Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis?

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
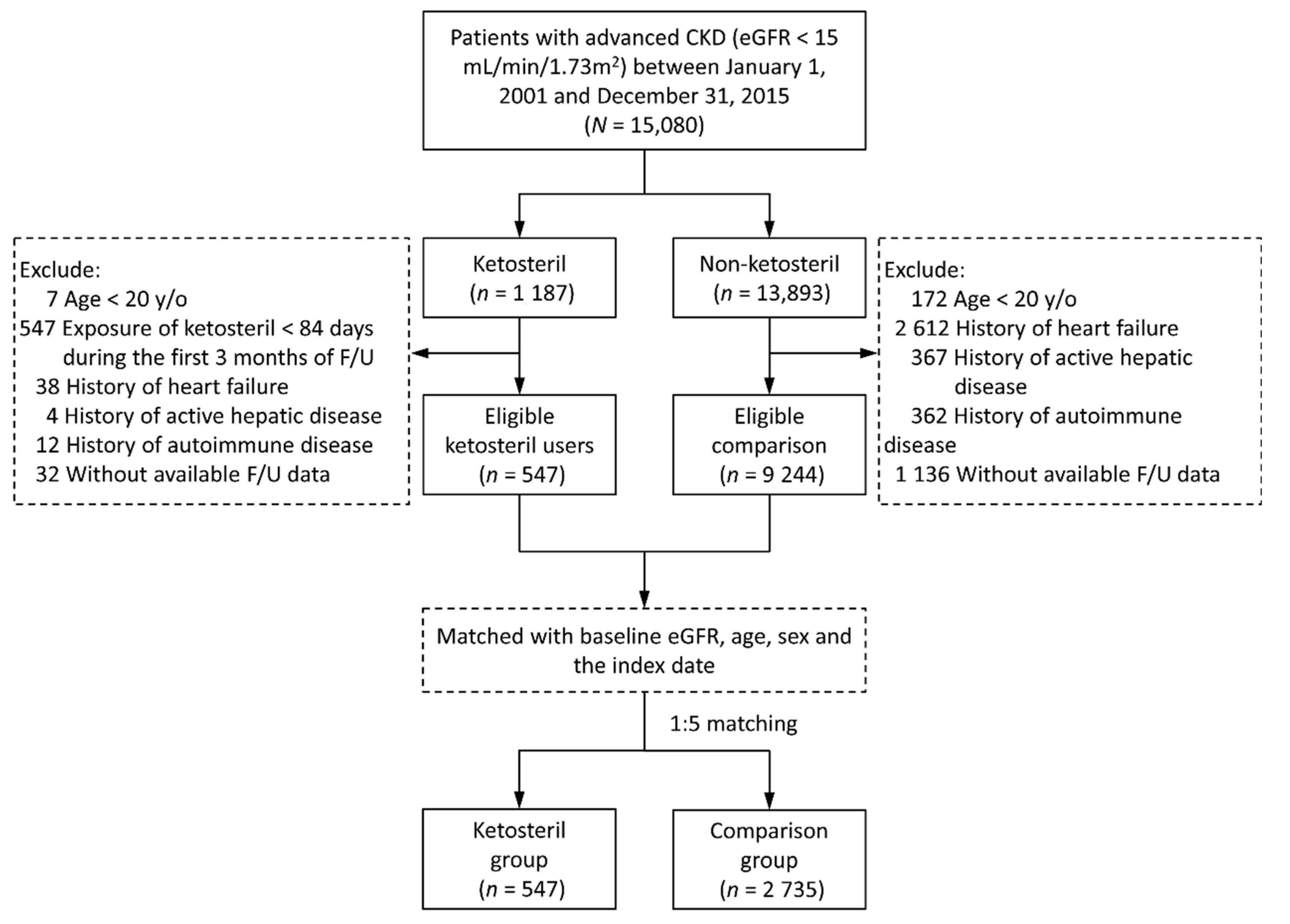
2.2. Patient Selection and Study Design
2.3. Covariates
2.4. Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
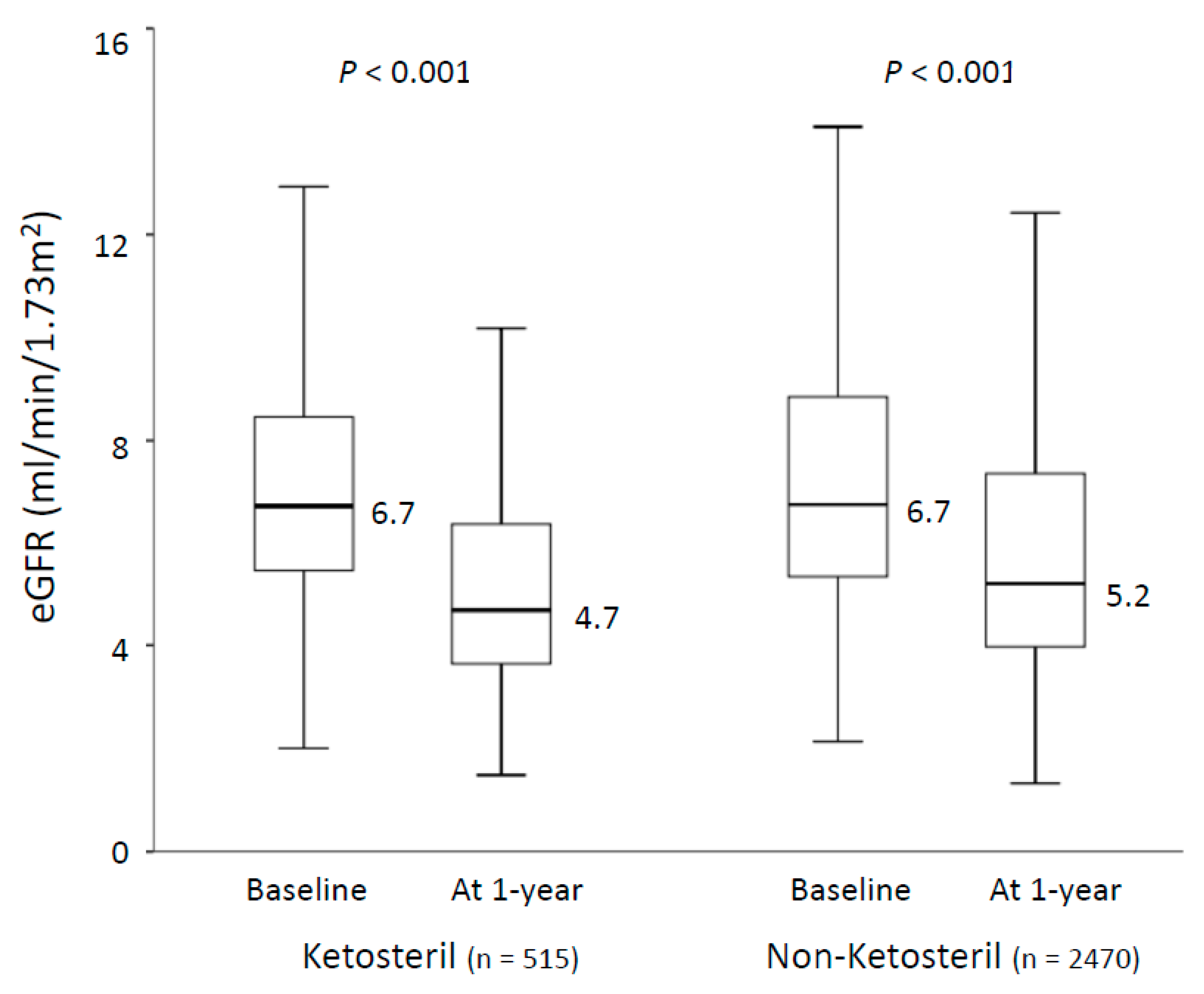
3.2. Outcomes during 1 Year Follow-Up
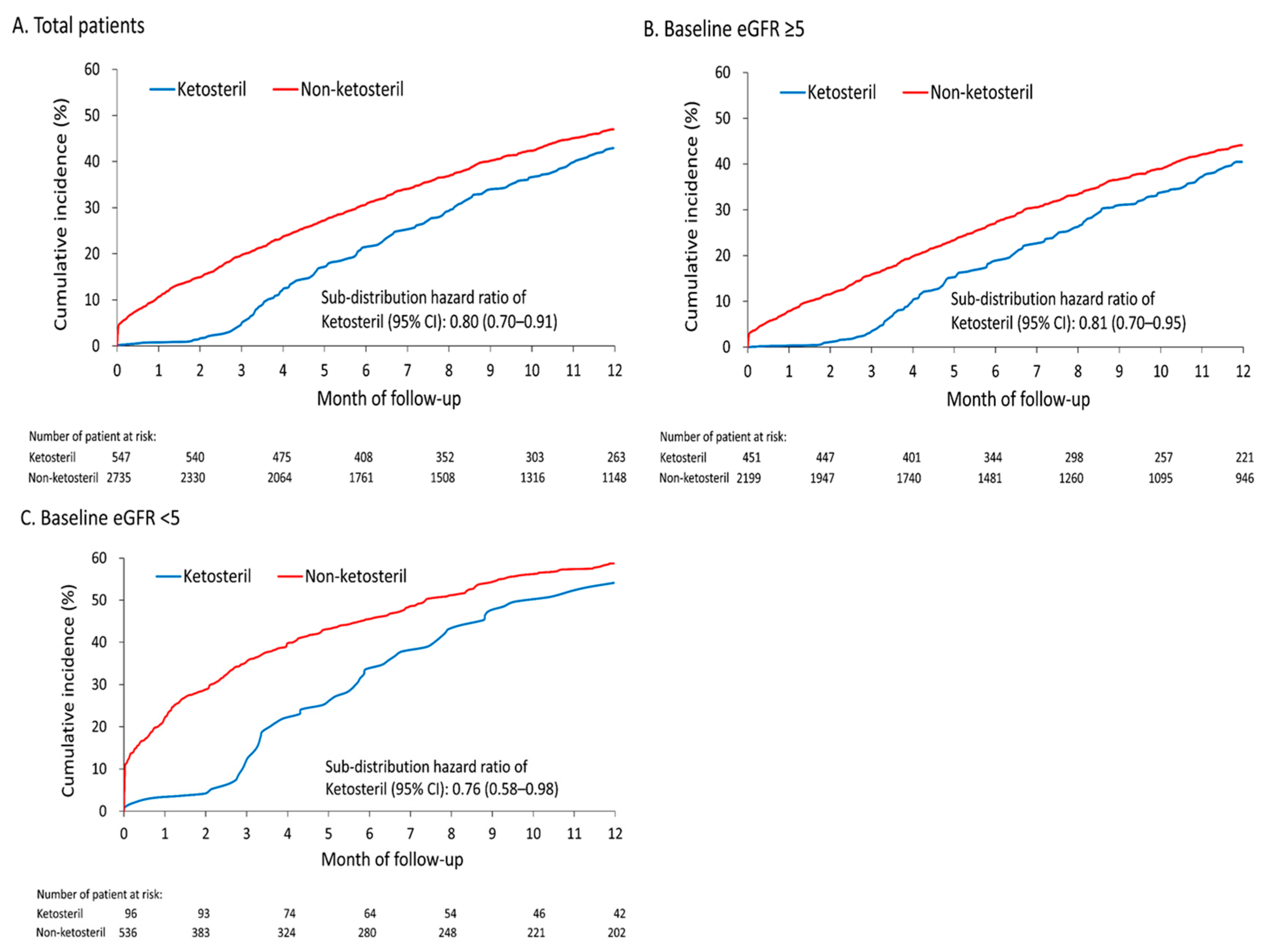
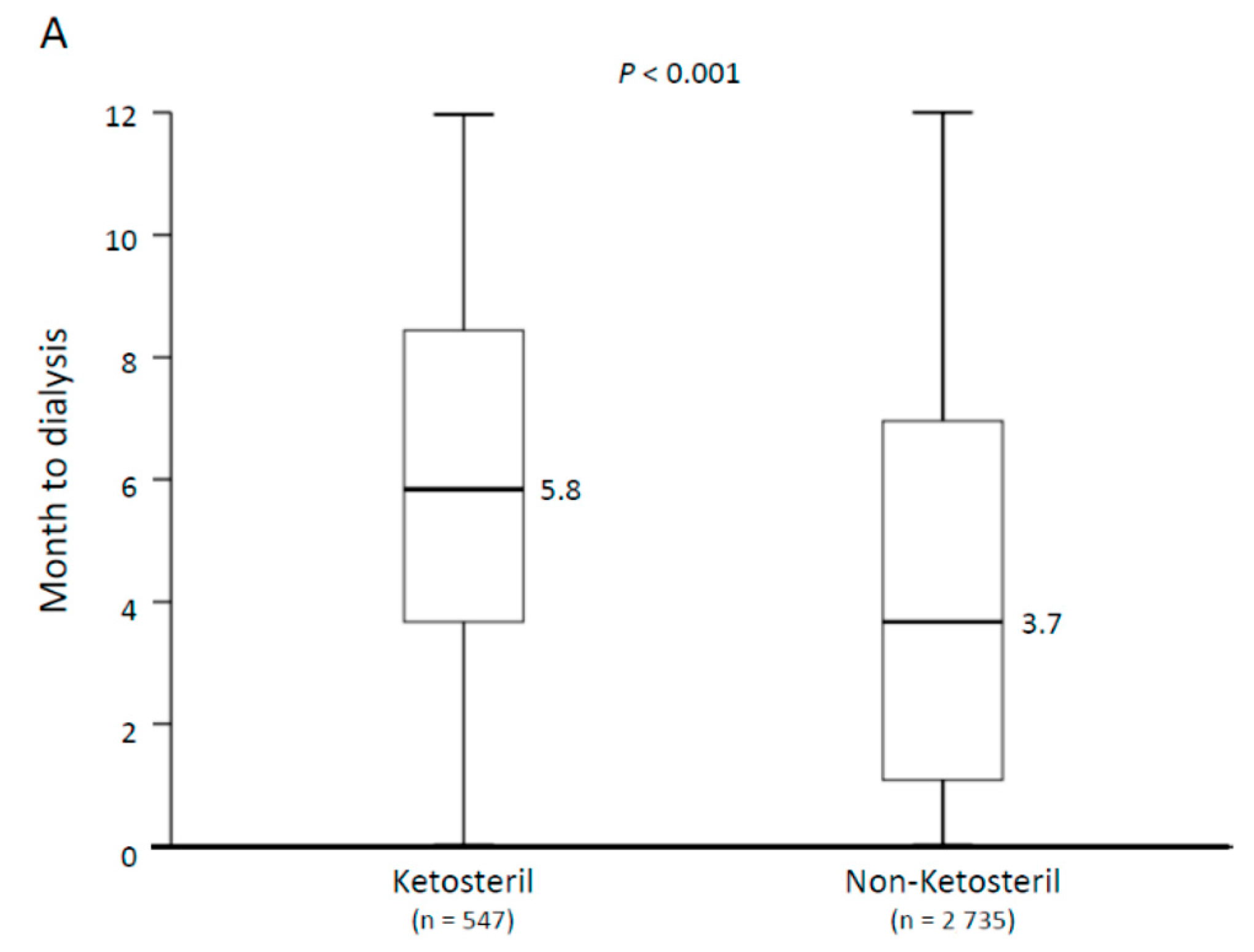
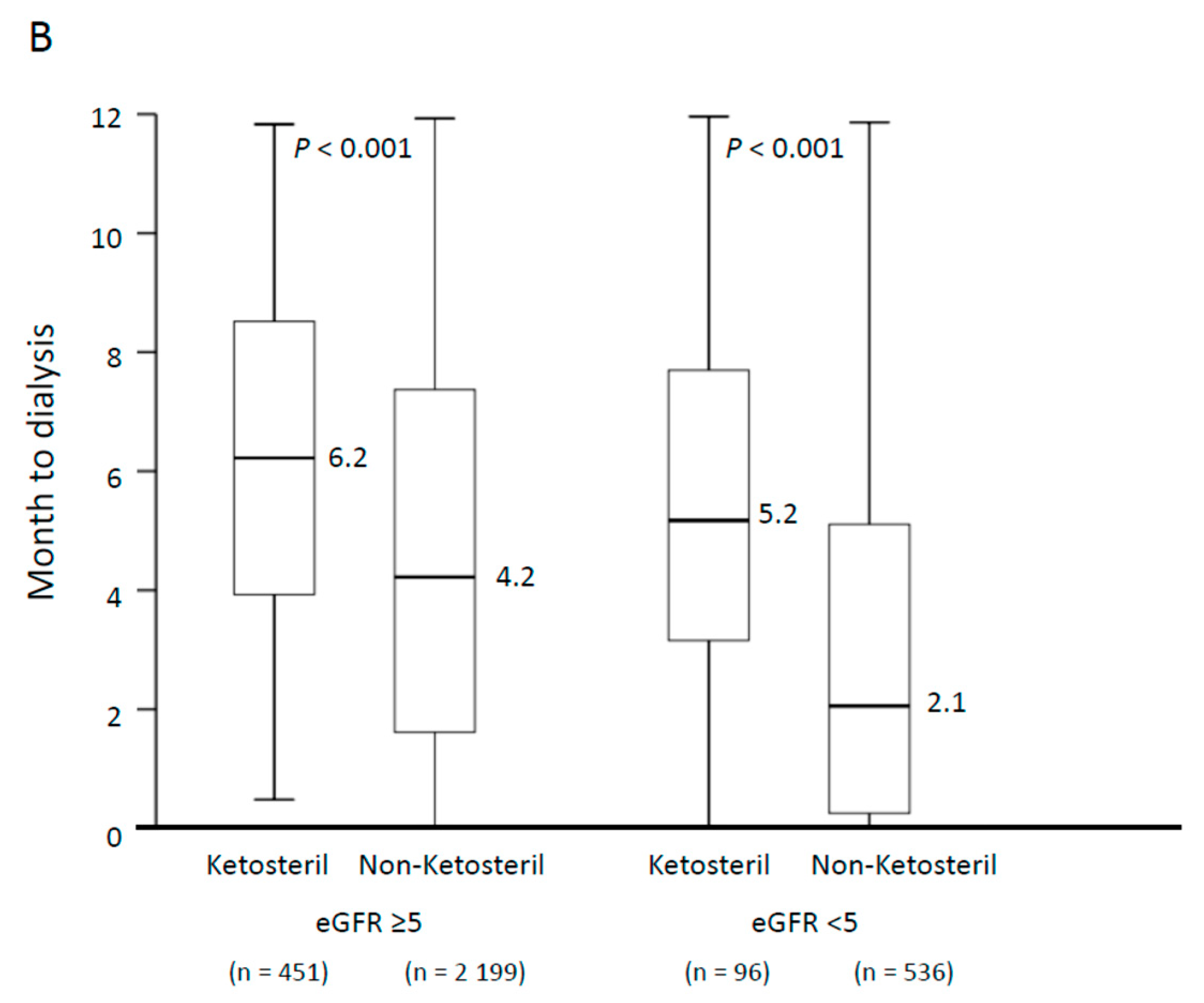
3.3. Risk of Dialysis across Different Baseline eGFRs
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Addis, T.; Lew, W. Diet and Death in Acute Uremia. J. Clin. Investig. 1939, 18, 773–775. [Google Scholar] [CrossRef] [PubMed]
- Lewis, D.S. On the Influence of a Diet with High Protein Content on the Kidney. Can. Med. Assoc. J. 1921, 11, 682–683. [Google Scholar] [PubMed]
- Cuppari, L.; Meireles, M.S.; Ramos, C.I.; Kamimura, M.A. Subjective Global Assessment for the Diagnosis of Protein–Energy Wasting in Nondialysis-Dependent Chronic Kidney Disease Patients. J. Ren. Nutr. 2014, 24, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Walser, M. Ketoacids in the treatment of uremia. Clin. Nephrol. 1975, 3, 180–186. [Google Scholar]
- Kang, C.W.; Tungsanga, K.; Walser, M. Effect of the level of dietary protein on the utilization of alpha-ketoisocaproate for protein synthesis. Am. J. Clin. Nutr. 1986, 43, 504–509. [Google Scholar] [CrossRef] [Green Version]
