The Effect of Preoperative Carbohydrate Loading on Clinical and Biochemical Outcomes after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomized Trials

 , , , and
, , , and
Abstract
:1. Introduction
1.1. Preoperative Fasting
1.2. Oral Carbohydrate Loading
1.3. Specific Aims
2. Materials and Methods
2.1. Search Strategy and Inclusion Criteria
- (i)
- Randomized controlled trial,
- (ii)
- Populations containing >15 patients,
- (iii)
- Intervention comprising of oral carbohydrate loading maximum 2 h prior to surgery,
- (iv)
- Randomization to carbohydrate loading versus fasting/placebo (e.g., water),
- (v)
- Available meta-analyzable change score/endpoint data on any biochemical and clinical outcomes, in particular any of the following: surgical stress response (e.g., white blood cells count, C-reactive protein (CRP) concentration, proinflammatory cytokines levels), postoperative complications (e.g., postoperative nausea and vomiting, surgical site infection, GI tract complications, blood loss), non-surgical complications (e.g., pneumonia/urinary tract infections, delirium, antibiotic therapy duration, insulin treatment), mortality, ICU length of stay, inotropic drugs usage, time to extubation, atrial fibrillation and arrythmia.
2.2. Data Extraction
2.3. Outcomes
2.4. Data Synthesis and Statistical Analysis
2.5. Risk of Bias
2.6. GRADE (Grading of Recommendations, Assessment, Development and Evaluation)—Quality of Evidence Assessment
3. Results
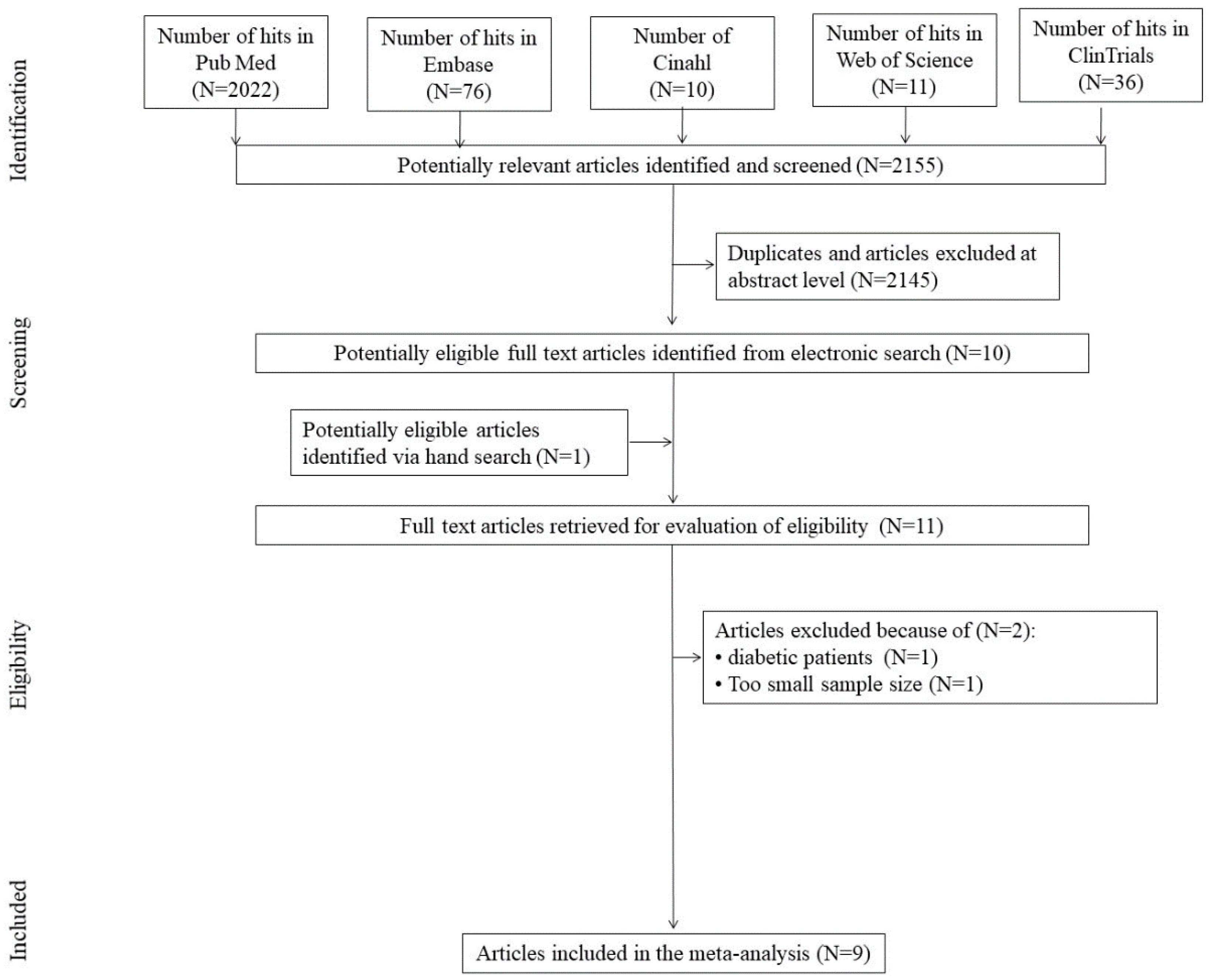
3.1. Search Results
3.2. Study, Patient and Treatment Characteristics
3.3. OCH Effects on Clinical and Biochemical Parameters
3.4. The Quality of Evidence Assessment (GRADE)
4. Discussion
4.1. Principal Findings
4.2. Results in the Context of other Meta-Analyses
4.3. Strengths of the Meta-Analysis
4.4. Limitations of the Meta-Analysis
4.5. Implication for Clinical Practice
4.6. Implications for Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| AAF | Acute atrial fibrillation |
| AC | Aortic clamping |
| AMI | Acute myocardial infarction |
| CABG | Coronary Artery Bypass Grafting |
| CABG with CPB | Coronary Artery Bypass Grafting with Cardio-Pulmonary Bypass |
| CPB | Cardio-Pulmonary Bypass |
| CRP | C-reactive protein |
| DB | Double blinding |
| DM | Differences in means |
| ERAS | Enhanced Recovery After Surgery |
| GA with ETT | General Anaesthesia with Endotracheal Intubation |
| GI | Gastrointestinal |
| GLN | Glutamine |
| ICU | Intensive care unit |
| LOS | Length of stay |
| OC | Observed cases |
| OCH | Oral carbohydrate |
| OPCAB | Off-Pump Coronary Artery Bypass Grafting |
| POAF | Postoperative atrial fibrillation |
| PONV | Post-operative nausea and vomiting |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCTs | Randomized controlled trials |
| ROB | Risk of bias |
| SB | Single blinding |
| SMD | Standardized mean difference |
| T2DM | Type 2 diabetes mellitus |
| VAS | Visual analog scale |
References
- Sato, H.; Carvalho, G.; Sato, T.; Lattermann, R.; Matsukawa, T.; Schricker, T. The association of preoperative glycemic control, intraoperative insulin sensitivity, and outcomes after cardiac surgery. J. Clin. Endocrinol. Metab. 2010, 95, 4338–4344. [Google Scholar] [CrossRef] [Green Version]
- Van Cromphaut, S.J. Hyperglycaemia as part of the stress response: The underlying mechanisms. Best Pract. Res. Clin. Anaesthesiol. 2009, 23, 375–386. [Google Scholar] [CrossRef]
- Kotfis, K.; Szylińska, A.; Listewnik, M.; Brykczyński, M.; Ely, E.W.; Rotter, I. Diabetes and elevated preoperative HbA1c level as risk factors for postoperative delirium after cardiac surgery: An observational cohort study. Neuropsychiatr. Dis. Treat. 2019, 15, 511–521. [Google Scholar] [CrossRef] [Green Version]
- Awad, S.; Constantin-Teodosiu, D.; Macdonald, I.A.; Lobo, D.N. Short-term starvation and mitochondrial dysfunction—A possible mechanism leading to postoperative insulin resistance. Clin. Nutr. 2009, 28, 497–509. [Google Scholar] [CrossRef]
