
Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. VCUG Procedure
2.2.1. Suprapubic Access
- Patient preparation:
- Local topic anesthesia: An EMLA® plaster (local anesthesia containing Lidocain and Prilocain, Aspen Germany GmbH, Munich, Germany)is applied in advance to the suprapubic region by the pediatrician or nursing staff. This helps to reduce pain and discomfort during the procedure.
- Patient preparation:
- The patient is positioned in the supine position on the fluoroscopy table and the plaster is removed.
- The lower abdomen is cleaned and sterilized to minimize the risk of infection.
- Target site identification:
- Ultrasound-guided identification of the optimal puncture site just above the symphysis.
- Needle insertion:
- A sterile needle connected to an extension line (Sterican®, 20 G, 0.90 × 40 mm or 70 mm; Original Perfusor Line®, 3 × 4.1 mm × 100 cm, both: Braun®, Melsungen, Germany) is inserted through the skin and abdominal wall and directed towards the bladder. The angle and depth of insertion are guided by ultrasound imaging to ensure precision.
- Bladder penetration:
- The needle is advanced through the abdominal wall until it penetrates the bladder. This is confirmed by the aspiration of urine into the syringe attached to the needle. The needle is gently secured to the skin with a loosely applied plaster.
- Sample collection:
- Some collected sterile urine is given on a rapid urine test strip to exclude a urinary tract infection at the time of VCUG. If negative, the fluoroscopy procedure is performed. In case of a pathologic urine test strip result, the examination is terminated, the patient is referred to pediatric care for treatment of the infection and VCUG is repeated after recovery.
- Bladder filling:
- Following catheterization, the bladder is fractionally filled with iodine contrast (Imeron 250 or 300, Bracco Imaging Germany GmbH®, Konstanz, Germany) under intermittent fluoroscopy until the age-adjusted bladder capacity is reached.
- Image acquisition:
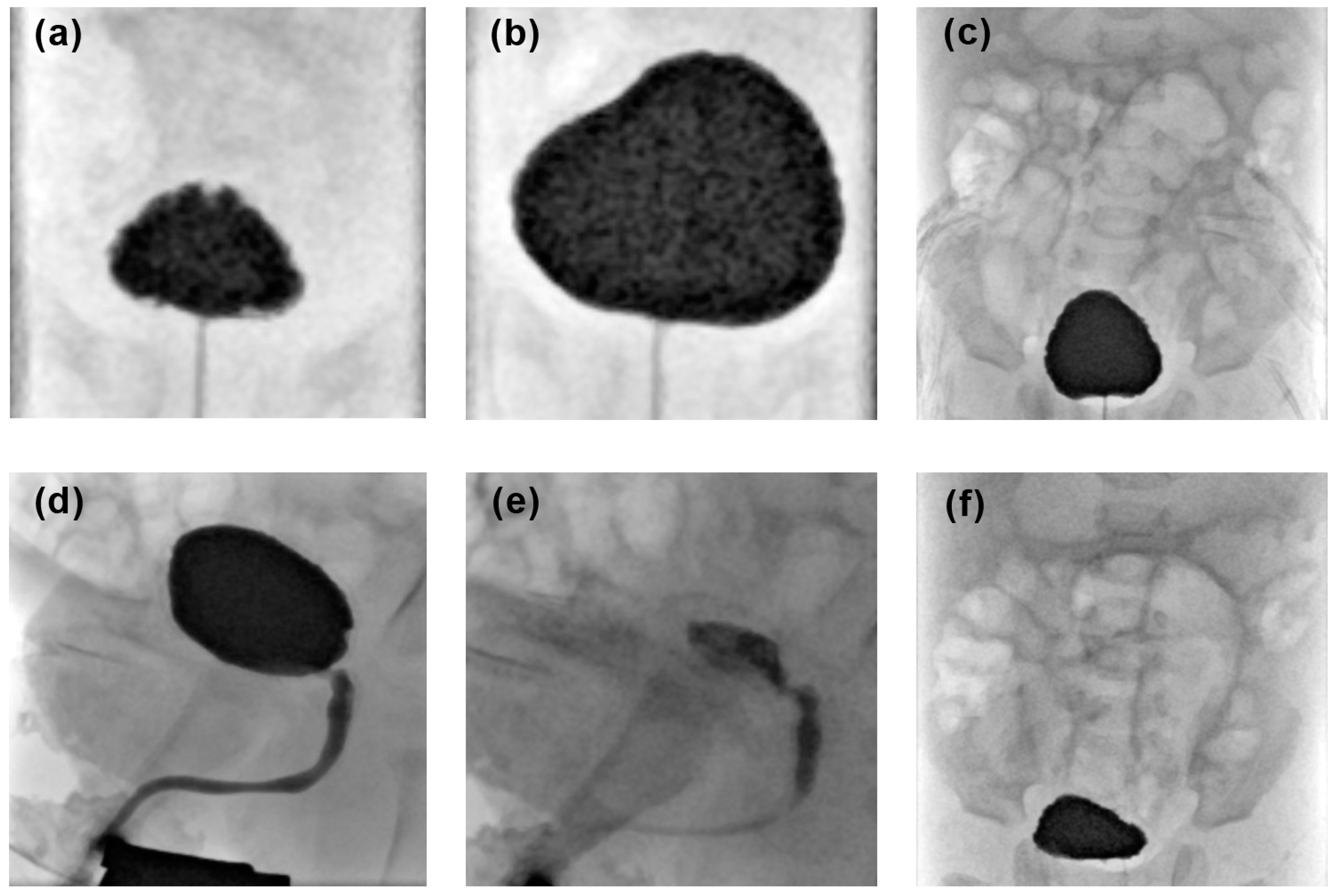
- The following fluoroscopic images are acquired (Figure 1):
- AP bladder projections with low and maximum filling in supine position;
- AP abdominal projection before micturition including the entire renal collective system and the bladder;
