Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet

 , and
, and
Abstract
:1. Introduction
2. Material and Methods
Statistical Analysis
3. Results
3.1. Study Population
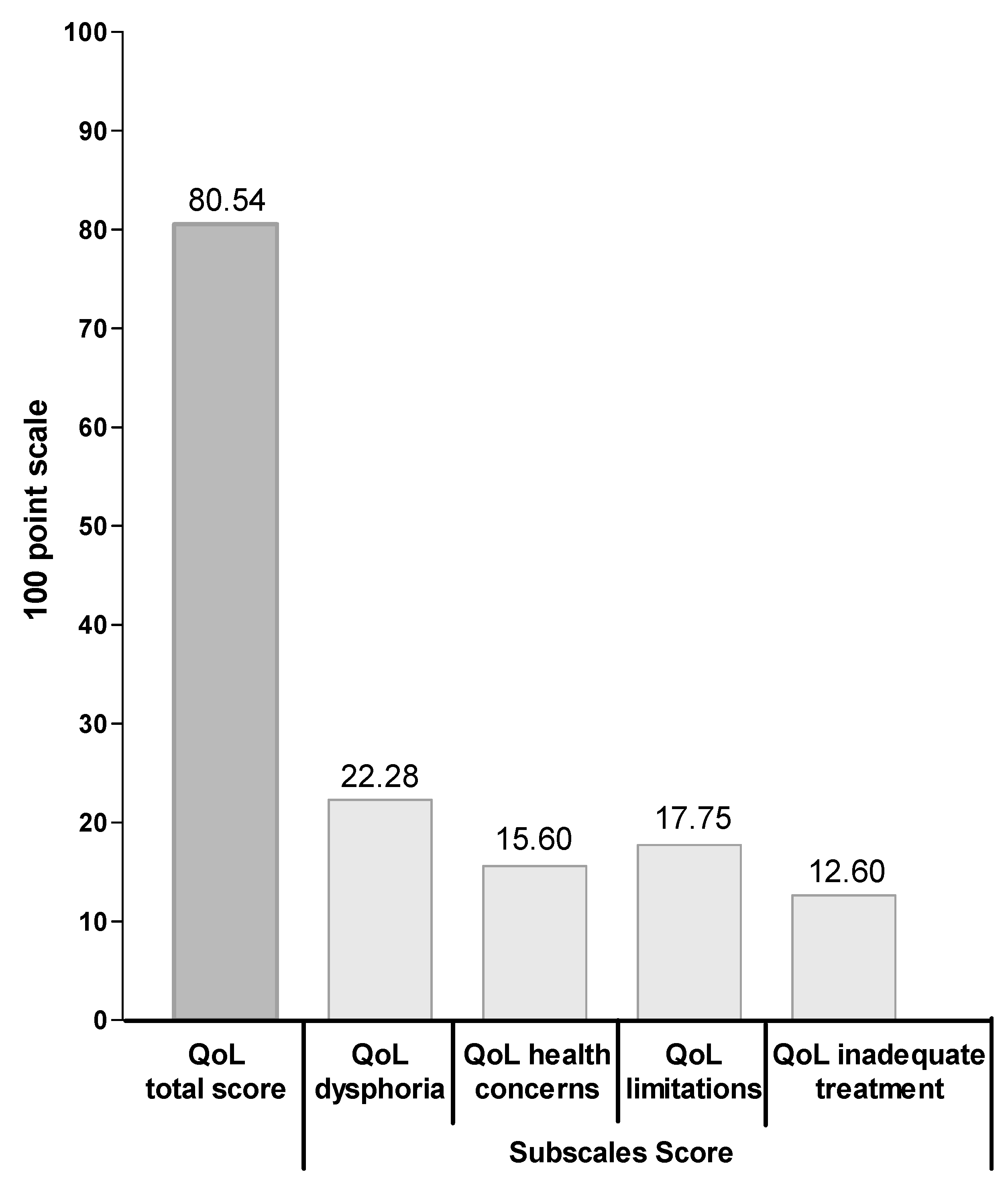
3.2. QoL Questionnaire
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Appendix A. CD-QoL Scale
| Statements | Not at All | A Little | Enough | Much | Very Much |
| 1. I feel limited by this disease | |||||
| 2. I feel worried that I will suffer from this disease | |||||
| 3. I fell concerned that this disease will cause other health problems | |||||
| 4. I feel worried about my increased risk of cancer from this disease | |||||
| 5. I feel socially stigmatized for having this disease | |||||
| 6. I feel like I’m limited in eating meals with co workers | |||||
| 7. I feel like I am not able to have special foods like birthday cake and pizza | |||||
| 8. I feel that the diet is insufficient treatment for my disease | |||||
| 9. I feel that there are not enough choices for treatment | |||||
| 10. I feel depressed because of my disease | |||||
| 11. I feel frightened by having this disease | |||||
| 12. I feel like I don’t know enough about the disease | |||||
| 13. I feel overwhelmed about having this disease | |||||
| 14. I have trouble socializing because of my disease | |||||
| 15. I find it difficult to travel or take long trips because of my disease | |||||
| 16. I feel like I cannot live a normal life because of my disease | |||||
| 17. I feel afraid to eat out because my food may be contaminated | |||||
| 18. I feel worried about the increased risk of one of my family members having celiac disease | |||||
| 19. I feel like I think about food all the time | |||||
| 20. I feel concerned that my long-term health will be affected |
References
- Balakireva, A.V.; Zamyatnin, J.A.A. Properties of Gluten Intolerance: Gluten Structure, Evolution, Pathogenicity and Detoxification Capabilities. Nutrients 2016, 8, 644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludvigsson, J.F.; Leffler, D.A.; Bai, J.C.; Biagi, F.; Fasano, A.; Green, P.H.R.; Hadjivassiliou, M.; Kaukinen, K.; Kelly, C.P.; Leonard, J.N.; et al. The Oslo definitions for coeliac disease and related terms. Gut 2012, 62, 43–52. [Google Scholar] [CrossRef]
- Al-Toma, A.; Volta, U.; Auricchio, R.; Castillejo, G.; Sanders, D.S.; Cellier, C.; Mulder, C.J.; Lundin, K.E. European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United Eur. Gastroenterol. J. 2019, 7, 583–613. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Murray, J.A. Epidemiology of Celiac Disease. Gastroenterol. Clin. N. Am. 2019, 48, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Catassi, C.; Gatti, S.; Fasano, A. The New Epidemiology of Celiac Disease. J. Pediatr. Gastroenterol. Nutr. 2014, 59, S7–S9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, J.M. Diagnosis of Celiac Disease: Taking a Bite out of the Controversy. Dig. Dis. Sci. 2018, 63, 1384–1391. [Google Scholar] [CrossRef]