- Czyż-Szypenbejl, K.; Mędrzycka-Dąbrowska, W.; Kwiecień-Jaguś, K.; Lewandowska, K. The Occurrence of Postoperative Cognitive Dysfunction (POCD)—Systematic Review. Występowanie zaburzeń poznawczych po zabiegach chirurgicznych przegląd systematyczny. Psychiatry Pol. 2019, 53, 145–160. [Google Scholar] [CrossRef]
- Koyfman, L.; Brotfain, E.; Erblat, A.; Kovalenko, I.; Reina, Y.Y.; Bichovsky, Y.; Borer, A.; Friger, M.; Frenkel, A.; Klein, M. The impact of the blood glucose levels of non-diabetic critically ill patients on their clinical outcome. Anaesthesiol. Intensive Ther. 2018, 50, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.W.; Allen, M.L.; Desai, A.; Macrae, D.; Pathan, N. Cardioprotective effects of insulin: How intensive insulin therapy may benefit cardiac surgery patients. Circulation 2012, 125, 721–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniyappa, R.; Montagnani, M.; Koh, K.K.; Quon, M.J. Cardiovascular actions of insulin. Endocr. Rev. 2007, 28, 463–491. [Google Scholar] [CrossRef] [PubMed]
- Furnary, A.P.; Wu, Y.; Bookin, S.O. Effect of hyperglycemia and continuous intravenous insulin infusions on outcomes of cardiac surgical procedures: The Portland Diabetic Project. Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2004, 10, 21–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Society of Anesthesiologists Committee. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: Application to healthy patients undergoing elective procedures: An updated report by the American society of anesthesiologists task force on preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration. Anesthesiology 2017, 126, 376–393. [Google Scholar]
- Bouvet, L.; Cercueil, E.; Barnoud, S.; Lilot, M.; Desgranges, F.-P.; Chassard, D. Relationship between the regurgitated and the aspirated volume of water. A manikin study. Anaesthesiol. Intensive Ther. 2019, 51, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Blaser, A.; Padar, M.; Tang, J.; Dutton, J.; Forbes, A. Citrulline and intestinal fatty acid-binding protein as biomarkers for gastrointestinal dysfunction in the critically ill. Anaesthesiol. Intensive Ther. 2019, 51, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Moonen, P.-J.; Blaser, A.R.; Starkopf, J.; Oudemans-van Straaten, H.M.; Van der Mullen, J.; Vermeulen, G.; Malbrain, M.L.N.G. The black box revelation: Monitoring gastrointestinal function. Anaesthesiol. Intensive Ther. 2018, 50, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Radtke, F.M.; Franck, M.; MacGuill, M.; Matthes, S.; Alawi, L.; Westhoff, S.; Neumann, U.; Wernecke, C.D.; Spies, C.D. Duration of fluid fasting and choice of analgesic are modifiable factors for early postoperative delirium. Eur J. Anaesthesiol. 2010, 27, 411–416. [Google Scholar] [CrossRef]
- Marra, A.; Kotfis, K.; Hosie, A.; MacLullich, A.M.; Pandharipande, P.P.; Ely, E.W.; Pun, B.T. Delirium Monitoring: Yes or No? That is the question. Am. J. Crit. Care 2019, 28, 127–135. [Google Scholar] [CrossRef]
- Kotfis, K.; Marra, A.; Ely, E.W. ICU delirium—A diagnostic and therapeutic challenge in the intensive care unit. Anaesthesiol. Intensive Ther. 2018, 50, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Reintam Blaser, A.; Starkopf, J.; Moonen, P.-J.; Malbrain, M.L.N.G.; Oudemans-van Straaten, H.M. Perioperative gastrointestinal problems in the ICU. Anaesthesiol. Intensive Ther. 2018, 50, 59–71. [Google Scholar] [CrossRef]
- Wu, C.L.; Benson, A.R.; Hobson, D.B.; Claro, P.D.; Demski, R.; Galante, D.J.; Pronovost, P.J.; Wick, E.C. Initiating an enhanced recovery pathway program: An anesthesiology department’s perspective. Jt. Comm. J. Qual. Patient Saf. 2015, 41, 447–456. [Google Scholar] [CrossRef]
- Wick, E.C.; Galante, D.J.; Hobson, D.B.; Benson, A.R.; Ken Lee, K.H.; Berenholtz, S.M.; Efron, J.E.; Pronovost, P.J.; Wu, C.L. Organizational culture changes result in improvement in patient-centered outcomes: Implementation of an integrated recovery pathway for surgical patients. J. Am. Coll. Surg. 2015, 221, 669–677. [Google Scholar] [CrossRef]