- Dynamic imaging during micturition including the bladder and the entire urethra in lateral view;
- AP abdominal projections after micturition including the entire renal collective system and the bladder;
- Additional images can be obtained to document present pathological findings.
- Post-procedure Care:
- The needle is removed and the puncture site is dressed with a sterile bandage to prevent infection.
- The patient may be monitored for any signs of complications, and post-procedural care instructions are provided
2.2.2. Transurethral Catheterization
- Patient preparation:
- The patient is typically positioned on the fluoroscopy table in supine position with legs spread apart.
- The genital area is carefully cleaned and sterilized to minimize the risk of infection.
- Gathering equipment:
- The healthcare provider assembles the necessary equipment, including a catheter catheter (single use catheter for children CH 06/40 or 50 cm, Uromed®, Ostssteinbek, Germany), lubricating gel, antiseptic solution and sterile gloves.
- Gloving:
- The doctor performing the examination uses sterile gloves to maintain aseptic conditions during the procedure.
- Local anesthesia:
- A local anesthetic gel is applied to the urethral opening to reduce discomfort during catheter insertion.
- Catheter insertion:
- The catheter is gently inserted through the urethral opening and advanced into the bladder. In boys, there is often a slight resistance during passage through the pars prostatica.
- Urine drainage:
- Once the catheter reaches the bladder, urine begins to drain.
- Some collected sterile urine is given on a rapid urine test strip to rule out present infection at the time of VCUG. If negative, the fluoroscopy procedure is performed. In the case of a pathologic urine test strip result, the examination is terminated, the patient is referred to pediatric care for treatment of the infection and VCUG is repeated after recovery.
- Catheter securement:
- The catheter is secured in place with a with a loosely applied plaster to prevent accidental dislocation. There is usually no inflating of the small balloon at the catheter’s tip within the bladder.
- Bladder filling and image acquisition is corresponding to points 7 and 8 of the before mentioned suprapubic access.
