Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study †


 ,
,  ,
,  , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Experimental Section
2.1. Pilot Study
2.2. Study Design
2.3. Inclusion and Exclusion Criteria
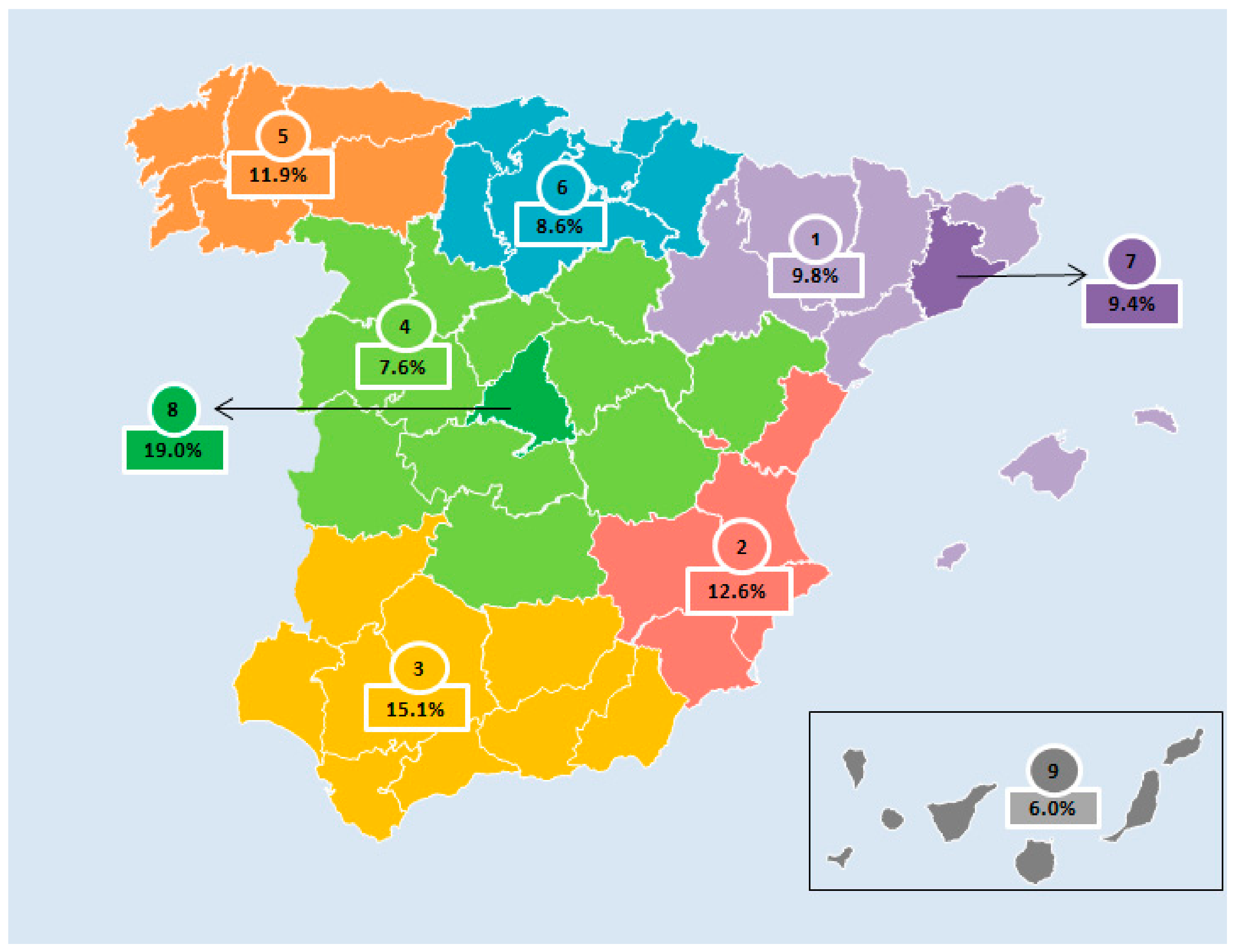
2.4. Sample
2.5. Ethical Aspects
Participant Confidentiality
2.6. Survey Instruments
2.6.1. Sociodemographic and Personal Questionnaire
2.6.2. Food Frequency Questionnaire
2.6.3. Twenty-Four-Hour Dietary Recall
2.6.4. Physical Activity and Sedentary Behavior Questionnaire
