1. Introduction
The World Health Organization defines health as the condition of full physical, mental, and social wellbeing, not as a mere absence of a disorder or disease. The right to health improvement, protection, and renewal is one of the fundamental human rights. Every man, regardless of race, religion, political orientation, economic, and social status, has the right to enjoyment of the highest achievable health standard and quality. Health care and protection is one of the fundamental human rights that apply to all people of the world [
1]. Life and health threats can occur at any place and time. Addressing an event including a threat to life and/or health of the population requires provision of urgent medical assistance, which needs deployment of the needed means and resources in the right place, time, quantity, and quality and at a reasonable cost.
This area is in the center of attention of individual countries and the professional public for the reason of protection of man in case of any incident, including traffic accidents. The individual areas related to the issue of interest are discussed in literature, including the area of health protection management [
2], means, and resource utilization planning [
3], and the use of medical care equipment is discussed by WHO [
4]. Mathematical models of spatial distribution of emergency medical care stations are published, for example, by [
5] and others.
The Slovak Republic pays appropriate attention to rescue of men in need. The medical rescue service (MRS) was established and is operated to provide emergency medical care to individuals in critical health condition, under immediate threat to life or serious health threat, and to address health issues connected with other emergencies [
6].
In compliance with [
7], MRS is provided by Operation Centers of Emergency Calls of MRS of the Slovak Republic and Healthcare Providers on the basis of certification by the Ministry of Health of the Slovak Republic for operation of MRS ambulances.
Healthcare providers are the basic rescue component of the integrated rescue system providing MRS in the area of emergency occurrence. They operate MRS stations including each a stationary center (building) and MRS ambulances (mobile means—vehicles or helicopters—adapted for transport of at least one person in a critical condition). The stationary center of MRS is a particular location defined by the relevant legislative decree of the Ministry of Health. The stationary center of MRS is occupied by a standby MRS team (including at least two medical rescue service providers), equipped with communication means, and operates 24 h a day, being in permanent connection with the Regional Operation Centre of MRS sending the medical rescue teams to the places of emergencies. The MRS team members do not directly receive emergency calls from legal entities of natural persons in need of medical rescue service, but are sent to the place of emergency by their sending MRS station, receiving these calls.
The requirements for material and technological and human resource equipment of MRS stations are directly defined in [
8] and follow from their primary mission to provide emergency medical care and assure primary and/or secondary transport of the persons under threat [
8].
The medical rescue service is a public service system with equal availability for inhabitants of all municipalities in need of urgent medical care for a sudden attack of a disease or for injury, whether in a peaceful and secure or emergency condition (including traffic accident). In the case of an emergency condition, the situation may be complicated by the emergency itself, including problems with non-negotiable road sections complicating the access of medical rescue service ambulance vehicles. As ambulances, MRS use as vehicles specially adapted Mercedes, Renault, Fiat, and Iveco types, which are equipped according to (SK, 2014) for the provision of healthcare with medical equipment from Braun, Dräger, Ferno, Leardal, PhysioControl, and Spencer. The factors affecting safety of MRS ambulances (vehicles) are addressed in detail, with use of cause and consequence diagrams. The activities and successful functioning of MRS stations, together forming an MRS network, require legal, organizational, material and technological, human resource, and financial background, within the responsibility of the certified healthcare providers. These factors, including the roles and activities of MRS, have been addressed by various authors, such as [
9,
10,
11], etc.
The purpose of the present article is to assess the current status of MRS and propose the optimum number of MRS stations for successfully addressing emergencies in the Žilina Self-Governing Region with an emphasis on provision of urgent medical care to large numbers of victims of extensive emergencies. The Self-Governing Region of Žilina is situated in the north of Slovakia. Its area of 6809 km2 is inhabited by 696,778 people living in 296 municipal units, making a population density of 101.4 persons/km2.
