The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults



Abstract
:1. Introduction
2. Materials and Methods
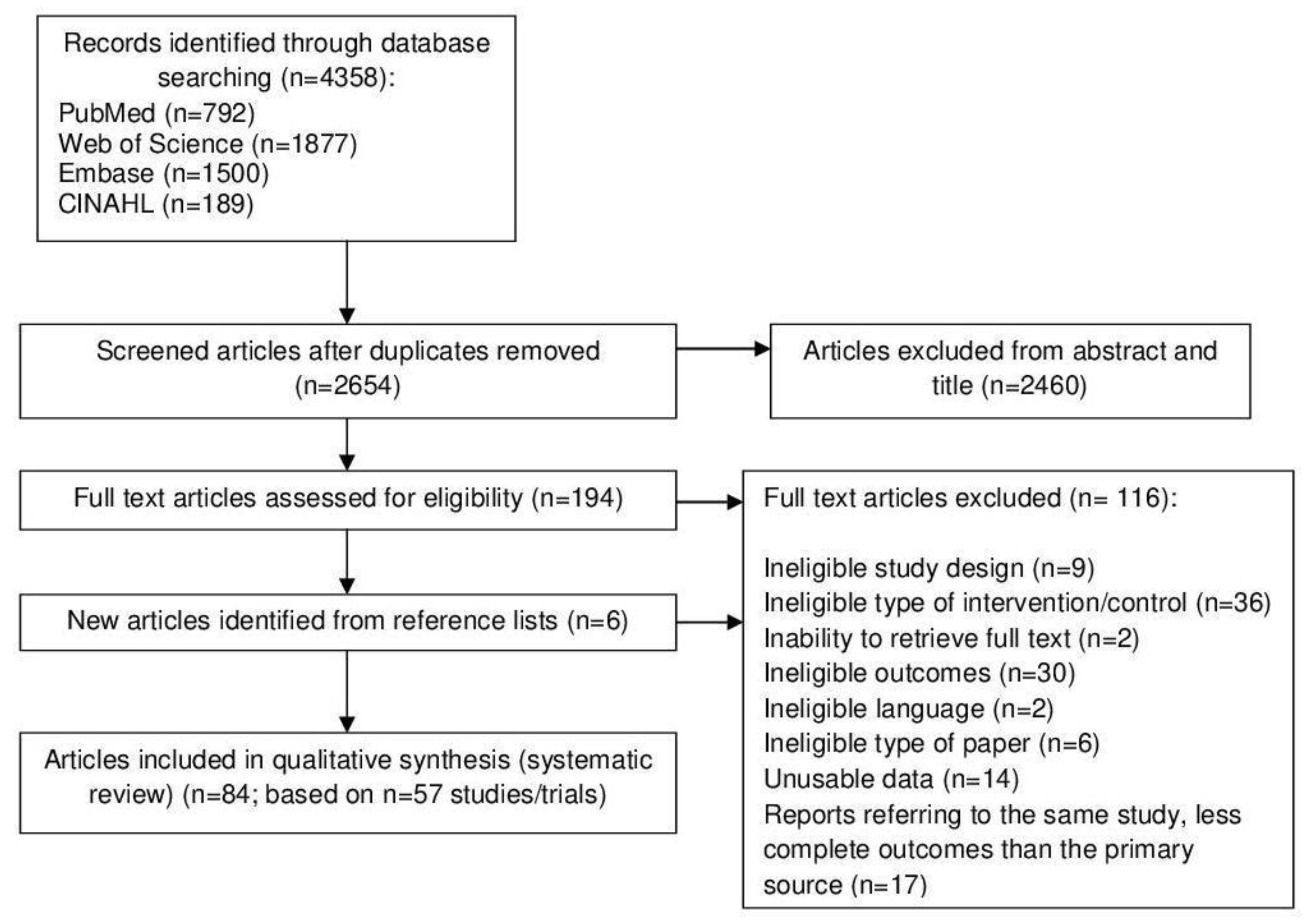
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
3.1. Study Characteristics
3.2. Metabolic Syndrome Incidence, Components and Risk Factors
3.3. Metabolic Syndrome-Related Comorbidities
3.4. Pharmacotherapy
3.5. Quality Assessment
3.6. Subgroup Analyses
3.7. Sensitivity Analyses
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Grundy, S.M. Metabolic syndrome pandemic. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 629–636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saklayen, M.G. The global epidemic of the metabolic syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [PubMed] [Green Version]
- Gami, A.S.; Witt, B.J.; Howard, D.E.; Erwin, P.J.; Gami, L.A.; Somers, V.K.; Montori, V.M. Metabolic syndrome and risk of incident cardiovascular events and death: A systematic review and meta-analysis of longitudinal studies. J. Am. Coll. Cardiol. 2007, 49, 403–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.A.; Lee, J.H.; Lim, S.Y.; Ha, H.S.; Kwon, H.S.; Park, Y.M.; Lee, W.C.; Kang, M.I.; Yim, H.W.; Yoon, K.H.; et al. Metabolic syndrome as a predictor of type 2 diabetes, and its clinical interpretations and usefulness. J. Diabetes Investig. 2013, 4, 334–343. [Google Scholar] [CrossRef]
- Kotronen, A.; Yki-Jarvinen, H. Fatty liver: A novel component of the metabolic syndrome. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 27–38. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Colao, A.; Lenzi, A.; Giugliano, D. Metabolic syndrome and risk of cancer: A systematic review and meta-analysis. Diabetes Care 2012, 35, 2402–2411. [Google Scholar] [CrossRef] [Green Version]
- Taylor, F.; Huffman, M.D.; Macedo, A.F.; Moore, T.H.; Burke, M.; Davey Smith, G.; Ward, K.; Ebrahim, S. Statins for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 1, CD004816. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Barbieri, L.; Kedhi, E.; Suryapranata, H.; De Luca, G. Percutaneous versus surgical revascularization for left main or multivessel coronary artery disease: Results from a large-scale meta-analysis in the era of drug-eluting stents. Angiology 2018, 69, 812–824. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Yannakoulia, M.; Chan, J.L.; Mantzoros, C.S. Management of the metabolic syndrome and type 2 diabetes through lifestyle modification. Annu. Rev. Nutr. 2009, 29, 223–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach-Faig, A.; Berry, E.M.; Lairon, D.; Reguant, J.; Trichopoulou, A.; Dernini, S.; Medina, F.X.; Battino, M.; Belahsen, R.; Miranda, G.; et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011, 14, 2274–2284. [Google Scholar] [CrossRef] [Green Version]
- Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906 individuals. J. Am. Coll. Cardiol. 2011, 57, 1299–1313. [Google Scholar] [CrossRef] [Green Version]
- Garcia, M.; Bihuniak, J.D.; Shook, J.; Kenny, A.; Kerstetter, J.; Huedo-Medina, T.B. The effect of the traditional Mediterranean-style diet on metabolic risk factors: A meta-analysis. Nutrients 2016, 8, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: An umbrella review of meta-analyses of observational studies and randomised trials. Eur. J. Clin. Nutr. 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Koloverou, E.; Esposito, K.; Giugliano, D.; Panagiotakos, D. The effect of Mediterranean diet on the development of type 2 diabetes mellitus: A meta-analysis of 10 prospective studies and 136,846 participants. Metabolism 2014, 63, 903–911. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Galbete, C.; Hoffmann, G. Adherence to Mediterranean diet and risk of cancer: An updated systematic review and meta-analysis. Nutrients 2017, 9, 1063. [Google Scholar] [CrossRef] [PubMed]
- Anania, C.; Perla, F.M.; Olivero, F.; Pacifico, L.; Chiesa, C. Mediterranean diet and nonalcoholic fatty liver disease. World J. Gastroenterol. 2018, 24, 2083–2094. [Google Scholar] [CrossRef] [PubMed]
- Bloomfield, H.E.; Greer, N.; Kane, R.; Wilt, T.J. Effects on health outcomes of a Mediterranean diet with no restriction on fat intake. Ann. Intern. Med. 2017, 166, 378–379. [Google Scholar] [CrossRef]
- Rees, K.; Hartley, L.; Flowers, N.; Clarke, A.; Hooper, L.; Thorogood, M.; Stranges, S. ‘Mediterranean’ dietary pattern for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2013, 8, CD009825. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T. The Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; Green, S., Ed.; The Cochrane Collaboration: London, UK, 2011; Available online: http://handbook.cochrane.org (accessed on 10 October 2020).
