Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
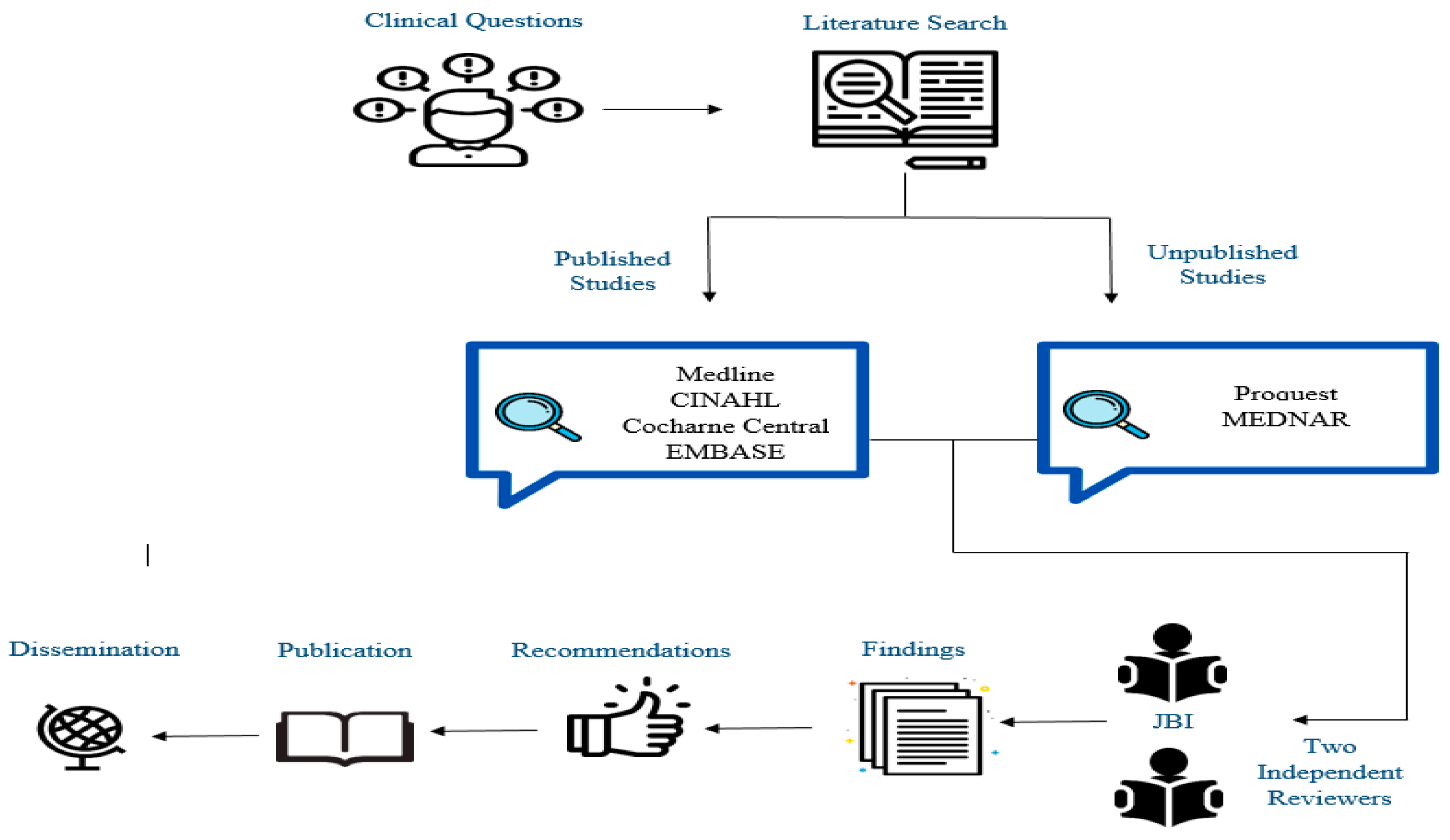
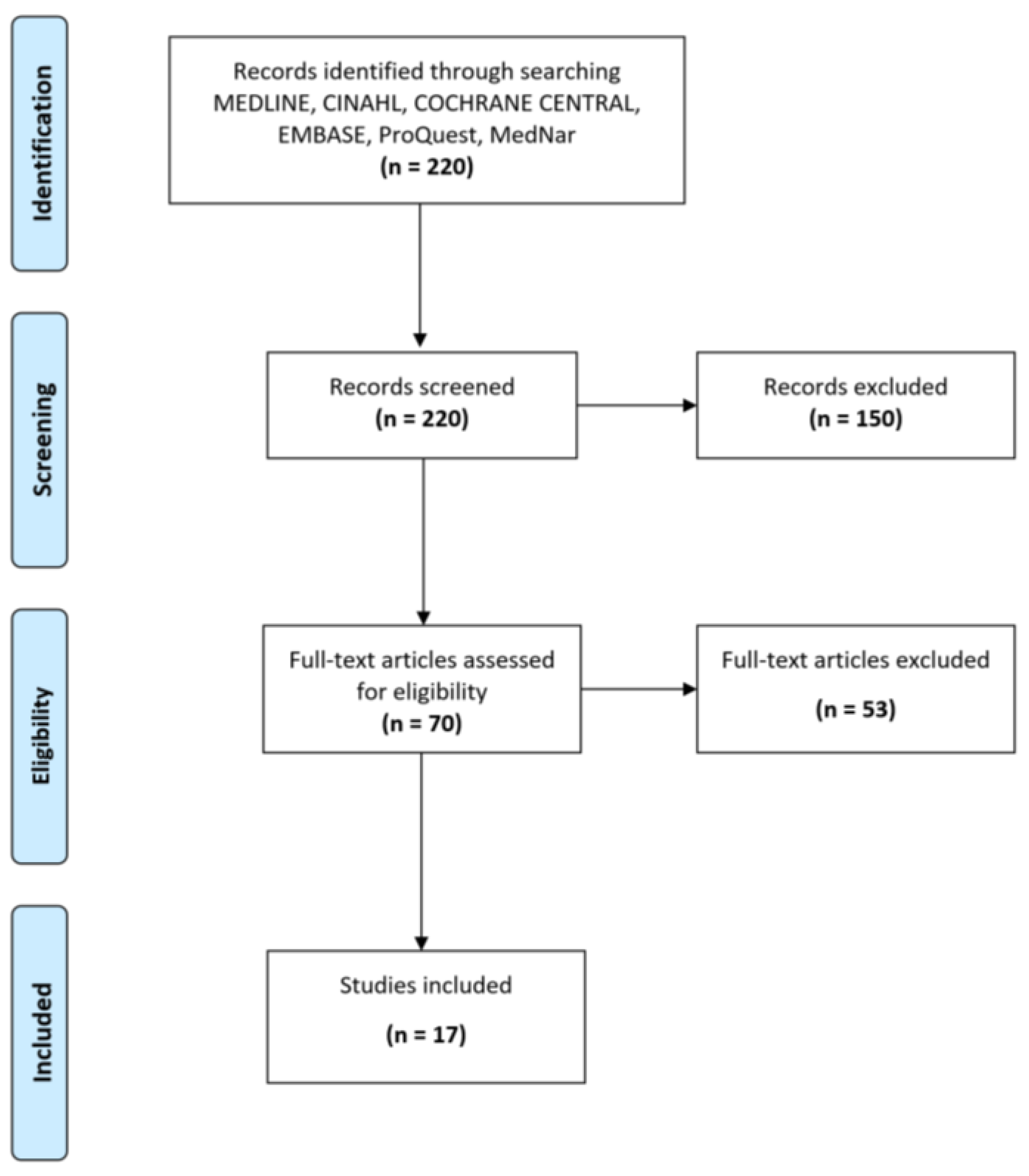
2. Methods
2.1. Data Sources
2.2. Quality Assessment of Extracted Data
3. Strategies to Meet Nursing Surge Capacity during the COVID-19 Pandemic
3.1. Recommendation 1: Regular Patient-to-Nurse Ratio
Rationale
3.2. Recommendation 2: Finding Alternate Staff from Internal and External Resources to Support ICU Staff during Crisis Time
Rationale
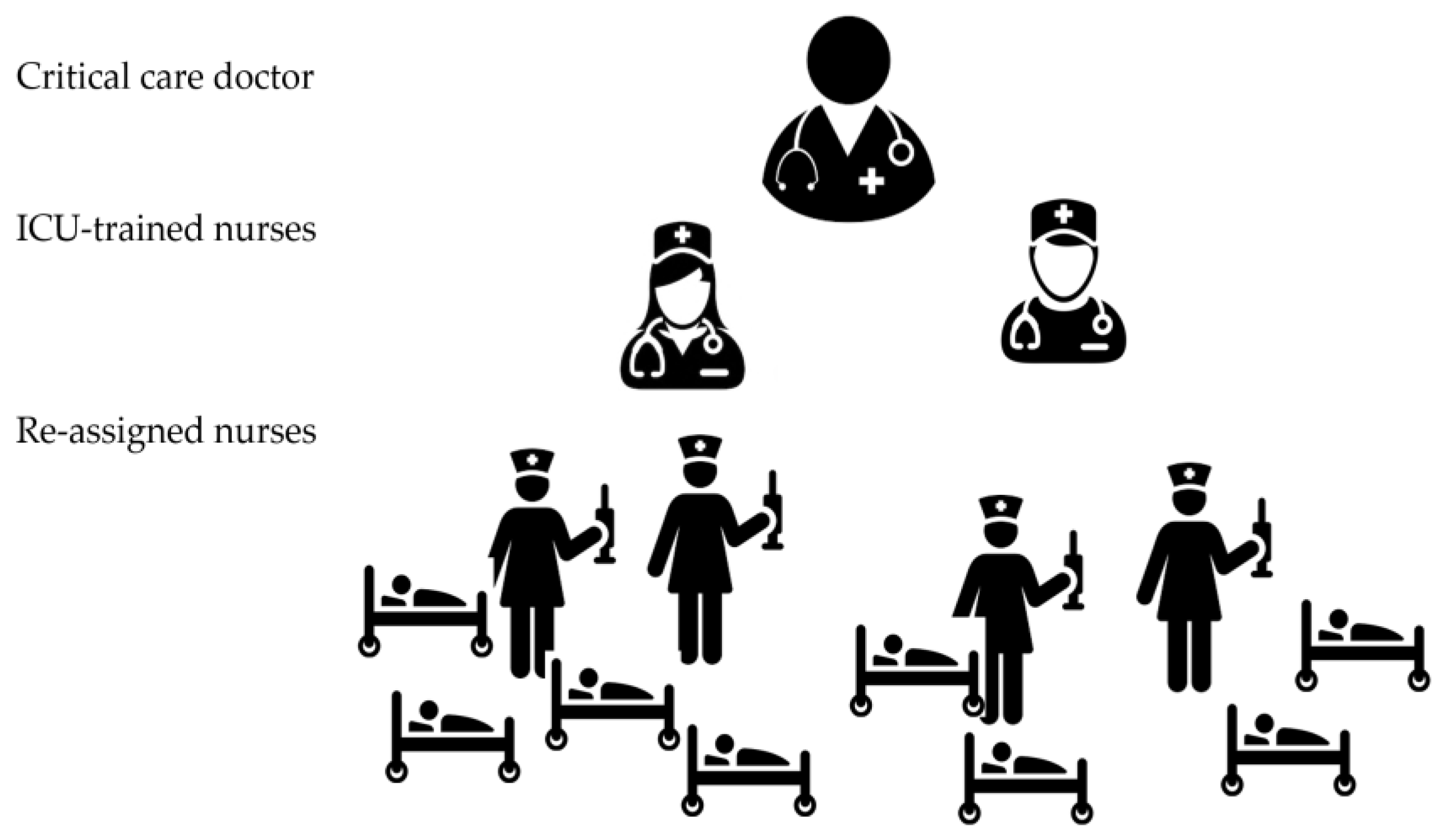
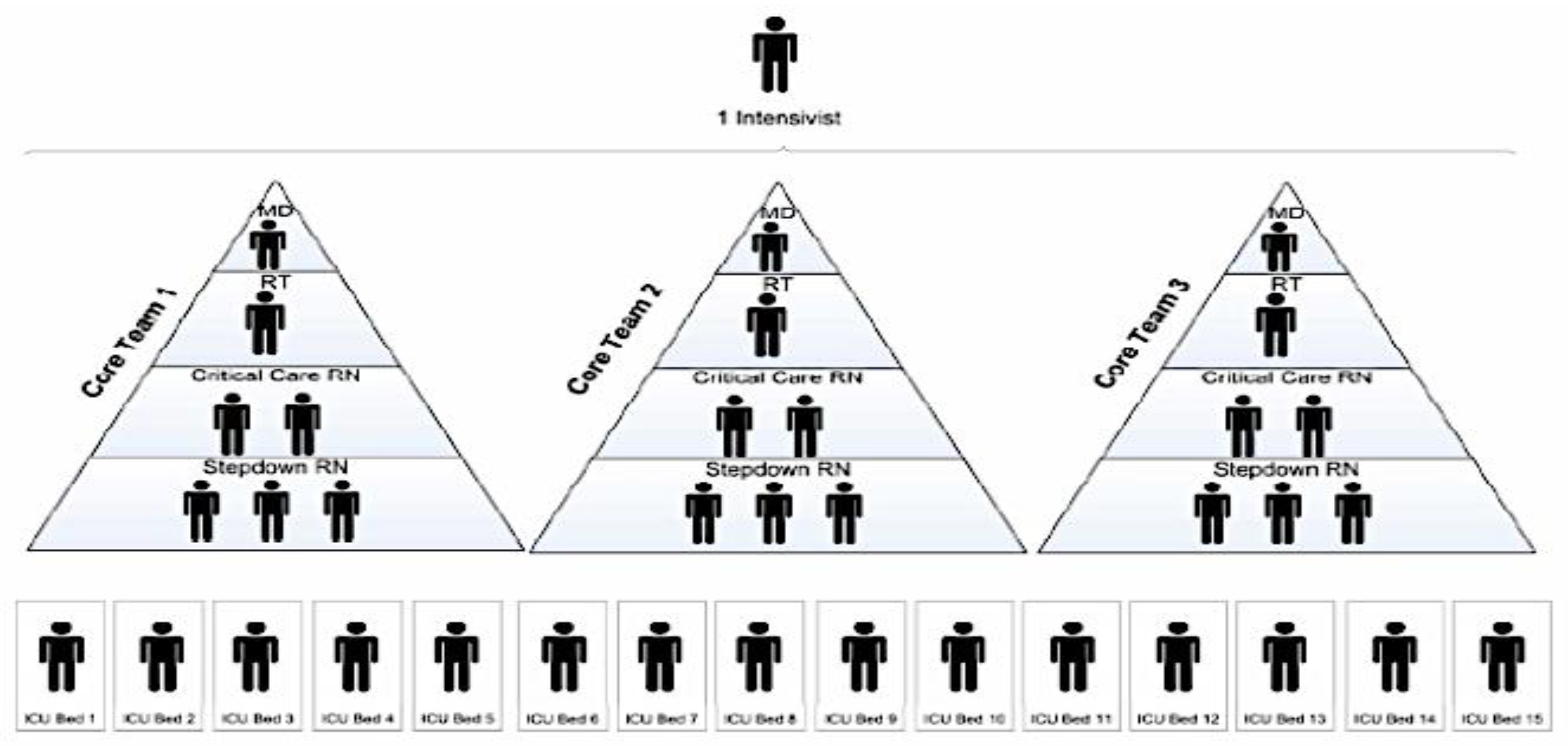
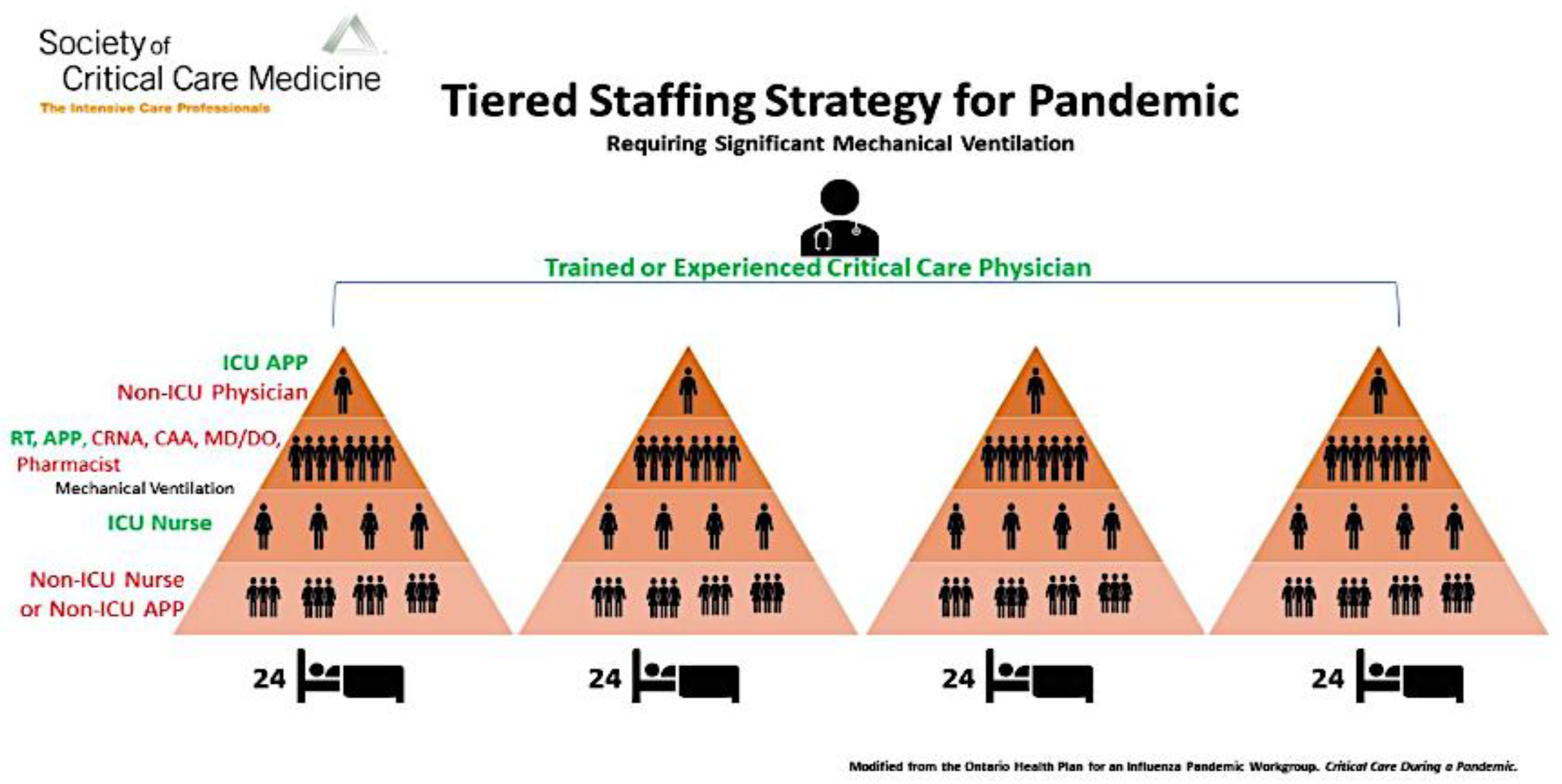
3.3. Recommendation 3: Implement a Team-Based Approach (Tiered Staffing Strategy or Care Team Model) to Manage Critically Ill Patients