- Gupta, R.; Gan, T.J. Preoperative nutrition and prehabilitation. Anesthesiol. Clin. 2016, 34, 143–153. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced recovery after surgery: A review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Coleman, S.R.; Chen, M.; Patel, S.; Yan, H.; Kaye, A.D.; Zebrower, M.; Gayle, J.A.; Liu, H.; Urman, R.D. Enhanced recovery pathways for cardiac surgery. Curr. Pain Headache Rep. 2019, 23, 28. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.C.; Isada, T.; Ruzankin, P.; Whitman, G.; Lawton, J.S.; Dood, J.; Barodka, V. Results from an enhanced recovery program for cardiac surgery. J. Thorac. Cardiovasc. Surg. 2020, 159, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, J.; Gan, T.J.; Qin, G.; Wang, L.; Zhu, M.; Zhang, Z.; Pan, Y.; Ye, Z.; Zhang, F.; et al. Enhanced recovery after surgery pathway for patients undergoing cardiac surgery: A randomized clinical trial. Eur. J. Cardio. Thorac. Surg. Off. J. Eur. Assoc. Cardio. Thorac. Surg. 2018, 54, 491–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noss, C.; Prusinkiewicz, C.; Nelson, G.; Patel, P.A.; Augoustides, J.G.; Gregory, A.J. Enhanced recovery for cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2018, 32, 2760–2770. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Kaye, A.D.; Venakatesh, A.G.; Green, M.S.; Asgarian, C.D.; Luedi, M.M.; Liu, H. Enhanced recovery after cardiac surgery: An update on clinical implications. Int. Anesthesiol. Clin. 2017, 55, 148–162. [Google Scholar] [CrossRef] [PubMed]
- Krzych, Ł.; Kucewicz-Czech, E. It is time for enhanced recovery after surgery in cardiac surgery. Pol. Heart J. 2017, 75, 415–420. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.G.; Wang, Q.; Wang, W.J.; Quin, H.J. Randomized clinical trial to compare the effects of preoperative oral carbohydrate versus placebo on insulin resistance after colorectal surgery. Br. J. Surg. 2010, 97, 327. [Google Scholar] [CrossRef]
- Soop, M.; Nygren, J.; Myrenfors, P.; Thorell, A.; Ljungqvist, O. Preoperative oral carbohydrate treatment attenuates immediate postoperative insulin resistance. Am. J. Physiol. Endocrinol. Metab. 2001, 280, E576–E583. [Google Scholar] [CrossRef]
- Svanfeldt, M.; Thorell, A.; Hausel, J.; Soop, M.; Rooyackers, O.; Nygren, J.; Ljungqvist, O. Randomized clinical trial of the effect of preoperative oral carbohydrate treatment on postoperative whole-body protein and glucose kinetics. Br. J. Surg. 2007, 94, 1342–1350. [Google Scholar] [CrossRef]
- Yuill, K.A.; Richardson, R.A.; Davidson, H.I.M.; Garden, O.J.; Parks, R.W. The administration of an oral carbohydrate-containing fluid prior to major elective upper-gastrointestinal surgery preserves skeletal muscle mass postoperatively—A randomised clinical trial. Clin. Nutr. 2005, 24, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Constantin-Teodosiu, D.; Constantin, D.; Rowlands, B.J.; Fearon, K.C.; Macdonald, I.A.; Lobo, D.N. Cellular mechanisms underlying the protective effects of preoperative feeding. Ann. Surg. 2010, 252, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Blackshaw, P.E.; Wright, J.W.; Macdonald, I.A.; Perkins, A.C.; Lobo, D.N. A randomized crossover study of the effects of glutamine and lipid on the gastric emptying time of a preoperative carbohydrate drink. Clin. Nutr. 2011, 30, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Awad, S.; Fearon, K.C.H.; Macdonald, I.A.; Lobo, D.N. A randomized cross-over study of the metabolic and hormonal responses following two preoperative conditioning drinks. Nutrition 2011, 27, 938–942. [Google Scholar] [CrossRef]
- Melis, G.C.; van Leeuwen, P.A.M.; von Blomberg-van der Flier, B.M.E.; Goedhart-Hiddinga, A.C.; Uitdehaag, B.M.; van Schijndel, R.J.; Wuisman, P.I.J.M.; van Bokhorst-de van der Schueren, M.A.E. A carbohydrate-rich beverage prior to surgery prevents surgery-induced immunodepression: A randomized, controlled, clinical trial. J. Parenter. Enter. Nutr. 2006, 30, 21–26. [Google Scholar] [CrossRef]