- Sterne, J.A.; Hernan, M.A.; Reeves, B.C.; Savovic, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malakou, E.; Linardakis, M.; Armstrong, M.E.G.; Zannidi, D.; Foster, C.; Johnson, L.; Papadaki, A. The combined effect of promoting the Mediterranean diet and physical activity on metabolic risk factors in adults: A systematic review and meta-analysis of randomised controlled trials. Nutrients 2018, 10, 1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Department of Health and Human Services and US Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; US Department of Health and Human Services and US Department of Agriculture: Bethesda, MA, USA, 2015. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 10 October 2020).
- US Department of Health & Human Services and National Heart Lung and Blood Institute. The National Heart, Lung, and Blood Institute Workshop: Toward Testing the Effects of a Mediterranean Dietary Pattern on Cardiovascular and Other Diseases in the US; US Department of Health & Human Services and National Heart Lung and Blood Institute: Bethsda, MA, USA, 2019. Available online: https://www.nhlbi.nih.gov/events/2016/national-heart-lung-and-blood-institute-workshop-toward-testing-effects-mediterranean (accessed on 17 November 2019).
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Health 2019, 7, 192–198. [Google Scholar] [CrossRef] [Green Version]
- Almanza-Aguilera, E.; Brunius, C.; Bernal-Lopez, M.R.; Garcia-Aloy, M.; Madrid-Gambin, F.; Tinabones, F.J.; Gomez-Huelgas, R.; Landberg, R.; Andres-Lacueva, C. Impact in plasma metabolome as effect of lifestyle intervention for weight-loss reveals metabolic benefits in metabolically healthy obese women. J. Proteome Res. 2018, 17, 2600–2610. [Google Scholar] [CrossRef]
- Alvarez-Perez, J.; Sanchez-Villegas, A.; Diaz-Benitez, E.M.; Ruano-Rodriguez, C.; Corella, D.; Martinez-Gonzalez, M.A.; Estruch, R.; Salas-Salvado, J.; Serra-Majem, L. Influence of a Mediterranean dietary pattern on body fat distribution: Results of the PREDIMED-Canarias intervention randomized trial. J. Am. Coll. Nutr. 2016, 35, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Ambring, A.; Friberg, P.; Axelsen, M.; Laffrenzen, M.; Taskinen, M.R.; Basu, S.; Johansson, M. Effects of a Mediterranean-inspired diet on blood lipids, vascular function and oxidative stress in healthy subjects. Clin. Sci. 2004, 106, 519–525. [Google Scholar] [CrossRef] [Green Version]
- Austel, A.; Ranke, C.; Wagner, N.; Gorge, J.; Ellrott, T. Weight loss with a modified Mediterranean-type diet using fat modification: A randomized controlled trial. Eur. J. Clin. Nutr. 2015, 69, 878–884. [Google Scholar] [CrossRef]
- Babio, N.; Toledo, E.; Estruch, R.; Ros, E.; Martinez-Gonzalez, M.A.; Castaner, O.; Bullo, M.; Corella, D.; Aros, F.; Gomez-Gracia, E.; et al. Mediterranean diets and metabolic syndrome status in the PREDIMED randomized trial. Can. Med. Assoc. J. 2014, 186, E649–E657. [Google Scholar] [CrossRef] [Green Version]
- Bajerska, J.; Chmurzynska, A.; Muzsik, A.; Krzyzanowska, P.; Madry, E.; Malinowska, A.M.; Walkowiak, J. Weight loss and metabolic health effects from energy-restricted Mediterranean and Central-European diets in postmenopausal women: A randomized controlled trial. Sci. Rep. 2018, 8, 11170. [Google Scholar] [CrossRef]
- Bemelmans, W.J.E.; Broer, J.; De Vries, J.H.M.; Hulshof, K.; May, J.F.; Meyboom-de Jong, B. Impact of Mediterranean diet education versus posted leaflet on dietary habits and serum cholesterol in a high risk population for cardiovascular disease. Public Health Nutr. 2000, 3, 273–283. [Google Scholar] [CrossRef] [Green Version]
- Ben-Avraham, S.; Harman-Boehm, I.; Schwarzfuchs, D.; Shai, I. Dietary strategies for patients with type 2 diabetes in the era of multi-approaches; review and results from the dietary intervention randomized controlled trial (DIRECT). Diabetes Res. Clin. Pract. 2009, 86, S41–S48. [Google Scholar] [CrossRef] [PubMed]
- Biolato, M.; Manca, F.; Marrone, G.; Cefalo, C.; Racco, S.; Miggiano, G.A.; Valenza, V.; Gasbarrini, A.; Miele, L.; Grieco, A. Intestinal permeability after Mediterranean diet and low-fat diet in non-alcoholic fatty liver disease. World J. Gastroenterol. 2019, 25, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Braakhuis, A.; Campion, P.; Bishop, K. The effects of dietary nutrition education on weight and health biomarkers in breast cancer survivors. Med. Sci. 2017, 5, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buscemi, S.; Verga, S.; Tranchina, M.R.; Cottone, S.; Cerasola, G. Effects of hypocaloric very-low-carbohydrate diet vs. Mediterranean diet on endothelial function in obese women. Eur. J. Clin. Investig. 2009, 39, 339–347. [Google Scholar] [CrossRef] [PubMed]
- Carruba, G.; Granata, O.M.; Pala, V.; Campisi, I.; Agostara, B.; Cusimano, R.; Ravazzolo, B.; Traina, A. A traditional Mediterranean diet decreases endogenous estrogens in healthy postmenopausal women. Nutr. Cancer 2006, 56, 253–259. [Google Scholar] [CrossRef] [PubMed]
- Casas, R.; Sacanella, E.; Urpi-Sarda, M.; Corella, D.; Castanr, O.; Lamuela-Raventos, R.M.; Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Ros, E.; Estruch, R. Long-term immunomodulatory effects of a Mediterranean diet in adults at high risk of cardiovascular disease in the prevencion con dieta mediterranea (predimed) randomized controlled trial. J. Nutr. 2016, 146, 1684–1693. [Google Scholar] [CrossRef]