- Sunil, P.; Pande, D.P.; Sharma, S.; Sharma, D.; Bal, C.S.; Kulkarni, H. Randomized, double-blind, placebo-controlled trial to evaluate efficacy of ketodiet in predialytic chronic renal failure. J. Ren. Nutr. 2004, 14, 89–96. [Google Scholar] [CrossRef] [Green Version]
- National Kidney Foundation Kidney Disease Outcomes Quality Initiative. Clinical practice guidelines for nutrition in chronic renal failure. Am. J. Kidney Dis. 2000, 35, S1–S140. [Google Scholar]
- Walser, M.; Hill, S.B.; Ward, L.; Magder, L. A crossover comparison of progression of chronic renal failure: Ketoacids versus amino acids. Kidney Int. 1993, 43, 933–939. [Google Scholar] [CrossRef] [Green Version]
- Jiang, N.; Qian, J.; Sun, W.; Lin, A.; Cao, L.; Wang, Q.; Ni, Z.; Wan, Y.; Linholm, B.; Axelsson, J.; et al. Better preservation of residual renal function in peritoneal dialysis patients treated with a low-protein diet supplemented with keto acids: A prospective, randomized trial. Nephrol. Dial. Transplant. 2009, 24, 2551–2558. [Google Scholar] [CrossRef] [Green Version]
- Bellizzi, V.; Chiodini, P.; Cupisti, A.; Viola, B.F.; Pezzotta, M.; De Nicola, L.; Minutolo, R.; Barsotti, G.; Piccoli, G.B.; Di Iorio, B. Very low-protein diet plus ketoacids in chronic kidney disease and risk of death during end-stage renal disease: A historical cohort controlled study. Nephrol. Dial. Transplant. 2015, 30, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.-H.; Yang, Y.-W.; Hung, S.-C.; Kuo, K.-L.; Wu, K.-D.; Wu, V.-C.; Hsieh, T.