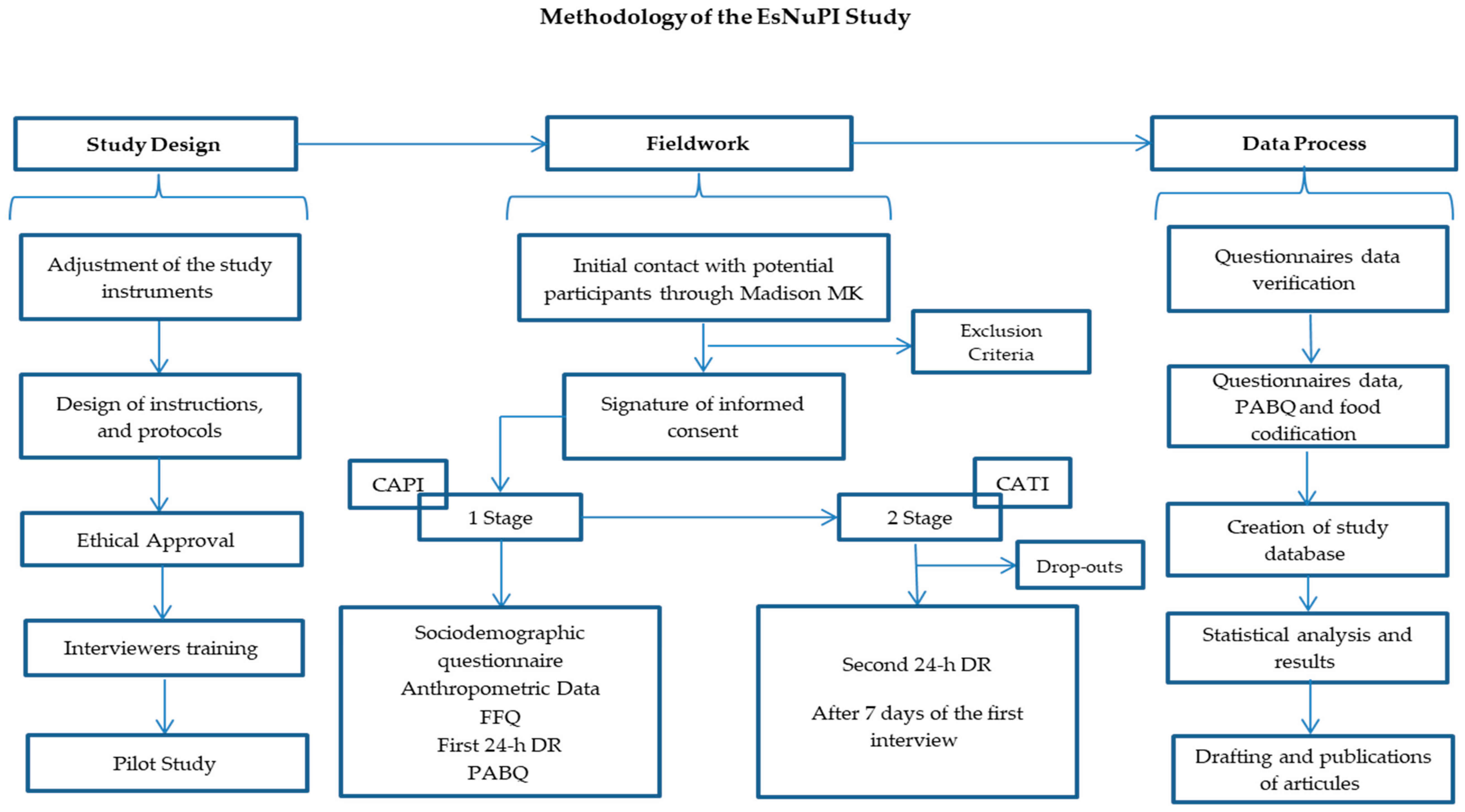
2.7. Stages of the Fieldwork
- Personal survey: the initial contact with the interviewer and the face-to-face interview.
- Telephone survey: contact with the interviewer through a telephone call.
2.7.1. Stage 1, Personal Survey: Initial Contact with the Interviewer and Face-To-Face Interview
- Classification and sociodemographic questionnaire (18 min).
- Anthropometric data (2 min): weight and size data declared by parents or caregivers based on the child’s health card.
