Microbiological Testing of Gastric Aspirate Improves the Diagnosis of Pulmonary Tuberculosis in Unconscious Adults with TB Meningitis


Abstract
:1. Introduction
2. Materials and Methods
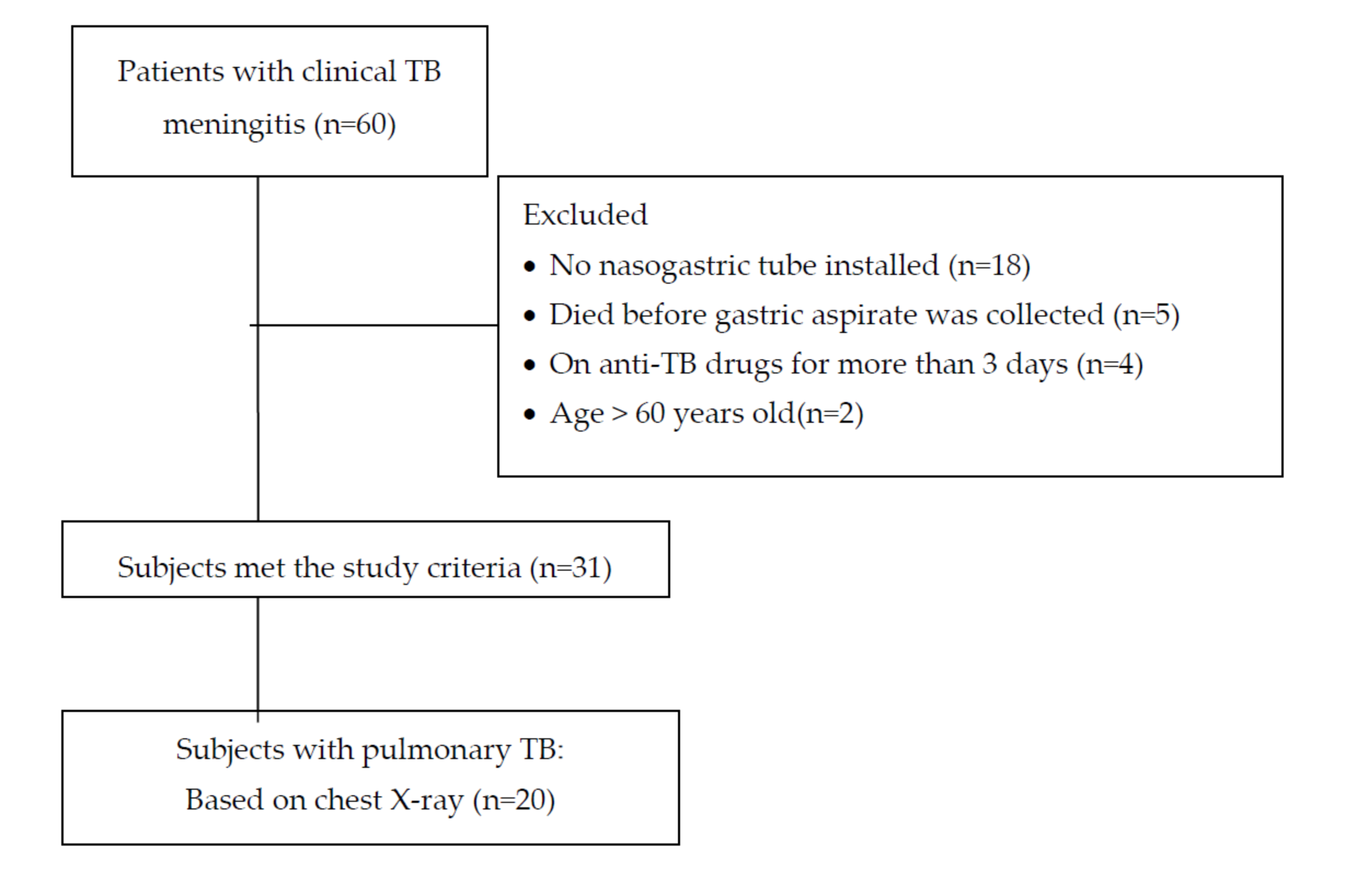
2.1. Patients’ Characteristics and Study Design
2.2. Gastric Lavage
2.3. Sample Processing
2.4. Diagnostic Criteria
2.5. Analysis and Statistics
3. Results
Patient Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zhang, L.; Feng, G.D.; Zhao, G. Tuberculous meningitis in Asia. Neurol. Asia 2015, 20, 1–6. [Google Scholar]
- WHO. WHO Global Tuberculosis Report 2020; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Ganiem, A.; Parwati, I.; Wisaksana, R.; Van Der Zanden, A.; Van De Beek, D.; Sturm, P.; Van Der Ven, A.; Alisjahbana, B.; Brouwer, A.-M.; Kurniani, N.; et al. The effect of HIV infection on adult meningitis in Indonesia: A prospective cohort study. AIDS 2009, 23, 2309–2316. [Google Scholar] [CrossRef] [PubMed]
- Van Laarhoven, A.; Dian, S.; Aguirre-Gamboa, R.; Avila-Pacheco, J.; Ricano-Ponce, I.; Ruesen, C.; Annisa, J.; Koeken, V.A.; Chaidir, L.; Li, Y.; et al. Cerebral tryptophan metabolism and outcome of tuberculous meningitis: An observational cohort study. Lancet Infect. Dis. 2018, 18, 526–535. [Google Scholar] [CrossRef]