- Davis, C.R.; Bryan, J.; Hodgson, J.M.; Woodman, R.; Murphy, K.J. A Mediterranean diet reduces F-2-isoprostanes and triglycerides among older Australian men and women after 6 months. J. Nutr. 2017, 147, 1348–1355. [Google Scholar] [CrossRef] [Green Version]
- Davis, C.R.; Hodgson, J.M.; Woodman, R.; Bryan, J.; Wilson, C.; Murphy, K.J. A Mediterranean diet lowers blood pressure and improves endothelial function: Results from the MedLey randomized intervention trial. Am. J. Clin. Nutr. 2017, 105, 1305–1313. [Google Scholar] [CrossRef] [Green Version]
- De Lorgeril, M.; Renaud, S.; Mamelle, N.; Salen, P.; Martin, J.L.; Monjaud, I.; Guidollet, J.; Touboul, P.; Delaye, J. Mediterranean alpha-linolenic acid-rich diet in secondary prevention of coronary heart disease. Lancet 1994, 343, 1454–1459. [Google Scholar] [CrossRef]
- Dus-Zchowska, M.; Bajerska, J.; Krzyzanowska, P.; Chmurzynska, A.; Miskiewicz-Chotnicka, A.; Muzsik, A.; Walkowiak, J. The Central European diet as an alternative to the Mediterranean diet in atherosclerosis prevention in postmenopausal obese women with a high risk of metabolic syndrome—A randomized nutritional trial. Acta Sci. Pol. Technol. Aliment. 2018, 17, 399–407. [Google Scholar] [CrossRef]
- Elhayany, A.; Lustman, A.; Abel, R.; Attal-Singer, J.; Vinker, S. A low carbohydrate Mediterranean diet improves cardiovascular risk factors and diabetes control among overweight patients with type 2 diabetes mellitus: A 1-year prospective randomized intervention study. Diabetes Obes. Metabol. 2010, 12, 204–209. [Google Scholar] [CrossRef]
- Entwistle, T.R.; Green, A.C.; Fildes, J.E.; Miura, K. Adherence to Mediterranean and low-fat diets among heart and lung transplant recipients: A randomized feasibility study. Nutr. J. 2018, 17, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Ciotola, M.; Giugliano, F.; Schisano, B.; Autorino, R.; Iuliano, S.; Vietri, M.T.; Cioffi, M.; De Sio, M.; Giugliano, D. Mediterranean diet improves sexual function in women with the metabolic syndrome. Int. J. Impot. Res. 2007, 19, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Maiorino, M.I.; Ciotola, M.; Di Palo, C.; Scognamiglio, P.; Gicchino, M.; Petrizzo, M.; Saccomanno, F.; Beneduce, F.; Ceriello, A.; et al. Effects of a Mediterranean-style diet on the need for antihyperglycemic drug therapy in patients with newly diagnosed type 2 diabetes: A randomized trial. Ann. Intern. Med. 2009, 151, 306–314. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Petrizzo, M.; Bellastella, G.; Giugliano, D. The Effects of a Mediterranean diet on the need for diabetes drugs and remission of newly diagnosed type 2 diabetes: Follow-up of a randomized trial. Diabetes Care 2014, 37, 1824–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esposito, K.; Marfella, R.; Ciotola, M.; Di Palo, C.; Giugliano, F.; Giugliano, G.; D’Armiento, M.; D’Andrea, F.; Giugliano, D. Effect of a Mediterranean-style diet on endothelial dysfunction and markers of vascular inflammation in the metabolic syndrome: A randomized trial. J. Am. Med. Assoc. 2004, 292, 1440–1446. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Pontillo, A.; Di Palo, C.; Giugliano, G.; Masella, M.; Marfella, R.; Giugliano, D. Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women: A randomized trial. J. Am. Med. Assoc. 2003, 289, 1799–1804. [Google Scholar] [CrossRef] [Green Version]
- Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Fito, M.; Chiva-Blanch, G.; Fiol, M.; Gomez-Gracia, E.; Aros, F.; Lapetra, J.; et al. Effect of a high-fat Mediterranean diet on bodyweight and waist circumference: A prespecified secondary outcomes analysis of the PREDIMED randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, e6–e17. [Google Scholar] [CrossRef]
- Estruch, R.; Martinez-Gonzalez, M.A.; Corella, D.; Salas-Salvado, J.; Ruiz-Gutierrez, V.; Covas, M.I.; Fiol, M.; Gomez-Gracia, E.; Lopez-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-style diet on cardiovascular risk factors—A randomized trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet supplemented with extra-virgin olive oil or nuts. N. Engl. J. Med. 2018, 378, e34. [Google Scholar] [CrossRef]
- Fito, M.; Estruch, R.; Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Aros, F.; Vila, J.; Corella, D.; Diaz, O.; Saez, G.; De La Torre, R.; et al. Effect of the Mediterranean diet on heart failure biomarkers: A randomized sample from the PREDIMED trial. Eur. J. Heart Fail. 2014, 16, 543–550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fortin, A.; Rabasa-Lhoret, R.; Lemieux, S.; Labonte, M.E.; Gingras, V. Comparison of a Mediterranean to a low-fat diet intervention in adults with type 1 diabetes and metabolic syndrome: A 6-month randomized trial. Nutr. Metabol. Cardiovascul. Dis. 2018, 28, 1275–1284. [Google Scholar] [CrossRef]