-C.; National Taiwan University Study Group on Acute Renal Failure (NSARF). Ketoanalogues supplementation decreases dialysis and mortality risk in patients with anemic advanced chronic kidney disease. PLoS ONE 2017, 12, e0176847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cianciaruso, B.; Pota, A.; Pisani, A.; Torraca, S.; Annecchini, R.; Lombardi, P.; Capuano, A.; Nazzaro, P.; Bellizzi, V.; Sabbatini, M. Metabolic effects of two low protein diets in chronic kidney disease stage 4-5--a randomized controlled trial. Nephrol. Dial. Transplant. 2008, 23, 636–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccoli, G.B.; Nazha, M.; Capizzi, I.; Vigotti, F.N.; Mongilardi, E.; Bilocati, M.; Avagnina, P.; Versino, E. Patient Survival and Costs on Moderately Restricted Low-Protein Diets in Advanced CKD: Equivalent Survival at Lower Costs? Nutrients 2016, 8, 758. [Google Scholar] [CrossRef] [Green Version]
- Yen, C.-L.; Tu, K.-H.; Lin, M.-S.; Chang, S.-W.; Fan, P.-C.; Hsiao, C.-C.; Chen, C.-Y.; Hsu, H.-H.; Tian, Y.-C.; Chang, C.-H. Does a Supplemental Low-Protein Diet Decrease Mortality and Adverse Events After Commencing Dialysis? A Nationwide Cohort Study. Nutrients 2018, 10, 1035. [Google Scholar] [CrossRef] [Green Version]
- Klahr, S.; Levey, A.S.; Beck, G.J.; Caggiula, A.W.; Hunsicker, L.; Kusek, J.W.; Striker, G. The Effects of Dietary Protein Restriction and Blood-Pressure Control on the Progression of Chronic Renal Disease. N. Engl. J. Med. 1994, 330, 877–884. [Google Scholar] [CrossRef]