- Leffler, D.A.; Green, P.H.R.; Fasano, A. Extraintestinal manifestations of coeliac disease. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 561–571. [Google Scholar] [CrossRef]
- Pinto-Sanchez, M.I.; Bai, J.C. Toward New Paradigms in the Follow up of Adult Patients with Celiac Disease on a Gluten-Free Diet. Front. Nutr. 2019, 6, 153. [Google Scholar] [CrossRef]
- Rodríguez-Almagro, J.; Almagro, D.R.; Ruíz, C.S.; Siles-González, J.; Martinez, A.H. The Experience of Living with a Gluten-Free Diet. Gastroenterol. Nurs. 2018, 41, 189–200. [Google Scholar] [CrossRef]
- White, L.E.; Bannerman, E.; Gillett, P.M. Coeliac disease and the gluten-free diet: A review of the burdens; factors associated with adherence and impact on health-related quality of life, with specific focus on adolescence. J. Hum. Nutr. Diet. 2016, 29, 593–606. [Google Scholar] [CrossRef]
- Burger, J.; De Brouwer, B.; IntHout, J.; Wahab, P.J.; Tummers, M.; Drenth, J.P.H. Systematic review with meta-analysis: Dietary adherence influences normalization of health-related quality of life in coeliac disease. Clin. Nutr. 2017, 36, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, V.; Kurppa, K.; Huhtala, H.; Mäki, M.; Kekkonen, L.; Kaukinen, K. Delayed celiac disease diagnosis predisposes to reduced quality of life and incremental use of health care services and medicines: A prospective nationwide study. United Eur. Gastroenterol. J. 2018, 6, 567–575. [Google Scholar] [CrossRef]
- Vilppula, A.; Kaukinen, K.; Luostarinen, L.; Krekelä, I.; Patrikainen, H.; Valve, R.; Luostarinen, M.; Laurila, K.; Mäki, M.; Collin, P. Clinical benefit of gluten-free diet in screen-detected older celiac disease patients. BMC Gastroenterol. 2011, 11, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ukkola, A.; Mäki, M.; Kurppa, K.; Collin, P.; Huhtala, H.; Kekkonen, L.; Kaukinen, K. Diet Improves Perception of Health and Well-being in Symptomatic, but Not Asymptomatic, Patients with Celiac Disease. Clin. Gastroenterol. Hepatol. 2011, 9, 118–123.e1. [Google Scholar] [CrossRef]
- Hallert, C.; Sandlund, O.; Broqvist, M. Perceptions of health-related quality of life of men and women living with coeliac disease. Scand. J. Caring Sci. 2003, 17, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Dorn, S.D.; Hernandez, L.; Minaya, M.T.; Morris, C.B.; Hu, Y.; Leserman, J.; Lewis, S.; Lee, A.; Bangdiwala, S.I.; Green, P.H.R.; et al. The development and validation of a new coeliac disease quality of life survey (CD-QOL). Aliment. Pharmacol. Ther. 2010, 31, 666–675. [Google Scholar] [CrossRef]