- Fraser, A.; Abel, R.; Lawlor, D.A.; Fraser, D.; Elhayany, A. A modified Mediterranean diet is associated with the greatest reduction in alanine aminotransferase levels in obese type 2 diabetes patients: Results of a quasi-randomised controlled trial. Diabetologia 2008, 51, 1616–1622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gepner, Y.; Shelef, I.; Komy, O.; Cohen, N.; Schwarzfuchs, D.; Bril, N.; Rein, M.; Serfaty, D.; Kenigsbuch, S.; Zelicha, H.; et al. The beneficial effects of Mediterranean diet over low-fat diet may be mediated by decreasing hepatic fat content. J. Hepatol. 2019, 71, 379–388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gepner, Y.; Shelef, I.; Schwarzfuchs, D.; Zelicha, H.; Tene, L.; Yaskolka Meir, A.; Tsaban, G.; Cohen, N.; Bril, N.; Rein, M.; et al. Effect of distinct lifestyle interventions on mobilization of fat storage pools: CENTRAL magnetic resonance imaging randomized controlled trial. Circulation 2018, 137, 1143–1157. [Google Scholar] [CrossRef]
- Hagfors, L.; Leanderson, P.; Skoldstam, L.; Andersson, J.; Johansson, G. Antioxidant intake, plasma antioxidants and oxidative stress in a randomized, controlled, parallel, Mediterranean dietary intervention study on patients with rheumatoid arthritis. Nutr. J. 2003, 2. [Google Scholar] [CrossRef] [Green Version]
- Hjerkinn, E.M.; Abdelnoor, M.; Breivik, L.; Bergengen, L.; Ellingsen, I.; Seljeflot, I.; Aase, O.; Ole Klemsdal, T.; Hjermann, I.; Arnesen, H.; et al. Effect of diet or very long chain omega-3 fatty acids on progression of atherosclerosis, evaluated by carotid plaques, intima-media thickness and by pulse wave propagation in elderly men with hypercholesterolaemia. Eur. J. Cardiovasc. Prev. Rehabil. 2006, 13, 325–333. [Google Scholar] [CrossRef]
- Jaacks, L.M.; Sher, S.; Staercke, C.; Porkert, M.; Alexander, W.R.; Jones, D.P.; Vaccarino, V.; Ziegler, T.R.; Quyyumi, A.A. Pilot randomized controlled trial of a Mediterranean diet or diet supplemented with fish oil, walnuts, and grape juice in overweight or obese US adults. BMC Nutr. 2018, 4, 26. [Google Scholar] [CrossRef]
- Jennings, A.; Berendsen, A.M.; de Groot, L.; Feskens, E.J.M.; Brzozowska, A.; Sicinska, E.; Pietruszka, B.; Meunier, N.; Caumon, E.; Malpuech-Brugere, C.; et al. Mediterranean-style diet improves systolic blood pressure and arterial stiffness in older adults. Hypertension 2019, 73, 578–586. [Google Scholar] [CrossRef]
- Katsagoni, C.N.; Papatheodoridis, G.V.; Ioannidou, P.; Deutsch, M.; Alexopoulou, A.; Papadopoulos, N.; Papageorgiou, M.V.; Fragopoulou, E.; Kontogianni, M.D. Improvements in clinical characteristics of patients with non-alcoholic fatty liver disease, after an intervention based on the Mediterranean lifestyle: A randomised controlled clinical trial. Br. J. Nutr. 2018, 120, 164–175. [Google Scholar] [CrossRef]
- Lasa, A.; Miranda, J.; Bullo, M.; Casas, R.; Salas-Salvado, J.; Larretxi, I.; Estruch, R.; Ruiz-Gutierrez, V.; Portillo, M.P. Comparative effect of two Mediterranean diets versus a low-fat diet on glycaemic control in individuals with type 2 diabetes. Eur. J. Clin. Nutr. 2014, 68, 767–772. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Pase, M.; Pipingas, A.; Raubenheimer, J.; Thurgood, M.; Villalon, L.; Macpherson, H.; Gibbs, A.; Scholey, A. Switching to a 10-day Mediterranean-style diet improves mood and cardiovascular function in a controlled crossover study. Nutrition 2015, 31, 647–652. [Google Scholar] [CrossRef]
- Maijo, M.; Ivory, K.; Clements, S.J.; Dainty, J.R.; Jennings, A.; Gillings, R.; Fairweather-Tait, S.; Gulisano, M.; Santoro, A.; Franceschi, C.; et al. One-year consumption of a mediterranean-like dietary pattern with vitamin D3 supplements induced small scale but extensive changes of immune cell phenotype, co-receptor expression and innate immune responses in healthy elderly subjects: Results from the United Kingdom arm of the NU-AGE trial. Front. Physiol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Maiorino, M.I.; Bellastella, G.; Petrizzo, M.; Scappaticcio, L.; Giugliano, D.; Esposito, K. Mediterranean diet cools down the inflammatory milieu in type 2 diabetes: The MEDITA randomized controlled trial. Endocrine 2016, 54, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Mayr, H.L.; Itsiopoulos, C.; Tierney, A.C.; Kucianski, T.; Radcliffe, J.; Garg, M.; Willcox, J.; Thomas, C.J. Ad libitum Mediterranean diet reduces subcutaneous but not visceral fat in patients with coronary heart disease: A randomised controlled pilot study. Clin. Nutr. ESPEN 2019, 32, 61–69. [Google Scholar] [CrossRef]
- Mayr, H.L.; Thomas, C.J.; Tierney, A.C.; Kucianski, T.; George, E.S.; Ruiz-Canela, M.; Hebert, J.R.; Shivappa, N.; Itsiopoulos, C. Randomization to 6-month Mediterranean diet compared with a low-fat diet leads to improvement in dietary inflammatory index scores in patients with coronary heart disease: The AUSMED heart trial. Nutr. Res. 2018, 55, 94–107. [Google Scholar] [CrossRef] [Green Version]