- Cianciaruso, B.; Capuano, A.; D’Amaro, E.; Ferrara, N.; Nastasi, A.; Conte, G.; Bellizzi, V.; Andreucci, V.E. Dietary compliance to a low protein and phosphate diet in patients with chronic renal failure. Kidney Int. Suppl. 1989, 27, 173–176. [Google Scholar]
- Tsai, M.-S.; Lin, M.-H.; Lee, C.-P.; Yang, Y.-H.; Chen, W.-C.; Chang, G.-H.; Tsai, Y.-T.; Chen, P.-C.; Tsai, Y.-H. Chang Gung Research Database: A multi-institutional database consisting of original medical records. Biomed. J. 2017, 40, 263–269. [Google Scholar] [CrossRef]
- Shao, S.; Chan, Y.; Yang, Y.K.; Lin, S.; Hung, M.; Chien, R.; Lai, C.; Lai, E.C. The Chang Gung Research Database—A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Kasiske, B.L.; Lakatua, J.D.; Ma, J.Z.; Louis, T.A. A meta-analysis of the effects of dietary protein restriction on the rate of decline in renal function. Am. J. Kidney Dis. 1998, 31, 954–961. [Google Scholar] [CrossRef]
- Laville, M.; Boissel, J.-P. Low protein diets for chronic kidney disease in non diabetic adults. Cochrane Database Syst. Rev. 2006, CD001892. [Google Scholar] [CrossRef]
- Pedrini, M.T.; Levey, A.S.; Lau, J.; Chalmers, T.C.; Wang, P.H. The Effect of Dietary Protein Restriction on the Progression of Diabetic and Nondiabetic Renal Diseases. Ann. Intern. Med. 1996, 124, 627–632. [Google Scholar] [CrossRef] [PubMed]
- Malvy, D.; Maingourd, C.; Pengloan, J.; Bagros, P.; Nivet, H. Effects of severe protein restriction with ketoanalogues in advanced renal failure. J. Am. Coll. Nutr. 1999, 18, 481–486. [Google Scholar] [CrossRef]
