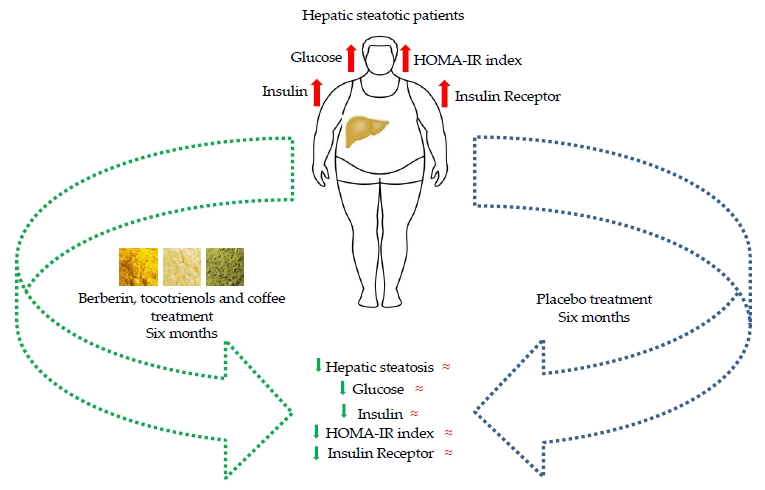
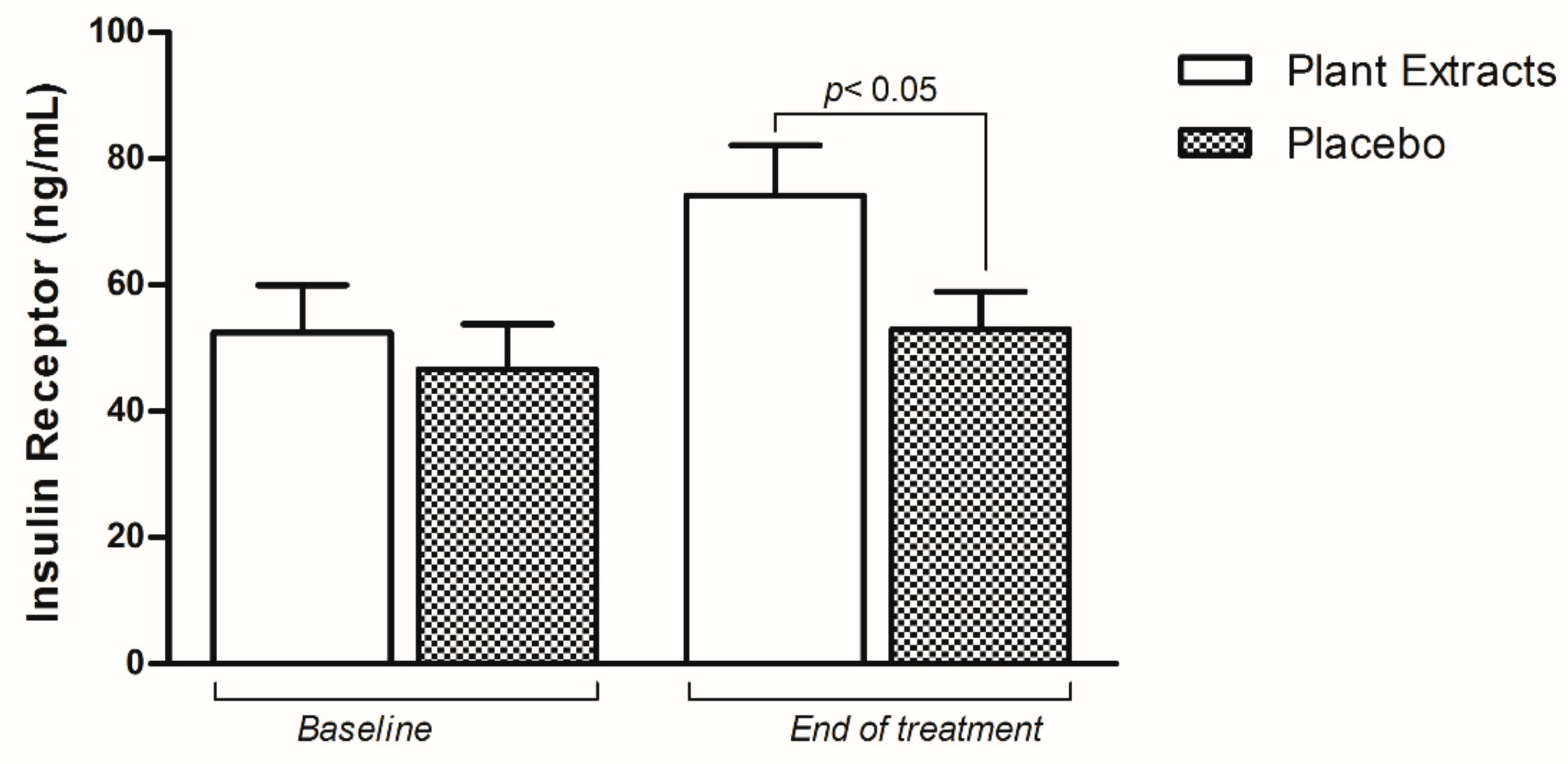
Berberis aristata, Elaeis guineensis and Coffea canephora Extracts Modulate the Insulin Receptor Expression and Improve Hepatic Steatosis in NAFLD Patients: A Pilot Clinical Trial

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Anthropometric Measurements
2.3. Biochemical Measurements
2.4. Serum Insulin Receptor Measurement
2.5. Quantification of Hepatic Steatosis
2.6. Statistical Analyses
3. Results
3.1. The Effect of Nutraceutical on Metabolic Parameters
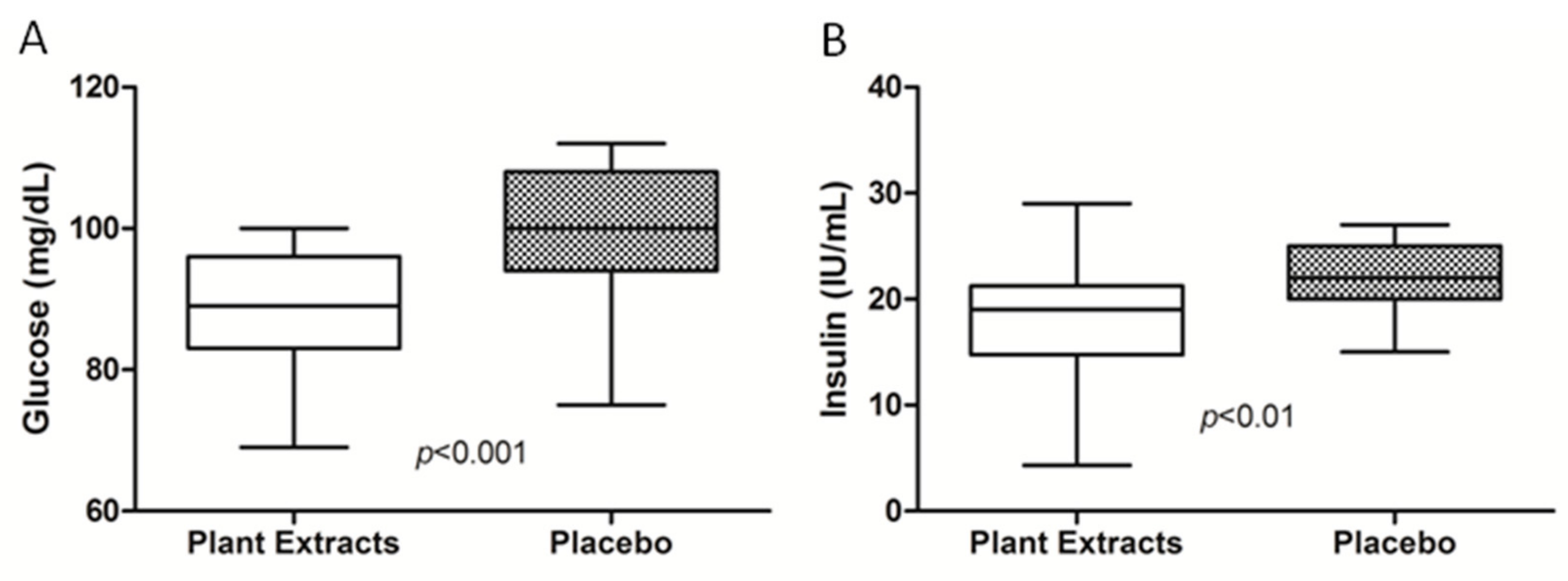
3.2. The Effect of Nutraceutical on Glycemic Profile and Insulin Resistance
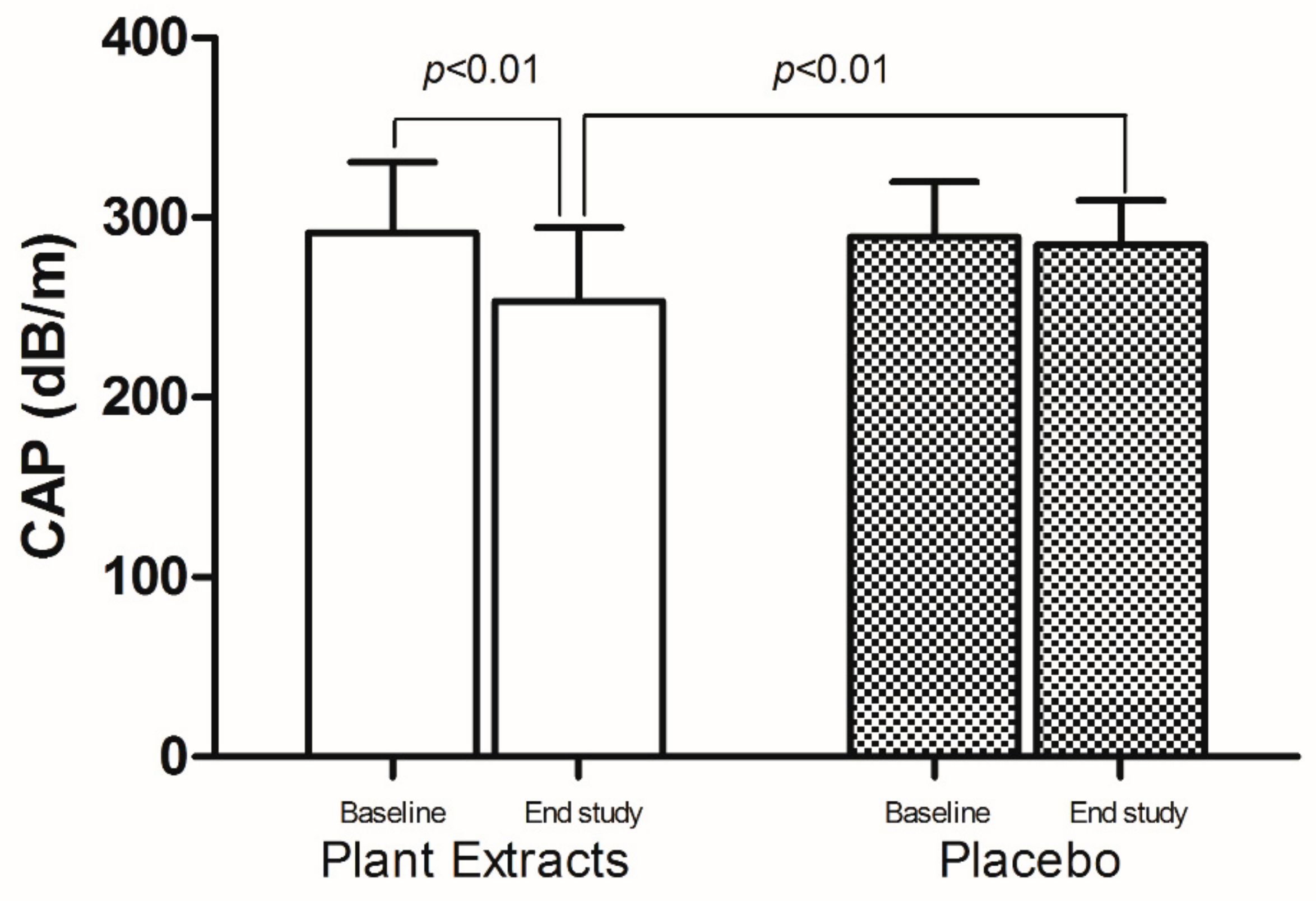
3.3. The Effect of Nutraceutical on Hepatic Steatosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Estes, C.; Razavi, H.; Loomba, R.; Younossi, Z.; Sanyal, A.J. Modelling the epidemic of non-alcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology 2018, 67, 123–133. [Google Scholar] [CrossRef]
- Taylor, S.I.; Accili, D.; Iami, Y. Insulin resistance or insulin deficiency. Which is the primary cause of NIDDM. Diabetes 1994, 43, 735–740. [Google Scholar] [CrossRef] [PubMed]
- Kido, Y.; Nakae, J.; Accilid, D. Clinical review 125: The insulin receptor and its cellular targets. J. Clin. Endocrinol. Metab. 2001, 86, 972–979. [Google Scholar] [PubMed] [Green Version]
- Pezzino, V.; Papa, V.; Costantino, A.; Frittitta, L.; Russo, P.; Goldfine, I.D.; Vigneri, R. Identification and Initial Characterization of Insulin Receptor-Like Immunoreactivity in Human Plasma. J. Clin. Endocrinol. Metab. 1992, 74, 1116–1121. [Google Scholar] [PubMed]