- During micturition the transurethral catheter is carefully pulled out to obtain perfect overlay-free images of the urethra.
2.3. Examination Parameters
2.3.1. Procedural Switch Rate
2.3.2. Complication Rate
2.3.3. Amount of Contrast Media
2.4. Radiation Parameters
- Fluoroscopy time in seconds
- Radiation dose in µGy·m2
2.5. Examination Quality
- excellent, if all of the abovementioned images were acquired (Figure 1);
- good, if a single projection was missing;
- fair, if two projections were missing;
- non-diagnostic, if more than two abdominal projections were missing or if the lateral voiding phase—a key image series for diagnostic interpretation of VCUG—was missing.
2.6. Statistical Analyses
3. Results
3.1. Examination Parameters
3.1.1. Procedural Switch Rate
3.1.2. Complication Rate
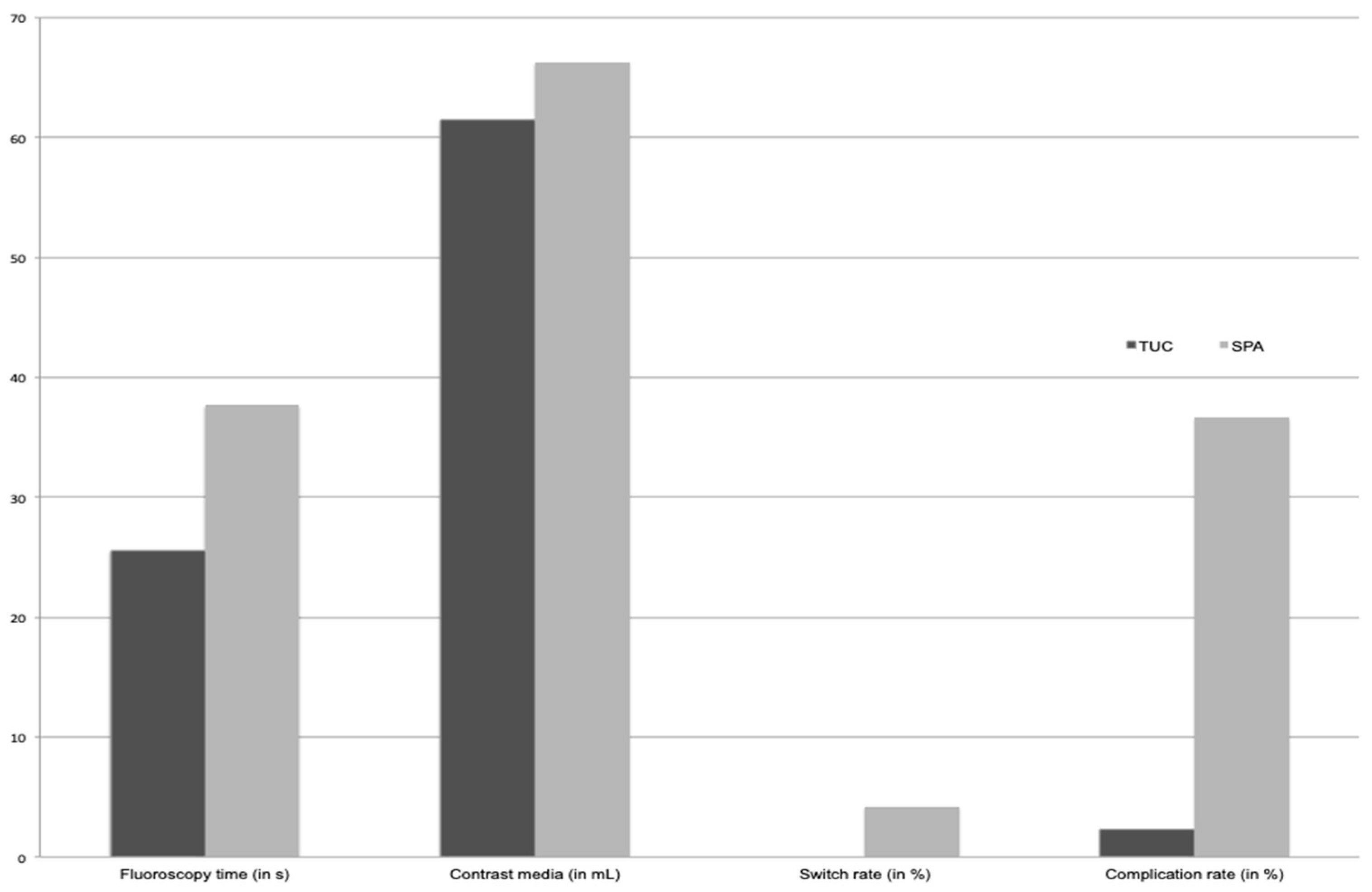
- Minor complications: Due to the access method, prevesical contrast leakage occurs in patients with SPA only and was found in 32 of 98 examinations performed with SPA (32.7%). Premature termination due to patient’s incompliance was necessary in two examinations performed with TUC (0.9%) and in a single examination with SPA (1.0%) (p > 0.05) (Figure 3).
- Major complications: There was no case of bladder perforation. Three patients had a urinary tract infection within 2 days of the VCUG procedure and were admitted to hospital: two after TUC (0.9% of all TUC-VCUG) and one after SPA. Another boy developed a fever shortly after SPA and was admitted to hospital for 3 days but no evidence for urinary tract infection was found (in total 2.0% of all SPA-VCUG) (p > 0.05).
3.1.3. Amount of Contrast Media
3.2. Radiation Parameters
3.3. Examination Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mattoo, T.K. Vesicoureteral reflux and reflux nephropathy. Adv. Chronic Kidney Dis. 2011, 18, 348–354. [Google Scholar] [CrossRef]
- Darge, K. Voiding urosonography with US contrast agent for the diagnosis of vesicoureteric reflux in children: An update. Pediatr. Radiol. 2010, 40, 956–962. [Google Scholar] [CrossRef] [PubMed]
- ‘t Hoen, L.A.; Bogaert, G.; Radmayr, C.; Dogan, H.S.; Nijman, R.J.M.; Quaedackers, J.; Rawashdeh, Y.F.; Silay, M.S.; Tekgul, S.; Bhatt, N.R.; et al. Update of the EAU/ESPU guidelines on urinary tract infections in children. J. Pediatr. Urol. 2021, 17, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Hellerstein, S. Urinary tract infections. Old and new concepts. Pediatr. Clin. N. Am. 1995, 42, 1433–1457. [Google Scholar] [CrossRef] [PubMed]