- FFQ (60–90 min).
- 24-h DR (20 min).
- PABQ (15 min).
2.7.2. Stage 2, Telephone Survey: Contact with the Interviewee through a Telephone Call
- Second 24-h DR, ≥7 days after the first survey, considering that one should collect information about weekdays and the other about weekends.
2.8. Quality Control
- Necessity to answer all the questionnaires’ items.
- The initial quality control was based on the descriptions sent by the participants and combined with the photo guide information. Special attention was given to validate some variables such as ingredients, brands of processed and fast food, portion size, or culinary technique in order to obtain adequate information for future codification.
- FEN and FINUT were responsible for checking the food consumption records during the study.
- From the beginning of the coding process, FEN and FINUT worked together with MADISON MK to check the information and give them individual feedback on their work.
- The surveys received throughout the fieldwork were coded and depurated, transferring continuous feedback to the interviewers about possible errors or inconsistencies in their completion.
- Verification calls were performed by each interviewer to verify the incomplete answers and correct possible inconsistencies.
- The questionnaires that did not pass the stipulated quality controls were removed.
- The final approval of the received information was given by FEN and FINUT.
2.9. Statistical Analysis
3. Outcome Measures
3.1. Primary Outcome Measures
3.1.1. Dietary Habits
3.1.2. Milk and Dairy Product Consumption
3.1.3. Energy, and Macro- and Micronutrient Composition of the Diet
3.1.4. Diet Quality
3.1.5. Active and Sedentary Behavior Habits
3.2. Secondary Outcome Measures
3.2.1. Growth and Body Mass Index
3.2.2. Misreporting: Under-Reporting and Over-Reporting of Energy Intake
3.2.3. Sociodemographic Information
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Martorell, R. Importancia de la nutrición en los primeros 1.000 días de vida. In Tratado de Nutrición, 3rd ed.; Angel Gil: Madrid, Spain, 2019; Volume 4, pp. 237–267. [Google Scholar]
- Gil, Á.; Ortega, R.M. Introduction and executive summary of the supplement, role of milk and dairy products in health and prevention of noncommunicable chronic diseases: A series of systematic reviews. Adv. Nutr. 2019, 10, 67–73. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Use of the EFSA Comprehensive European Food Consumption Database in Exposure Assessment. EFSA J. 2011, 9, 2097. [Google Scholar] [CrossRef]
- González-Gil, E.M.; Santabárbara, J.; Russo, P.; Ahrens, W.; Claessens, M.; Lissner, L.; Börnhorst, C.; Krogh, V.; Lacoviello, L.; Molnar, D.; et al. Food intake and inflammation in European children: The IDEFICS study. Eur. J. Nutr. 2016, 55, 2459–2468. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.; Whitehead, R.; Maes, L.; Focus, G.H. An overview of adolescent dietary behaviours. In Dietary Habits; HBSC’s International Coodinating Centre: Glasgow, Scotland, 2017; 4p, Available online: http://www.hbsc.org/publications/factsheets/Dietary-Habits-english.pdf.
- GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2019, 393, 1958–1972. [Google Scholar] [CrossRef] [Green Version]
- Dalmau, J.; Peña Quintana, L.; Morais, A.; Martínez, V.; Varea, V.; Martínez, M.; Soler, B. Análisis cuantitativo de la ingesta de nutrientes en niños menores de 3 años. An. Pediatr. (Barc) 2015, 82, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Servicios Sociales e Igualdad Agencia Española de Consumo. Encuesta Nacional de consumo de Alimentos en población Infantil y Adolescentes (ENALIA) (2012–2014); Ministerio de Sanidad, Consumo, Igualdad y Servicios Sociales: Madrid, Spain, 2013.