3.3.1. Rationale
3.3.2. Applications of a Team-Based Approach
3.4. Recommendation 4: Training Model for ICU Tiered Staffing Strategy for COVID-19 Pandemic
Rationale
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alhazzani, W.; Al-Suwaidan, F.; Al Aseri, Z.; Al Mutair, A.; Alghamdi, G.; Rabaan, A.; Algamdi, M.; Alohali, A.; Asiri, A.; Alshahrani, M.; et al. The saudi critical care society clinical practice guidelines on the management of COVID-19 patients in the intensive care unit. Saudi Crit. Care J. 2020, 4, 27–44. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Livingston, E.; Bucher, K. Coronavirus disease 2019 (COVID-19) in Italy. JAMA 2020, 323, 1335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Milton, D.K.; Fabian, M.P.; Cowling, B.J.; Grantham, M.L.; McDevitt, J.J. Influenza virus aerosols in human exhaled breath: Particle size, culturability, and effect of surgical masks. PLoS Pathog. 2013, 9, e1003205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Corona Virus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 13 July 2020).
- World Health Organization. Rational Use of Personal Protective Equipment for Coronavirus Disease 2019 (COVID-19) Interim Guidance 27 February 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/331215/WHO-2019-nCov-IPCPPE_use-2020.1-eng.pdf (accessed on 5 April 2020).