- Li, L.; Wang, Z.; Ying, X.; Tian, J.; Sun, T.; Yi, K.; Zhang, P.; Zhang, J.; Yang, K. Preoperative carbohydrate loading for elective surgery: A systematic review and meta-analysis. Surg. Today 2012, 42, 613–624. [Google Scholar] [CrossRef]
- Hausel, J.; Nygren, J.; Lagerkranser, M.; Hellström, P.M.; Hammarqvist, F.; Almström, C.; Lindh, A.; Thorell, A.; Ljungqvist, O. A carbohydrate-rich drink reduces preoperative discomfort in elective surgery patients. Anesth. Analg. 2001, 93, 1344. [Google Scholar] [CrossRef] [Green Version]
- Nygren, J.; Thorell, A.; Ljungqvist, O. Preoperative oral carbohydrate nutrition: An update. Curr. Opin. Clin. Nutr. Metab. Care 2001, 4, 255–2559. [Google Scholar] [CrossRef]
- Brady, M.; Kinn, S.; Stuart, P. Preoperative fasting for adults to prevent perioperative complications. Cochrane Database Syst. Rev. 2003, 4. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.; et al. ESPEN guideline: Clinical nutrition in surgery. Clin. Nutr. 2017, 36, 623–650. [Google Scholar] [CrossRef] [Green Version]
- Vermeulen, M.A.R.; Richir, M.C.; Garretsen, M.K.; van Schie, A.; Ghatei, M.A.; Holst, J.J.; Heijboer, A.C.; Uitdehaag, B.M.J.; Diamant, M.; Eekhoff, E.M.W.; et al. Gastric emptying, glucose metabolism and gut hormones: Evaluation of a common preoperative carbohydrate beverage. Nutrition 2011, 27, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Dock-Nascimento, D.B.; de Aguilar-Nascimento, J.E.; Magalhaes Faria, M.S.; Caporossi, C.; Slhessarenko, N.; Waitzberg, D.L. Evaluation of the effects of a preoperative 2-hour fast with maltodextrine and glutamine on insulin resistance, acute-phase response, nitrogen balance, and serum glutathione after laparoscopic cholecystectomy: A controlled randomized trial. J. Parenter. Enter. Nutr. 2012, 36, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Braga, M.; Bissolati, M.; Rocchetti, S.; Beneduce, A.; Pecorelli, N.; Di Carlo, V. Oral preoperative antioxidants in pancreatic surgery: A double-blind, randomized, clinical trial. Nutrition 2012, 28, 160–164. [Google Scholar] [CrossRef] [PubMed]
- Soop, M.; Nygren, J.; Thorell, A.; Weidenhielm, L.; Lundberg, M.; Hammarqvist, F.; Ljungqvist, O. Preoperative oral carbohydrate treatment attenuates endogenous glucose release 3 days after surgery. Clin. Nutr. 2004, 23, 733–741. [Google Scholar] [CrossRef]
- Tran, S.; Wolever, T.M.S.; Errett, L.E.; Ahn, H.; Mazer, C.D.; Keith, M. Preoperative carbohydrate loading in patients undergoing coronary artery bypass or spinal surgery. Anesth. Analg. 2013, 117, 305–313. [Google Scholar] [CrossRef] [Green Version]
- PRISMA. Available online: http://www.prisma-statement.org/Protocols/ (accessed on 19 March 2020).
- Şavluk, Ö.F.; Kuşçu, M.A.; Güzelmeriç, F.; Gurcu, M.E.; Erkilinc, A.; Cevirme, D.; Kocak, T. Do preoperative oral carbohydrates improve postoperative outcomesin patients undergoing coronary artery bypass grafts? Turk. J. Med Sci. 2017, 47, 1681–1686. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Duval, S.; Tweedie, R. A nonparametric “Trim and Fill” method of accounting for publication bias in meta-analysis. J. Am. Stat. Assoc. 2000, 449, 89–98. [Google Scholar] [CrossRef]
- GRADE Handbook. Available online: https://gdt.gradepro.org/app/handbook/handbook.html (accessed on 25 September 2020).
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H.; et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef] [PubMed]