- Di Iorio, B.; Di Micco, L.; Torraca, S.; Sirico, M.L.; Russo, L.; Pota, A.; Mirenghi, F.; Russo, D. Acute Effects of Very-Low-Protein Diet on FGF23 Levels: A Randomized Study. Clin. J. Am. Soc. Nephrol. 2012, 7, 581–587. [Google Scholar] [CrossRef]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mircescu, G. Ketoanalogue-Supplemented Vegetarian Very Low–Protein Diet and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [CrossRef] [Green Version]
- Brunori, G.; Viola, B.F.; Parrinello, G.; De Biase, V.; Como, G.; Franco, V.; Garibotto, G.; Zubani, R.; Cancarini, G.C. Efficacy and Safety of a Very-Low-Protein Diet When Postponing Dialysis in the Elderly: A Prospective Randomized Multicenter Controlled Study. Am. J. Kidney Dis. 2007, 49, 569–580. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Gul, A.; Sarnak, M.J. Cardiovascular risk factors in chronic kidney disease. Kidney Int. 2005, 68, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Hassan, H.I.C.; Tang, M.; Djurdjev, O.; Langsford, D.; Sood, M.M.; Levin, A. Infection in advanced chronic kidney disease leads to increased risk of cardiovascular events, end-stage kidney disease and mortality. Kidney Int. 2016, 90, 897–904. [Google Scholar] [CrossRef] [PubMed]
- Mircescu, G.; Gârneaţă, L.; Stancu, S.; Capuşă, C. Effects of a Supplemented Hypoproteic Diet in Chronic Kidney Disease. J. Ren. Nutr. 2007, 17, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.; Fouque, D.; Laville, M.; Zech, P. Effects of low-protein diet supplemented with ketoacids on plasma lipids in adult chronic renal failure. Miner. Electrolyte Metab. 1996, 22, 143–146. [Google Scholar] [PubMed]