- McManus, K.; Antinoro, L.; Sacks, F. A randomized controlled trial of a moderate-fat, low-energy diet compared with a low fat, low-energy diet for weight loss in overweight adults. Intern. J. Obes. 2001, 25, 1503–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meir, A.Y.; Tsaban, G.; Zelicha, H.; Rinott, E.; Kaplan, A.; Youngster, I.; Rudich, A.; Shelef, I.; Tirosh, A.; Brikner, D.; et al. A green-mediterranean diet, supplemented with mankai duckweed, preserves iron-homeostasis in humans and is efficient in reversal of anemia in rats. J. Nutr. 2019, 149, 1004–1011. [Google Scholar] [CrossRef]
- Mezzano, D.; Leighton, F.; Martinez, C.; Marshall, G.; Cuevas, A.; Castillo, O.; Panes, O.; Munoz, B.; Perez, D.D.; Mizon, C.; et al. Complementary effects of Mediterranean diet and moderate red wine intake on haemostatic cardiovascular risk factors. Eur. J. Clin. Nutr. 2001, 55, 444–451. [Google Scholar] [CrossRef] [Green Version]
- Michielsen, C.; Hangelbroek, R.W.J.; Feskens, E.J.M.; Afman, L.A. Disentangling the effects of monounsaturated fatty acids from other components of a mediterranean diet on serum metabolite profiles: A randomized fully controlled dietary intervention in healthy subjects at risk of the metabolic syndrome. Mol. Nutr. Food Res. 2019, 63, e1801095. [Google Scholar] [CrossRef]
- Misciagna, G.; Diaz, M.D.; Caramia, D.V.; Bonfiglio, C.; Franco, I.; Noviello, M.R.; Chiloiro, M.; Abbrescia, D.I.; Mirizzi, A.; Tanzi, M.; et al. Effect of a low glycemic index Mediterranean diet on non-alcoholic fatty liver disease. A randomized controlled clinici trial. J. Nutr Health Aging 2017, 21, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Ortner Hadziabdic, M.; Vitali Cepo, D.; Rahelic, D.; Bozikov, V. The effect of the Mediterranean diet on serum total antioxidant capacity in obese patients: A randomized controlled trial. J. Am. Coll. Nutr. 2016, 35, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Osella, A.R.; Colaianni, G.; Correale, M.; Pesole, P.L.; Bruno, I.; Buongiorno, C.; Deflorio, V.; Leone, C.M.; Colucci, S.C.; Grano, M.; et al. Irisin serum levels in metabolic syndrome patients treated with three different diets: A post-hoc analysis from a randomized controlled clinical trial. Nutrients 2018, 10, 844. [Google Scholar] [CrossRef] [Green Version]
- Paniagua, J.A.; Gallego de la Sacristana, A.; Romero, I.; Vidal-Puig, A.; Latre, J.M.; Sanchez, E.; Perez-Martinez, P.; Lopez-Miranda, J.; Perez-Jimenez, F. Monounsaturated fat-rich diet prevents central body fat distribution and decreases postprandial adiponectin expression induced by a carbohydrate-rich diet in insulin-resistant subjects. Diabetes Care 2007, 30, 1717–1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papadaki, A.; Martinez-Gonzalez, M.A.; Alonso-Gomez, A.; Rekondo, J.; Salas-Salvado, J.; Corella, D.; Ros, E.; Fito, M.; Estruch, R.; Lapetra, J.; et al. Mediterranean diet and risk of heart failure: Results from the PREDIMED randomized controlled trial. Eur. J. Heart Fail. 2017, 19, 1179–1185. [Google Scholar] [CrossRef]
- Papadaki, A.; Martinez-Gonzalez, M.A.; Alonso-Gomez, A.; Rekondo, J.; Salas-Salvado, J.; Corella, D.; Ros, E.; Fito, M.; Estruch, R.; Lapetra, J.; et al. Erratum to: Mediterranean diet and risk of heart failure: Results from the PREDIMED randomized controlled trial: Mediterranean diet and heart failure risk. Eur. J. Heart Fail. 2019, 21, 389–391. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, A.; Scott, J.A. The Mediterranean eating in Scotland experience project: Evaluation of an internet-based intervention promoting the Mediterranean diet. Br. J. Nutr. 2005, 94, 290–298. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, A.; Scott, J.A. Follow-up of a web-based tailored intervention promoting the Mediterranean diet in Scotland. Patient Educ. Counsel. 2008, 73, 256–263. [Google Scholar]
- Papandreou, C.; Schiza, S.E.; Bouloukaki, I.; Hatzis, C.M.; Kafatos, A.G.; Siafakas, N.M.; Tzanakis, N.E. Effect of Mediterranean diet versus prudent diet combined with physical activity on OSAS: A randomised trial. Eur. Resp. J. 2012, 39, 1398–1404. [Google Scholar] [CrossRef] [Green Version]
- Parcina, M.; Brune, M.; Kaese, V.; Zorn, M.; Spiegel, R.; Vojvoda, V.; Fleming, T.; Rudofsky, G.; Nawroth, P.P. No short-term effects of calorie-controlled Mediterranean or fast food dietary interventions on established biomarkers of vascular or metabolic risk in healthy individuals. Nutr. Res. Pract. 2015, 9, 165–173. [Google Scholar] [CrossRef] [Green Version]
- Properzi, C.; O’Sullivan, T.A.; Sherriff, J.L.; Ching, H.L.; Jeffrey, G.P.; Buckley, R.F.; Tibballs, J.; MacQuillan, G.C.; Garas, G.; Adams, L.A.; et al. Ad libitum Mediterranean and low-fat diets both significantly reduce hepatic steatosis: A randomized controlled trial. Hepatology 2018, 68, 1741–1754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richard, C.; Couture, P.; Desroches, S.; Charest, A.; Lamarche, B. Effect of the Mediterranean diet with and without weight loss on cardiovascular risk factors in men with the metabolic syndrome. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 628–635. [Google Scholar] [CrossRef] [PubMed]