Location tasks [
12,
13,
14,
15,
16] can help optimize means and resources of MRS with an emphasis on quick provision of urgent medical care to the sufficient number of injured victims or a large emergency. A similar issue has been discussed for the Slovak Republic under different angles by several authors, for example [
17,
18,
19].
2. Materials and Methods
Addressing the individual issues connected with implementation of the main objective was based on information obtained from generally accessible media resources, by study of collected materials and consultations with MRS experts, transport providers, and members of the Police Corps of the Slovak Republic. Evaluation of the current status in the area of interest made use of the following logical methods: deduction and induction and definitions of basic notions and relations needed for understanding the MRS system, analysis of applicable legislation concerning MRS, investigation of properties of the MRS transport system and revealing its substantial features, synthesis of the individual components of MRS description, comparison of MRS in individual areas of the Žilina Self-Governing Region, and selection of methods to be used. The location task method was applied too.
As of 1 January 2019, there were 13 MRS providers in Slovakia, operating various types of mobile MRS ambulances from MRS stations. The MRS network was made of 280 stationary MRS centers with 24/7 operation across the Slovak Republic [
20,
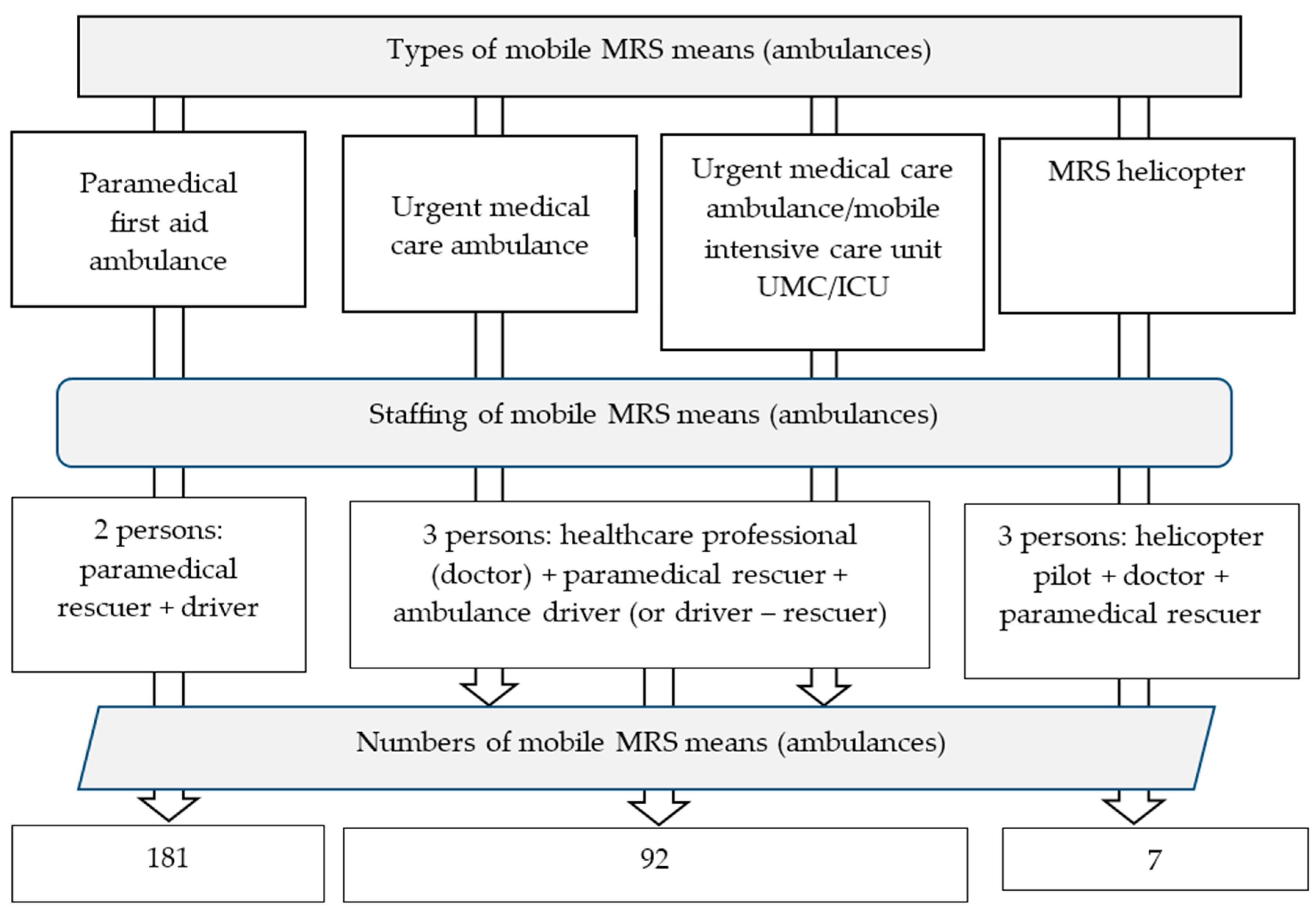
21]. One MRS ambulance provides urgent medical care to more than 19.4 thousand inhabitants of Slovakia on average. The types of mobile MRS means (ambulances) [
3], their numbers, and staffing are shown in
Figure 1.
At present, the most important providers of MRS can be included, for example, Life Star Emergency, s.r.o., Rescue Medical Service Košice, Rescue Medical Service Bratislava, etc.
At present, the number of stationary emergency medical services is the same. There are 92 urgent medical care ambulances, 181 paramedical first aid ambulances, and seven MRS helicopters in continuous operation. This number should be increased by 48 MRS vehicles type “S”.
The starting point of the optimization was availability of urgent medical care to the population within a defined time. The time to arrival of a MRS ambulance from a stationary MRS center to a person in need caused by an emergency was defined as the maximum permitted. The calculation based on this maximum time considered its increase/decrease. The location was based on a quantity of candidates. The candidates included every municipality characterized by its population. Locations of MRS stations were considered inside the municipalities. The optimization of MRS station numbers also considered the level of risk of emergency occurrence.