- Greenfield Sp, W.J. Vesicoureteral reflux: Practical aspects of evaluation and management. Pediatr. Nephrol. 1996, 10, 789–794. [Google Scholar] [CrossRef]
- Johansen, T.E. The role of imaging in urinary tract infections. World J. Urol. 2004, 22, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.; De Souza, A.; Konijeti, R.; Baskin, L.S. The anatomy and embryology of posterior urethral valves. J. Urol. 2006, 175, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, D.; Deshpande, A.V.; Kennedy, S.E. Epidemiology and demography of recently diagnosed cases of posterior urethral valves. Pediatr. Res. 2014, 76, 560–563. [Google Scholar] [CrossRef]
- Levin, T.; Han, B.; Little, B. Congenital anomalies of the male urethra. Pediatr. Radiol. 2007, 37, 851–862. [Google Scholar] [CrossRef]
- Verla, W.; Waterloos, M.; Waterschoot, M.; Van Camp, C.; Lambert, E.; Spinoit, A.F.; Lumen, N. POIROT trial: Post-operative imaging after urethroplasty with peri-catheter retrograde urethrography or trial of voiding with voiding cysto-urethrography. World J. Urol. 2022, 40, 1195–1201. [Google Scholar] [CrossRef]
- Frimberger, D.; Bauer, S.B.; Cain, M.P.; Greenfield, S.P.; Kirsch, A.J.; Ramji, F.; Mercado-Deane, M.G.; Cooper, C.S. Establishing a standard protocol for the voiding cystourethrography. J. Pediatr. Urol. 2016, 138, e20162590. [Google Scholar] [CrossRef]
- Oswald, J.; Riccabona, M.; Lusuardi, L.; Ulmer, H.; Bartsch, G.; Radmayr, C. Voiding cystourethrography using the suprapubic versus transurethral route in infants and children: Results of a prospective pain scale oriented study. J. Urol. 2002, 168, 2586–2589. [Google Scholar] [CrossRef]
- Mohammed, S.H. Suprapubic micturition cystourethrography. Acta Radiol. 1988, 29, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Brandt, M.P.; Goller, J.; Staatz, G.; Allegra, G.R.; Fischer, N.; Haferkamp, A.; Stein, R.; Schroder, A. A comparison of patient and parental experiences and diagnostic quality of suprapubic versus transurethral voiding cystourethrogram in children. Minerva Pediatr. 2022. [Google Scholar] [CrossRef] [PubMed]
- Fairhurst, J.J.; Rubin, C.M.E.; Hyde, I.; Freeman, N.V.; Williams, J.D. Bladder capacity in infants. J. Pediatr. Surg. 1991, 26, 55–57. [Google Scholar] [CrossRef] [PubMed]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 22, 55. [Google Scholar]