- Bellizzi, V.; Di Iorio, B.; De Nicola, L.; Minutolo, R.; Zamboli, P.; Trucillo, P.; Catapano, F.; Di Cristofano, C.; Scalfi, L.; Conte, G.; et al. Very low protein diet supplemented with ketoanalogs improves blood pressure control in chronic kidney disease. Kidney Int. 2007, 71, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauveau, P.; Combe, C.; Rigalleau, V.; Vendrely, B.; Aparicio, M. Restricted Protein Diet Is Associated With Decrease in Proteinuria: Consequences on the Progression of Renal Failure. J. Ren. Nutr. 2007, 17, 250–257. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Valid N | Ketosteril Group (n = 547) | Non- Ketosteril Group (n = 2735) | p Value |
|---|---|---|---|---|
| Male sex | 3282 | 278 (50.8) | 1383 (50.6) | 0.913 |
| Age (years) | 3282 | 62.2 (53.3, 72.0) | 62.7 (53.7, 71.7) | 0.777 |
| Baseline comorbidity | ||||
| Diabetes | 3282 | 224 (41.0) | 1122 (41.0) | 0.975 |
| Hepatitis B virus infection | 3282 | 5 (0.9) | 10 (0.4) | 0.083 |
| Hepatitis C virus infection | 3282 | 6 (1.1) | 3 (0.1) | <0.001 |
| Hypertension | 3282 | 366 (66.9) | 1758 (64.3) | 0.240 |
| Renal function | ||||
| eGFR (mL/min/1.73 m2) | 3282 | 6.7 (5.4, 8.5) | 6.7 (5.3, 8.8) | 0.830 |
| Baseline eGFR < 10 (%) | 3282 | 477 (87.2) | 2322 (84.9) | 0.165 |
| Baseline eGFR < 5 (%) | 3282 | 96 (17.6) | 536 (19.6) | 0.268 |
| Albumin/creatinine ratio (mg/d) | 152 | 2072 (1106, 3448) | 1857 (575, 4029) | 0.842 |