- Pérez, C.; Gil, Á.; González-Gross, M.; Ortega, R.; Serra-Majem, L.; Varela-Moreiras, G. Clustering of dietary patterns, lifestyles, and overweight among Spanish children and adolescents in the ANIBES study. Nutrients 2015, 8, 11. [Google Scholar] [CrossRef]
- Fernández-Alvira, J.M.; Bammann, K.; Pala, V.; Krogh, V.; Barba, G.; Eiben, G.; Hebestreit, A.; Veidebaum, T.; Reisch, L.; Tornaritis, M.; et al. Country-specific dietary patterns and associations with socioeconomic status in European children: The IDEFICS study. Eur. J. Clin. Nutr. 2014, 68, 811–821. [Google Scholar] [CrossRef]
- Hebestreit, A.; Intemann, T.; Siani, A.; De Henauw, S.; Eiben, G.; Kourides, Y.A.; Kovacs, E.; Moreno, L.A.; Veidebaum, T.; Krogh, V.; et al. Dietary patterns of European children and their parents in association with family food environment: Results from the I. family study. Nutrients 2017, 9, 126. [Google Scholar] [CrossRef] [Green Version]
- Hebestreit, A.; Börnhorst, C.; Barba, G.; Siani, A.; Huybrechts, I.; Tognon, G.; Eiben, G.; Moreno, L.A.; Fernández Alvira, J.M.; Loit, H.M.; et al. Associations between energy intake, daily food intake and energy density of foods and BMI z-score in 2–9-year-old European children. Eur. J. Nutr. 2014, 53, 673–681. [Google Scholar] [CrossRef] [Green Version]
- Dror, D.K.; Allen, L.H. Dairy product intake in children and adolescents in developed countries: Trends, nutritional contribution, and a review of association with health outcomes. Nutr. Rev. 2014, 72, 68–81. [Google Scholar] [CrossRef]
- Lamas, C.; Castro, M.J.; Gil-Campos, M.; Gil, A.; Couce, M.L.; Leis, R. Effects of dairy product consumption on height and bone mineral content in children: A systematic review of controlled trials. Adv. Nutr. 2019, 10, 88–96. [Google Scholar]
- Santaliestra-Pasías, A.M.; González-Gil, E.; Pala, V.; Intemann, T.; Hebestreit, A.; Russo, P.; Van Aart, C.; Rise, P.; Veidebaum, T.; Molnar, D.; et al. Predictive associations between lifestyle behaviours and dairy consumption: The IDEFICS study. Nutr. Metab. Cardiovasc. Dis. 2019, 19, 1–24. [Google Scholar]
- Ortega, R.O.; González-Rodríguez, L.; Jiménez Ortega, A.; Perea Sánchez, J.; Bermejo López, L. N°920030, G. de investigación. Implicación del consumo de lácteos en la adecuación de la dieta y de la ingesta de calcio y nutrientes en niños españoles. Nut. Clin. Diet Hosp. 2012, 32, 28–36. [Google Scholar]
- MERCASA. Alimentación en España 2018, 21st ed.; Ministerio de Agricultura, Pesca y Alimentación: Madrid, Spain, 2018; pp. 333–344.
- Informe del Consumo Alimentario en España. 2018. Available online: https://www.mapa.gob.es/es/alimentacion/temas/consumo-y-comercializacion-y-distribucion-alimentaria/panel-de-consumo-alimentario/ultimos-datos/ (accessed on 1 August 2019).
- Instituto Nacional de Estadística. Available online: https://www.ine.es/dyngs/INEbase/es/categoria.htm?c=Estadistica_P&cid=1254734710990 (accessed on 1 January 2018).
- Gil-Campos, M.; Personal Comunication of Mercedes Gil-Campos, as cordinator of the Meli-Pop Proyect (Expediente PI18/0093 del Fondo de Investigaciones Sanitarias, Instituto Carlos III). Personal Comunication, 2018.