- Feguri, G.R.; de Lima, P.R.L.; de Cerqueira Borges, D.; Toledo, L.R.; Batista, L.N.; Carvalho e Silva, T.; Segri, N.J.; de Aguilar-Nascimento, J.E. Preoperative carbohydrate load and intraoperatively infused omega-3 polyunsaturated fatty acids positively impact nosocomial morbidity after coronary artery bypass grafting: A double-blind controlled randomized trial. Nutr. J. 2017, 16, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feguri, G.R.; Lima, P.R.L.; de Franco, A.C.; de la Cruz, F.R.H.; Borges, D.C.; Toledo, L.R.; Segri, N.J.; de Aguilar-Nascimento, J.E. Benefits of fasting abbreviation with carbohydrates and omega-3 infusion during cabg: A double-blind controlled randomized trial. Braz. J. Cardiovasc. Surg. 2019, 34, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Feguri, G.R.; Lima, P.R.L.; Lopes, A.M.; Roledo, A.; Marchese, M.; Trevisan, M.; Ahmad, H.; de Freitas, B.B.; de Aguilar-Nascimento, J.E. Clinical and metabolic results of fasting abbreviation with carbohydrates in coronary artery bypass graft surgery. Braz. J. Cardiovasc. Surg. 2012, 27, 7–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Järvelä, K.; Maaranen, P.; Sisto, T. Pre-operative oral carbohydrate treatment before coronary artery bypass surgery. Acta Anaesthesiol. Scand. 2008, 52, 793–797. [Google Scholar] [CrossRef]
- Rapp-Kesek, D.; Stridsberg, M.; Andersson, L.-G.; Berne, C.; Karlsson, T. Insulin resistance after cardiopulmonary bypass in the elderly patient. Scand. Cardiovasc. J. Sci. 2007, 41, 102–108. [Google Scholar] [CrossRef]
- Lee, B.; Soh, S.; Shim, J.-K.; Kim, H.Y.; Lee, H.; Kwak, Y.-L. Evaluation of preoperative oral carbohydrate administration on insulin resistance in off-pump coronary artery bypass patients: A randomised trial. Eur. J. Anaesthesiol. 2017, 34, 740–747. [Google Scholar] [CrossRef]
- Sokolic, J.; Knezevic, D.; Kuharic, J.; Medved, I.; Sustic, A.; Zupan, Z.; Laskarin, G.; Tadin, T.; Tokmadžić, V.S. Decrease of perforin expressing lymphocytes after on-pump coronary artery bypass grafting surgery irrespective of carbohydrate preoperative oral feeding. Heart Surg. Forum 2019, 22, E218. [Google Scholar] [CrossRef] [Green Version]
- Amer, M.A.; Smith, M.D.; Herbison, G.P.; Plank, L.D.; McCall, J.L. Network meta-analysis of the effect of preoperative carbohydrate loading on recovery after elective surgery. Br. J. Surg. 2017, 104, 187–197. [Google Scholar] [CrossRef]
- Breuer, J.-P.; von Dossow, V.; von Heymann, C.; Griesbach, M.; von Schickfus, M.; Mackh, E.; Hacker, C.; Elgeti, U.; Konertz, W.; Wernecke, K.D.; et al. Preoperative oral carbohydrate administration to ASA III-IV patients undergoing elective cardiac surgery. Anesth. Analg. 2006, 103, 1099–1108. [Google Scholar] [CrossRef]
- Awad, S.; Varadhan, K.K.; Ljungqvist, O.; Lobo, D.N. A meta-analysis of randomised controlled trials on preoperative oral carbohydrate treatment in elective surgery. Clin. Nutr. 2013, 32, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.K.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for perioperative care in cardiac surgery: Enhanced recovery after surgery society recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Kehlet, H.; Wilmore, D.W. Multimodal strategies to improve surgical outcome. Am. J. Surg. 2002, 183, 630–641. [Google Scholar] [CrossRef]
- de-Aguilar-Nascimento, J.E.; Salomão, A.B.; Waitzberg, D.L.; Dock-Nascimento, D.B.; Correa, M.I.T.D.; Campos, A.C.L.; Corsi, P.R.; Filho, P.E.P.; Caporossi, C. ACERTO guidelines of perioperative nutritional interventions in elective general surgery. Revista Colégio Brasileiro Cirurgiões. 2017, 44, 633–648. [Google Scholar] [CrossRef] [Green Version]
- Ban, K.A.; Berian, J.R.; Ko, C.Y. Does implementation of enhanced recovery after surgery (ERAS) protocols in colorectal surgery improve patient outcomes? Clin. Colon Rectal Surg. 2019, 32, 109–113. [Google Scholar] [CrossRef]
- van der Geest, L.G.M.; Lemmens, V.E.P.P.; de Hingh, I.H.J.T.; van Laarhoven, C.J.H.M.; Bollen, T.L.; Nio, C.Y.; van Eijck, C.H.J.; Busch, O.R.C.; Besselink, M.G.H. Nationwide outcomes in patients undergoing surgical exploration without resection for pancreatic cancer. Br. J. Surg. 2017, 104, 1568–1577. [Google Scholar] [CrossRef]
- Ueland, W.; Walsh-Blackmore, S.; Nisiewicz, M.; Davenport, D.L.; Plymale, M.A.; Plymale, M.; Roth, J.S. The contribution of specific enhanced recovery after surgery (ERAS) protocol elements to reduced length of hospital stay after ventral hernia repair. Surg. Endosc. 2019, 34. [Google Scholar] [CrossRef]