- Younossi, Z.M. Non-alcoholic fatty liver disease—A global public health perspectives. J. Hepatol. 2019, 70, 531–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.; Tacke, F.; Arrese, M.; Chander-Sharma, B.; Mostafa, I.; Bugianesi, E.; Wai-Sun Wong, V.; Yilmaz, Y.; George, J.; Fan, J.; et al. Global perspectives on non-alcoholic fatty liver disease and non-alcoholic steatohepatitis. Hepatology 2019, 69, 2672–2682. [Google Scholar] [CrossRef] [Green Version]
- Vilar-Gomez, E.; Chalasani, N. Non invasive assessment of non-alcoholic fatty liver disease: Clinical prediction rules and blood-based biomarkers. J. Hepatol. 2018, 68, 305–315. [Google Scholar] [CrossRef]
- Petta, S.; Maida, M.; Macaluso, F.S.; Di Marco, V.; Cammà, C.; Cabibi, D.; Craxì, A. The severity of steatosis influences liver stiffness measurement in patients with non-alcoholic fatty liver disease. Hepatology 2015, 62, 1101–1110. [Google Scholar] [CrossRef]
- Petta, S.; Wong, V.W.; Cammà, C.; Hiriart, J.B.; Wong, G.L.; Marra, F.; Vergniol, J.; Chan, A.W.; Di Marco, V.; Merrouche, W.; et al. Improved noninvasive prediction of liver fibrosis by liver stiffness measurement in patients with non-alcoholic fatty liver disease accounting for controlled attenuation parameter values. Hepatology 2017, 65, 1145–1155. [Google Scholar] [CrossRef]
- Bril, F.; Cusi, K. Management of Nonalcoholic Fatty Liver Disease in Patients With Type 2 Diabetes: A Call to Action. Diabetes Care 2017, 40, 419–430. [Google Scholar] [CrossRef] [Green Version]