- Fernandez-Ballart, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Martin-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly mediterranean population of spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [Green Version]
- Pérez, C.; Aranceta, J.; Salvador, G.; Varela-Moreiras, G. Métodos de Frecuencia de consumo alimentario. Rev. Esp. Nutr. Com. 2015, 21, 45–52. [Google Scholar]
- Castell, G.; Serra, L.; Ribas, L. ¿Qué y cuánto comemos? El método Recuerdo de 24 horas. Rev. Esp. Nutr. Comunitaria 2015, 2, 42–44. [Google Scholar]
- Ortega, R.; Perez-Rodrigo, C.; Lopez-Sobaler, A.M. Métodos de evaluación de la ingesta actual: Registro o diario dietético. Nutr. Hosp. 2015, 21, 34–41. [Google Scholar]
- European Food Safety Authority (EFSA). Guidance of the EU Menu methodology. EFSA J. 2014, 12, 3944. [Google Scholar]
- Fundación Española de la Nutrición (FEN). Tablas de Medidas Caseras y Raciones Habituales de Consumo; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2013. [Google Scholar]
- López, R.; Martínez de Victoria, E.; Gil, A.M. Guía Fotográfica de Porciones de Alimentos Consumidos en España, Universidad de Granada; Fundación Iberoamericana de Nutrición: Granada, Spain, 2019. [Google Scholar]
- Martínez-Lemos, R.I.; Ayán Pérez, C.; Sánchez Lastra, A.; Cancela Carral, J.M.; Valcarce Sánchez, R. Cuestionarios de actividad física para niños y adolescentes españoles: Una revisión sistemática. An. Sist. Sanit. Navar. 2016, 39, 1137–6627. [Google Scholar]
- Camargo, D.M.; Santisteban, S.; Paredes, E.; Flórez, M.; Bueno, D.A. Confiabilidad de un cuestionario para medir actividad física y comportamientos sedentarios en niños desde preescolar a cuarto grado de primaria. Biomedica 2015, 35, 347–356. [Google Scholar] [CrossRef] [Green Version]
- Zhao, W.; Yu, K.; Tan, S.; Zheng, Y.; Zhao, A.; Wang, P.; Zhang, Y. Dietary diversity scores: An indicator of micronutrient inadequacy instead of obesity for Chinese children. BMC Public Health 2017, 17, 440. [Google Scholar] [CrossRef] [Green Version]
- Royo-Bordonada, M.A.; Gorgojo, L.; Oyab, M.; Garcés, C.; Rodríguez-Artalejo, F.; Rubio, R.; Barrio, J.L. Variedad y diversidad de la dieta de los niños españoles: Estudio Cuatro Provincias. Med. Clin. 2003, 120, 167–171. [Google Scholar] [CrossRef]
- Vadiveloo, M.; Dixon, L.B.; Mijanovich, T.; Elbel, B.; Parekh, N. Development and evaluation of the US Healthy Food Diversity index. Br. J. Nutr. 2014, 112, 1562–1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newby, P.K.; Tucker, K.L. Empirically derived eating patterns using factor or cluster analysis: A review. Nutr. Rev. 2004, 62, 177–203. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. Dietary patterns análisis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Sociedad Española de la Nutrición Comunitaria. Guía de la Alimentación Saludable, Recomendaciones para una Alimentación Individual, Familiar o Colectiva Saludable, Responsable y Sostenible, 1st ed.; Sociedad Española de la Nutrición Comunitaria: Madrid, Spain, 2018; pp. 1–32. [Google Scholar]
- Sociedad Española de la Nutrición Comunitaria, Pirámide de la Alimentación Saludable. Available online: http://www.nutricioncomunitaria.org/es/noticia/piramide-de-la-alimentacion-saludable-senc-2015 (accessed on 5 June 2019).
- Serra-Majem, L.; Aranceta Bartrina, J. Objetivos nutricionales para la población española: Consenso de la Sociedad Española de Nutrición Comunitaria 2011. Rev. Esp. Nutr. Comu. 2011, 17, 178–199. [Google Scholar]
- Fundación Española de la Nutrición (FEN). Software VD-FEN 2.1 Programa de Valoración Dietética de la FEN; Fundación Española de la Nutrición (FEN): Madrid, Spain, 2013. [Google Scholar]
- Moreiras, O.; Carbajal, A.; Cabrera, L. Ingestas Diarias Recomendadas de Energía y Nutrientes para la Población Española. Tablas de Composición de Alimentos, 19th ed.; Ediciones Pirámide (Grupo Anaya, SA): Madrid, Spain, 2018. [Google Scholar]
- European Food Safety Authority. Available online: https://0-efsa-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/epdf/10.2903/j.efsa.2013.3408 (accessed on 22 April 2018).