- Richard, C.; Couture, P.; Desroches, S.; Lamarche, B. Effect of the Mediterranean diet with and without weight loss on markers of inflammation in men with metabolic syndrome. Obesity 2013, 21, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, D.; Macas, D.; Milner, M.; Liu, Y.S.; Klonizakis, M. Contrasting effects of short-term Mediterranean and vegan diets on microvascular function and cholesterol in younger adults: A comparative pilot study. Nutrients 2018, 10, 1897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, M.C.; Itsiopoulos, C.; Thodis, T.; Ward, G.; Trost, N.; Hofferberth, S.; O’Dea, K.; Desmond, P.V.; Johnson, N.A.; Wilson, A.M.; et al. The Mediterranean diet improves hepatic steatosis and insulin sensitivity in individuals with non-alcoholic fatty liver disease. J. Hepatol. 2013, 59, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Salas-Salvado, J.; Bullo, M.; Estruch, R.; Ros, E.; Covas, M.I.; Ibarrola-Jurado, N.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.; et al. Prevention of diabetes with Mediterranean diets: A subgroup analysis of a randomized trial. Ann. Intern. Med. 2014, 160, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Sala-Vila, A.; Romero-Mamani, E.S.; Gilabert, R.; Nunez, I.; De la Torre, R.; Corella, D.; Ruiz-Gutierrez, V.; Lopez-Sabater, M.C.; Pinto, X.; Rekondo, J.; et al. Changes in ultrasound-assessed carotid intima-media thickness and plaque with a Mediterranean diet: A substudy of the PREDIMED trial. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 439–445. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Schwarzfuchs, D.; Henkin, Y.; Shahar, D.R.; Witkow, S.; Greenberg, I.; Golan, R.; Fraser, D.; Bolotin, A.; Vardi, H.; et al. Weight loss with a low-carbohydrate, Mediterranean, or low-fat diet. N. Engl. J. Med. 2008, 359, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Shai, I.; Spence, J.D.; Schwarzfuchs, D.; Henkin, Y.; Parraga, G.; Rudich, A.; Fenster, A.; Mallett, C.; Liel-Cohen, N.; Tirosh, A.; et al. Dietary intervention to reverse carotid atherosclerosis. Circulation 2010, 121, 1200–1208. [Google Scholar] [CrossRef] [Green Version]
- Singh, R.B.; Dubnov, G.; Niaz, M.A.; Ghosh, S.; Singh, R.; Rastogi, S.S.; Manor, O.; Pella, D.; Berry, E.M. Effect of an Indo-Mediterranean diet on progression of coronary artery disease in high risk patients (Indo-Mediterranean diet heart study): A randomised single-blind trial. Lancet 2002, 360, 1455–1461. [Google Scholar] [CrossRef]
- Singh, R.B.; Saboo, B.; Mahashwari, A.; Bharatdwaj, K.; Verma, N.; Hristova, K.; Ghosh, S.; Niaz, M.A.; Singh, J.; Adeghate, E.; et al. Effects of Indo-Mediterranean style diet and low fat diet on incidence of diabetes in acute coronary syndromes. World Heart J. 2017, 9, 25–36. [Google Scholar]
- Skoldstam, L.; Hagfors, L.; Johansson, G. An experimental study of a Mediterranean diet intervention for patients with rheumatoid arthritis. Ann. Rheum. Dis. 2003, 62, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Skouroliakou, M.; Grosomanidis, D.; Massara, P.; Kostara, C.; Papandreou, P.; Ntountaniotis, D.; Xepapadakis, G. Serum antioxidant capacity, biochemical profile and body composition of breast cancer survivors in a randomized Mediterranean dietary intervention study. Eur. J. Nutr. 2018, 57, 2133–2145. [Google Scholar] [CrossRef]
- Sofi, F.; Dinu, M.; Pagliai, G.; Cesari, F.; Gori, A.M.; Sereni, A.; Becatti, M.; Fiorillo, C.; Marcucci, R.; Casini, A.; et al. Low-calorie vegetarian versus Mediterranean diets for reducing body weight and improving cardiovascular risk profile. Circulation 2018, 137, 1103–1113. [Google Scholar] [CrossRef]
- Sola, R.; Fito, M.; Estruch, R.; Salas-Salvado, J.; Corella, D.; De la Torre, R.; Munoz, M.A.; Lopez-Sabater, M.D.; Martinez-Gonzalez, M.A.; Aros, F.; et al. Effect of a traditional Mediterranean diet on apolipoproteins B, A-I, and their ratio: A randomized, controlled trial. Atherosclerosis 2011, 218, 174–180. [Google Scholar] [CrossRef]
- Stachowska, E.; Gutowska, I.; Strzelczak, A.; Wesolowska, T.; Safranow, K.; Ciechanowski, K.; Chlubek, D. The use of neural networks in evaluation of the direction and dynamics of changes in lipid parameters in kidney transplant patients on the Mediterranean diet. J. Ren. Nutr. 2006, 16, 150–159. [Google Scholar] [CrossRef]
- Storniolo, C.; Casillas, R.; Bullo, M.; Castaner, O.; Ros, E.; Saez, G.; Toledo, E.; Estruch, R.; Ruiz-Gutierrez, V.; Fito, M.; et al. A Mediterranean diet supplemented with extra virgin olive oil or nuts improves endothelial markers involved in blood pressure control in hypertensive women. Eur. J. Nutr. 2017, 56, 89–97. [Google Scholar] [CrossRef]
- Thomazella, M.C.D.; Góes, M.F.; Andrade, C.R.; Debbas, V.; Barbeiro, D.F.; Correia, R.L.; Marie, S.K.; Cardounel, A.J.; Laurindo, F.R. Effects of high adherence to Mediterranean or low-fat diets in medicated secondary prevention patients. Am. J. Cardiol. 2011, 108, 1523–1529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timar, R.; Timar, B.; Horhat, F.; Oancea, C. The impact of Mediterranean diet on glycemic control and cardiovascular risk factors in type 2 diabetic patients. J. Food Agricult. Environ. 2013, 11, 561–563. [Google Scholar]