Further appropriate conditions (for example that one MRS ambulance can serve maximum 25,000 people, and every person must be secured with a backup coverage—i.e., by at least two available ambulances) were selected, defined, and formulated for the purpose of addressing the optimum distribution of stationary MRS centers.
The purpose of the addressed location task was to reach, with the help of the software tool XPRESS-IVE, the optimum distribution of MRS stations in the municipalities within the area of interest [
13], with the aim to be able to provide medical first aid within 15 min at each location and to form a proposal of a MRS station network assuring higher-standard response to emergencies. The application of the MRS station number optimization was performed for the model locality of the Žilina Self-Governing Region.
The software tool XPRESS IVE is generally used for addressing various complicated optimization issues. The tool includes [
17]:
A resolution algorithm (solver),
A module for entering the mathematical model of the given task (modeler),
A module including means for fine tuning of syntactic errors in the model entry.
The advantages of XPRESS IVE include management of the computation process, for example termination of the search of the quantity of the acceptable solutions after the elapse of a defined time. Its disadvantages include the need to write the mathematical model in Mosel language.
The multi-criteria decision using the Expert choice software is used for specification of the value of the individual criteria and sub-criteria on the basis of which priority municipalities for establishment of stationary MRS centers were selected in our case.
The optimization of the number of MRS stations was addressed as a location issue. The location issue, together with transport and allocation issues, is part of the special category of linear programming, represented by distribution issues. Possible methods of addressing location issues include tasks within public service systems. The essence of these tasks is the need for equal accessibility of emergency medical care for every citizen of the Slovak Republic. The outcome is represented by a proposal of the optimum distribution of MRS stations (means and resources of MRS) as the source of addressing emergency medical assistance in case of emergencies that may result in a larger number of injured victims.