- Amirshahi, M.; Behnamfar, N.; Badakhsh, M.; Rafiemanesh, H.; Keikhaie, K.R.; Sheyback, M.; Sari, M. Prevalence of postoperative nausea and vomiting: A systematic review and meta-analysis. Saudi J. Anaesth. 2020, 14, 48. [Google Scholar] [CrossRef]
- Champion, S.; Zieger, L.; Hemery, C. Prophylaxis of postoperative nausea and vomiting after cardiac surgery in high-risk patients: A randomized controlled study. Ann. Card. Anaesth. 2018, 21, 8–14. [Google Scholar] [CrossRef]
- Apfel, C.C.; Läärä, E.; Koivuranta, M.; Greim, C.A.; Roewer, N. A simplified risk score for predicting postoperative nausea and vomiting: Conclusions from cross-validations between two centers. Anesthesiology 1999, 91, 693–700. [Google Scholar] [CrossRef] [Green Version]
- Koivuranta, M.; Läärä, E.; Snåre, L.; Alahuhta, S. A survey of postoperative nausea and vomiting. Anaesthesia 1997, 52, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Halkos, M.E.; Puskas, J.D.; Lattouf, O.M.; Kilgo, M.; Kerendi, F.; Song, H.K.; Guyton, R.A.; Thourani, V.H. Elevated preoperative hemoglobin A1c level is predictive of adverse events after coronary artery bypass surgery. J. Thorac. Cardiovasc. Surg. 2008, 136, 631–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, J.; Zoungas, S.; Wright, C.; Teede, H. Evidence-based guidelines for perioperative management of diabetes in cardiac and vascular surgery. World J. Surg. 2010, 34, 500–513. [Google Scholar] [CrossRef] [PubMed]
- Stoppe, C.; Goetzenich, A.; Whitman, G.; Ohkuma, R.; Brown, T.; Hatzakorzian, R.; Kristof, A.; Meybohm, P.; Mechanick, J.; Evans, A.; et al. Role of nutrition support in adult cardiac surgery: A consensus statement from an International Multidisciplinary Expert Group on Nutrition in Cardiac Surgery. Crit. Care 2017, 21. [Google Scholar] [CrossRef] [Green Version]
- Wernio, E.; Małgorzewicz, S.; Dardzińska, J.A.; Jagielak, D.; Rogowski, J.; Gruszecka, A.; Klapkowski, A.; Bramlage, P. Association between nutritional status and mortality after aortic valve replacement procedure in elderly with severe aortic stenosis. Nutrients 2019, 11, 446. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Overall Study Characteristics (First Author, Year, Country) | Study Design | Intervention | Patients Characteristics | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Blinding/ROB | Focus of the Study | Surgery Technique/Anesthesia | OCH Specification, % | Oral Dose, mL | Comparator | R/A (n) | Age—Years; Mean (SD); Median | Male, %/T2DM, % | ||
| 1 | Feguri et al., 2017, Brazil [54] | DB/6 | morbidity (especially POAF) in ICU patients | CABG with CPB/GA with ETT | 12.5 | 200 * | water | 30/28 | 62.1 (9.7) | 78.6/25 |
| 2 | Feguri et al., 2019, Brazil [55] | DB/6 | morbidity, blood glucose, inflammation, recovery | CABG with CPB/GA with ETT | 12.5 | 200 * | water | 62.1 (9.7) | 78.6/25 | |
| 3 | Feguri et al., 2012, Brazil [56] | DB/5 | perioperative glycemic control and IR of nondiabetic patients | CABG with CPB/GA with ETT | 12.5 | 600 † | water | 40/40 | 58.5 (7.2) | 65/0 |
| 4 | Jarvela et al., 2008, Finland [57] | OL/4 | perioperative insulin requirements in non-diabetic patients | CABG with CPB/GA with ETT | 12.5 | 400 * | fasting | 101/101 | 65.4 (10.2) | 83.2/0 |
| 5 | Lee et al., 2017, Korea [59] | OL/6 | insulin resistance and free-fatty acid (FFA) concentrations | OPCAB/GA with ETT | 12.8 | 800 ‡ | fasting | 60/57 | 64.5 (8.5) | 86/0 |
| 6 | Savluk et al., 2017a, Turkey [47] | OL/3 | postoperative insulin requirements, postoperative patient discomfort, inotropic support, length of the ICU stay, the duration of postoperative mechanical ventilation | CABG with CPB/GA with ETT | 12.5 | 1200 § | fasting | 77/77 | 58 (11.6) | 83/0 |
| Savluk et al., 2017b, Turkey [47] | CABG with CPB/GA with ETT | 12.5 | 400 ¶ | fasting | 76/76 | 57.5 (11.5) | 81.2/0 | |||