- Toledo, E.; Hu, F.B.; Estruch, R.; Buil-Cosiales, P.; Corella, D.; Salas-Salvado, J.; Covas, M.I.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; et al. Effect of the Mediterranean diet on blood pressure in the PREDIMED trial: Results from a randomized controlled trial. BMC Med. 2013, 11, 207. [Google Scholar] [CrossRef] [Green Version]
- Toledo, E.; Salas-Salvado, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fito, M.; Hu, F.B.; Aros, F.; et al. Mediterranean diet and invasive breast cancer risk among women at high cardiovascular risk in the predimed trial a randomized clinical trial. JAMA Intern. Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Troseid, M.; Arnesen, H.; Hjerkinn, E.M.; Seljeflot, I. Serum levels of interleukin-18 are reduced by diet and n-3 fatty acid intervention in elderly high-risk men. Metab. Clin. Exp. 2009, 58, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Tutino, V.; De Nunzio, V.; Caruso, M.G.; Bonfiglio, C.; Franco, I.; Mirizzi, A.; De Leonardis, G.; Cozzolongo, R.; Giannuzzi, V.; Giannelli, G.; et al. Aerobic physical activity and a low glycemic diet reduce the AA/EPA ratio in red blood cell membranes of patients with NAFLD. Nutrients 2018, 10, 1299. [Google Scholar] [CrossRef] [Green Version]
- Vincent-Baudry, S.; Defoort, C.; Gerber, M.; Bernard, M.; Verger, P.; Helal, O.; Portugal, H.; Planells, R.; Grolier, P.; Amiot-Carlin, M.; et al. The Medi-RIVAGE study: Reduction of cardiovascular disease risk factors after a 3-mo intervention with a Mediterranean-type diet or a low-fat diet. Am. J. Clin. Nutr. 2005, 82, 964–971. [Google Scholar] [PubMed] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Murphy, K.J. A Mediterranean diet supplemented with dairy foods improves markers of cardiovascular risk: Results from the MedDairy randomized controlled trial. Am. J. Clin. Nutr. 2018, 108, 1166–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wade, A.T.; Davis, C.R.; Dyer, K.A.; Hodgson, J.M.; Woodman, R.J.; Murphy, K.J. Effects of Mediterranean diet supplemented with lean pork on blood pressure and markers of cardiovascular risk: Findings from the MedPork trial. Br. J. Nutr. 2019, 122, 873–883. [Google Scholar] [CrossRef]
- Wardle, J.; Rogers, P.; Judd, P.; Taylor, M.A.; Rapoport, L.; Green, M.; Nicholson Perry, K. Randomized trial of the effects of cholesterol-lowering dietary treatment on psychological function. Am. J. Med. 2000, 108, 547–553. [Google Scholar] [CrossRef]
- Vincent, S.; Gerber, M.; Bernard, M.; Defoort, C.; Loundou, A.; Portugal, H.; Planells, R.; Juhan-Vague, I.; Charpiot, P.; Grolier, P.; et al. The Medi-RIVAGE study (Mediterranean Diet, cardiovascular risks and gene polymorphisms): Rationale, recruitment, design, dietary intervention and baseline characteristics of participants. Public Health Nutr. 2004, 7, 531–542. [Google Scholar]
- Schwingshackl, L.; Hoffmann, G. Mediterranean dietary pattern, inflammation and endothelial function: A systematic review and meta-analysis of intervention trials. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 929–939. [Google Scholar] [CrossRef]
- Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss: Meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 2011, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Papadaki, A.; Thanasoulias, A.; Pound, R.; Sebire, S.J.; Jago, R. Employees’ expectations of internet-based, workplace interventions promoting the Mediterranean diet: A qualitative study. J. Nutr. Educ. Behav. 2016, 48, 706–715. [Google Scholar] [CrossRef] [Green Version]
- Moore, S.E.; McEvoy, C.T.; Prior, L.; Lawton, J.; Patterson, C.C.; Kee, F.; Cupples, M.; Young, I.S.; Appleton, K.; McKinley, M.C.; et al. Barriers to adopting a Mediterranean diet in Northern European adults at high risk of developing cardiovascular disease. J. Hum. Nutr. Diet. 2018, 31, 451–462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willett, W.C. The Mediterranean diet: Science and practice. Public Health Nutr. 2006, 9, 105–110. [Google Scholar] [PubMed] [Green Version]
- Liyanage, T.; Ninomiya, T.; Wang, A.; Neal, B.; Jun, M.; Wong, M.G.; Jardine, M.; Hillis, G.S.; Perkovic, V. Effects of the Mediterranean diet on cardiovascular outcomes—A systematic review and meta-analysis. PLoS ONE 2016, 11, e0159252. [Google Scholar] [CrossRef] [Green Version]
- Grosso, G.; Marventano, S.; Yang, J.; Micek, A.; Pajak, A.; Scalfi, L.; Galvano, F.; Kales, S.N. A comprehensive meta-analysis on evidence of Mediterranean diet and cardiovascular disease: Are individual components equal? Crit. Rev. Food Sci. Nutr. 2017, 57, 3218–3232. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Missbach, B.; Konig, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292–1299. [Google Scholar] [CrossRef] [Green Version]
- De Vries, F.M.; Kolthof, J.; Postma, M.J.; Denig, P.; Hak, E. Efficacy of standard and intensive statin treatment for the secondary prevention of cardiovascular and cerebrovascular events in diabetes patients: A meta-analysis. PLoS ONE 2014, 9, e111247. [Google Scholar] [CrossRef]