- Zingone, F.; Iavarone, A.; Tortora, R.; Imperatore, N.; Pellegrini, L.; Russo, T.; Dorn, S.D.; Ciacci, C. The Italian translation of the Celiac Disease-specific Quality of Life Scale in celiac patients on gluten free diet. Dig. Liver Dis. 2013, 45, 115–118. [Google Scholar] [CrossRef]
- Biagi, F.; Bianchi, P.I.; Marchese, A.; Trotta, L.; Vattiato, C.; Balduzzi, D.; Brusco, G.; Andrealli, A.; Cisarò, F.; Astegiano, M.; et al. A score that verifies adherence to a gluten-free diet: A cross-sectional, multicentre validation in real clinical life. Br. J. Nutr. 2012, 108, 1884–1888. [Google Scholar] [CrossRef]
- Zingone, F.; Swift, G.L.; Card, T.; Sanders, D.S.; Ludvigsson, J.F.; Bai, J.C. Psychological morbidity of celiac disease: A review of the literature. United Eur. Gastroenterol. J. 2014, 3, 136–145. [Google Scholar] [CrossRef]
- Ludvigsson, J.F.; Card, T.; Ciclitira, P.J.; Swift, G.L.; Nasr, I.; Sanders, D.S.; Ciacci, C. Support for patients with celiac disease: A literature review. United Eur. Gastroenterol. J. 2014, 3, 146–159. [Google Scholar] [CrossRef]
- Shah, S.; Akbari, M.; Vanga, R.; Kelly, C.P.; Hansen, J.; Theethira, T.; Tariq, S.; Dennis, M.; Leffler, D.A. Patient Perception of Treatment Burden Is High in Celiac Disease Compared with Other Common Conditions. Am. J. Gastroenterol. 2014, 109, 1304–1311. [Google Scholar] [CrossRef] [Green Version]
- Häuser, W.; Gold, J.; Stallmach, A.; Caspary, W.F.; Stein, J. Development and Validation of the Celiac Disease Questionnaire (CDQ), a Disease-specific Health-related Quality of Life Measure for Adult Patients with Celiac Disease. J. Clin. Gastroenterol. 2007, 41, 157–166. [Google Scholar] [CrossRef]
- Crocker, H.; Jenkinson, C.; Peters, M. Quality of life in coeliac disease: Item reduction, scale development and psychometric evaluation of the Coeliac Disease Assessment Questionnaire (CDAQ). Aliment. Pharmacol. Ther. 2018, 48, 852–862. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Schiepatti, A.; Malamut, G.; Marchese, A.; Cellier, C.; Bakker, S.F.; Mulder, C.J.J.; Volta, U.; Zingone, F.; Ciacci, C.; et al. PROgnosticating COeliac patieNts SUrvivaL: The PROCONSUL Score. PLoS ONE 2014, 9, e84163. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Schiepatti, A.; Maiorano, G.; Fraternale, G.; Agazzi, S.; Zingone, F.; Ciacci, C.; Volta, U.; Caio, G.; Tortora, R.; et al. Risk of complications in coeliac patients depends on age at diagnosis and type of clinical presentation. Dig. Liver Dis. 2018, 50, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Deepak, C.; Berry, N.; Vaiphei, K.; Dhaka, N.; Sinha, S.K.; Kochhar, R. Quality of life in celiac disease and the effect of gluten-free diet. JGH Open 2018, 2, 124–128. [Google Scholar] [CrossRef]