- World Health Organization. Coronavirus. Available online: https://www.who.int/health-topics/coronavirus#tab=tab_1 (accessed on 16 July 2020).
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; Chu, D.K.; Akl, E.A.; El-harakeh, A.; Bognanni, A.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- World Health Organization. Advice on the Use of Masks in the Context of COVID-19. Available online: https://www.who.int/publications/i/item/advice-on-the-use-of-masks-in-the-community-during-home-care-and-in-healthcare-settings-in-the-context-of-the-novel-coronavirus-(2019-ncov)-outbreak (accessed on 7 September 2020).
- Society of Critical Care Medicine. United States Resource Availability for COVID-19. Available online: https://sccm.org/getattachment/Blog/March-2020/United-States-Resource-Availability-for-COVID-19/United-States-Resource-Availability-for-COVID-19.pdf?lang=en-US (accessed on 7 September 2020).
- Aragon Penoyer, D. Nurse staffing and patient outcomes in critical care: A concise review. Crit. Care Med. 2010, 38, 15211528. [Google Scholar] [CrossRef] [PubMed]
- Ontario Health Plan for an Influenza Pandemic Care. Critical Care During a Pandemic. Available online: http://www.cidrap.umn.edu/sites/default/files/public/php/21/21_report.pdf (accessed on 7 September 2020).
- Maves, R.C.; Downar, J.; Dichter, J.R.; Hick, J.L.; Devereaux, A.; Geiling, J.A.; Kissoon, N.; Hupert, N.; Niven, A.S.; King, M.A.; et al. Triage of scarce critical care resources in COVID-19—An implementation guide for regional allocation: An expert panel report of the task force for mass critical care and the American College of Chest Physicians. Chest 2020, 158, 212–225. [Google Scholar] [CrossRef]
- Chung, W.; Sohn, M. The impact of nurse staffing on in-hospital mortality of stroke patients in Korea. J. Cardiovasc. Nurs. 2018, 33, 47–54. [Google Scholar] [CrossRef] [PubMed]
- The University of Toronto Interdepartmental Division of Critical Care Medicine Working Group. Management Principles of Adult Critically Ill COVID-19 Patients. Available online: https://criticalcare.utoronto.ca/file/180/download?token=E8_KA4WU (accessed on 23 March 2020).