| Urine protein (U)/creatinine ratio (mg/d) | 556 | 2053 (1104, 4987) | 2688 (1046, 5640) | 0.440 |
| Laboratory data | ||||
| HbA1c (%) | 1420 | 6.2 (5.6, 7.0) | 6.3 (5.7, 7.2) | 0.174 |
| Total cholesterol (mg/dL) | 1674 | 172 (146, 196) | 170 (144, 199) | 0.556 |
| Triglyceride, mg/dL | 1652 | 118 (83, 185) | 123 (86, 181) | 0.692 |
| Antihypertensive therapy | ||||
| Antihypertensive drugs | 3282 | 366 (66.9) | 1758 (64.3) | 0.240 |
| ACEIs/ARBs | 3282 | 324 (59.2) | 1318 (48.2) | <0.001 |
| Nitrogen waste products | ||||
| Serum urea (mg/dL) | 3055 | 77.6 (62.0, 93.5) | 74.0 (58.0, 93.0) | 0.022 |
| Serum uric acid (mg/dL) | 2036 | 7.6 (6.6, 8.8) | 7.5 (6.4, 8.9) | 0.434 |
| Acid-base balance | ||||
| Serum bicarbonate (mEq/L) | 1542 | 19.5 (17.0, 22.0) | 20.4 (17.6, 22.8) | 0.008 |
| Calcium-phosphorus metabolism | ||||
| Serum calcium (mg/dL) | 2839 | 8.6 (8.2, 8.9) | 8.6 (8.1, 9.1) | 0.106 |
| Serum phosphates (mg/dL) | 2725 | 5.1 (4.3, 5.8) | 5.1 (4.3, 5.9) | 0.951 |
| Calcium supplementation | 3282 | 145 (26.5) | 566 (20.7) | 0.003 |
| Vitamin D therapy | 3282 | 62 (11.3) | 174 (6.4) | <0.001 |
| Unadjusted Analysis | Adjusted Analysis # | |||||
|---|---|---|---|---|---|---|
| Outcome | Ketosteril Group (n = 547) | Non-Ketosteril Group (n = 2735) | HR or SHR of Ketosteril (95% CI) | p Value | HR or SHR of Ketosteril (95% CI) | p Value |
| Primary outcome: dialysis | 220 (40.2) | 1215 (44.4) | 0.80 (0.70–0.91) | 0.001 | 0.73 (0.64–0.84) | <0.001 |