The tasks addressing the proposal of the optimum structure of the public service systems, also usable for addressing the optimum distribution of MRS stations, include:
Location Set Covering Problem (LSCP),
Maximal Covering Location Problem (MCLP),
Maximal Backup Covering Location Problem (MBCLP). [
17]
Application of the location task for a solution uses special effective algorithms, considering specifics of mathematical models of the individual types of tasks. Every mathematical model is defined by a purpose, function, and limiting conditions.
In the case of the LSCP type task, the general objective of the purpose-defined function is to minimize the number of stations needed for coverage of every client by at least one center, within the maximum distance defined by Tmax. In the case of the solution of the optimum distribution of the means and resources for MRS, the purpose-defined function focuses on distribution of the minimum number of the stationary MRS sites for every inhabitant of every municipality of the Žilina Self-Governing Region to be secured with emergency medical care provision within 15 min from its need reporting. When preparing the proposal for the network of MRS stations, the economic side of the task must also be considered, i.e., the costs of establishment of an individual MRS station.
The purpose-defined function in the case of a LSCP type task focuses on minimization of the costs connected with MRS station building. Every possible built stationary MRS site
i ∈ I (“I” representing the quantity of all candidate municipalities where a MRS station can be built, and “
i” representing an element of the quantity) is evaluated by the “
fi” constant, representing the amount of costs of its building. The municipalities for which emergency medical care needs to be provided form the final quantity “J”. The distances, defined by times of response to emergency, between potential locations of MRS stations and the individual municipalities to be served by them, are defined by the matrix
tij (
i ∈ I,
j ∈ J). The decision whether a MRS station will be built or not is expressed in the model by the bivalent variable “
yi”. If the stationary site is decided to be built, then
yi = 1, if not then
yi = 0. The matrix “
aij“ expresses coverage of a municipality
j ∈ J (
tij ≤ 15) by a MRS station
i ∈ I, if covered, then
aij = 1, if not then
aij = 0 [
17].
Table 1 shows the mathematical model of such a task.
The purpose of the MCLP task applied to the issue of interest lies in maximization of the number of covered clients (inhabitants) with regard to the number of MRS stations that need to be located. Maximization however does not require 100% coverage of all clients. From the economical point of view, the purpose of the MCLP task solution is to assure the acceptable price of the solution.
When addressing the issue of distribution of the MRS stations the inputs must include the number of MRS stations that need to be distributed with the aim to provide emergency medical care within 15 min from its need reporting to the maximum possible number of inhabitants of the Self-Governing Region of Žilina. The aim of the purpose-defined function is to maximize the number of inhabitants covered by the emergency medical care within 15 min.
Table 2 shows the mathematical expression of the MCLP task focused on the network of MRS stations.
Variable “
oj” represents the populations of the individual municipalities. The number of MRS stations that need to be built considering the defined conditions is marked “
p”. If a MRS station is built in a municipality, then
yi = 1, otherwise
yi = 0. The “
zj” variable is coverage identifier; if
zj = 1, then municipality
jJ is covered with emergency medical care provision by MRS. The quantity “
Nj” represents possible locations of MRS stations providing urgent medical care with the help of MRS ambulances within T
max minutes.
The third variant of addressing MRS station locations is application of the MBCLP task focused on locations of multiple MRS stations in one place. Addressing the transport aspect of MRS considers locations of multiple MRS stations in a single municipality. The mathematical model of the MBCLP task is shown by
Table 3.
The task model is nearly identical to the MCLP task. The oj variable represents the populations of the individual municipalities and the P variable the number of MRS stations to be built to meet the defined conditions. To apply the MBCLP task, the 1st limiting conditions of the MCLP task must be changed. The following applies to the coverage variable zj: if zj = 1, the municipality in question is covered with at least two MRS stations, otherwise zj = 0.