- Patkar, D.; Narang, J.; Yanamandala, R.; Lawande, M.; Shah, G.V. Central Nervous System Tuberculosis. Neuroimaging Clin. N. Am. 2012, 22, 677–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marais, S.; Thwaites, G.; Schoeman, J.F.; Török, M.E.; Misra, U.K.; Prasad, K.; Donald, P.R.; Wilkinson, R.J.; Marais, B.J. Tuberculous meningitis: A uniform case definition for use in clinical research. Lancet Infect. Dis. 2010, 10, 803–812. [Google Scholar] [CrossRef]
- Siddiqi, Z.; Siddiqi, M.S.; Fatma, J.; Karoli, R.; Singhal, V.; Gupta, M. Cerebrospinal Fluid Lactate ini Tubercular Meningitis: Diagnostic or Prognostic Marker? J. Assoc. Physician India 2018, 66, 18–21. [Google Scholar]
- Rahbar, M.; Hajia, M. Value of Gastric Lavage for Diagnosis of Pulmonary Tuberculosis. Pak. J. Med. Sci. 2007, 23, 3. [Google Scholar]
- Maciel, E.L.N.; Brotto, L.D.D.A.; Sales, C.M.M.; Zandonade, E.; Sant’Anna, C.C. Gastric lavage in the diagnosis of pulmonary TB in Children. Rev. Saúde Pública 2010, 44, 735–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dian, S.; Hermawan, R.; van Laarhoven, A.; Immaculata, S.; Achmad, T.H.; Ruslami, R.; Anwary, F.; Soetikno, R.D.; Ganiem, A.R.; van Crevel, R. Brain MRI findings in relation to clinical characteristics and outcome of tuberculous meningitis. PLoS ONE 2020, 15, e0241974. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Republic of Indonesia. Sub: Case Definition. Indonesia Tuberculosis Prevalence Survey 2013–2014; Ministry of Health Republic of Indonesia: Jakarta, Indonesia, 2015; p. 37.