- Ward, V.L.; Strauss, K.J.; Barnewolt, C.E.; Zurakowski, D.; Venkatakrishnan, V.; Fahey, F.H.; Lebowitz, R.L.; Taylor, G.A. Pediatric radiation exposure and effective dose reduction during voiding cystourethrography. Radiology 2008, 249, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Roberts, K.B.; Downs, S.M.; Finnell, S.M.E.; Hellerstein, S.; Shortliffe, L.D.; Wald, E.R.; Zerin, J.M. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Pollack, C.V.; Pollack, E.S.; Andrew, M.E. Suprapubic Bladder Aspiration Versus Urethral Catheterization in Ill Infants: Success, Efficiency, and Complication Rates. Ann. Emerg. Med. 1994, 23, 225–230. [Google Scholar] [CrossRef]
- Spencer, J.D.; Bates, C.M.; Mahan, J.D.; Niland, M.L.; Staker, S.R.; Hains, D.S.; Schwaderer, A.L. The accuracy and health risks of a voiding cystourethrogram after a febrile urinary tract infection. J. Pediatr. Urol. 2012, 8, 72–76. [Google Scholar] [CrossRef]
- Johnson, E.K.; Malhotra, N.R.; Shannon, R.; Jacobson, D.L.; Green, J.; Rigsby, C.K.; Holl, J.L.; Cheng, E.Y. Urinary tract infection after voiding cystourethrogram. J. Pediatr. Urol. 2017, 13, 384.e1–384.e7. [Google Scholar] [CrossRef]
- Costa, D.F.G.; Lavallée, L.T.; Dubois, C.; Leonard, M.; Guerra, L. Are we accurately predicting bladder capacity in infants? J. Can. Urol. Assoc. 2014, 8, 329. [Google Scholar] [CrossRef]
- Ward, V.L. Patient dose reduction during voiding cystourethrography. Pediatr. Radiol. 2006, 36, 168–172. [Google Scholar] [CrossRef]
- Tzanis, E.; Raissaki, M.; Konstantinos, A.; Damilakis, J.; Perisinakis, K. Radiation exposure to infants undergoing voiding cystourethrography: The importance of the digital imaging technology. Phys. Med. 2021, 85, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.; Dangle, P.P.; Cannon, G.M.; Schneck, F.X.; Stephany, H.A. Prospective evaluation of radiation dose with conventional fluoroscopic voiding cystourethrogram in pediatric patients. J. Pediatr. Urol. 2021, 17, 790.e1–790.e5. [Google Scholar] [CrossRef] [PubMed]
- Ghodadra, A.; Bartoletti, S. Reducing Radiation Dose in Pediatric Diagnostic Fluoroscopy. J. Am. Coll. Radiol. 2016, 13, 55–58. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Indication | Total (n = 311) | TUC | SPA |
|---|---|---|---|
| Hydronephrosis | 132 | 94 (=71.2%) | 38 (=28.8%) |
