Carbopol 971P | Sodium alginate | Xanthan Gum | |||||
| 0.1% | 0.5% | 0.1% | 0.5% | 0.05% | 0.1% | |||
| 20 °C | G′ (Pa) | 0.02 ± 0.02 | 0.03 ± 0.03 | - | 0.08 ± 0.07 | 0.09 ± 0.17 | 0.29 ± 0.02 | 0.61 ± 0.09 |
| G″ (Pa) | 0.25 ± 0.14 | 0.33 ± 0.04 | - | 0.28 ± 0.07 | 0.69 ± 0.18 | 0.45 ± 0.16 | 0.87 ± 0.46 | |
| 37 °C | G′ (Pa) | 3810 ± 385 | 1204 ± 14 | - | 1123 ± 132 | 1198 ± 107 | 1528 ± 99 | 1209 ± 233 |
| G″ (Pa) | 1073 ± 51 | 169 ± 69 | - | 150 ± 6 | 220 ± 36 | 369 ± 44 | 215 ± 79 | |
| tan δ 20 °C | 13.92 ± 3.85 | 10.62 ± 3.60 | - | 3.62 ± 0.12 | 7.13 ± 0.18 | 1.60 ± 0.66 | 1.43 ± 0.70 | |
| tan δ 37 °C | 0.28 ± 0.02 | 0.14 ± 0.06 | - | 0.13 ± 0.01 | 0.18 ± 0.04 | 0.24 ± 0.02 | 0.17 ± 0.03 | |
| Tsol–gel (°C) | 30.5 ± 0.4 | 30.8 ± 0.6 | - | 30.2 ± 0.3 | 31.0 ± 0.2 | 29.7 ± 0.6 | 29.6 ± 0.5 | |
| Sample | Control Sample (D) | F | G | H | I | J | K |
|---|---|---|---|---|---|---|---|
| Mucoadhesive Agent | - b | Carbopol C971P | Sodium Alginate | Xanthan Gum | |||
| Wt% | 0 | 0.1 | 0.5 | 0.1 | 0.5 | 0.05 | 0.1 |
| Fadh (N) | 45.5 ± 1.2 | 42.9 ± 2.9 | ND a | 44.9 ± 2.8 | 53.1 ± 1.1 | 56.6 ± 6.5 | 58.2 ± 0.6 |
| Fm-adh (N) | 60.9 ± 1.5 | 56.5 ± 2.0 | ND a | 79.7 ± 9.0 | 78.8 ± 5.9 | 66.2 ± 3.4 | 71.4 ± 2.9 |
| Wadh (mJ) | 2.2 ± 0.1 | 2.4 ± 0.2 | ND a | 3.4 ± 0.3 | 3.1 ± 0.5 | 2.5 ± 0.2 | 3.3 ± 0.2 |
| Wm-adh (mJ) | 3.7 ± 0.3 | 3.2 ± 0.4 | ND a | 4.4 ± 0.6 | 3.6 ± 0.5 | 3.9 ± 0.3 | 4.6 ± 0.6 |
| Sample | Korsmeyer–Peppas Fitted-Model | Short-Time Korsmeyer–Peppas Fitted-Model | ||||||
|---|---|---|---|---|---|---|---|---|
| Code | MA Agent | [C] | R2 Adjusted | n | K | R2 Adjusted | n | K |
| Control | Ø | - | 0.9953 | 0.015 | 93.5 | ND a | ND a | ND a |
| F | Carbopol | 0.1 | 0.9076 | 0.094 | 69.1 | ND a | ND a | ND a |
| H | Alginate | 0.1 | 0.9818 | 0.055 | 78.8 | ND a | ND a | ND a |
| I | Alginate | 0.5 | 0.9414 | 0.043 | 83.2 | ND a | ND a | ND a |
| J | XG | 0.05 | * | * | * | 0.999 | 0.76 | 7.6 |
| K | XG | 0.10 | * | * | * | 0.999 | 0.69 | 8.8 |
| Code | MA Agent | [C] | Peppas-Sahlin Fitted Model | |||||
|---|---|---|---|---|---|---|---|---|
| Short-Time | Long-Time | |||||||
| K1 | K2 | R2 Adjusted | K1 | K2 | R2 Adjusted | |||
| J | XG | 0.05 | 6.3 | 2.4 | 0.998 | 24.8 | - | 0.965 |
| K | XG | 0.10 | 8.5 | 1.6 | 0.994 | 24.3 | - | 0.992 |
| Sample | Short-Times Drug Release Time (min) | Long-Times Drug Release Time (min) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Code | MA Agent | [C] (wt%) | T25 | T50 | T80 | T90 | T25 | T50 | T80 | T90 |
| J | XG | 0.05 | 4.8 | 12.0 | 21.5 | 24.9 | 4.6 | 9.1 | 24.0 | 35.5 |
| K | XG | 0.10 | 4.5 | 12.7. | 24.6 | 28.8 | 8.3 | 13.0 | 28.6 | 41.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Salmeron, R.; Toussaint, B.; Huang, N.; Bourgeois Ducournau, E.; Alviset, G.; Goulay Dufaÿ, S.; Hillaireau, H.; Dufaÿ Wojcicki, A.; Boudy, V. Mucoadhesive Poloxamer-Based Hydrogels for the Release of HP-β-CD-Complexed Dexamethasone in the Treatment of Buccal Diseases. Pharmaceutics 2021, 13, 117. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13010117
Diaz-Salmeron R, Toussaint B, Huang N, Bourgeois Ducournau E, Alviset G, Goulay Dufaÿ S, Hillaireau H, Dufaÿ Wojcicki A, Boudy V. Mucoadhesive Poloxamer-Based Hydrogels for the Release of HP-β-CD-Complexed Dexamethasone in the Treatment of Buccal Diseases. Pharmaceutics. 2021; 13(1):117. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13010117
Chicago/Turabian StyleDiaz-Salmeron, Raul, Balthazar Toussaint, Nicolas Huang, Etienne Bourgeois Ducournau, Gabriel Alviset, Sophie Goulay Dufaÿ, Hervé Hillaireau, Amélie Dufaÿ Wojcicki, and Vincent Boudy. 2021. "Mucoadhesive Poloxamer-Based Hydrogels for the Release of HP-β-CD-Complexed Dexamethasone in the Treatment of Buccal Diseases" Pharmaceutics 13, no. 1: 117. https://0-doi-org.brum.beds.ac.uk/10.3390/pharmaceutics13010117