- Baghaei, P.; Tabarsi, P.; Farnia, P.; Radaei, A.H.; Kazempour, M.; Faghani, Y.A.; Mirsaeidi, M.; Novin, A.; Chitsaz, E.; Mansouri, D.; et al. Utility of gastric lavage for diagnosis of tuberculosis in patients who are unable to expectorate sputum. J. Glob. Infect. Dis. 2011, 3, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Aslam, W.; Tahseen, S.; Schomotzer, C.; Hussain, A.; Khanzada, F.; Haq, M.U.; Mahmood, N.; Fatima, R.; Qadeer, E.; Heldal, E. Gastric specimens for diagnosing tuberculosis in adults unable to expectorate in Rawalpindi, Pakistan. Public Heal. Action 2017, 7, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Shi, J.; Dong, W.; Ma, Y.; Liang, Q.; Shang, Y.; Wang, F.; Huang, H.; Pang, Y. GeneXpert MTB/RIF Outperforms Mycobacterial Culture in Detecting Mycobacterium tuberculosis from Salivary Sputum. BioMed Res. Int. 2018, 2018, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, M. Comparative Study of GeneXpert with ZN Stain and Culture in Samples of Suspected Pulmonary Tuberculosis. J. Clin. Diagn. Res. 2016, 10, DC09-12. [Google Scholar] [CrossRef] [PubMed]
- Campos, L.C.; Rocha, M.V.V.; Willers, D.M.C.; Silva, D.R. Characteristics of Patients with Smear-Negative Pulmonary Tuberculosis (TB) in a Region with High TB and HIV Prevalence. PLoS ONE 2016, 11, e0147933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kwan, C.K.; Ernst, J.D. HIV and Tuberculosis: A Deadly Human Syndemic. Clin. Microbiol. Rev. 2011, 24, 351–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revendran, J.; Nair, G.; Uppe, A.; Sengal, V.; Sinha, K.; Jain, S. Title: Smear Negative Pulmonary Tuberculosis: Clinico-radiological profile and diagnostic role of bronchoscopy with BAL studies in Indian population. Tuberculosis 2017, 50 (Suppl. S61). [Google Scholar] [CrossRef]


{kind=link}
| General Characteristics | |
| Age in years—median (IQR) | 34 (25–43) |
| Sex | |
| Male | 13 (41.9) |
| Female | 18 (58.1) |
| History of pulmonary TB | 3 (9.7) |
| Positive HIV serology | 3 (9.7) |
| Laboratory examination | |
| Blood test | |
| Serum sodium (mEq/L)—median (IQR) | 129 (123–137) |
| Blood glucose (mg/dL)—median (IQR) | 117 (94–128) |
| CSF | |
| Protein (mg/dL)—median (IQR) | 191.7 (136–327) |
| Cell count (cell/mL)—median (IQR) | 71 (6–195) |
| % lymphocyte—median (IQR) | 81 (56–96) |
| % glucose ratio CSF:serum—median (IQR) | 16.9 (10.4–35.8) |
| Microbiology of gastric aspirate | |
| Positive direct staining | 6 (19.4) |
| Positive culture | 13 (42.0) |
| Positive rapid molecular testing | 15 (48.4) |
| Radiology | |
| Chest X-rays | |
| Not pulmonary TB | 11 (35.5) |
| Abnormal: | |
| -Nonmiliary pulmonary TB | 14 (45.2) |
| -Miliary pulmonary TB | 6 (19.4) |
| Head CT | |
| Communicating hydrocephalus | 10 (32.3) |
| Noncommunicating hydrocephalus | 2 (6.45) |
| Diagnosis | |
| Grade of TB meningitis * | |
| Grade 2 | 30 (96.8) |
| Grade 3 | 1 (3.2) |
| Tuberculous meningitis | |
| Definite | 22 (71.0) |
| Probable | 4 (12.9) |
| Possible | 5 (16.1) |
| Pulmonary TB | |
| Definite | 17 (54.8%) |
| Chest X-rays | Mycobacteriology Result * | |
|---|---|---|
| Positive | Negative | |
| No pulmonary TB (n = 11) | 5 | 6 |
| Nonmiliary pulmonary TB (n = 14) | 7 | 7 |
| Miliary pulmonary TB (n = 6) | 5 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ganiem, A.R.; Djung, L.W.; Chaidir, L.; Gamayani, U. Microbiological Testing of Gastric Aspirate Improves the Diagnosis of Pulmonary Tuberculosis in Unconscious Adults with TB Meningitis. Infect. Dis. Rep. 2020, 12, 134-140. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030025
Ganiem AR, Djung LW, Chaidir L, Gamayani U. Microbiological Testing of Gastric Aspirate Improves the Diagnosis of Pulmonary Tuberculosis in Unconscious Adults with TB Meningitis. Infectious Disease Reports. 2020; 12(3):134-140. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030025
Chicago/Turabian StyleGaniem, Ahmad Rizal, Lilya Wati Djung, Lidya Chaidir, and Uni Gamayani. 2020. "Microbiological Testing of Gastric Aspirate Improves the Diagnosis of Pulmonary Tuberculosis in Unconscious Adults with TB Meningitis" Infectious Disease Reports 12, no. 3: 134-140. https://0-doi-org.brum.beds.ac.uk/10.3390/idr12030025