- Kong, W.J.; Zang, H.; Song, D.Q.; Xue, R.; Zhao, W.; Wei, J.; Wang, Y.M.; Shan, N.; Zhou, Z.X.; Yang, P.; et al. Berberine reduces insulin resistance through protein kinase C-dependent up-regulation of insulin receptor expression. Metabolism 2009, 58, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Vafa, M.; Haghighat, N.; Moslehi, N.; Eghtesadi, S.; Heydari, I. Effect of Tocotrienols enriched canola oil on glycemic control and oxidative status in patients with type 2 diabetes mellitus: A randomized double-blind placebo-controlled clinical trial. J. Res. Med. Sci. 2015, 20, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Vitaglione, P.; Morisco, F.; Mazzone, G.; Amoruso, D.C.; Ribecco, M.T.; Romano, A.; Fogliano, V.; Caporaso, N.; D’Argenio, G. Coffee reduces liver damage in a rat model of steatohepatitis: The underlying mechanisms and the role of polyphenols and melanoidins. Hepatology 2010, 52, 1652–1661. [Google Scholar] [CrossRef] [PubMed]
- De Ledinghen, V.; Vergniol, J.; Capdepont, M.; Chermak, F.; Hiriart, J.B.; Cassinotto, C.; Merrouche, W.; Foucher, J.; Brigitte, L.B. Controlled attenuation parameter (CAP) for the diagnosis of steatosis: A prospective study of 5323 examinations. J. Hepatol. 2014, 60, 1026–1031. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; De Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- Stepanova, M.; Rafiq, N.; Makhlouf, H.; Agrawal, R.; Kaur, I.; Younoszai, Z.; McCullough, A.; Goodman, Z.; Younossi, Z.M. Predictors of all-cause mortality and liver-related mortality in patients with non-alcoholic fatty liver disease (NAFLD). Dig. Dis. Sci. 2013, 58, 3017–3023. [Google Scholar] [CrossRef]