- Usai, P.; Minerba, L.; Marini, B.; Cossu, R.; Spada, S.; Carpiniello, B.; Cuomo, R.; Boy, M.F. Case control study on health-related quality of life in adult coeliac disease. Dig. Liver Dis. 2002, 34, 547–552. [Google Scholar] [CrossRef]
- Collin, P.; Vilppula, A.; Luostarinen, L.; Holmes, G.K.T.; Kaukinen, K. Review article: Coeliac disease in later life must not be missed. Aliment. Pharmacol. Ther. 2018, 47, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Zingone, F.; D’Odorico, A.; Lorenzon, G.; Marsilio, I.; Farinati, F.; Savarino, E.V. Risk of COVID-19 in celiac disease patients. Autoimmun. Rev. 2020, 102639. [Google Scholar] [CrossRef]
- Siniscalchi, M.; Zingone, F.; Savarino, E.V.; D’Odorico, A.; Ciacci, C. COVID-19 pandemic perception in adults with celiac disease: An impulse to implement the use of telemedicine. Dig. Liver Dis. 2020. [Google Scholar] [CrossRef]
- Nachman, F.; Del Campo, M.P.; Gonzalez, A.; Corzo, L.; Vázquez, H.; Sfoggia, C.; Smecuol, E.; Pinto-Sanchez, M.I.; Niveloni, S.; Sugai, E.; et al. Long-term deterioration of quality of life in adult patients with celiac disease is associated with treatment noncompliance. Dig. Liver Dis. 2010, 42, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Barratt, S.M.; Leeds, J.S.; Sanders, D.S. Quality of life in Coeliac Disease is determined by perceived degree of difficulty adhering to a gluten-free diet, not the level of dietary adherence ultimately achieved. J. Gastrointest. Liver Dis. 2011, 20, 241–245. [Google Scholar]
- Hopman, E.; Koopman, H.M.; Wit, J.M.; Mearin, M.L. Dietary compliance and health-related quality of life in patients with coeliac disease. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Zarkadas, M.; Cranney, A.; Case, S.; Molloy, M.; Switzer, C.; Graham, I.D.; Butzner, J.D.; Rashid, M.; Warren, R.E.; Burrows, V. The impact of a gluten-free diet on adults with coeliac disease: Results of a national survey. J. Hum. Nutr. Diet. 2006, 19, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Zarkadas, M.; Dubois, S.; MacIsaac, K.; Cantin, I.; Rashid, M.; Roberts, K.C.; La Vieille, S.; Godefroy, S.; Pulido, O.M. Living with coeliac disease and a gluten-free diet: A Canadian perspective. J. Hum. Nutr. Diet. 2012, 26, 10–23. [Google Scholar] [CrossRef]
- Ford, S.; Howard, R.; Oyebode, J.R. Psychosocial aspects of coeliac disease: A cross-sectional survey of a UK population. Br. J. Health Psychol. 2012, 17, 743–757. [Google Scholar] [CrossRef] [Green Version]