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, youth and the Mediterranean diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in children and adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- Roset-Sall, A.M.; Ramon-Cabot, J.; Salabarnada-Torras, J.; Pera, G.; Dalmau, A. Educational intervention to improve adherence to the Mediterranean diet among parents and their children aged 1–2 years. Public Health Nutr. 2015, 19, 1131–1144. [Google Scholar] [CrossRef] [Green Version]
- Krebs-Smith, S.M.; Pannucci, T.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the Healthy Eating Index: HEI-2015. J. Acad. Nutr. Diet 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [Green Version]
- Tognon, G.; Moreno, L.A.; Mouratidou, T.; Veidebaum, T.; Molnár, D.; Russo, P.; Siani, A.; Akhandaf, Y.; Krogh, V.; Tornaritis, M.; et al. Adherence to a Mediterranean-like dietary pattern in children from eight European countries. The IDEFICS study. Int. J. Obes. 2017, 2, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Manios, Y.; Kourlaba, G.; Grammatikaki, E.; Androutsos, O.; Moschonis, G.; Roma-Giannikou, E. Development of a diet-lifestyle quality index for young children and its relation to obesity: The Preschoolers Diet-Lifestyle Index. Public Health Nutr. 2010, 13, 2000–2009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butte, N.F.; Watson, K.B.; Ridley, K.; Zakeri, I.F.; Mcmurray, R.G.; Pfeiffer, K.A.; Fulton, J.E. A youth compendium of physical activities: Activity codes and metabolic intensities. Med. Sci. Sports Exerc. 2017, 50, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Schofield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39, 5–41. [Google Scholar] [PubMed]
- Koletzko, B.; Goulet, O.; Hunt, J.; Krohn, K.; Shamir, R.; ESPGHAN; ESPEN. Guidelines on Paediatric Parenteral Nutrition of the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN) and the European Society for Clinical Nutrition and Metabolism (ESPEN), Supported by the European Society of Paediatric Research (ESPR). J. Pediatr. Gastroenterol. Nutr. 2005, 2, 1–87. [Google Scholar]
- World Health Organization. Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Ministry of Health, Social Services and Equality. Physical Activity for Health and sedentary behavior reduction. Recommendations for population. In Estrategy for Health Promotion and Prevention in the National Health System; Ministry of Health, Social Services and Equality: Madrid, Spain, 2015. [Google Scholar]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; Doncarlos, L.; Ware, J.C. National Sleep Foundations updated sleep duration recommendations: Final report. SLEH 2015, 1, 233–243. [Google Scholar]
- Paruthi, S.; Brooks, L.; Ambrosio, C.D.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Troester, M.M. Recommended Amount of Sleep for Pediatric Populations: A consensus statement of the American academy of sleep medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef]
- Contardo Ayala, A.M.; Nijpels, G.; Lakerveld, J. Validity of self-measured waist circumference in adults at risk of type 2 diabetes and cardiovascular disease. BMC Med. 2014, 12, 170. [Google Scholar] [CrossRef] [Green Version]
- Patrones de Crecimiento Infantil de la OMS. Available online: https://www.who.int/childgrowth/es/ (accessed on 2 July 2019).
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify under-recording. Eur. J. Clin. Nutr. 1991, 45, 569–581. [Google Scholar]
- Black, A.E.; Goldberg, G.R.; Jebb, S.A.; Livingstone, M.B.; Cole, T.J.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology 2 Evaluating the results of published surveys. Eur. J. Clin. Nutr. 1991, 45, 583–599. [Google Scholar]
- Nelson, M.; Black, A.E.; Morris, J.A.; Cole, T.J. Between- and within-subject variation in nutrient intake from infancy to old age: Estimating the number of days required to rank dietary intakes with desired precision. Am. J. Clin. Nutr. 1989, 50, 155–167. [Google Scholar] [CrossRef] [Green Version]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake: Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [Green Version]
- McGowan, L.; Pot, G.K.; Stephen, A.M.; Lavelle, F.; Spence, M.; Raats, M.; Dean, M. The influence of socio-demographic, psychological and knowledge-related variables alongside perceived cooking and food skills abilities in the prediction of diet quality in adults: A nationally representative cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 111. [Google Scholar] [CrossRef] [Green Version]
- UOE Data Collection on Formal Education, Manual on Concepts, Definitions and Classifications. Available online: http://uis.unesco.org/sites/default/files/documents/uoe2016manual_11072016_0.pdf (accessed on 15 September 2019).
- Instituto Nacional de Estadística. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177033&menu=ultiDatos&idp=1254735976614 (accessed on 9 October 2019).