The proposed computation methodology, applied to the Self-Governing Region of Žilina, can equally be applied to the other regions of the Slovak Republic (the results of the proposed numbers of MRS stations will differ for different region areas, if the distance parameter is maintained).
3. Results
The history of MRS in the Slovak Republic is rich, commenced in the late 19th century by the fire corps of Bratislava and Košice, who mainly transported injured victims of accidents [
19,
20,
22], by specially adapted rescue vehicles pulled by horses. At that time, the first stationary facilities for rescue of persons were also established. The stationary MRS sites and their mobile ambulances have undergone major changes since their origin. The breakthrough year in MRS in the Slovak Republic was the year 2004, the year when the special MRS Act was passed [
3] with its executive decrees, updated and amended several times until now. The most significant amendment was the clause permitting private companies to become MRS providers (for 72 MRS providers provided, example in 2004 road rescue ambulance service). Another significant amendment was represented by an increase of the required number of MRS stations and rescue ambulances for MRS provision in any place within 15 min from receipt of the intervention order. The reform resulted in an increase in the number of stationary facilities with development of the related legislation from the original 91 [
18,
23] to 259. The numbers of MRS ambulances changed in 2013, 2016, 2018, and 2019 and another change is expected in 2021. The change of MRS providers occurred in 2019, when a new tender for the provision of MRS was announced. One of the most important and largest providers of MRS in Slovakia, namely Falck Rescue, a. S., which ceased to operate in Slovakia in the field of MRS in the course of 2020, did not participate in the announced tender. Another significant change in 2019 is the establishment of a new type of ambulance MRS “S”, which is designed primarily to provide urgent transport of a person between medical facilities, if the person’s state of health requires the provision of health care to paramedics during such transport. The number of MRS is expected to increase by 48. In the course of 2020, as a result of the Covid-19 pandemic, the MRS outpatient clinics adopted specific organizational and hygienic measures for the transport of persons suspected of Covid-19. A number of ambulance MRS have been set aside for the transport of these persons, the interior of which, including medical equipment, is regularly disinfected. Instructed dedicated MRS staff use specific personal protective medical equipment. When defining the optimum need for MRS stations, the Ministry of Health considered the regional population, area, and geographical position with the aim to balance their distribution and workloads, and the time needed by an ambulance to reach any human settlement to never exceed 15 min, so that the highest possible population percentage may receive medical first aid within 480 s within the “first hour quintet” [
21,
22]. According to [
23,
24], the first 15 min are decisive for survival of the injured, because in 5 min of asystole and apnoea the brain cells begin to necrotize, and 10 min of bleeding can result in an irreversible shock leading to multi-organ failure within a couple of days.
Distribution of MRS stations and numbers of MRS ambulances depend on multiple factors. The most important ones to be considered represented the municipality areas and populations, the regional structure of the Slovak Republic, accessibility of the points with the highest risk of emergency occurrence, etc.
Since 1992, urgent medical care was provided in the Self-Governing Region of Žilina by 10 MRS stations. In 2004, their number increased, and as of December 31, 2018, their number was 36, including 10 ambulance stations of emergency medical assistance and 26 ambulance stations of emergency paramedical first aid.
The current valid legislation of the Slovak Republic [
2,
3,
4] no longer specifies the maximum time for a MRS ambulance to reach the place of emergency from receipt of the intervention order.