- Clappison, E.; Hadjivassiliou, M.; Zis, P. Psychiatric Manifestations of Coeliac Disease, a Systematic Review and Meta-Analysis. Nutrients 2020, 12, 142. [Google Scholar] [CrossRef] [Green Version]
- Paavola, A.; Kurppa, K.; Ukkola, A.; Collin, P.; Lähdeaho, M.-L.; Huhtala, H.; Mäki, M.; Kaukinen, K. Gastrointestinal symptoms and quality of life in screen-detected celiac disease. Dig. Liver Dis. 2012, 44, 814–818. [Google Scholar] [CrossRef]
- Jacobsson, L.R.; Hallert, C.; Milberg, A.; Friedrichsen, M. Coeliac disease—Women’s experiences in everyday life. J. Clin. Nurs. 2012, 21, 3442–3450. [Google Scholar] [CrossRef]
- Hallert, C.; Grännö, C.; Hultén, S.; Midhagen, G.; Ström, M.; Svensson, H.; Valdimarsson, T. Living with coeliac disease: Controlled study of the burden of illness. Scand. J. Gastroenterol. 2002, 37, 39–42. [Google Scholar] [CrossRef]
- Ciacci, C.; D’Agate, C.; De Rosa, A.; Franzese, C.; Errichiello, S.; Gasperi, V.; Pardi, A.; Quagliata, D.; Visentini, S.; Greco, L. Self-Rated Quality of Life in Celiac Disease. Dig. Dis. Sci. 2003, 48, 2216–2220. [Google Scholar] [CrossRef] [PubMed]
- Gerasimidis, K.; Zafeiropoulou, K.; Mackinder, M.; Ijaz, U.Z.; Duncan, H.; Buchanan, E.; Cardigan, T.; Edwards, C.A.; McGrogan, P.; Russell, R. Comparison of Clinical Methods with the Faecal Gluten Immunogenic Peptide to Assess Gluten Intake in Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, 356–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Coeliac Disease Population Characteristic | |
|---|---|
| N° | 100 |
| Female gender | 86 |
| Age at time of testing (mean (SD)) | 39.73 (13.51) |
| Age at CD diagnosis, yrs (mean (SD)) Age at DIA ˃ 35 yrs (n° patients) | 33.09 (12.92) 40 |
| Yrs from DIA (mean (SD)) Yrs from DIA ˃ 5 yrs (n° patients) | 6.64 (6.39) 39 |
| CD presentation (n° patients) | |
| Classical CD Only anaemia Non-classical CD Asymptomatic | 43 16 32 9 |
| tTG-IgA antibody at DIA (n° patients) | |
| Negative Positive | 2 98 |
| tTG-IgA antibody at FU (n° patients) | |
| Negative Positive | 85 15 |
| CD-QoL | Time DIA | P ° | Age DIA | P ° | Biagi Score | P ° | Gender | P | Symptoms | P ° | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ≤5 yrs | >5 yrs | ≤35 yrs | >35 yrs | Non-Adherent | Adherent | M | F | Other | Classic | ||||||
| CD-QoL * total | 80.7 | 80.3 | 0.88 | 81.5 | 79.1 | 0.32 | 73.7 | 81.2 | 0.07 | 80.6 | 80.5 | 0.97 | 81.3 | 79.5 | 0.46 |
| Low | 34.4% | 35.9% | 0.79 | 35% | 35% | 0.66 | 55.6% | 33% | 0.28 | 28.6% | 36.1% | 0.64 | 31.6% | 39.5% | 0.11 |
| Medium | 31.2% | 35.9% | 30% | 37.5% | 33.3% | 33% | 28.6% | 33.7% | 28.1% | 39.5% | |||||