| Secondary outcome: | ||||||
| All-cause mortality | 10 (1.8) | 67 (2.4) | 0.73 (0.38–1.43) | 0.362 | 0.74 (0.38–1.43) | 0.367 |
| Acute myocardial infarction | 7 (1.3) | 63 (2.3) | 0.55 (0.25–1.19) | 0.129 | 0.50 (0.23–1.11) | 0.088 |
| Ischemic stroke | 6 (1.1) | 46 (1.7) | 0.64 (0.28–1.50) | 0.309 | 0.61 (0.26–1.42) | 0.253 |
| MACCE * | 20 (3.7) | 160 (5.9) | 0.61 (0.38–0.97) | 0.035 | 0.58 (0.36–0.92) | 0.021 |
| Infection-related hospitalization | 85 (15.5) | 479 (17.5) | 0.86 (0.68–1.08) | 0.193 | 0.83 (0.66–1.05) | 0.126 |
| Heart failure hospitalization | 15 (2.7) | 95 (3.5) | 0.78 (0.45–1.34) | 0.362 | 0.73 (0.42–1.25) | 0.247 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yen, C.-L.; Fan, P.-C.; Lee, C.-C.; Kuo, G.; Tu, K.-H.; Chen, J.-J.; Lee, T.-H.; Hsu, H.-H.; Tian, Y.-C.; Chang, C.-H. Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis? Nutrients 2020, 12, 3358. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113358
Yen C-L, Fan P-C, Lee C-C, Kuo G, Tu K-H, Chen J-J, Lee T-H, Hsu H-H, Tian Y-C, Chang C-H. Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis? Nutrients. 2020; 12(11):3358. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113358
Chicago/Turabian StyleYen, Chieh-Li, Pei-Chun Fan, Cheng-Chia Lee, George Kuo, Kun-Hua Tu, Jia-Jin Chen, Tao-Han Lee, Hsiang-Hao Hsu, Ya-Chun Tian, and Chih-Hsiang Chang. 2020. "Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis?" Nutrients 12, no. 11: 3358. https://0-doi-org.brum.beds.ac.uk/10.3390/nu12113358