- Murthy, S.; Gomersall, C.D.; Fowler, R.A. Care for critically Ill patients with COVID-19. JAMA 2020, 323, 1499–1500. [Google Scholar] [CrossRef] [Green Version]
- Ajao, A.; Nystrom, S.V.; Koonin, L.M.; Patel, A.; Howell, D.R.; Baccam, P.; Lant, T.; Malatino, E.; Chamberlin, M.; Meltzer, M.I. Assessing the capacity of the US health care system to use additional mechanical ventilators during a large-scale public health emergency. Disaster Med. Pub. Health Prep. 2015, 9, 634–641. [Google Scholar] [CrossRef]
- Kleinpell, R.M.; Grabenkort, W.R.; Kapu, A.N.; Constantine, R.; Sicoutris, C. Nurse practitioners and physician assistants in acute and critical care: A concise review of the literature and data 2008–2018. Crit. Care Med. 2019, 47, 1442–1449. [Google Scholar] [CrossRef] [Green Version]
- McHugh, M.D.; Ma, C. Hospital nursing and 30-day readmissions among medicare patients with heart failure, acute myocardial infarction, and pneumonia. Med. Care 2013, 51, 52–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, E.; Chin, D.L.; Kim, S.; Hong, O. The relationships of nurse staffing level and work environment with patient adverse events. J. Nurs. Scholarsh. 2016, 48, 74–82. [Google Scholar] [CrossRef] [PubMed]
- American College of Chest Physicians. Surge Priority Planning COVID-19: Critical Care Staffing and Nursing Considerations. Available online: http://www.chestnet.org/Guidelines-and-Resources/Resources/Surge-Priority-Planning-COVID-19-Critical-Care-Staffing-and-Nursing-Considerations (accessed on 7 September 2020).
- Scott, D.; Irfan, U.; Kirby, J. The Next Coronavirus Crisis Will Be A Shortage of Doctors and Nurses. Available online: https://www.vox.com/2020/3/26/21192191/coronavirus-us-new-york-hospitals-doctors-nurses (accessed on 29 March 2020).
- Society of Critical Care Medicine. Critical Care Statistics. Available online: https://www.sccm.org/Communications/Critical-Care-Statistics (accessed on 7 September 2020).
- Driscoll, A.; Grant, M.J.; Carroll, D.; Dalton, S.; Deaton, C.; Jones, I.; Lehwaldt, D.; McKee, G.; Munyombwe, T.; Astin, F. The effect of nurse-to-patient ratios on nurse-sensitive patient outcomes in acute specialist units: A systematic review and meta-analysis. Eur. J. Cardiovasc. Nurs. 2017, 17, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Kleinpell, R.M. ICU workforce: Revisiting nurse staffing. Crit. Care Med. 2014, 42, 1291–1292. [Google Scholar] [CrossRef] [PubMed]
- North Carolina Healthcare Foundation. Strategies to Support Nursing Surge Capacity during Biological Event. Available online: https://www.ncbon.com/vdownloads/coronavirus/nursing-surge-capacity-resource.pdf (accessed on 20 July 2020).







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Mutair, A.; Amr, A.; Ambani, Z.; Salman, K.A.; Schwebius, D. Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19. Nurs. Rep. 2020, 10, 23-32. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep10010004
Al Mutair A, Amr A, Ambani Z, Salman KA, Schwebius D. Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19. Nursing Reports. 2020; 10(1):23-32. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep10010004
Chicago/Turabian StyleAl Mutair, Abbas, Anas Amr, Zainab Ambani, Khulud Al Salman, and Deborah Schwebius. 2020. "Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19" Nursing Reports 10, no. 1: 23-32. https://0-doi-org.brum.beds.ac.uk/10.3390/nursrep10010004