| High | 34.4% | 28.2% | 35% | 27.5% | 11.1% | 34% | 42.8% | 30.2% | 40.3% | 21% | |||||
| Dysphoria * | 22.4 | 22.1 | 0.67 | 22.4 | 22.2 | 0.71 | 21.2 | 22.4 | 0.3 | 22.2 | 22.3 | 0.92 | 22.2 | 22.4 | 0.85 |
| Low | 36.1% | 38.5% | 0.55 | 35% | 40% | 0.76 | 66.7% | 34% | 0.05 | 28.6% | 38.4% | 0.46 | 35.1% | 39.5% | 0.55 |
| Medium | 31.2% | 38.5% | 33.3% | 35% | 0% | 37.4% | 28.6% | 34.9% | 31.6% | 37.2% | |||||
| High | 32.7% | 23% | 31.7% | 25% | 33.3% | 28.6% | 42.8% | 26.7% | 33.3% | 23.3% | |||||
| Health concerns * | 15.7 | 15.5 | 0.78 | 16.2 | 14.7 | 0.03 | 13.8 | 15.8 | 0.09 | 15.7 | 15.6 | 0.87 | 16.1 | 15 | 0.13 |
| Low | 39.3% | 48.8% | 0.62 | 35% | 55% | 0.13 | 55.6% | 41.8% | 0.10 | 57.1% | 40.7% | 0.19 | 36.8% | 51.2% | 0.35 |
| Medium | 27.9% | 25.6% | 30% | 22.5% | 44.4% | 25.3% | 7.2% | 30.2% | 29.8% | 23.3% | |||||
| High | 32.8% | 25.6% | 35% | 22.5% | 0% | 32.9% | 35.7% | 29.1% | 33.4% | 25.5% | |||||
| Limitations * | 17.8 | 17.6 | 0.87 | 17.8 | 17.5 | 0.68 | 16 | 17. 9 | 0.17 | 17.2 | 17.8 | 0.60 | 17.9 | 17.4 | 0.47 |
| Low | 36.1% | 30.8% | 0.25 | 35% | 32.5% | 0.96 | 44.4% | 32.9% | 0.73 | 42.9% | 32.6% | 0.61 | 29.8% | 39.5% | 0.25 |
| Medium | 27.8% | 43.6% | 33.3% | 35% | 33.3% | 34.2% | 35.7% | 33.7% | 31.6% | 37.2% | |||||
| High | 36.1% | 25.6% | 31.7% | 32.5% | 22.3% | 32.9% | 21.4% | 33.7% | 38.6% | 23.3% | |||||
| Inadequate treatment * | 12.5 | 12.8 | 0.51 | 12.7 | 12.5 | 0.64 | 11.8 | 12.7 | 0.32 | 12.9 | 12.6 | 0.61 | 12.6 | 12.5 | 0.83 |
| Low | 36.1% | 33.4% | 0.90 | 33.3% | 37.5% | 0.84 | 55.6% | 33% | 0.21 | 28.6% | 36.1% | 0.22 | 33.4% | 37.3% | 0.53 |
| Medium | 44.3% | 48.7% | 48.3% | 42.5% | 44.4% | 46.2% | 34.7% | 47.7% | 43.8% | 48.8% | |||||
| High | 19.6% | 17.9% | 18.4% | 20% | 0% | 20.8% | 35.7% | 16.2% | 22.8% | 13.9% | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marsilio, I.; Canova, C.; D’Odorico, A.; Ghisa, M.; Zingone, L.; Lorenzon, G.; Savarino, E.V.; Zingone, F. Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet. Nutrients 2020, 12, 2981. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102981
Marsilio I, Canova C, D’Odorico A, Ghisa M, Zingone L, Lorenzon G, Savarino EV, Zingone F. Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet. Nutrients. 2020; 12(10):2981. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102981
Chicago/Turabian StyleMarsilio, Ilaria, Cristina Canova, Anna D’Odorico, Matteo Ghisa, Letizia Zingone, Greta Lorenzon, Edoardo Vincenzo Savarino, and Fabiana Zingone. 2020. "Quality-of-Life Evaluation in Coeliac Patients on a Gluten-Free Diet" Nutrients 12, no. 10: 2981. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12102981