{kind=link}
| Parameter | Criterion |
|---|---|
| Population | Adults aged ≥18 years |
| Intervention | Mediterranean or Mediterranean-style diet |
| Comparator | No treatment, usual care, or advice to follow a different diet |
| Outcome |
|
| Study design | Controlled trials |
| Outcome | No. of Studies | No. of Participants | Effect Estimate (MD, 95% CI) | p-Value | I2 |
|---|---|---|---|---|---|
| Anthropometric markers | |||||
| Body weight (kg) | 40 | 12,571 | −1.72 (−2.40, −1.05) | <0.001 | 98.6% |
| Body mass index (kg/m2) | 37 | 5679 | −0.41 (−0.71, −0.10) | 0.010 | 98.6% |
| Waist circumference (cm) (MetSyn component) | 27 | 9690 | −1.47 (−2.54, −0.39) | 0.007 | 99.6% |
| Total fat mass (kg) | 9 | 963 | −0.47 (−1.53, 0.60) | 0.389 | 85.1% |
| Total body fat (%) | 8 | 661 | −0.12 (−1.60, 1.37) | 0.878 | 89.7% |
| Blood pressure (MetSyn component) | |||||
| Systolic blood pressure (mm Hg) | 27 | 4930 | −1.34 (−2.00, −0.67) | <0.001 | 93.6% |
| Diastolic blood pressure (mm Hg) | 27 | 4930 | −0.81 (−1.30, −0.32) | 0.001 | 92.8% |
| Biochemical and insulin resistance markers | |||||
| Glucose (mg/dL) (MetSyn component) | 31 | 3662 | −2.98 (−4.54, −1.42) | <0.001 | 98.1% |
| Insulin (μU/mL) | 20 | 2184 | −0.94 (−1.72, −0.16) | 0.019 | 97.2% |
| HOMA-IR index | 18 | 2098 | −0.42 (−0.70, −0.15) | 0.003 | 97.7% |
| HbA1c (%) | 18 | 869 | −0.15 (−0.41, 0.12) | 0.274 | 81.3% |
| Total cholesterol (mg/dL) | 37 | 4603 | −5.70 (−9.96, −1.43) | 0.009 | 98.6% |
| LDL-cholesterol (mg/dL) | 29 | 3633 | −8.24 (−13.50, −2.99) | 0.002 | 99.6% |
| HDL-cholesterol (mg/dL) (MetSyn component) | 36 | 4433 | 1.30 (0.38, 2.21) | 0.005 | 98.1% |
| Triglycerides (mg/dL) (MetSyn component) | 38 | 4658 | −12.30 (−15.60, −8.99) | <0.001 | 94.8% |
| Non-HDL-cholesterol (mg/dL) | 2 | 584 | −1.39 (−19.40, 16.61) | 0.880 | 42.3% |
| Total:HDL-cholesterol ratio | 6 | 670 | −0.83 (−2.67, 1.01) | 0.378 | 99.6% |
| Homocysteine (μmol/L) | 2 | 171 | −0.04 (−0.61, 0.53) | 0.882 | 0.0% |
| AST (UI/L) | 3 | 193 | −3.44 (−7.56, 0.68) | 0.102 | 97.7% |
| ALT (UI/L) | 8 | 729 | −5.66 (−9.44, −1.87) | 0.003 | 97.3% |
| GGT (UI/L) | 7 | 393 | −2.51 (−5.38, 0.35) | 0.086 | 63.7% |
| Hepatic fat mass (%) | 3 | 224 | −2.80 (−5.52, −0.08) | 0.044 | 79.0% |
| Oxidative stress markers | |||||
| Oxidized LDL-cholesterol (U/L) | 2 | 970 | 4.38 (−16.49, 25.25) | 0.681 | 97.7% |
| Inflammatory markers | |||||
| C-reactive protein (mg/L) | 13 | 1071 | −0.77 (−1.14, −0.39) | <0.001 | 92.6% |
| Interleukin-6 (pg/mL) | 4 | 261 | −0.61 (−0.93, −0.30) | <0.001 | 0.0% |
| Adiponectin (μg/mL) | 4 | 546 | 0.76 (−1.16, 2.67) | 0.438 | 70.4% |
| Tumor necrosis factor-a (pg/mL) | 2 | 283 | −0.81 (−1.03, −0.60) | <0.001 | 0.0% |
| Markers of endothelial function | |||||
| Flow-mediated dilatation (%) | 3 | 206 | 1.49 (0.61, 2.37) | <0.001 | 0.0% |
| Outcome | No. of Studies | Intervention | Control | Effect Estimate (RR, 95% CI) | p-Value | I2 | ||
|---|---|---|---|---|---|---|---|---|
| Events | Total | Events | Total | |||||
| Metabolic Syndrome-related comorbidities | ||||||||
| CVD mortality | 3 | 90 | 5503 | 96 | 2955 | 0.72 (0.43, 1.01) | 0.090 | 0.0% |
| CVD incidence | 2 | 119 | 703 | 201 | 703 | 0.61 (0.42, 0.80) | <0.001 | 0.0% |
| Sudden cardiac death | 2 | 15 | 703 | 34 | 703 | 0.45 (−0.15, 1.04) | 0.142 | 0.0% |
| Stroke incidence | 2 | 88 | 5496 | 71 | 2951 | 0.67 (0.35, 0.98) | <0.001 | 0.0% |
| Heart failure incidence | 2 | 73 | 5470 | 67 | 2933 | 0.69 (0.08, 1.30) | 0.300 | 59.4% |
| Non-fatal myocardial infarction | 2 | 26 | 801 | 60 | 804 | 0.45 (−0.001, 0.900) | 0.051 | 0.0% |
| Fatal myocardial infarction | 2 | 30 | 703 | 44 | 703 | 0.68 (0.23, 1.12) | 0.090 | 0.0% |
| Type 2 diabetes incidence | 2 | 207 | 2598 | 144 | 1349 | 0.81 (0.61, 1.02) | 0.051 | 0.0% |
| Pharmacotherapy | ||||||||
| Use of blood pressure lowering drugs | 3 | 2444 | 3299 | 1130 | 1657 | 0.99 (0.96, 1.02) | 0.550 | 0.0% |
| Use of lipid-lowering agents | 2 | 1552 | 2738 | 602 | 1090 | 1.01 (0.95, 1.08) | 0.690 | 0.0% |
| Use of anti-platelet therapy | 2 | 818 | 2738 | 338 | 1090 | 0.99 (0.90, 1.08) | 0.830 | 0.0% |
| Use of insulin | 2 | 271 | 2738 | 109 | 1090 | 0.99 (0.78, 1.20) | 0.890 | 0.0% |
| Use of oral antidiabetic agents | 3 | 1112 | 2846 | 520 | 1197 | 0.83 (0.58, 1.09) | 0.230 | 64.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Papadaki, A.; Nolen-Doerr, E.; Mantzoros, C.S. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients 2020, 12, 3342. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113342
Papadaki A, Nolen-Doerr E, Mantzoros CS. The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults. Nutrients. 2020; 12(11):3342. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113342
Chicago/Turabian StylePapadaki, Angeliki, Eric Nolen-Doerr, and Christos S. Mantzoros. 2020. "The Effect of the Mediterranean Diet on Metabolic Health: A Systematic Review and Meta-Analysis of Controlled Trials in Adults" Nutrients 12, no. 11: 3342. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113342