- Zhang, H.; Wei, J.; Xue, R.; Wu, J.D.; Zhao, W.; Wang, Z.Z.; Wang, S.K.; Zhou, Z.X.; Song, D.Q.; Wang, Y.M.; et al. Berberine lowers blood glucose in type 2 diabetes mellitus patients through increasing insulin receptor expression. Metabolism 2010, 59, 285–292. [Google Scholar] [CrossRef]
- Wang, Y.; Yan, A.; Li, S.; Liu, B.; Li, H.; Yan, Y. Efficacy and safety of berberine in the treatment of type 2 diabetes with insulin resistance: Protocol for a systematic review. Medicine 2019, 98, e16947. [Google Scholar] [CrossRef]
- Lee, H.; Lim, Y. Tocotrienol-rich fraction supplementation reduces hyperglycemia-induced skeletal muscle damage through regulation of insulin signaling and oxidative stress in type 2 diabetic mice. J. Nutr. Biochem. 2018, 57, 77–85. [Google Scholar] [CrossRef]
- Pang, K.L.; Chin, K.Y. The Role of Tocotrienol in Protecting Against Metabolic Diseases. Molecules 2019, 24, 923. [Google Scholar] [CrossRef] [Green Version]
- Natella, F.; Scaccini, C. Role of coffee in modulation of diabetes risk. Nutr. Rev. 2012, 70, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Baspinar, B.; Eskici, G.; Ozcelik, A.O. How coffee affects metabolic syndrome and its components. Food Funct. 2017, 8, 2089–2101. [Google Scholar] [CrossRef] [PubMed]