The usual time to arrival of a MRS ambulance to the place of its need in EU Member States is up to 15 min, and some of the Member States have this time defined by the applicable legislation. For example in the Czech Republic [
25] the ambulance time to the place of emergency of 15 min was extended to 20 min. In Germany every federal state has not only its special medical rescue service legislation but also the accurately specified time standard for an ambulance to reach the person in need (for example within 12 min in Bavaria or within 10 min in Hessen.) If the medical rescue service dispatching office in London assesses that the arrival of the nearest MRS ambulance to the place of intervention might take more than seven minutes, a rescuer is sent to the location of the emergency on a bicycle or a motorcycle to secure first aid before a MRS ambulance arrival [
10,
26]. In the Slovak Republic, the applicable legislation [
4] defines that the operation conditions of a MRS station must assure an ambulance set off to the place of emergency in 2 min from receipt of the relevant instruction from an integrated rescue system coordination center or a MRS operation center. The particular MRS ambulance type is sent to the destination by a Regional MRS Operation Centre (they are eight at present and form parts of the coordination centers of the integrated rescue system). The operation centers sending ambulances to the places of need use the satellite vehicle monitoring system (for automatic vehicle location) and telecommunication connections. MRS ambulances are sent out for intervention by the Regional MRS Operation Centers on the basis of emergency calls, assessment of the conditions of the persons in need, and availability of MRS ambulances. The MRS ambulances receive instructions from an integrated rescue system coordination center or a MRS operation center requesting intervention or emergency transport, perform the emergency intervention or transport on the basis of examination of the health state of the person(s) in need, and observe instructions of the healthcare/medical intervention leaders on the emergency spot with multiple victims [
4].
A MRS ambulance sets off for the ordered place of intervention or to assure emergency transport from its MRS station, or from another place of a current emergency intervention, if already finished and prepared for a new intervention (for example after delivery of the person(s) in need to the nearest hospital), and before or during return to its home station [
26,
27] in the place of intervention the members of MRS ambulance crew must perform all actions needed to help the person(s) in need and if necessary provide for transport to the specified healthcare facility.
The address of the place of intervention is sent for the MRS ambulance crew to the automatic vehicle location system, where the touch screen displays to the crew the data of the intervention and the accurate time. The work of the MRS operator is crucial, for after receipt of each emergency call the operator must decide whether an ambulance crew with/without a doctor will be sent, and whether a road vehicle or a helicopter needs to be used for the intervention. Emergency conditions are to be addressed by the crew nearest to the place of the emergency and where cardiopulmonary resuscitation, brain trauma, or any other severe trauma are expected, sending of a crew with a doctor on board immediately follows [
28]. The total numbers of interventions by all MRS ambulances in the period 2013 to 2019 are shown in
Table 4.
The experiment minimized the number of persons in the municipalities where medical first aid was not provided within the defined D-Max time. The results of the experiment are shown in
Table 5.
The experiments were evaluated by the decision-making matrix method, on a scale from 1 to 10, with 1 corresponding to the lowest weight and 10 to the highest weight. The same scale was used for evaluation of compliance of the individual variants to the selected criteria. The order of appropriateness of the individual optimization proposals is shown in
Table 6.
The total number of interventions of the 6 MRS operators in the Žilina Self-Governing Region increased by 21.1% in that period. The increase points to the need for optimization of the MRS station distribution across the individual municipalities.
4. Discussion
Application of decision-supporting instruments was utilized for optimization with consideration of the places of emergency occurrence. The main aim of the optimization was to minimize the sums of distances between the individual municipalities of the Self-Governing Region of Žilina and the nearest MRS station locations. The distance sums were expressed by the times of travel of ambulances with the MRS crews from the MRS stations to various municipalities of the Žilina Self-Governing Region. The proposed network of MRS stations was based on the criterion of minimization of the number of persons not served within the defined time [
17]. Possible places of emergencies of the accident-with-multiple-victims type were defined by Analyses of Potential Occurrence of Emergencies in the districts of the region governed by district councils in Čadca, Dolný Kubín, Liptovský Mikuláš, Námestovo, Ružomberok, and Žilina. The municipalities of the Žilina Self-Governing Region were evaluated by means of multi-criteria decision-making using the decision-making matrix method on the basis of the defined criteria [
10]. The result was represented by the quantity of 137 municipalities selected for establishment of MRS stations on the basis of the probability of emergency occurrence. The selection was followed by numerical experiments focused on reduction/extension of the times to arrivals of MRS ambulances from MRS stations to the places of emergencies.