| Savluk et al., 2017c, Turkey [47] | CABG with CPB/GA with ETT | 12.5 | 400 * | fasting | 77/77 | 57 (11) | 81.8/0 | |||
| 7 | Sokolic et al., 2019a, Croatia [60] | OL/3 | frequency and perforin expression in peripheral blood lymphocytes | OPCAB/GA with ETT | 12.6 | 200* | fasting | 40/40 | 66 ‡‡; 67.5 §§ | 72.5/0 |
| Sokolic et al., 2019b, Croatia [60] | CABG with CPB/GA with ETT | 12.6 | fasting | 40/40 | 68.5 ‡‡; 66 §§ | 67.5/0 | ||||
| 8 | Tran et al., 2013, Canada [45] | OL/3 | glucose and insulin levels, insulin resistance, markers of inflammation (CRP, IL-6), FFA levels, time of mechanical ventilation, incidence of infection, blood transfusions, LOS in the ICU, LOS in the hospital, subjective feelings of discomfort (VAS) | CABG with CPB/GA with ETT | 12.5 | 1200 ** | fasting | 26/26 | 55 ‡‡; 59 §§ | 80.8/0 |
| 9 | Rapp-Kesek et al., 2007, Sweden [58] | OL/3 | Muscle strength, insulin resistance, stress hormone response | CABG with CPB/GA with ETT | 12.5 | 800 †† | fasting | 18/18 | 72 (1.4) | nd/0 |
| Outcomes | Treatment Group | Control Group | References | ||
|---|---|---|---|---|---|
| Cases | n | Cases | n | ||
| Bronchial aspiration during induction of anesthesia | 0 | 14 | 0 | 14 | Feguri et al., 2017, Brazil [54] |
| 0 | 14 | 0 | 14 | Feguri et al., 2019, Brazil [55] | |
| 0 | 20 | 0 | 20 | Feguri et al., 2012, Brazil [56] | |
| 0 | 50 | 0 | 51 | Jarvela et al., 2008, Finland [57] | |
| Stroke | 0 | 14 | 1 | 14 | Feguri et al., 2017, Brazil [54] |
| 0 | 20 | 0 | 20 | Feguri et al., 2012, Brazil [56] | |
| In-hospital mortality | 0 | 14 | 1 | 14 | Feguri et al., 2017, Brazil [54] |
| 0 | 20 | 0 | 20 | Feguri et al., 2012, Brazil [56] | |
| Thirst | 0 | 20 | 3 | 20 | Feguri et al., 2012, Brazil [56] |
| Acute atrial fibrillation | 6 | 14 | 8 | 14 | Feguri et al., 2019, Brazil [55] |
| Any post-surgery complication | nd | nd | 2 | 14 | Feguri et al., 2019, Brazil [55] |
| 8 | 28 | 12 | 29 | Lee et al., 2017, Korea [59] | |
| 34 † | 13 | 51 | 13 | Tran et al., 2013, Canada [45] | |
| Transfusion intra-operatively | 7 | 14 | 7 | 14 | Feguri et al., 2017, Brazil [54] |
| 6 | 28 | 4 | 29 | Lee et al., 2017, Korea [59] | |
| Transfusion post-operatively | 6 * | 14 | 5 | 14 | Feguri et al., 2017, Brazil [54] |
| Pneumonia | 3 | 14 | 3 | 14 | Feguri et al., 2019, Brazil [55] |
| 0 | 13 | 0 | 13 | Tran et al., 2013, Canada [45] | |
| Reoperation | 1 | 28 | 1 | 29 | Lee et al., 2017, Korea [59] |
| Any complication intra-operatively | 1 | 14 | 2 | 14 | Feguri et al., 2017, Brazil [54] |
| EVA (encephalic vascular accident) | 0 | 14 | 2 | 14 | Feguri et al., 2017, Brazil [54] |
| Outcomes | Treatment Group | Control Group | References/Country | ||
|---|---|---|---|---|---|
| Mean (SD); Median (IQR) | n | Mean (SD); Median (IQR) | n | ||
| Postoperative blood loss; mL | 820 (670; 1010) ^,† | 28 | 720(530; 830) ^,† | 29 | Lee et al., 2017, Korea [59] |
| Duration of mechanical ventilation; h | 10 (9; 10) ^ | 20 | 10 (10; 15) ^ | 20 | Sokolic et al., 2019a, Croatia [60] |
| 10 (10; 13.5) ^ | 20 | 9 (7.5; 10) ^ | 20 | Sokolic et al., 2019b, Croatia [60] | |
| 6 (4.1; 11.2) ^ | 13 | 6.7 (4.6; 12.5) ^ | 12 | Tran et al., 2009, Canada [45] | |
| Hospital length of stay; days | 8.42 (7.79) | 14 | 8.07 (4.5) | 14 | Feguri et al., 2017, Brazil [54] |
| 7.8 (1.4) | 20 | 9.7(3.1) | 20 | Feguri et al., 2012, Brazil [56] | |
| 11 (10; 14) ^ | 28 | 11 (0;14) | 29 | Lee et al., 2017, Korea [59] | |
| 4 (4; 5) ^ | 12 | 5 (5; 6) | 13 | Tran et al., 2009, Canada [45] | |
| ICU stay (hours) | 48 (48; 72) ^ | 28 | 72 (48; 72) ^ | 29 | Lee et al., 2017, Korea [59] |
| 24 (24; 48) ^ | 20 | 24 (24; 24) ^ | 20 | Sokolic et al., 2019a, Croatia [60] | |
| 24 (24; 24) ^ | 20 | 24 (24; 24) ^ | 20 | Sokolic et al., 2019b, Croatia [60] | |
| 21.3 (20.4; 22.9) ^ | 13 | 23.1 (21.8; 25.6) ^ | 12 | Tran et al., 2009, Canada [45] | |
| Duration of the surgery; min | 220 (197.5; 242.5) ^ | 13 | 220 (195; 240) ^ | 13 | Tran et al., 2009, Canada [45] |