| Urinary tract infection with fever | 115 | 83 (=72.2%) | 32 (=27.8%) |
| Micturition disorder | 12 | 7 (=58.3%) | 5 (=41.7%) |
| Renal malformation | 36 | 26 (=72.2%) | 10 (=27.8%) |
| Postoperative control | 10 | 2 (=20%) | 8 (=80%) |
| Others (e.g., post-traumatic) | 6 | 1 (=16.7%) | 5 (=83.3%) |
| TUC | SPA | p-Value | |
|---|---|---|---|
| Total no. of examinations = 311 | 213 | 98 | |
| Age | |||
| mean ± SD (yrs) | 1.45 ± 2.35 | 2.46 ± 3.12 | <0.01 |
| Periprocedural Switch Rate | From SPA to TUC: n = 9 (9%) | ||
| Complication rate: | 4 (1.9%) | 35 (35.7%) | <0.001 |
| Major | 2 (0.9%) | 2 (2.0%) | >0.05 |
| Minor | 2 (0.9%) | 33 (33.7%) | <0.001 |
| Prevesical leakage | - | 32 (32.6%) | |
| Premature termination of VCUG procedure | 2 (0.9%) | 1 (1.0%) | >0.05 |
| Examination parameters: | |||
| Radiation dose ± SD (µGy·m2) | 0.6 ± 1.2 | 1.7 ± 2.9 | <0.001 |
| Contrast media amount (mL) | 61.5 ± 39.9 | 66.3 ± 41.3 | >0.05 |
| Fluoroscopy time (s) | 25.6 ± 19.4 | 37.7 ± 33.1 | <0.01 |
| Examination quality | |||
| 121 (56.8%) | 44 (44.9%) | >0.05 |
| 68 (31.9%) | 42 (42.8%) | >0.05 |
| 6 (2.81%) | 6 (6.1%) | >0.05 |
| 18 (8.4%) | 6 (6.1%) | >0.05 |
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Occurrence of complications | 0.958 | 0.125–0.479 | <0.001 | 1.004 | 1.000–1.006 | 0.0001 |
| Fluoroscopy time | 0.978 | 0.972–0.991 | <0.05 | 0.984 | 0.973–0.9945 | 0.04 |
| Age | 0.992 | 0.818–0.972 | 0.09 | |||
| Contrast media amount | 0.998 | 0.992–1.004 | 0.45 | |||
| Radiation dose | 0.995 | 0.958–1.040 | 0.78 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schlötelburg, W.; Benoit, C.; Kasper, M.; Petritsch, B.; Weng, A.M.; Bley, T.A.; Veldhoen, S. Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients. Pediatr. Rep. 2024, 16, 190-200. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16010017
Schlötelburg W, Benoit C, Kasper M, Petritsch B, Weng AM, Bley TA, Veldhoen S. Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients. Pediatric Reports. 2024; 16(1):190-200. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16010017
Chicago/Turabian StyleSchlötelburg, Wiebke, Clemens Benoit, Mandy Kasper, Bernhard Petritsch, Andreas Max Weng, Thorsten Alexander Bley, and Simon Veldhoen. 2024. "Suprapubic and Transurethral Bladder Access for Voiding Cystourethrography in Pediatric Male Patients" Pediatric Reports 16, no. 1: 190-200. https://0-doi-org.brum.beds.ac.uk/10.3390/pediatric16010017