According to the calculations (also considering the road class and the ambulance speed following from the ambulance priority pass rights), the time of arrival of an ambulance to a precisely specified place within these municipalities may take more than 15 min. Some municipalities of the Žilina Self-Governing Region (for example Čičmany) are more remote from MRS stations, and an ambulance may reach some of the municipalities (for example Divina) in more than 19 min if the nearest ambulance is occupied.
The computations needed for the optimization were based on real data of the road network of the Self-Governing Region of Žilina. The result of the numeric optimization experiments, with consideration of the accident-critical locations and the populations of the individual municipalities, included three solution variants. The second variant was selected as the best, on the basis of multi-criteria decision-making, for the 15-min theoretical reach by an ambulance sent from a MRS station to any place of emergency. According to the data mentioned by [
29], the times of ambulance reach were roughly the same in 2017 and 2019, i.e., 9 min 40 s on average.
The advantage of the proposed solution is the application of the model to a real area location, which is based on the obligation of the state to provide urgent medical care in accordance with the specified arrival times. The disadvantage is the fact that if the arrival time is shortened, it is necessary to increase the total number of stations, or the number of ambulances MRS. Increased financial costs are associated with the construction or reconstruction of a building for the station, its equipment, or an increase in the number of ambulances MRS. This service is provided by private entities and their purpose of business is to realize a profit, not to incur costs, when their return may not be guaranteed in the event of a further change in legislation. In a built-up agglomeration (urban units), there is no problem in the availability of urgent health care, but the problem is the issue of the passability of the communication network for vehicles with the right of priority driving, regardless of the pandemic situation or the normal situation.
5. Conclusions
MRS ambulances, inter alia, play an important role in the system of urgent medical care provision to persons in need, under secure conditions or in emergency, in Slovakia. Ambulance work is governed by special legislation and secured by a sufficient number of MRS stations and their staffing, technological, and material equipment. A certain problem is represented by funding, which mainly affects deployment of MRS ambulances with a doctor on board. Optimization of the number of MRS stations was addressed as a location task of the special category of distribution issue linear programming. A public service system such as MRS must assure accessibility of MRS ambulance service to all citizens of the Slovak Republic. Each of the location tasks applied required a different mathematical model, mainly focused on seeking a bound function extreme (minimum, maximum) under the defined conditions.
The location-coverage task does not consider the situation of intervention by more MRS ambulances in one place. The results of a MCLP type task generally represent lower real municipality coverage and MRS ambulance reach of persons in need than calculated, especially at the moment of a requirement that could not be addressed by the nearest MRS station.
The MBCLP task appears to be the best for addressing the optimum distribution of MRS stations, if extended by more conditions, considering, inter alia, limitation of the workload per MRS ambulance (i.e., 1 MRS ambulance per max. 25,000 inhabitants) or the necessity of building MRS stations in priority municipalities with the highest risk of emergencies—accidents—with large numbers of injured victims. The adjustment of the number of MRS stations resulted in 2–3 times shorter time needed by MRS ambulances to reach a place of emergency. The computations also pointed out the fact that the time to an ambulance arrival at a place of emergency, for the proposed station distribution, as well as in comparison to practice (mean reach time 12 min), falls within the 16-min limit for circa 90 % of the Žilina Self-Governing Region population.
The current number of MRS providers even during a pandemic is sufficient to secure the population. Only in the current pandemic situation has the number of daily departures from individual stations increased. Area location of MRS stations is in accordance with the calculated model and fully corresponds to the needs and principles of providing urgent medical care.
The mathematical algorithm used for the location task solution is generally applicable in different regions and countries of the European Union, if the local standards, or legislation, define the maximum ambulance reach times. The mathematical algorithm for calculating the area location of MRS stations is applicable to any region, provided that the distances are known in relation to the specified arrival time, which is part (in Central European countries) of the applicable laws on the provision of urgent health care.

 ,
, 

{kind=link}