- Ziauddeen, N.; Page, P.; Penney, T.L.; Nicholson, S.; Kirk, S.F.; Almiron-Roig, E. Eating at food outlets and leisure places and “on the go” is associated with less-healthy food choices than eating at home and in school in children: Cross-sectional data from the UK National Diet and Nutrition Survey Rolling Program (2008–2014). Am. J. Clin. Nutr. 2018, 107, 992–1003. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, A.L. FITS and KNHS overview: Methodological challenges in dietary intake data collection among infants, toddlers, and children in selected countries. Nestle Nutr. Inst. Workshop Ser. 2019, 91, 69–78. [Google Scholar] [PubMed]
- Varela-Moreiras, G. Libro Blanco de la Nutrición en España (White Book on Nutrition in Spain); Spanish Foundation on Nutrition/Spanish Agency on Food Safety and Nutrition (AESAN, MSSSI): Madrid, Spain, 2013.
- Ferrari, P.; Friedenreich, C.; Matthews, C.E. The role of measurement error in estimating levels of physical activity. Am. J. Epidemiol. 2007, 166, 832–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ocké, M.; De Boer, E.; Brants, H.; Van der Laan, J.; Niekerk, M.; Van Rossum, C.; Temme, L.; Freisling, H.; Nicolas, G.; Casagrande, C.; et al. Pancake—Pilot study for the Assessment of Nutrient intake and food Consumption Among Kids in Europe. EFSA J. 2012, 9, 1–120. [Google Scholar] [CrossRef]
- Petra, A.; Hardie, L.J.; Frost, G.; Alwan, N.; Carter, M.; Elliot, P.; Ford, E.; Hancock, N.; Morris, M.; Mulla, U.; et al. Validity of an online 24-h recall tool (myfood24) for dietary assessment in population studies: Comparison with biomarkers and standard interviews. BMC Med. 2018, 16, 1–14. [Google Scholar]
- Castro Morais, D.; Sousa Moraes, L.; Guimarães da Silva, D.C.; Aparecida Pinto, C.; Farias de Novaes, J. Methodological aspects of dietary quality assessment in Brazil: Systematic review. Cien Saude Colet 2017, 22, 2671–2680. [Google Scholar]
- Example of a Protocol for Identification of Misreporting (under- and Overreporting of Energy Intake) Based on the PILOT-PANEU Project. Available online: http://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/3944A-8-2-1.pdf (accessed on 5 October 2019).



{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Healthy participants between 1 and <10 years old without diseases entailing changes in their dietary patterns. | Children with any disease that causes changes in their dietary patterns or any dietary restriction, or children following a therapeutic diet due to recent surgery or any other medical prescription and pathology. |
| Children whose parents/caregivers report that they are following their habitual diet. | Children whose parents reported that they were not following a normal diet for any reason, including a transitory pathology (cold, flu, gastroenteritis, chickenpox, etc.) at the time of the fieldwork. |
| Children whose parents or caregivers can read and understand the questionnaires properly. | Children following a vegan diet. |
| Children who live in an institution (boarding schools, nursing homes, hospitals, host institutions, etc.). | |
| Children related to Madison MK or Lactalis employees *. | |
| Children whose parents or caregivers did not provide a signed consent form for their participation or did not complete any study phase. |
| Sample (n) | ||||||
|---|---|---|---|---|---|---|
| Targeted Sample (n = 1500) | Final Sample (n = 1514) | |||||
| Reference * | Booster ** | Reference * | Booster ** | Total | ||
| n = 750 | n = 750 | n = 742 | n = 772 | n = 1514 | ||
| Sex | Boys | 375 | 375 | 374 | 385 | 759 |
| Girls | 375 | 375 | 368 | 387 | 755 | |
| Age (years) | 1 to <3 | 250 | 250 | 171 | 303 | 474 |
| 3 to <6 | 250 | 250 | 257 | 276 | 533 | |
| 6 to <10 | 250 | 250 | 314 | 193 | 507 | |
| Food Groups | |
|---|---|
| Dairy products Breast milk (150 mL), infant formula, toddler’s milk formula, cow’s milk, enriched milk, and specially formulated milk, 200 mL Vegetable drinks (200 mL) Yogurt (125 g) Fresh cheese (15–30 g) and cured cheese (15 g) Sugared dairy dessert (125 g) and ice cream (120 g) Other dairy products (condensed milk, 10 g; cream, 20 g; and flavored milk, 200 mL) | Oils and fats Olive oil (10 g) Other vegetable oils and lard (10 g) Margarine and butter (12 g) |