- Vuppalanchi, R.; Siddigui, M.S.; Van Natta, M.L.; Hallinan, E.; Brandman, D.; Kowdley, K.; Neuschwander-Tetri, B.A.; Loomba, R.; Dasarathy, S.; Abdelmalek, M.; et al. Performance characteristics of vibration-controlled transient elastography for evaluation of nonalcoholic fatty liver disease. Hepatology 2018, 67, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Romero-Gomez, M.; Zelber-Sagi, S.; Trenell, M. Treatment of NAFLD with diet, physical activity and exercise. J. Hepatol. 2017, 67, 829–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Baseline | End-of-Study | ||||
|---|---|---|---|---|---|---|
| Plant Extracts (n = 26) | Placebo (n = 23) | p-Value | Plant Extracts (n = 26) | Placebo (n = 23) | p-Value | |
| BMI (Kg/m2) | 28.6 ± 3 | 28.2 ± 2.8 | 0.633 | 27.8 ± 2.8 | 27.6 ± 3 | 0.756 |
| Waist-Hip Ratio | 0.93 ± 0.05 | 0.94 ± 0.05 | 0.308 | 0.93 ± 0.07 | 0.9 ± 0.07 | 0.405 |
| AST (times ULN) | 0.69 ± 0.3 | 0.60 ± 0.2 | 0.256 | 0.63 ± 0.3 | 0.6 ± 0.2 | 0.622 |
| ALT (times ULN) | 0.85 ± 0.5 | 0.64 ± 0.3 | 0.09 | 0.72 ± 0.3 | 0.7 ± 0.3 | 0.695 |
| γ-GT (times ULN) | 1.1 ± 1.3 | 1.0 ± 1.1 | 0.788 | 0.98 ± 1.1 | 1 ± 0.9 | 0.695 |
| Triglycerides (mg/dL) | 154.5 ± 43.4 | 142 ± 54.6 | 0.375 | 134.5 ± 59.9 | 143 ± 54.5 | 0.602 |
| Total cholesterol (mg/dL) | 194.7 ± 36 | 191.3 ± 19 | 0.681 | 182.9 ± 29.7 | 193.4 ± 23.3 | 0.135 |
| HDL cholesterol (mg/dL) | 42.1 ± 10.8 | 39.7 ± 8 | 0.374 | 44.2 ± 9.8 | 42 ± 8.9 | 0.333 |
| LDL cholesterol (mg/dL) | 120.3 ± 28.1 | 107.2 ± 20.5 | 0.07 | 109,5 ± 29.4 | 116.4 ± 20.7 | 0.136 |
| Glucose (mg/dL) | 97.7 ± 16.6 | 98 ± 11.9 | 0.934 | 88.8 ± 7.5 | 98.8 ± 9.9 | <0.001 |