| Postoperative blood transfusion; mL | 200 (0; 295) ^,† | 28 | 200 (0; 420) ^,† | 29 | Lee et al., 2017, Korea [59] |
| CPB duration; min | 59 (50.5; 81.5) ^ | 13 | 61 (51.8; 72.5) ^ | 12 | Tran et al., 2009, Canada [45] |
| Intra-operative gastric drainage; mL | 26.8 (57.9) | 50 | 16.3 (37.9) | 51 | Jarvela et al., 2008, Finland [57] |
| Post-operative gastric drainage; mL | 88.8(75.4) | 50 | 49.9 (63.4) | 51 | Jarvela et al., 2008, Finland [57] |
| Exogenous insulin intra-operatively; IU | 5.9 (5.7) | 20 | 7.5 (5) | 20 | Feguri et al., 2012, Brazil [56] |
| 0 | 28 | 0 | 29 | Lee et al., 2017, Korea [59] | |
| HOMA-IR endpoint | 11.2 (8.2) | 20 | 11.6 (7.6) | 20 | Feguri et al., 2012, Brazil [56] |
| 3.2 (0.9; 6.3) ^ | 12 | 1.8 (1.1; 3.8) ^ | 13 | Tran et al., 2013, Canada [45] | |
| 7.56 (1.48) ‡ | 9 | 7.2 (2.44) | 9 | Rapp-Kesek et al., 2007, Sweden [58] | |
| CRP endpoint; mg.dL−1 | 3.75 (nd) | 14 | 5.15 (nd) | 14 | Feguri et al., 2019, Brazil [55] |
| −0.25 (-0.47; 0.21) ^,§ | 10 | −0.1 (0.34; 0.39) ^,§ | 13 | Tran et al., 2013, Canada [45] | |
| IL-6 endpoint; pg·mL−1 | 1.92 (1.68–2.03) ^,§ | 7 | 1.79 (1.73; 1.91) ^,§ | 6 | Tran et al., 2013, Canada [45] |
| Blood glucose post-operatively; mmol·L−1 | 8.15 (nd) ¶,(a),(b) | 14 | 8.91 (nd) | 14 | Feguri et al., 2019, Brazil [55] |
| 6.44 (0.99) **,(a) | 50 | 6.32 (nd) | 51 | Jarvela et al., 2008, Finland [57] | |
| 7.8 (7.0; 8.2) ^,†† | 28 | 7.3 (7.8; 6.3) ^ | 29 | Lee et al., 2017, Korea [59] | |
| 6.7 (5.4; 7.1) ‡‡ | 13 | 6.6 (5.9; 8.1) ^ | 13 | Tran et al., 2013, Canada [45] | |
| 7.9 (0.5)‡ | 9 | 8.2 (0.7) | 9 | Rapp-Kesek et al., 2007, Sweden [58] | |
| Certainty Assessment | № of patients | Effect | Certainty | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| № of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | OCH Loading (Treatment) | Fasting or Water (Control) | Relative (95% CI) | Absolute (95% CI) | |
| AC duration (min) | |||||||||||
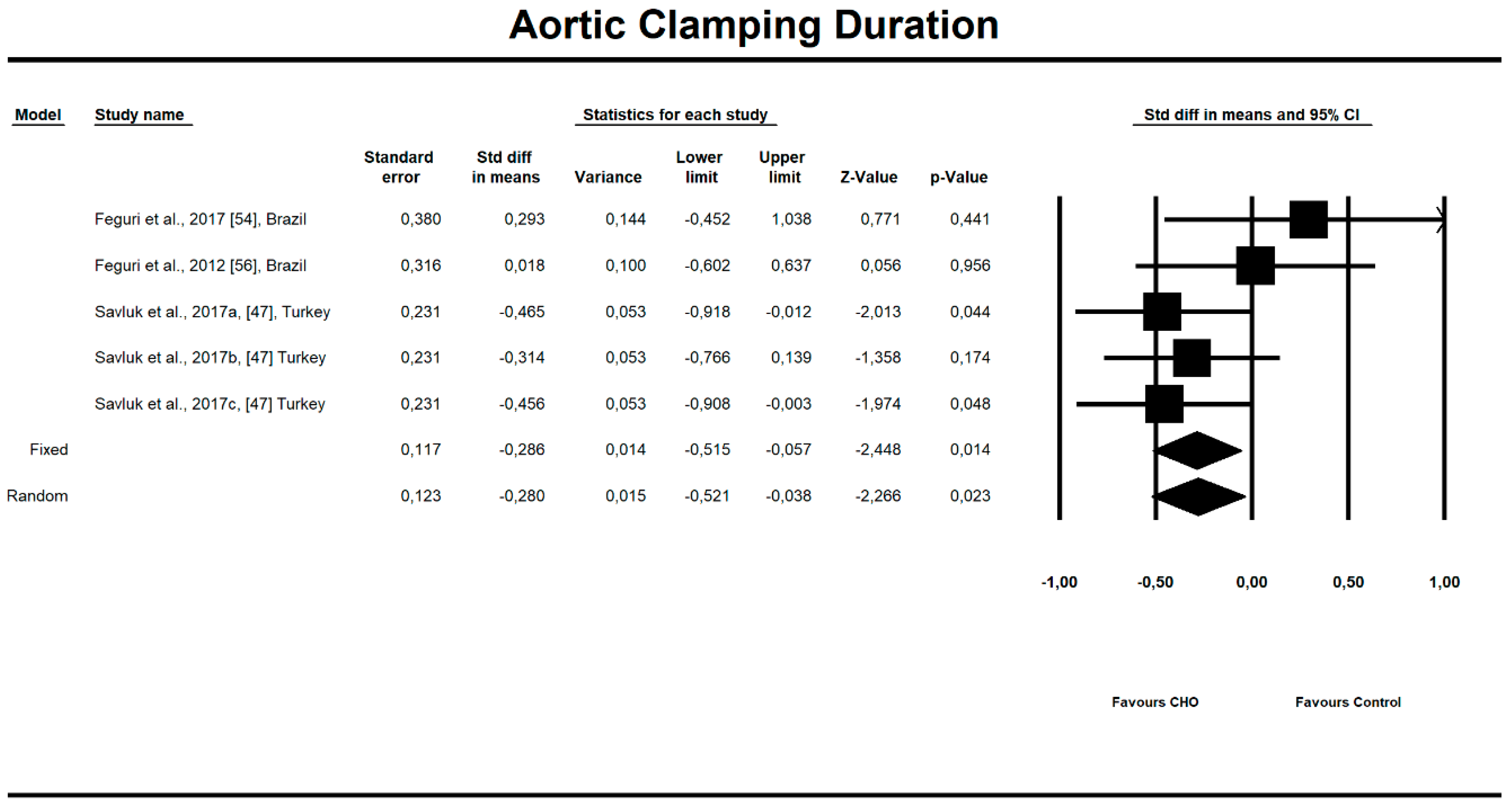
| 3 (5 interventions) | randomized trials | not serious a | not serious | not serious | not serious b | publication bias strongly suspected c | 147 | 73 | - | MD 6.388 lower (11.246 lower to 1.529 lower) | ⨁⨁⨁◯ MODERATE |
| ICU stay (hours) | |||||||||||
| 4 (6 interventions) | randomized trials | not serious d | serious e | not serious | not serious f | none | 197 | 124 | - | MD 25.925 SD lower (44.568 lower to 7.283 lower) | ⨁⨁⨁◯ MODERATE |
| Exogenous insulin postoperatively (IU) | |||||||||||
| 3 | randomized trials | not serious | not serious | not serious | serious g | none | 84 | 85 | - | MD 4.523 lower (8.417 lower to 0.63 lower) | ⨁⨁⨁◯ MODERATE |
| Inotropic drugs overall | |||||||||||
| 4 (6 interventions) | randomized trials | serious h | not serious | serious i | not serious | none | 82/174 (47.1%) | 51/101 (50.5%) | RR 0.795 (0.689 to 0.919) | 104 fewer per 1000 (from 157 fewer to 41 fewer) | ⨁⨁◯◯ LOW |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotfis, K.; Jamioł-Milc, D.; Skonieczna-Żydecka, K.; Folwarski, M.; Stachowska, E. The Effect of Preoperative Carbohydrate Loading on Clinical and Biochemical Outcomes after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomized Trials. Nutrients 2020, 12, 3105. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103105
Kotfis K, Jamioł-Milc D, Skonieczna-Żydecka K, Folwarski M, Stachowska E. The Effect of Preoperative Carbohydrate Loading on Clinical and Biochemical Outcomes after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomized Trials. Nutrients. 2020; 12(10):3105. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103105
Chicago/Turabian StyleKotfis, Katarzyna, Dominika Jamioł-Milc, Karolina Skonieczna-Żydecka, Marcin Folwarski, and Ewa Stachowska. 2020. "The Effect of Preoperative Carbohydrate Loading on Clinical and Biochemical Outcomes after Cardiac Surgery: A Systematic Review and Meta-Analysis of Randomized Trials" Nutrients 12, no. 10: 3105. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12103105