| Eggs, meat, and fish Eggs (64 g) Chicken and turkey with or without skin, medium-fat meat, fatty pork, lamb meat, rabbit meat, or liver and other viscera (55 g) “Serrano” ham, cooked ham, sausages, other processed meats (15 g) Fish: white fish (55 g), bluefish (small and large, 55 g), fresh seafood (90–100 g), and canned fish (25 g) | Bakery products Cookies and cakes (25–50 g) Homemade bakery products (50 g) Sugary cocoa (5 g), nougat (20 g), and shortbread cookies (45 g) |
| Vegetables and potatoes All kind of vegetables (55 g) Potatoes (55–80 g) | Miscellaneous Industrial pre-cooked products (25–50 g) Homemade pre-cooked products (25–50 g) Sauces (8 g) Condiments (0.25 g) Sugar, honey, and marmalade (10 g) Low- or no-calorie sweetener (0.05 g) Snacks (fried snacks, 50 g) |
| Fruits and nuts All kinds of fresh fruits (100–200 g) Olives (20 g) Fruits with juice and fruits with syrup (50 g) Dried fruits (20 g)Nuts (17.5 g) | Beverages Sugar-sweetened carbonated beverages or low-calorie carbonated beverages (200 mL) Natural juices and commercial juices (200 mL) Mixtures of fruit juice and milk, sugar-sweetened or low-calorie sweetened (200 mL) |
| Legumes, cereals, and pasta Legumes (40 g) Bread (20–25 g) Breakfast cereals (30 g) Rice and pasta (40 g) | Homemade and commercial baby food, homemade and commercial baby porridge Homemade baby food (200 mL) Fruit commercial baby food (200 mL) Vegetable baby food (200 mL) Vegetable commercial baby food (200 mL) Vegetables with meat and/or fish homemade baby food (200 mL) Cereals with milk homemade baby porridge (200 mL) Cereals with milk commercial baby porridge (200 mL) |
| AGE GROUP (years) | ||||
|---|---|---|---|---|
| <1 | 1–2 | 3–4 | 5–17 | |
| World Health Organization [49,50] | At least 30 min every day | At least 180 min every day | At least 180 min every day, with 60 min of moderate-to-vigorous intensity | At least 60 min every day of moderate-to-vigorous intensity |
| AGE GROUP (years) | ||||
|---|---|---|---|---|
| <1 | 1–2 | 3–4 | 5–17 | |
| World Health Organization [49,50] | 0 min | 1 year: 0 min 2 years: no more than 60 min | No more than 60 min | - |
| Ministry of Health, Social Services and Equality [51] | 0 to <2 | 2–4 | 5–17 | |
| 0 min | No more than 60 min | No more than 120 min | ||
| AGE GROUP (years) | ||||
|---|---|---|---|---|
| <1 | 1–2 | 3–4 | 5–17 | |
| World Health Organization [50] | 0–3 months 14–17 h 4–11 months 12–16 h | 11–14 h | 10–13 h | - |
| National Sleep Foundation [52] | <1 | 1–2 | 3–5 | 6–13 |
| 0–3 months 14–17 h 4–11 months 12–15 h | 11–14 h | 10–13 h | 9–11 h | |
| The American Academy of Sleep Medicine [53] | <1 | 1–2 | 3–5 | 6–12 |
| 4–12 months 12–16 h | 11–14 h | 10–13 h | 9–12 h | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madrigal, C.; Soto-Méndez, M.J.; Hernández-Ruiz, Á.; Ruiz, E.; Valero, T.; Ávila, J.M.; Lara-Villoslada, F.; Leis, R.; Martínez de Victoria, E.; Moreno, J.M.; et al. Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study. Nutrients 2019, 11, 3050. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123050
Madrigal C, Soto-Méndez MJ, Hernández-Ruiz Á, Ruiz E, Valero T, Ávila JM, Lara-Villoslada F, Leis R, Martínez de Victoria E, Moreno JM, et al. Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study. Nutrients. 2019; 11(12):3050. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123050
Chicago/Turabian StyleMadrigal, Casandra, María José Soto-Méndez, Ángela Hernández-Ruiz, Emma Ruiz, Teresa Valero, José Manuel Ávila, Federico Lara-Villoslada, Rosaura Leis, Emilio Martínez de Victoria, Jose Manuel Moreno, and et al. 2019. "Dietary and Lifestyle Patterns in the Spanish Pediatric Population (One to <10 Years Old): Design, Protocol, and Methodology of the EsNuPI Study" Nutrients 11, no. 12: 3050. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123050