| Insulin (IU/mL) | 23.8 ± 6.5 | 23.1 ± 2.9 | 0.663 | 17.9 ± 5.7 | 22.3 ± 3.3 | <0.01 |
| HOMA-IR index | 5.8 ± 2.3 | 5.6 ± 1.2 | 0.697 | 3.9 ± 1.3 | 5.5 ± 1.2 | <0.001 |
| Liver Stiffness (kPa) | 6.2 ± 3 | 6.1 ± 3.8 | 0.298 | 5.7 ± 2.7 | 5.4 ± 1.3 | 0.763 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cossiga, V.; Lembo, V.; Guarino, M.; Tuccillo, C.; Morando, F.; Pontillo, G.; Fiorentino, A.; Caporaso, N.; Morisco, F. Berberis aristata, Elaeis guineensis and Coffea canephora Extracts Modulate the Insulin Receptor Expression and Improve Hepatic Steatosis in NAFLD Patients: A Pilot Clinical Trial. Nutrients 2019, 11, 3070. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123070
Cossiga V, Lembo V, Guarino M, Tuccillo C, Morando F, Pontillo G, Fiorentino A, Caporaso N, Morisco F. Berberis aristata, Elaeis guineensis and Coffea canephora Extracts Modulate the Insulin Receptor Expression and Improve Hepatic Steatosis in NAFLD Patients: A Pilot Clinical Trial. Nutrients. 2019; 11(12):3070. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123070
Chicago/Turabian StyleCossiga, Valentina, Vincenzo Lembo, Maria Guarino, Concetta Tuccillo, Federica Morando, Giuseppina Pontillo, Andrea Fiorentino, Nicola Caporaso, and Filomena Morisco. 2019. "Berberis aristata, Elaeis guineensis and Coffea canephora Extracts Modulate the Insulin Receptor Expression and Improve Hepatic Steatosis in NAFLD Patients: A Pilot Clinical Trial" Nutrients 11, no. 12: 3070. https://0-doi-org.brum.beds.ac.uk/10.3390/nu11123070